
Abstract
Objective
This study aims to evaluate the effectiveness of digital health interventions compared to standard care in promoting exclusive breastfeeding (EBF) among postpartum women in low-and middle-income countries (LMICs).
Methods
The PRISMA guidelines of reporting were followed for the searching of four databases and screening following eligibility criteria: articles presenting digital health interventions, conducted as randomized control trials (RCTs), quasi-experimental, or mixed-method studies, reporting on EBF duration and early initiation of breastfeeding, and published in the English language were included.
Results
Of 1595 articles screened, only 10 published between 2013 and 2023 met the criteria. Most studies were from Nigeria (n = 3), with others from Kenya, South Africa, Ethiopia, China, India, and Lebanon. Six were RCTs, and four were quasi-experimental. The meta-analysis shows digital health interventions significantly increase EBF duration, with the strongest effects at 6 months (odds ratio (OR) = 2,1.66–2.40), followed by 5, 3, 2, and 1 month postpartum, including the initial feed.
Conclusion
This suggests digital health interventions have the potential to enhance breastfeeding practices among postpartum mothers in LMICs. For future research, it is essential to consider accessibility, delivery intervention, healthcare professional collaboration, and the sustainable development of digital health interventions for postpartum mothers in LMICs.
Introduction
The World Health Organization (WHO) defines exclusive breastfeeding (EBF) as an infant receiving only breast milk without any other liquids or solids, including water and expressed breast milk. 1 EBF provides many short-term and long-term benefits for both mothers and children. 2 The WHO, in its guidelines, recommends EBF for the first 6 months and has set a global goal of 6-month EBF to reach 50% of infants in 2025. 1 Globally 44% of children under 6 months of age are exclusively breastfed, 3 with low EBF rates reported in low- and middle-income countries (LMICs). LMICs face challenges in promoting EBF, including limited knowledge, short maternity leave, aggressive formula marketing, family beliefs, traditions, and unskilled healthcare professionals.4,5
It is well established that digital health, including text messaging, mobile apps, telemedicine, etc., can influence health outcomes. 6 Digital health interventions have become increasingly popular due to the ease with which they can be implemented and scaled to large and often dispersed populations 7 and can be more cost-effective compared to other interventions. 8 Several digital health studies initially conducted in LMIC have shown to improve the duration of EBF9–11 but thus far there has not been a collation of this body of evidence. Therefore, this systematic review aims to explore the existing research on the effectiveness of digital health interventions and synthesize the findings to determine whether digital health interventions have a statistically significant effect on EBF duration when compared to standard care in LMICs.
Methods
This systematic review followed the PRISMA guideline 12 and the Joanna Briggs Institute methodology for systematic reviews. 13 The process started with formulating the review questions, defining the PICO (population, intervention, comparator, and outcome) and eligibility criteria, developing the search strategy, selecting relevant articles, assessing the quality, extracting the data, analysing, and interpreting the results. The protocol was registered with PROSPERO 2023 (CRD42023391783).
This systematic review explores the effectiveness of digital health in supporting the EBF duration in LMIC. The inclusion criteria (Table 1) included PICO aspects, namely the key population (P) of interest was women who had no complications during birth and breastfeeding. The intervention (I) was digital health, with the key comparator (C) of interest being standard care. The primary outcome (O) compared was EBF duration and a secondary outcome was breastfeeding initiation within the first hour of life. In addition, the inclusion criteria included experimental and quasi-experimental study designs, with or without random allocations to groups, randomized controlled trials (RCTs), nonrandomized control trials, and mixed methods. All papers needed to be published in a peer-reviewed journal and studies had to be conducted in countries defined as LMICs, as defined by the World Bank. 14 Included studies had to have been published since 2013 The exclusion criteria were studies conducted with postpartum women with complications. Feasibility studies, case reports, qualitative studies, policy briefs, study protocols, reports from governmental and nongovernmental organizations, commentaries, systematic reviews, and oral presentations were excluded. Studies for which English translation was not possible also were excluded.
Eligibility criteria criteria.

