
Abstract
Exclusive breastfeeding is recommended for the first 6 months of life, and up to 1 year with complementary food. Breastfeeding rates have improved over the last 20 years, but exclusive breastfeeding, and breastfeeding to 6 months have not yet met Healthy People 2020 goals. Given that the majority of women return to work shortly after delivery, workplace support for breastfeeding could facilitate breastfeeding continuance. The Patient Protection and Affordable Care Act (ACA) was the first federal legislation to address breastfeeding in the workplace. This article examines employee breastfeeding behavior before and after implementation of workplace breastfeeding support policies and practices. Breastfeeding behavior change over time was assessed by comparing employees’ responses by age of their youngest children. Results indicated that breastfeeding among employees and breastfeeding after returning to work improved after initiation of breastfeeding support policies in this university setting.
The many benefits of breastfeeding have been well-established in current literature. Breast-fed infants have fewer clinic visits during the first year of life and fewer reported instances of otitis media, upper respiratory and urinary tract infections, and atopic diseases than bottle-fed infants (Dewey, Heinig, & Nommsen-Rivers, 1995). Breastfeeding provides a protective effect against the incidence of dental caries, and development of obesity and diabetes in later life (Arenz, Ruckerl, Koletzko, & von Kries, 2004). Evidence of enhanced cognitive development among breastfed infants is also emerging (Kramer et al., 2008). Benefits for breastfeeding women include protection against breast cancer, ovarian cancer and osteoporosis. A shorter return to prepregnancy weight has also been reported (Baker et al., 2008).
The unique protective immunological constituents of breast milk make it superior to all substitute feeding products, particularly when bottle feeding preparation or water sources are unsanitary. The dramatic protective benefits of exclusive breastfeeding on both infant mortality and morbidity rates in the third world, compared with the rates for bottle-fed infants, have been attributed to environmental conditions that render bottle feeding both unsanitary and unhealthy. In first world settings where better environmental conditions are likely, controlled trials conducted in Europe (Kramer et al., 2001) and the United States (Bonuck, Trombley, Freeman, & McKee, 2005) have demonstrated the benefits of breastfeeding in reducing gastrointestinal infection, atopic eczma, and otitis media.
Over time, breastfeeding rates in the United States have fluctuated to a low in the 1950s, increasing through the 1970s, decreasing slightly again in the 1990s, with an uptake in the 2000s. The 2016 ever breastfed rate is 81.1% (Centers for Disease Control and Prevention & National Center for Chronic Disease Prevention and Health Promotion, 2016). Women likely to breastfeed can generally be described as middle and upper income; some education after high school; Hispanic, non-Hispanic White, or Asian; nonsmoker; over age 30 years; and living in the west and northwest. Women less likely to breastfeed can generally be described as low income; smokers; no post-high-school education; non-Hispanic Black; less than age 30 years; and living in the south (Amir & Donath, 2007; Labbok, Wardlaw, Blanc, Clark, & Terreri, 2006; Singh, Kogan, & Dee, 2007).
It is well-documented that barriers to successful breastfeeding include embarrassment, lack of family, peer or other social support (Jones, Power, Queenan, & Schulkin, 2015), and lack of timely assistance when problems arise (Kaunonen, Hannula, & Tarkka, 2012). Health care providers’ knowledge of and coaching mothers about breastfeeding is not consistent across all sectors of the U.S. health care system, and access to lactation support can be limited (Busch, Logan, & Wilkinson, 2014). Economic pressure to return to work in both dual and single parent households, limited family leave time, and requirements of welfare-to-work have emerged as strong barriers to both initiation and duration of breastfeeding (Mills, 2009). The most recent data indicate that the lowest breastfeeding rates are among low-income women regardless of other demographic characteristics (Jiang, Foster, & Gibson-Davis, 2010). The underlying context of low-income and low socioeconomic status is emerging as the key barrier to breastfeeding.
