
Abstract
Background:
Breastfeeding is recommended for infants through 6 months of age, when solid foods are introduced, and continued until 12 months of age. However, many mothers in the United States discontinue breastfeeding at an early age and return to work following childbirth. The purpose of this study was to identify individual and organizational factors associated with breastfeeding practices in a sample of employed mothers who participated in the Infant Feeding Practices Study II.
Methods:
A secondary analysis was conducted on a sample of 953 employed mothers who completed the Infant Feeding Practices Study II between 2005 and 2007. The analysis compares infant feeding status (breastfeeding/feeding pumped milk vs. not breastfeeding/feeding pumped milk) over a 12-month period, using generalized linear mixed modeling (GLMM).
Findings:
Generalized linear mixed modeling (GLMM) revealed that working mothers who were employed part-time (≤34 hours/week) were 97% more likely to continue breastfeed compared with mothers employed full-time over the 12-month follow-up period (OR = 1.97, p = .002). Mothers who perceived high levels of breastfeeding support in the workplace were 178% more likely to continue breastfeeding compared with those with low levels of perceived support (OR = 2.78, p < .001).
Conclusions:
Prenatal breastfeeding only feeding intentions, non-smoking, part-time employment, and higher levels of perceived breastfeeding support in the workplace were significant predictors of breastfeeding/feeding pumped milk at all time points.
Application to Practice:
Occupational health nurses may be able to address barriers to breastfeeding in the workplace and improve supportive workplace practices to promote continued breastfeeding in employed mothers consistent with national and international recommendations.
Background
Breastfeeding provides widely recognized health benefits for mothers such as reduced risk of breast cancer, ovarian cancer, type 2 diabetes, myocardial infarction, and postpartum depression (Victora et al., 2016). Physical and mental health benefits for children who are breastfed are also well established (Horta et al., 2023; Soled et al., 2021). Multiple national and international health agencies recommend exclusive breastfeeding, defined as infant feeding with breast milk only, without any additional food or drink, until 6 months of age when solid foods are introduced, and continued breastfeeding until 12 months of age (Meek & Noble, 2022; World Health Organization, 2021). The most frequent reasons cited by employed mothers for discontinuing breastfeeding their babies before 6 months of age include lack of managerial lactation support, an unsupportive work environment, and difficulties locating suitable milk pumping and storage locations at work (Murtagh & Moulton, 2011; Spitzmueller et al., 2016). Olson and colleagues (2020) propose tangible workplace lactation supports (i.e., policy, support groups, physical facilities and break time) as well as intangible supports (i.e., coworkers and managers) influence employees breastfeeding behavior. Variations in the overall climate for lactation support in an organization as well as the development and evaluation of lactation support programs and policies may contribute to low rates of continued breastfeeding in employed mothers (Olson et al., 2020). In a review of worksite lactation accommodations, corporate lactation support was related to continued breastfeeding in employed mothers; conversely, physical facilities for lactation and break time for milk expression were not associated with sustained breastfeeding (Hilliard, 2016). Mothers in the United States continue to experience barriers to breastfeeding after return to work (Cheyney et al., 2019). Occupational health nurses are in a unique position to act as advocates for breastfeeding mothers through collaboration with employers, supervisors, and other key personnel in the workplace. Given that the labor force participation rate (percent of the population working or looking for work) for all mothers with children under the age of 18 was 71.2% in 2021 (U.S. Bureau of Labor Statistics, 2022a), the need for research on factors associated with sustained breastfeeding in employed mothers is critically important.
The Socio-Ecological Model (Figure 1) was used to guide the examination of individual and organizational factors associated with breastfeeding practices in employed mothers. The Socio-Ecological Model framework, first introduced by Bronfenbrenner in 1974 and later expanded by McLeroy, Bibeau, Steckler, and Glanz, is a theory-based framework for understanding the multifaceted and interactive effects of personal and environmental factors that influence behavior (McLeroy et al., 1988). The Socio-Ecological Model describes five dimensions that influence health behavior including individual, interpersonal, organizational, community, and public policy. The Socio-Ecological Model is useful in identifying multi-level factors that may influence an employed mother’s decision to continue or discontinue breastfeeding. The purpose of this study was to identify individual and organizational factors, guided by the Socio-Ecological Model, associated with breastfeeding practices in a sample of employed mothers who participated in the Infant Feeding Practices Study II (IFPS II).