EBF: exclusive breastfeeding; RCT: randomized controlled trial.
The search strategy was developed based on the PICO framework. The MeSH terms of each search term were explored with the assistance of a medical librarian to develop the final search strategy (Table 2). Four databases, namely, CINAHL, Pubmed, Proquest and Cochrane library were searched in February 2023. The digital health interventions were defined as eHealth, digital health, social media, online, Internet, web-based, telephone, telecommunication, eHealth, tele-referral, tele referral, tele-referrals, telehealth, virtual medicine, “medicine, virtual,” tele-intensive care, mobile application, mobile, cell phone, mobile health, health, mobile, mHealth, text message, text messaging, and short messaging system (SMS).
Searching strategy (PICO).

Search results were imported to Elsevier Mendeley Desktop Reference Manager and de-duplicated by two researcher (KK and JK). The final list of articles was exported into RIS format and then imported into Rayyan for initial screening of the titles and abstracts by two independent reviewers (TT and GC). Following the title and abstract screening, conflict resolution was discussed with the third (DM) and fourth (JT) reviewers. This was followed by the second stage of full-text screening which was reviewed by three independent reviewers (TT, JT, and GC) and any conflicts were resolved through online discussion with the fourth reviewer (DM). Reasons for the exclusion of papers at the full-text stage were recorded. The eligible studies were reported in a PRISMA flow diagram.
For the critical appraisal, the eligible studies were critically appraised by two independent reviewers (TT and GC) at the study level for methodological quality, using standardized critical appraisal instruments from the Joanna Briggs Institute (JBI) for RCTs and quasi-experimental studies. 15 Then, data was extracted from the eligible studies by two independent reviewers (TT and GC) using a standardized data extraction tool. The data extraction included the population criteria, study design, intervention and variables, results from two main outcomes, and strengths/limitations of these studies. Any conflicts in quality assessment or data extraction decisions were either resolved by discussion between the two researchers (TT and GC) or by a third researcher (DM). Finally, statistical pooling and meta-analysis were conducted to analyze the data.
Results
The initial search yielded 1595 articles from four databases, with 11 duplicates identified (Figure 1). After screening, 22 articles were selected for full-text review. Ten studies met the inclusion criteria and were included in the final sample, while 12 articles were excluded for reasons including incorrect intervention (n = 2), incorrect population (n = 4), incorrect study design (n = 4), and incorrect outcome (n = 2).