Once initiated, the times when risk of weaning is greatest and therefore the times when support is most needed are immediately following a mother’s discharge from the hospital, and again when she returns to work or school (Ahluwalia, Morrow, & Hsia, 2005). Both limited paid maternity leave and the pressure to return to work present tremendous challenges to breastfeeding duration for even the most motivated mothers. It is possible that low-income women may experience these factors more often than women who earn higher incomes. It is clear from the evidence that when worksite wellness policies provide supportive environments (e.g., pumping room, facilities for storage, flexible hours, job sharing), more women continue breastfeeding when they return to work (Brown, Poag, & Kasprzycki, 2001). When established, workplace policies that address breastfeeding can result in prolonged breastfeeding duration (Johnston & Esposito, 2007).
The state of New York was the first to enact legislation that both protected and supported breastfeeding women. In 1984, legislation that exempted breastfeeding from existing indecency laws was passed. In 2002, the New York State Labor Law (Labor Law, Article 7, Section 206-c.) was amended (National Conference of State Legislatures, 2016), requiring employers to provide break time for breastfeeding women as well as make reasonable accommodations for women to breastfeed or express milk, and prohibited discrimination against women who chose to exercise these options in the workplace.
Subsequently, all 50 states have passed legislation that addresses breastfeeding in at least one of five ways: (a) providing space and break time for working women, (b) prohibiting discrimination against breastfeeding employees, (c) allowing breastfeeding in any public or private location, (d) exempting breastfeeding from public indecency laws, and (e) exempting breastfeeding women from jury duty (Nguyen & Hawkins, 2013). In March 2010, the Patient Protection and Affordable Care Act (ACA) became the first federal legislation to support breastfeeding in the workplace. The ACA requires that employers set aside break time and private space for breastfeeding women up to 1 year postpartum (Raju, 2014).
With this new emphasis on workplace accommodations for breastfeeding women, the Health Resources and Services Administration (HRSA) has provided employers with materials, training, and support to help them address newly passed federal and state labor laws. Their national campaign, Business Case for Breastfeeding (Office on Women’s Health, n.d.), provides human resource departments with materials and strategies for supporting breastfeeding women at the workplace.
It is in this context of changing labor laws and emphasis on supporting breastfeeding women in the workplace that Cornell University (CU) Career/Life Services in Human Resources explored breastfeeding support initiatives for University employees. This office secured grants and implemented programs to facilitate a supportive family-friendly breastfeeding atmosphere across campus. In addition, this office developed social networks for prenatal and breastfeeding women, prenatal education and postpartum breastfeeding support classes, and an extensive referral list of local community resources for university employees. These efforts were subsequently formalized into university policy. An interim policy on lactation and break time was published in January 2008, and finalized as CU Human Resource Policy 6.9 Lactation and Time Away from Work (CU, Human Resources, 2008) in June 2008.
The purpose of this study was to examine the influence of institutional policies on employee breastfeeding behavior. In particular, the researchers investigated whether the implementation of institutional polices influenced breastfeeding among low wage workers, and how this policy affected the likelihood that employees would continue to breastfeed when they returned to work.
Method
The Cornell Child Grant Subsidy Program (CCGSP) was established in 2001 to assist parents with child care challenges. Employees with a household income up to US$150,000 are eligible for grants to spend on any legal child care for children up to age 13 years. In 2009, US$1,660,000 was awarded to 882 employee families for child care support.
The CCGSP developed an extensive staff survey to assess the impact of the grant program on potential changes in the quality of child care purchased with grant funds and associated employee satisfaction. Data on family size, number and age of children, child care practices, and parent demographics were collected. The author added questions regarding breastfeeding behavior to this survey, thereby providing an opportunity to assess the breastfeeding practices of employees. “When your youngest child was an infant, did you/your partner breastfeed”? and “Did you or your spouse breastfeed after returning to work (BFRW)?”
All Cornell employees with at least one dependent child age 12 or younger were sent the questionnaire through the employee electronic mail system (email) in February 2009. The survey was administered by Survey Research Institute (SRI), an independent survey research firm. The initial correspondence was followed by reminder emails to nonrespondents. Data collection ended in March 2009. A total of 1,047 staff members completed the survey of a possible 2,564 employees; the response rate was 40.8%. Incomplete surveys, those with no response to the breastfeeding questions, were eliminated, leaving a pool of 919 (35.82% of the total possible and 87.77% of completed and returned surveys).