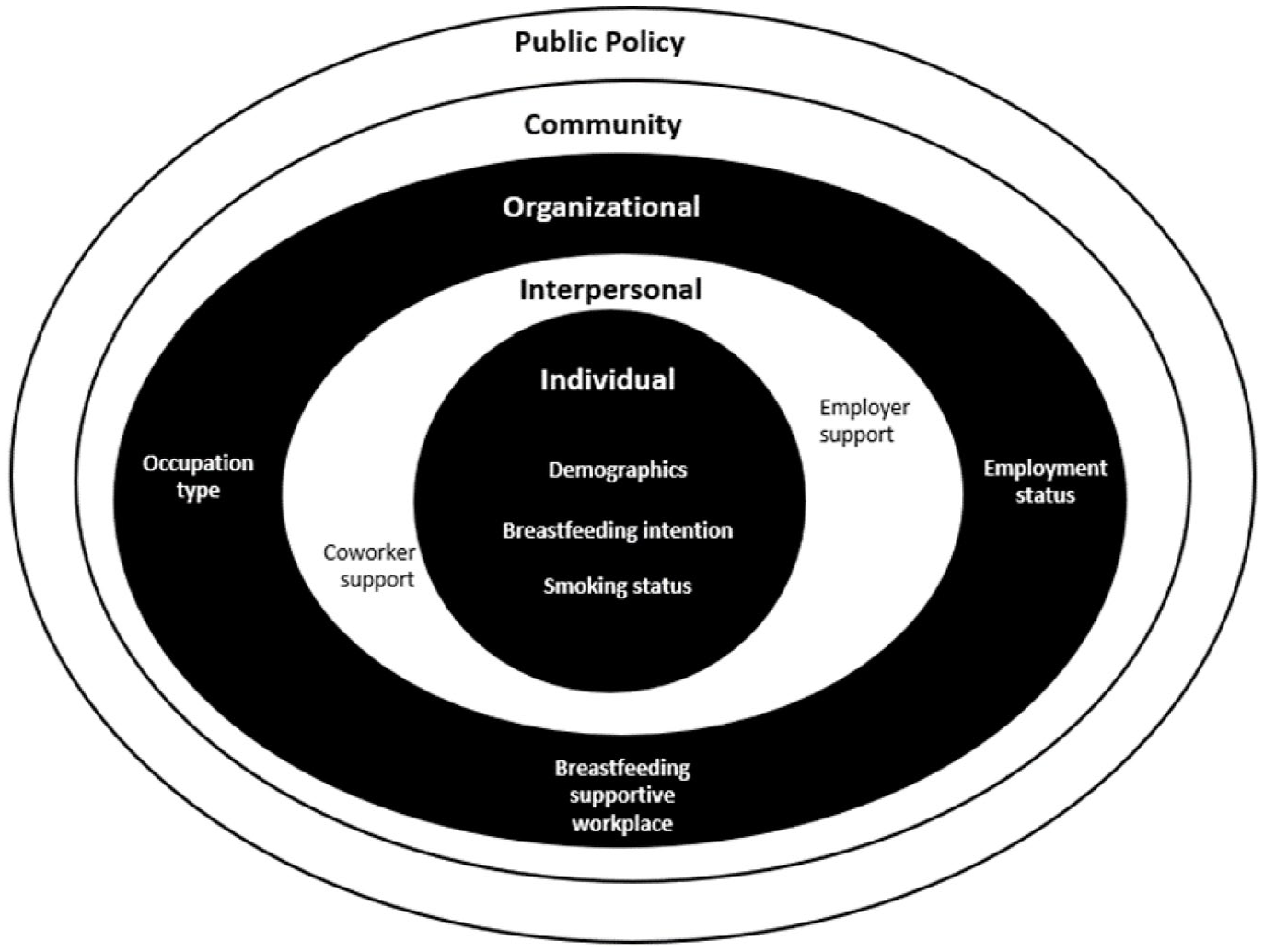
Socio-Ecological Model to Promote Breastfeeding Continuation in Employed Mothers.
The specific aims were to (a) examine the association of individual factors (e.g., prenatal infant feeding intentions and smoking status) and breastfeeding/feeding pumped milk versus not breastfeeding/feeding pumped milk at 3-, 6-, 9-, and 12-month assessments controlling for age, race, marital status, and household income; and (b) examine the association of organizational factors (e.g., employment status, occupation type, and perceived level of breastfeeding support in workplace) and breastfeeding/feeding pumped milk versus not breastfeeding/feeding pumped milk at all time intervals; controlling for age, race, marital status, and household income.
It was hypothesized that employed mothers who expressed prenatal intention to breastfeed only and are not current smokers would be more likely to breastfeed/feed pumped milk at all-time intervals (3, 6, 9, and 12 months, controlling for age, race, marital status, and household income). Regarding organizational factors, mothers who work part-time would be more likely to breastfeed/feed pumped milk compared with mothers who work full-time at all-time intervals, controlling for age, race, marital status, and household income. In addition, mothers in professional/executive occupations would be more likely to breastfeed/feed pumped milk at all time intervals compared with women employed in other occupations, controlling for age, race, marital status, and household income. Furthermore, employed mothers who report a more supportive workplace environment for breastfeeding would be more likely to breastfeed/feed pumped milk compared with women who report lower levels of breastfeeding support in the workplace at all time intervals, controlling for age, race, marital status, and household income.