PRISMA flow chart of the study selection process.
Critical appraisal
Seven articles were found to be robustly conducted with a high level (70%) of quality, whereas three RCTs showed some areas of concern for bias (Tables 3 and 4). There were some biases in these three studies such as participants had not been blinded to treatment assignment and the treatment allocation was not concealed. However, there are challenges to blinding interventions given the nature of digital media versus standard care. These biases were discussed amongst the team and a decision was made that no papers were excluded during the critical appraisal stage.
Critical appraisal of the selected RCTs.
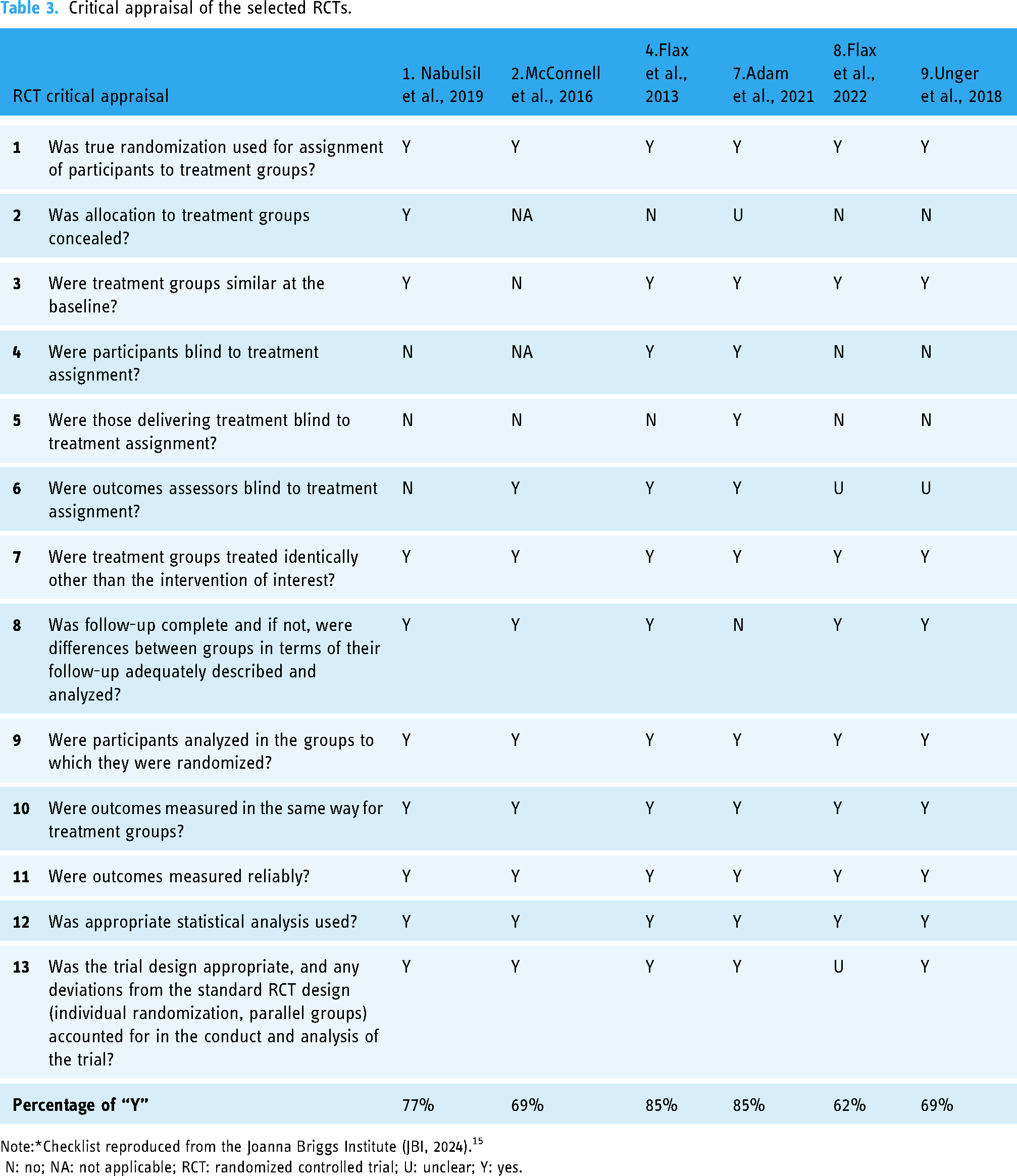
Note:*Checklist reproduced from the Joanna Briggs Institute (JBI, 2024). 15
N: no; NA: not applicable; RCT: randomized controlled trial; U: unclear; Y: yes.
Critical appraisal of the selected Quasi-experimental studies.

Note:*Checklist reproduced from the Joanna Briggs Institute (JBI, 2024). 15
N: no; NA: not applicable; U: unclear; Y: yes.
Study characteristics
Of the 10 studies, 7 were conducted in African countries (Nigeria =3,10,16,17 Kenya = 2,18,19 South Africa =1, 20 Ethiopia = 1, 11 while one each was conducted in China, 21 India, 22 and Lebanon 23 (Table 3)). One study was conducted and reported in two cities in Nigeria (Kaduna, Lagos). 10 Six of the studies were RCTs,10,16,18–20,23 while four were quasi-experimental.11,17,21,22 For the sample size, there were 28,984 participants in total. The largest study was a quasi-experimental study in India with 19,800 participants, 22 while 6 of the studies had under 600 participants. Studies were published between 2013 and 2023. The population targeted by most interventions were pregnant women and also newborns. Husbands were included in one study. 11
Various digital health interventions were found across all ten studies such as SMS,11,16,17,19,21 mHealth platform, 22 phone call,22,23 WhatsApp, 17 mass media (TV, radio, leaflet, spot advertisement, and poster),10,17 song/drama, 16 and video.20,22,23 Three studies conducted an intervention with a multicomponent package, for example, a package of health education (HE), phone call, peer support, maternal support, and (monthly) home visits, 23 or a package of HE, phone text/voice message, and song/drama, 16 or a package of HE and group support. 17 Nearly 90% of interventions started during the 3rd trimester of pregnancy and continued into the postpartum period, and the length depended on the outcome measurement of the study (Table 5).
The summary of the review studies.