Independent Variables
Demographic and work-related variables were considered independent variables and captured on the survey described below.
Demographic variables
The survey included seven categories of annual household income: less than or equal to US$20,000, more than US$20,000 to US$40,000, more than US$40,000 to US$60,000, more than US$60,000 to US$85,000, more than US$85,000 to US$100,000, more than US$100,000 to US$150,000, and more than US$150,000. The lowest two categories were combined for incomes up to US$40,000. Respondents self-identified race by the following categories: White, Black, Hispanic, Asian, and American Indian. These categories were collapsed to White, Black, and Other, given the low number of Hispanic, Asian, and American Indian staff in the respondent pool. Marital status was ascertained using three response categories: married, single, and domestic partnership. Respondents who chose “domestic partnership” were combined with the married category for analysis. The four categories of education included: high school or less, some college, college degree, and graduate training or degree. Participants identified their sex. The respondents were divided into two groups based on the age of their youngest children: recent group had children less than 36 months of age, and distant group had children 3 years and older.
Work-related variables
Respondents were asked to rate the flexibility of their work schedule to manage or balance work and caretaker responsibilities. The five categories of flexibility were as follows: none, very little, some flexibility, as much as I need, more than I need. “None” and “very little” were combined into one category representing the lowest level of flexibility. “As much as I need” and “more than I need” were combined for analysis to represent the most flexibility. The five categories for position type included the following: staff hourly, staff salaried, postdoctorate, academic/nonfaculty and academic faculty. Academic nonfaculty and postdoctorate categories were combined for analysis as the nature of work performed by both are similar, and the distinction between these two types of employees was not meaningful. Twenty “unit” choices indicated affiliation with schools and colleges, service units and administrative offices. Colleges and schools included College of Agriculture and Life Sciences (CALS), Arts and Sciences, Architecture, Engineering, Hotel Administration, Human Ecology, Industrial and Labor Relations (ILR), Johnson Business School, Law School, and Veterinary Medicine.
Given the small number of employees and the contiguous location on the same university quad, Architecture was combined with Arts and Sciences, and the Law, Johnson, Hotel, and ILR Schools were combined, based on similar small numbers of staff, and situated in relatively close proximity on campus. The remaining schools were treated as stand-alone units.
The service units and administrative offices included Academic Programs and Institutes, Academic Support Services, Office of Human Resources, Office of Information Technology, Planning and Budget, President-Direct Reports, Provost-Direct Reports, Student and Academic Services-Direct Reports, University Communications, Alumni Affairs and Development, Campus and Business Services, Financial Affairs, Comptroller, Research and Advanced Studies, Risk Management and Public Safety, Chief Financial Officer-Direct Reports, Facilities Services, University Library System, and Gannet Health Clinic. These administrative units were grouped into three categories: (a) Library and Health, (b) Facilities Services Group, and (c) Administrative Group (i.e., staff supporting the business functions of the university). These staff are more likely to be office bound, work 9 to 5 office hours and be connected to administrative policies versus the unique policies of a single college. A total of nine units were used in the analysis of Distant group data. Given the small number of respondents in the Recent group, units were collapsed into three groups for analysis. The units were designated by letter in the data tables to protect the confidentiality of respondents who could be identified as pregnant during the study period.
An opportunity to respond to any child or elder care concern was included at the end of the survey: If you have ideas on how CU could help you manage work, elder care, and child care responsibilities, please share them. Qualitative data in response to this statement were reviewed for relevance to breastfeeding behaviors and practices after employees’ return to work.
Data Analysis
The data, codebook, summary statistics by survey question, and text of open-ended questions were prepared by SRI and provided to the principal investigator for analysis. Data analysis was conducted using JMP 10.0.0 (SAS Inc., Clary, North Carolina). Statistical significance was set at p < .05. Dependent outcomes of interest were breastfeeding (yes or no) and breastfeeding after returning to work (yes or no). A chi-square test of independence was used to test the associations between characteristics of employee groups and the outcomes.