Methods
Study Population and Recruitment
This study was a secondary analysis of the Infant Feeding Practices Study II, a longitudinal study focused on infant feeding practices conducted by the Food and Drug Administration (FDA) and Centers for Disease Control and Prevention (CDC, 2017). The population for the IFPS II study was drawn from Synovate, a consumer opinion panel consisting of 500,000 households, throughout the United States between 2005 and 2007. Women had to be at least 18 years old and able to speak English to be eligible to participate in the IFPS II. Between May and December 2005, 4,900 pregnant women from across the United States were recruited via mail to participate in the IFPS II and invited to complete a series of 12 surveys including a demographic and prenatal survey during the third trimester, a birth screener interview at the time of delivery, and postpartum surveys monthly from 2 to 7 months of age and then every 7 weeks until the infant was 12 months old. To qualify for the IFPS II postpartum surveys, the infant had to be a singleton born at ≥35 weeks gestation, weighing at least 5 lbs, and without medical conditions that would affect feeding. Approximately 2,000 mother–infant dyads completed the final 12-month postpartum assessment (CDC, 2017).
The IFPS II survey items provided detailed information including foods fed to infants, including breast milk; contributing factors to infant feeding practices and breastfeeding success; and mothers’ employment status. Postpartum questionnaires were mailed to the mother monthly from the time her infant was 2 months through 7 months of age, then 3 times (about every 7 weeks) until 12 months of age, for a total of nine postpartum surveys. These questionnaires consisted of nine modules containing content related to infant feeding and health; breastfeeding cessation; breastfeeding, pumping and expressing milk; and employment. Overall, response rates ranged from 63% to 87% across all questionnaires for the full study (CDC, 2017).
Study Protocol
To qualify for this analysis, participants were employed either part-time (≤ 34 hours/week) or full-time (> 35 hours/week) at any time during the 12-month postpartum period and must have answered all variables of interest at the four time points (3-, 6-, 9-, and 12-month postpartum). A secondary analysis was conducted on a sample of 953 employed mothers who participated in the IFPS II to compare infant feeding status (breastfeeding/feeding pumped milk vs. not breastfeeding/feeding pumped milk) over a 12-month period. Institutional review board approval through the Office of Research Integrity at the University of Kentucky was not required as the data were publicly available and deidentified. Individual factors including age (years), race (White or non-White); marital status (married or unmarried); and household income ($0–$59,999 or > $60,000) were collected during the prenatal survey. Prenatal feeding intention (breastfeed only versus breast/formula feed or formula feed only) was also collected at the prenatal survey. Smoking status (number of cigarettes smoked per day) and employment status, assessed as work for pay within the past 4 weeks (yes/no), were collected during the prenatal survey as well as the 3-, 6-, 9- and 12-month postpartum surveys. Organizational variables collected during the 3-, 6-, 9-, and 12-month postpartum surveys included the number of hours the mothers worked per week (X number of hours per week); occupation type (broad categories such as professional, administrative support, sales, etc.); and level of perceived breastfeeding support in place of employment (1 = not at all supportive, 2 = not too supportive, 3 = somewhat supportive, and 4 = very supportive). For this analysis, variables were recoded into numbers of hours worked per week for employment status (part-time ≤ 34 hours/week or full-time > 35 hours/week); occupation type (professional/executive or other occupation types); and level of perceived support for breastfeeding in place of employment from low = 1 (not at all supportive or not too supportive) to high = 2 (somewhat supportive and very supportive). Scores for perceived support for breastfeeding in place of employment ranged from 1 to 2, with higher scores reflecting more support. Breastfeeding status was collected during the 3-, 6-, 9- and 12-month postpartum surveys by asking the mother if she breastfed or fed pumped milk for any time in the past 4 weeks (yes/no).
Data Analysis
Descriptive statistics, including means and standard deviations or frequency distributions, were used to characterize the sample. Women who reported breastfeeding/feeding pumped milk at designated time intervals were compared with those not breastfeeding/feeding pumped milk at designated time intervals (3, 6, 9, and 12 months) using independent t tests for continuous variables and chi-square tests of association for categorical variables. Group comparisons were made between those breastfeeding/feeding pumped milk and those not at each of the time intervals (for prenatal breastfeeding intention and similarly for smoking status, employment status, occupation type, and perceived breastfeeding support in the workplace).
Generalized linear mixed modeling (GLMM) was used to identify which individual and organizational factors were most strongly linked to the binary outcome (breastfeeding/feeding pumped milk vs. not breastfeeding/feeding pumped milk) over the 12-month follow-up period. Since the participants were employed mothers who were invited to complete Infant Feeding Practices Study II (IFPS II) surveys at multiple points in time, with clustered responses due to the repeated measures design, GLMM was chosen as an appropriate data analysis method. The logistic link function was specified given the binary outcome. Time-dependent factors included infant feeding status (breastfeeding/feeding pumped milk vs. not breastfeeding/feeding pumped milk; the outcome variable), smoking status, and breastfeeding support in the workplace at the four time points (3, 6, 9, and 12 months postpartum). Data were analyzed using SPSS version 27.0 for Windows (IBM, 2020, SPSS, New York, United States) and SAS version 9.4 (SAS, 2020, North Carolina, United States). An a priori alpha level of .05 was used as the significance level for the analysis.