RCT: randomized controlled trial.
The duration of EBF
Five of the 10 studies reported the 6-month EBF duration. Only four studies provided sufficient data for pooling in the meta-analysis. According to the meta-analysis, the overall estimate for the pooled effect is a risk ratio of 2.00 (95% confidence interval (CI) 1.66–2.40) indicating a statistically significance. This means that digital health interventions significantly doubled the chances of EBF for 6 months. However, a high degree of heterogeneity was found between the studies (I2 = 77%) (Figure 2). Four studies showed that the 6-month EBF duration in experimental group was significantly higher than the 6-month EBF duration in control group.16,17,19,21 The total sample size of these 4 studies was 2257 people. The interventions included video, phone calls, SMS, voice messages, songs, and dramas. The four studies were conducted in Lebanon, Nigeria, and China.

The effect of digital health on 6-month exclusive breastfeeding (EBF) duration.
The effect of digital health on 5-month EBF duration was reported by 2 studies only. The estimated pooled effect at 5-months found that the risk was significant but a little lower at 1.41 (95% CI 1.23–1.62) (Figure 3). Once again, there was a high level of heterogeneity between studies (I2 = 93%). In Kaduna, Nigeria, a positive differential effect of the intervention was found for EBF for 5 months (P < 0.05). 10 The other study in South Africa did not show a significant difference (P = 0.28). 20 The combined sample size of these 3 studies was 3635 participants. The interventions included video and mass media, such as posters, leaflets, infant and young child feeding (IYCF) messages on LED screens, television, and radio. Two of the studies were conducted in South Africa and Nigeria (Kaduna, Lagos).

The effect of digital health on 5-month exclusive breastfeeding (EBF) duration.
Two studies reported EBF rates at 4 months.19,21 In Kenya, there was a significant difference in EBF for 4 months 19 when digital interventions were implemented while a significant difference was not found in China. 21 The participants were only 736 people. The SMS was the main intervention. The two studies were carried out in Kenya and China.
Three studies reported the effect of digital health intervention on 3-month EBF duration.11,16,23 According to the forest plot, the estimated pooled effect is a significant risk ratio of 1.51 (95% CI was 1.14–2.01). with a higl level of heterogeneity (67%) (Figure 4). The EBF rate was significantly different in Ethiopia (P = 0.04) 11 and Nigeria (95% CI =1.1–3.0). 16 However, in Lebanon, there was no significant difference in EBF duration at the 3rd month (P = 0.07). 23 The participants were 816 people. The intervention were VDO, phone call, M-health, SMS, voice message, songs, and dramas. The research was conducted in Kenya, Nigeria, and Ethiopia.

The effect of digital health on 3-month exclusive breastfeeding (EBF) duration.
Three studies reported the EBF rate at 2 months with a significant estimated pooled effect of a lower risk ratio of 1.82 (95% CI 1.35–2.44) and a medium level of heterogeneity (I2 = 44%) (Figure 5). The total sample size was 1228 people. The interventions were video, SMS, mass-media messages, and WhatsApp. The research was conducted in the same country as the studies that reported the effect of digital health interventions on 3-month EBF duration.

The effect of digital health on 2-month exclusive breastfeeding (EBF) duration.
Four studies reported the effect of digital healthcare on 1-month EBF duration. The meta-analysis showed a high degree of heterogeneity (I2 = 64%) (Figure 6). The pooled effect was a statistically significant risk ratio of 1.88 (95% CI was 1.55–2.27). One study in Ethiopia showed the significance of 1-month EBF, 11 however, in Lebanon and South Africa, the nonsignificance of 1-month EBF was found.20,23 The studies included a total of 1998 participants. The interventions used were videos, phone calls, SMS, voice messages, songs, and dramas. The research took place in Lebanon, Nigeria, Ethiopia, and South Africa.