To assess changes in employee breastfeeding practices over time, two employee groups were created based on the age of the last biological child. Children’s age groups were created based on parent selection of age categories listed on the survey: Infant (0-17 months), Toddler (18-36 months), Preschool/Pre-Kindergarten (3-5 years), and School Age (5-12 years). The Distant group was created by combining the older children identified as Preschool/Pre-Kindergarten and School Age; the Recent group was created by combining Infants and Toddlers.
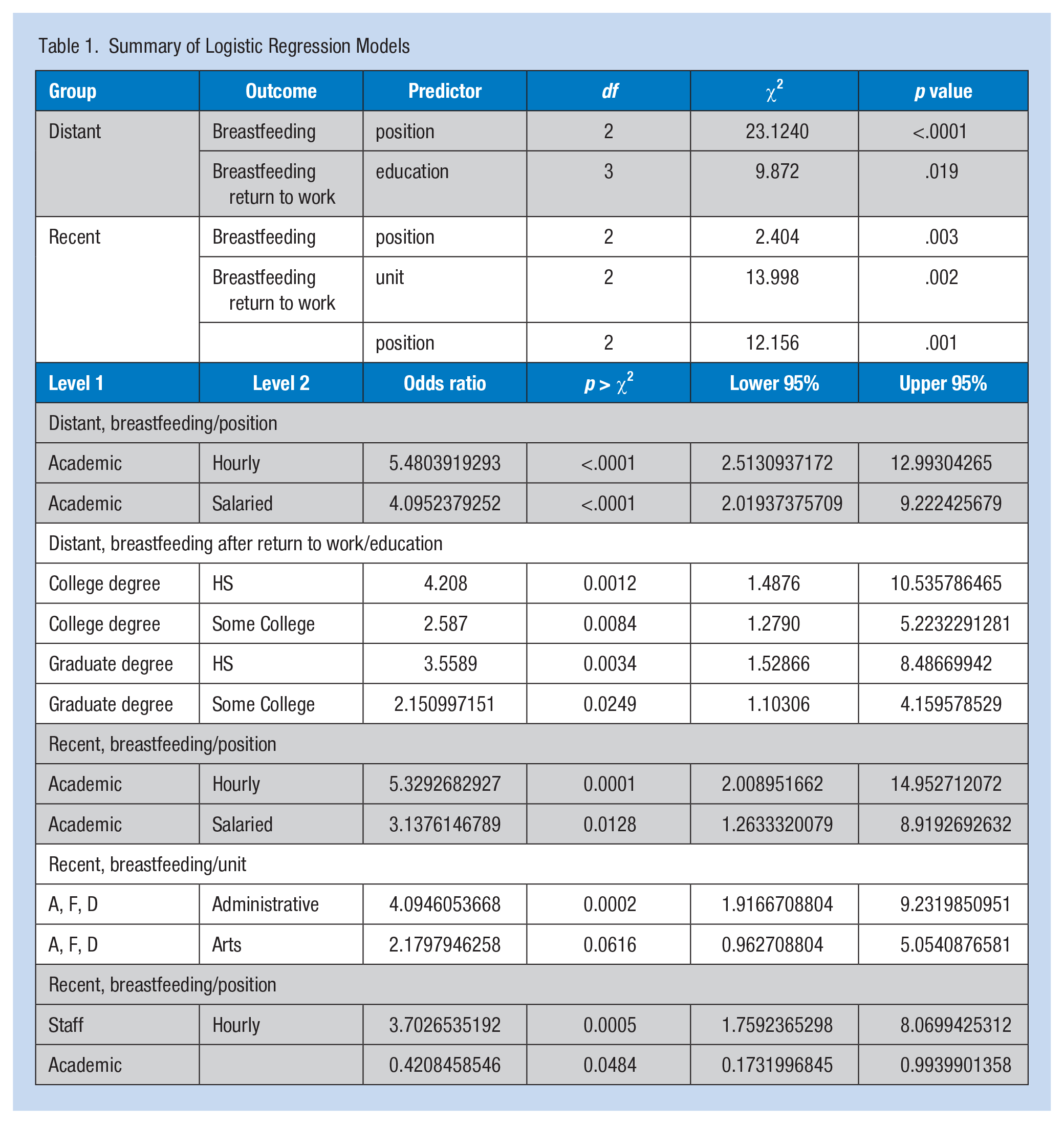
Multiple logistic regression analyses were conducted to examine the predictors of the two breastfeeding behaviors: breastfeeding and breastfeeding after return to work in Distant and Recent groups separately. The multiple logistic regression analysis was run for the Distant group with all independent variables that were significantly (p < .05) associated with the outcomes in the preliminary bivariate analyses for breastfeeding (i.e., education, marital status, income, position, unit). The process was repeated for the Distant group for breastfeeding after returning to work (i.e., education, position). Similar analyses were completed for the Recent group for breastfeeding (i.e., education, position, unit) and breastfeeding upon returning to work (i.e., position, unit). Independent variables having a statistically significant impact on breastfeeding that remained in the models are shown in Table 1. A multiple regression model was run combining both birth cohort groups. The results are displayed in Table 6. Review of written responses to the open-ended questions at the end of the survey was completed to assess emergent themes.