Results
At baseline (3 months postpartum; N = 953), over half of the mothers were breastfeeding or feeding pumped milk (57%). The mean age of the sample was 29.6 ± 5.4, and the sample was predominantly White (88%) and married (79%). Most participants had a household income of less than $60,000 (68%), and six of 10 mothers (62%) expressed prenatal infant feeding intentions to only breastfeed following the birth of the child. The majority (86%) did not smoke cigarettes during the prenatal period (Table 1).
Demographic and Individual Characteristics of Employed Mothers Who Participated in IFPS II Survey at 3 Months Postpartum, With Comparisons by Breastfeeding Status (N = 953)
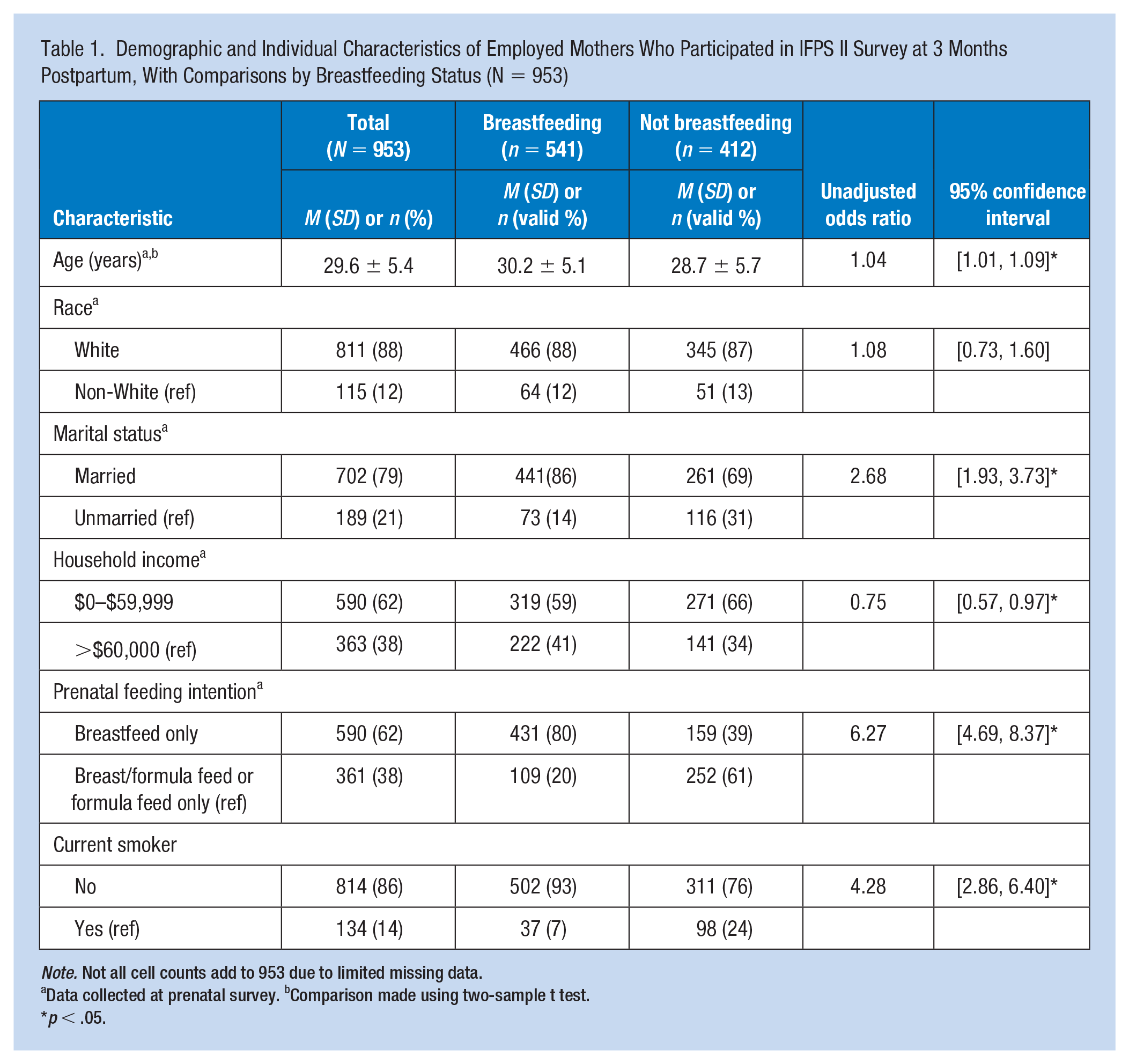
Note. Not all cell counts add to 953 due to limited missing data.
Data collected at prenatal survey. bComparison made using two-sample t test.
p < .05.