The effect of digital health on 1-month exclusive breastfeeding (EBF) duration.
The conclusions of the effectiveness of digital health on EBF duration across different time periods are presented in Figure 7. The Figure 7 shows a high impact at 1-month (1.88 times more likely that mothers EBF at one month if involved in a digital health intervention compared to other interventions) and then a gradual increase in the chances of EBF as time progresses to it being double the chance at 6 months

The conclusions of the effectiveness of digital health to exclusive breastfeeding (EBF) duration.
Five studies reported the effect of digital health on the initiation of BF duration (Figure 8). Overall, the estimated pooled effect is statistically significant with an odds ratio of 1.07 (95% CI 1.02–1.13) with a high degree of heterogeneity between the studies (I2 = 88%). Three studies showed a statistically significant difference between the experimental group and control group.10,16,22 The study of Balakrishnan et al. reported that the percentage of mothers initiating breastfeeding within 1 hour of birth was 97.7%, but this result was not statistically significant for the digital intervention. 22 Two other studies reported no significant increase in the initiation of breastfeeding rates17,20 when digital interventions were employed compared to usual care.

The effect of digital health on initiation of breastfeeding.
Discussion
This systematic review aimed to assess the effectiveness of digital health interventions compared to standard care in promoting EBF duration among postpartum mothers in LMICs. The findings reveal several important insights and implications for future research and practice.
The meta-analysis demonstrated that digital health interventions significantly impact the initiation of BF and EBF duration from 1 month right the way through to and more so at 6 months EBF compared to traditional health intervention. This suggests digital health interventions have the potential to enhance breastfeeding practices among postpartum mothers in LMICs, particularly to 6 months as per the WHO recommendations. These findings are consistent with previous studies highlighting the effectiveness of digital health tools, such as health education, SMS and song/drama intervention, 6 in promoting health behavior change, including breastfeeding. 17
The observed effectiveness of digital health interventions may be attributed to several factors. Firstly, the widespread availability and accessibility of smartphones in LMICs have facilitated the delivery of digital health interventions to a large population. 24 Moreover, the scalability and cost-effectiveness of digital health interventions make them a feasible solution for addressing breastfeeding disparities in resource-limited settings. 25
Another important point is integrating digital health interventions into existing healthcare systems. A strategic approach that ensures interoperability, usability, and sustainability should be implemented. Stakeholders, including healthcare professionals and postpartum mothers, should share their experiences with digital health, highlighting both the benefits and limitations. 26 Policymakers should also provide strategies to implement digital health in the current healthcare system. 27 Along with this process, IT teams and administrators should ensure smooth alignment of technology and workflows for digital health implementation. 28 The expansion of training programs, as well as monitoring and evaluation for both healthcare professionals and postpartum mothers to use digital health, is recommended. 26
Despite the promising findings, several limitations should be acknowledged. Firstly, the heterogeneity among the included studies in terms of intervention components, study designs, and outcome measures may have influenced the overall effect estimates. Additionally, the quality of evidence varied across studies, with some studies exhibiting a high risk of bias. Moreover, the long-term sustainability and scalability of digital health interventions beyond the study period remain uncertain.
Moving forward, future research should focus on addressing the methodological limitations identified in this review. Standardization of intervention components and outcome measures would facilitate comparability across studies and enhance the robustness of evidence. Longitudinal studies with extended follow-up periods are needed to evaluate the sustained impact of digital health interventions on breastfeeding outcomes. Furthermore, qualitative research exploring the acceptability and feasibility of digital health interventions among postpartum mothers in LMICs would provide valuable insights into implementation strategies.
Conclusions
In conclusion, digital health interventions show promise in promoting exclusive breastfeeding duration among postpartum mothers in LMICs. However, further research is warranted to optimize intervention delivery, and ensure long-term sustainability. Collaborative efforts between researchers, policymakers, and healthcare providers are essential to harness the potential of digital health technologies in improving maternal and child health outcomes, including EBF, globally.
Footnotes
Contributorship
All authors made a significant contribution to the work reported, whether that is in the conception, data searching, data extraction, data analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This systematic review and meta-analysis was registered with PROSPERO 2023 (CRD42023391783).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
The consent statement
The informed consent of this systematic and meta analysis is not applicable. All data is collected through database.