Summary of Logistic Regression Models
Results
Table 2 shows the frequency distributions for each of the characteristics of the Ithaca campus sample responding to the survey by whether they or their partners breast-fed their youngest child. Overall, breastfeeding was significantly (p < .05) associated with education, marital status, position, race, and unit as described in more detail below.
Employee Characteristics by Infant Feeding Choice for Their Most Recent Child (N = 963)
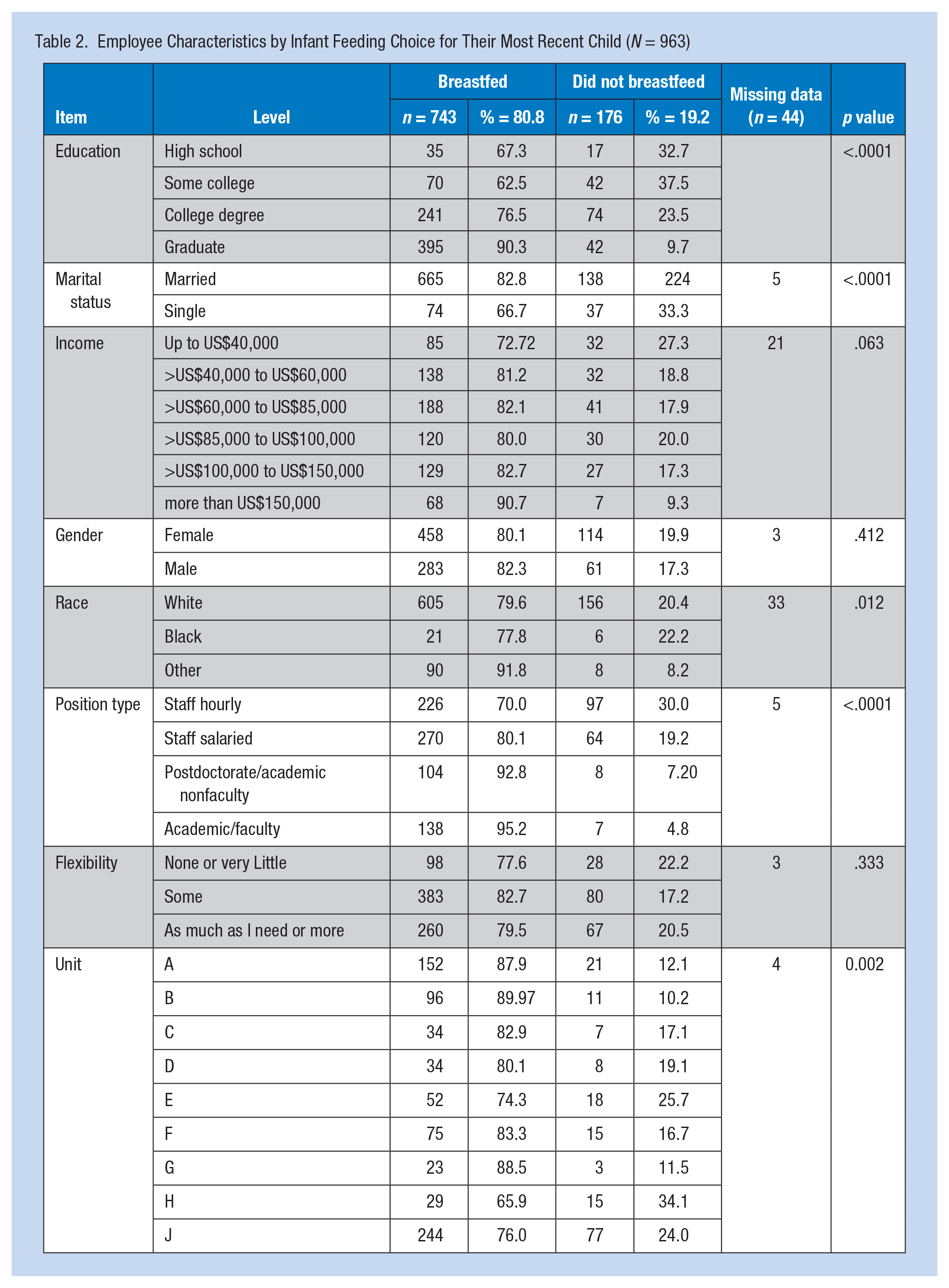
All respondents had at least one child under 12 years of age; 80.8% breastfed their last child. Breastfeeding was more common (90.7%) among the highest income group, and less common among the lowest income group (72.7%). Breastfeeding among the remaining income groups was virtually the same (80%-82.7%).
Little difference was found in breastfeeding rates based on the sex of the respondent employee: female (80.1%), or male (82.3%). Very few single employees (10.5%) responded to the survey compared with those reporting married or domestic partnership statuses. Single respondents were significantly less likely to breastfeed (8.1% vs. 66.7%).
As might be expected, the sample was highly educated: 47.7% had earned graduate degrees, 34.3% college degrees, 12.2% had attended college, and 5.6% had completed high school. Breastfeeding rates increased significantly with education.
Staff with hourly positions breastfed considerably less than those with salaried or academic positions: 70% versus 95.2%. Breastfeeding was lowest among the facilities group (65.9%) compared with all other work units.