More than half of the mothers (54%) worked part-time; slightly less than half (49%) worked in professional or executive occupations. Most participants (81%) reported their workplace was either very supportive (50%) or somewhat supportive of breastfeeding (31%) (Table 2). Breastfeeding employed mothers were significantly older (p < .001), more likely to be married (p < .001), and reported a higher socioeconomic status (p = .019). They expressed prenatal infant feeding intentions to breastfeed only (p < .001), were more likely to be non-smokers (p < .001), employed part-time (p = .001) in a professional/executive occupation (p < .001), and reported a higher level of perceived breastfeeding support in the workplace (p < .001) compared with non-breastfeeding employed mothers (Tables 1 and 2).
Organizational Factors Associated With Breastfeeding Status in Employed Mothers Who Participated in the IFPS II at 3 Months Postpartum (N = 953)
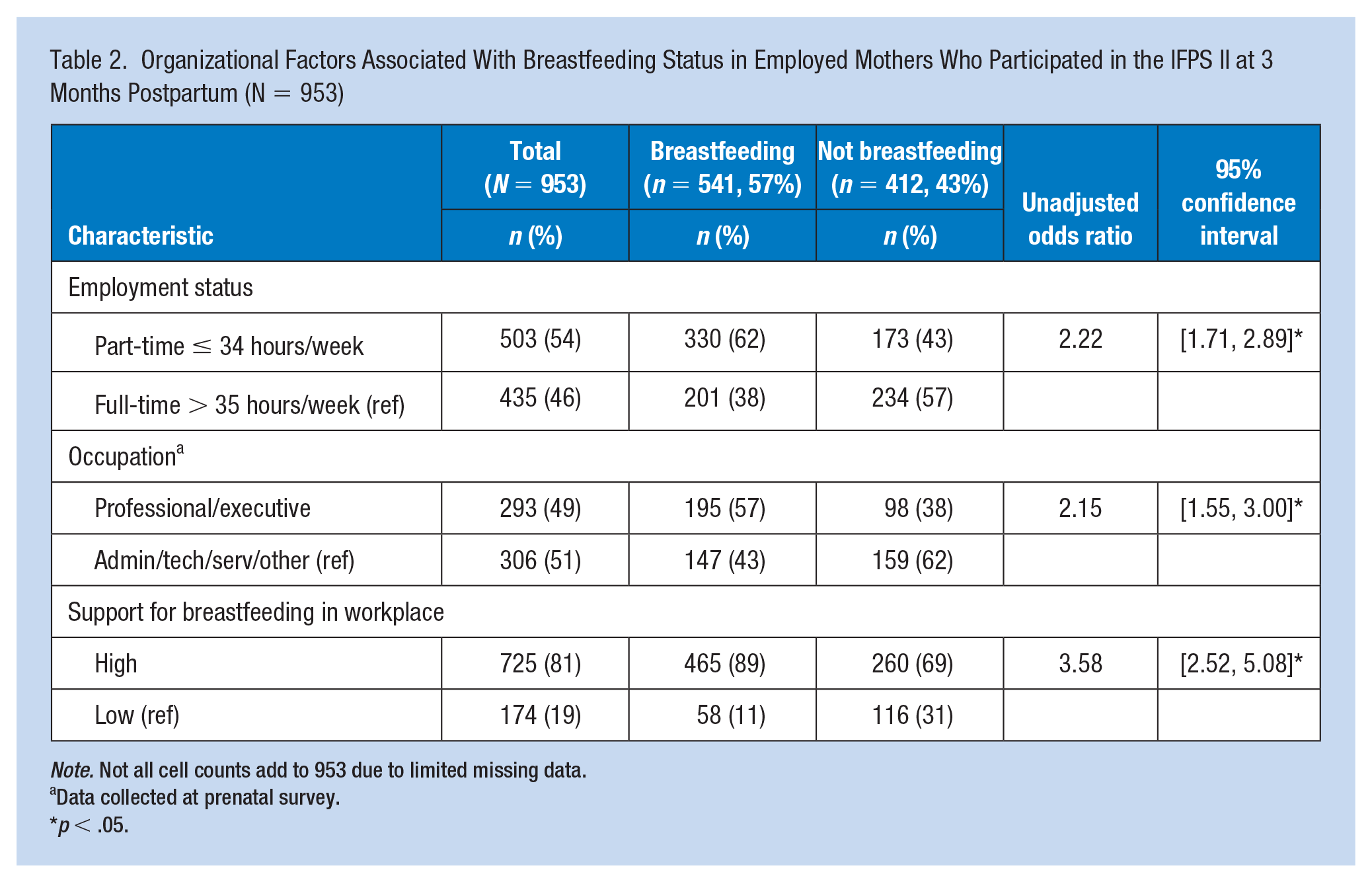
Note. Not all cell counts add to 953 due to limited missing data.
Data collected at prenatal survey.
p < .05.
Prenatal infant feeding intention, smoking status, employment status, and perceived level of breastfeeding support in the workplace remained factors associated with breastfeeding status at all subsequent time points. Occupation type was associated with breastfeeding status at the 6- and 9-month assessments; however, it was no longer associated with breastfeeding status at the 12-month assessment.
The GLMM included results for a sample of employed mothers who worked either part-time (≤34 hours/week) or full-time (>35 hours/week) over the 12-month postpartum period, including variables correlated with breastfeeding/feeding pumped milk in the bivariate analysis at any of the four time points (3, 6, 9, and 12 months postpartum) as well as demographic factors included as controls including age, race, marital status, and household income (n = 302). These variables were adjusted for in the model since they are well known to be associated with breastfeeding status. In the GLMM subsample, the mean age was 31.2 (SD = 5.1), predominately White (89%), and married (82%). Slightly over half (55%) of the subsample had a household income of $60,000 or less, and 62% of the participants expressed prenatal infant feeding intentions to breastfeed only. Most participants in the subsample were employed in professional/executive occupations (70%) and support for breastfeeding in the workplace ranged from 77% at the 3-month postpartum survey to 80% at the 12-month survey. Rates of breastfeeding/feeding pumped milk in subsample participants decreased from 59% at 3 months postpartum to 22% at the 12-month survey. Comparatively, rates of breastfeeding/feeding pumped milk in the full sample decreased from 60% at 3 months postpartum to 25% at the 3-month survey. The percentage of non-smokers was consistent throughout the 12-month postpartum period with 87% of participants reporting no cigarette smoking at the 3-month survey and 88% at 12 months. The percentage of mothers employed part-time decreased from 51% at 3 months postpartum to 44% at the 12-month survey.
Significant predictors of breastfeeding/feeding pumped milk over the 12-month period were: prenatal infant feeding intention to breastfeed only, being a non-smoker, employed part-time, and higher perceived level of breastfeeding support in the workplace. Employed mothers who expressed prenatal feeding intentions to breastfeeding only were much more likely to have sustained breastfeeding during the study period (OR = 10.50, p < .001). Non-smoking employed mothers were more likely to breastfeed over the 12-month period compared with employed mothers who smoked (OR = 3.91, p < .001). Mothers employed part-time (compared with full-time) were more likely to continue breastfeeding over the follow-up period (OR = 1.97, p = .002). Employed mothers who perceived high levels of breastfeeding support in the workplace were more likely to have continued breastfeeding compared with those with low levels of perceived breastfeeding support in the workplace across the follow-up period (OR = 2.78, p < .001) (Table 3).
Generalized Linear Mixed Model to Determine Factors Associated With Breastfeeding Status Over Time (3, 6, 9, and 12 Months Postpartum) (n = 302)
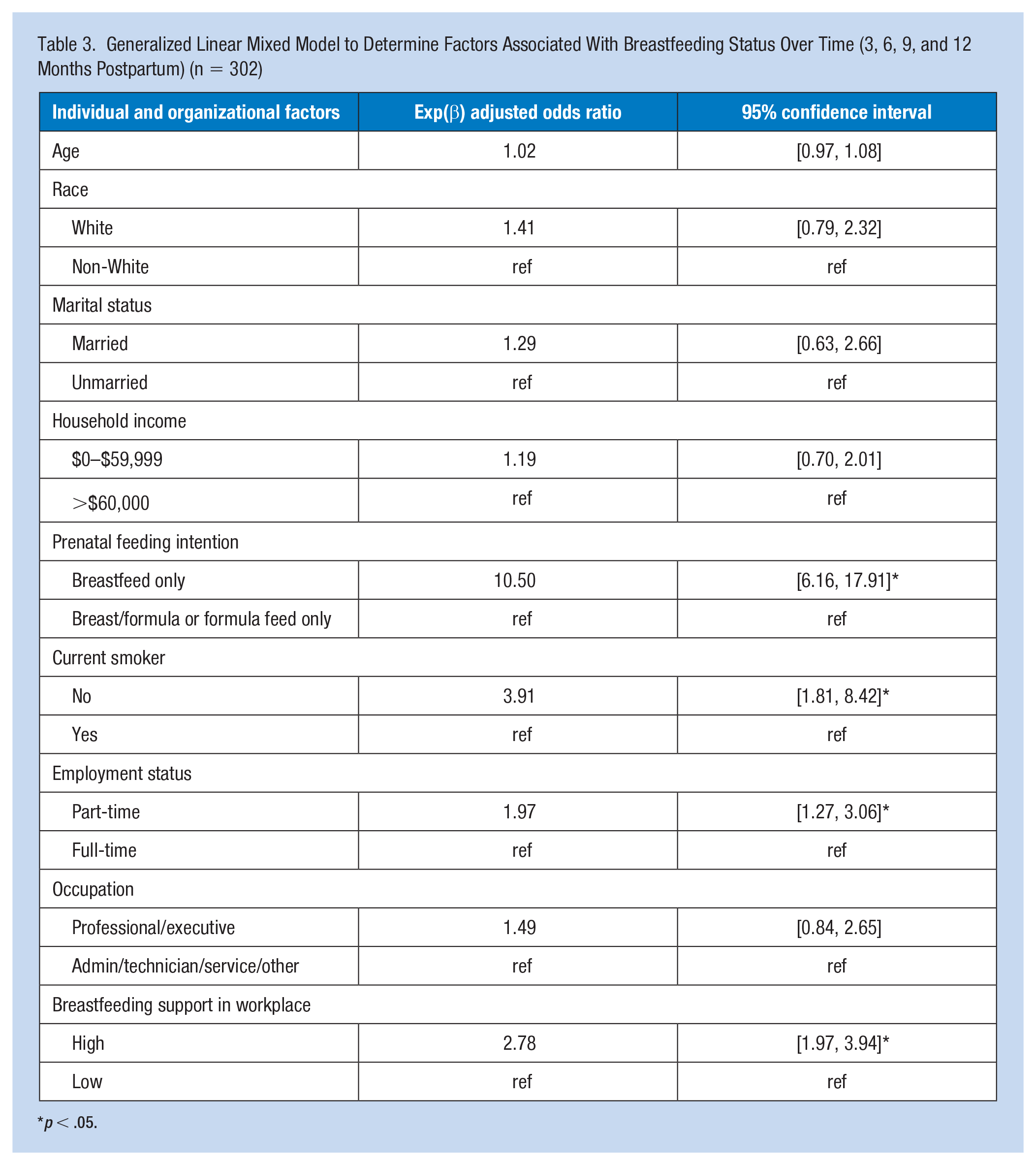
p < .05.
Discussion
Individual factors associated with breastfeeding/feeding pumped milk among employed mothers at all four time points were prenatal feeding intention to breastfeed only and smoking status, consistent with the hypothesis. Consistent with our findings, breastfeeding intention has been well established as a strong predictor of breastfeeding. Our results support similar findings that mothers who are non-smokers are more likely to initiate and continue breastfeeding/feeding pumped milk compared to mothers who smoke (Godleski et al., 2020).Smoking more than 10 cigarettes per day decreases milk production and alters the metabolic properties of milk composition, which may also contribute to the decreased rate of breastfeeding/feeding pumped milk in mothers who smoke (Macchi et al., 2021). Occupational health nurses and worksite wellness programs need to encourage working mothers regardless of smoking status to continue breastfeeding.
Occupation type was not a significant predictor of continued breastfeeding in the GLMM, which was not consistent with the hypothesis or previous literature on occupation type and breastfeeding practices. Mothers may have been able to navigate and overcome any barriers to continued breastfeeding encountered throughout the 12-month follow-up period. Whitley et al. (2021), in a study on work, race, and breastfeeding outcomes in mothers in the United States, found that mothers working in service occupations had the shortest breastfeeding duration compared with mothers who did not work outside of the home and mothers working in professional occupations. This study also demonstrated that women who reported higher levels of perceived support for breastfeeding in the workplace were more likely to breastfeed/feed pumped milk at all time points compared with mothers who reported a low level of perceived breastfeeding support in the workplace. In a recent systematic review of workplace environment interventions to facilitate breastfeeding in employed mothers, Vilar-Compte and colleagues (2021) reported that lactation support interventions in the workplace positively impact breastfeeding duration and reduce the introduction of breast milk substitutes such as formula. Key strategies to support and promote breastfeeding in employed mothers included a designated lactation space in the workplace, reasonable break time for milk expression, and organizational policies supportive of breastfeeding (Vilar-Compte et al., 2021).
When comparing characteristics of the cohort of mothers who participated in the IFPS II survey with current mothers, several differences were noted. According to the CDC (2022b), the percentage of babies receiving any breast milk at 3 months of age nationally in 2019 (69.1%) was higher than the percentage of babies receiving any breast milk at 3 months of age in this study (57%). Smoking during the prenatal period was lower with only 5.5% of women who gave in birth in 2020 reporting smoking cigarettes during the prenatal period compared with 14% in this study (CDC, 2022a). In 2021, 77.2% of mothers with children under age 6 worked full-time compared with only 46% of mothers who worked full-time in this study (U.S. Bureau of Labor Statistics, 2022b). Despite improvements in overall breastfeeding rates over the past 15 years, breastfeeding initiation and duration still fall behind national and global targets. Policies at the organizational, state, and federal level are needed to promote breastfeeding supportive workplace environments. Breastfeeding employees receive some protection at the federal level under the Patient Protection and Affordable Care Act (ACA), enacted in 2010 (U.S. Department of Labor, 2010). Under the ACA, the Fair Labor Standards Act and the new federal law (Break Time for Nursing Mothers Act) require employers to provide reasonable break time and a private, non-bathroom place for nursing mothers to express breast milk during the workday for 1 year after the child’s birth. While this law is a great step in the right direction for supporting the rights of breastfeeding mothers upon returning to work, issues with implementation, compliance, and enforcement may exist under the authority of local and state agencies. Recent passage of the Providing Urgent Maternal Protections for Mothers (PUMP) for Nursing Mothers Act may strengthen the Break Time law by providing additional breastfeeding accommodations for employed mothers (Maloney, 2021). Given the labor participation rate for women with children under the age of 6 has steadily increased over the last 50 years from 39.0% in 1945 to 65.6% in 2021, it is vital for federal laws promote breastfeeding in the workplace be enacted (U.S. Bureau of Labor Statistics, 2022a).
Given IFPS II data were collected between 2005 and 2007 (prior to implementation of the Break Time for Nursing Mothers’ Act in 2010 under the Affordable Care Act), findings may not be representative of the views of current breastfeeding mothers. In addition, workplace lactation programs, policies, and support for breastfeeding in the workplace may have changed over the past 18 years. The use of a consumer opinion panel as the recruitment method for the IFPS II sample may have led to selection bias. Lack of variability in race and marital status in the sample limits generalizability of the findings. In addition, with only 5% of the sample identifying as Hispanic, there was a lack of variability in ethnicity. Maternal self-report recall bias and social desirability bias were also limitations. The nine-item IFPS II Breastfeeding and Employment Scale was only administered to employed breastfeeding mothers, so we were unable to include this scale in the GLMM for comparison between employed mothers who breastfeed/fed pumped milk versus those who did not. In addition, the questionnaire was only available in English, limiting the representation of non-English speaking mothers in the study sample. Furthermore, the use of a one-item survey question to measure perceived breastfeeding support in the workplace may not accurately reflect the entire construct of workplace breastfeeding support. However, this one item was found to be moderately correlated with the IFPS II nine-item Breastfeeding and Employment Scale (Rho = −.50, p < .001). Finally, only factors at the individual and organizational levels were included in the model.
This study identified individual and organizational factors associated with breastfeeding practices in a subsample of employed mothers in the United States who participated in the IFPS II. Unlike the Mandal and colleagues’ study (2010), the study reported here included a variety of infant feeding practice data obtained during the prenatal and postpartum IFPS II surveys and used GLMM to analyze data at multiple time points. Additional research is needed to identify determinants of breastfeeding/feeding pumped milk in employed mothers beyond individual and organizational factors. Subsequent studies need to examine multi-level factors, including the interpersonal, community, and policy dimensions of the Socio-Ecological Model to better understand how interpersonal and environmental factors influence breastfeeding practices in employed mothers. Future research examining multi-level components of the Socio-Ecological Model is needed to better understand the complex processes involved in breastfeeding practices in the workplace. Study findings were congruent with published research findings that prenatal infant feeding intentions to breastfeed only, maternal non-smoking, part-time employment, and high levels of perceived breastfeeding support in the workplace predict breastfeeding/feeding pumped milk over time in employed mothers.
Implications for Occupational Health Nursing Practice
It is important to understand from the nursing mothers’ perspective, which individual, interpersonal, organizational, community, and policy-level factors influence breastfeeding practices in employed mothers. Occupational health can serve as advocates for breastfeeding employees as well as to serve as liaisons between employees and employers. Furthermore, occupational health nurses can provide employed breastfeeding mothers who smoke with evidence-based smoking cessation and reduction interventions including smoking as far away from the infant as possible, cutting back on the number of cigarettes smoked per day or quitting smoking including the use of cessation aids, and smoking after breastfeeding or pumping milk. Worksite wellness programs including smoking cessation and lactation support are critically important to provide a supportive environment for employed mothers.
In conclusion, occupational health nurses can assess and address barriers to breastfeeding in the workplace and advocate for continued breastfeeding in employed mothers consistent with national and international breastfeeding recommendations. Understanding the association between multi-level factors of workplace lactation support and breastfeeding practices in employed mothers is essential for the development, implementation, evaluation, and enforcement of workplace lactation programs and policies to improve maternal and child health outcomes.
Applying Research to Occupational Health Practice
Generalized linear mixed modeling (GLMM) revealed predictors of breastfeeding over time were individual factors of prenatal breastfeeding intention and non-smoking, and organizational factors of part-time employment and perceived support for breastfeeding in the workplace. Occupational health nurses can use the evidence from this study to address barriers to breastfeeding in the workplace, advocate for breastfeeding employees, as well as to serve as liaisons between employees and employers to promote continued breastfeeding in the workplace. In addition, occupational health nurses can assist in the development, implementation, evaluation, and enforcement of workplace programs and policies including access to a dedicated private location for direct feeding or milk expression, refrigeration space for milk storage, and reasonable break time for milk expression. Clear expectations and responsibilities of employers and employees are needed to provide a breastfeeding supportive workplace environment for all employed breastfeeding mothers.
Footnotes
Acknowledgements
The author thanks Ellen J. Hahn, PhD, RN, FAAN, and Mary Kay Rayens, PhD, for their assistance in preparing this article.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by CARERC through Grant 6T42OH010278. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIOSH/CDC.
Human Subjects Review
On February 23, 2022, the University of Kentucky Institutional Review Board determined that this author’s study did not require IRB review because the project used secondary data that were publicly available and not identifiable.