Breastfeeding was lowest among Black employees compared with all other racial groups. The Other group was small but consisted of a large proportion of Asian staff who breastfed at the highest rate.
In summary, breastfeeding was associated with higher education, marriage, higher income, academic position versus hourly position, and work unit compared with those who did not breastfeed. Employee gender and job flexibility did not distinguish those who breastfed from those who did not breastfeed.
Distant and Recent Groups
Respondents were divided into two groups for analysis based on the age of their last or youngest children to detect any changes in breastfeeding behavior over time. Respondents with toddlers and preschoolers (children up to 36 months) were labeled “Recent.” Respondents whose youngest children were 3 years and older were labeled “Distant.” This division was necessary to distinguish between employees with “Recent” infant care and breastfeeding experience from those whose breastfeeding experiences could be up to 11 years prior to the survey, and not necessarily associated with employment at Cornell.
Characteristics of the Distant group (Table 3) included 77.3% breastfed their last child and breastfeeding was significantly (p < .05) associated with education, marital status, income, race, position type and unit, as described below. Breastfeeding increased as income increased, from 70.5% in the lowest to 92% in the highest income groups. Similarly, breastfeeding rates increased with increasing education. The majority of the Distant group was married (82%), and 79.4% of married respondents breastfed their last children.
Characteristics of Employees Whose Last Child Was Born More Than 36 Months Ago (Distant) by Infant Feeding Choice (N = 579)
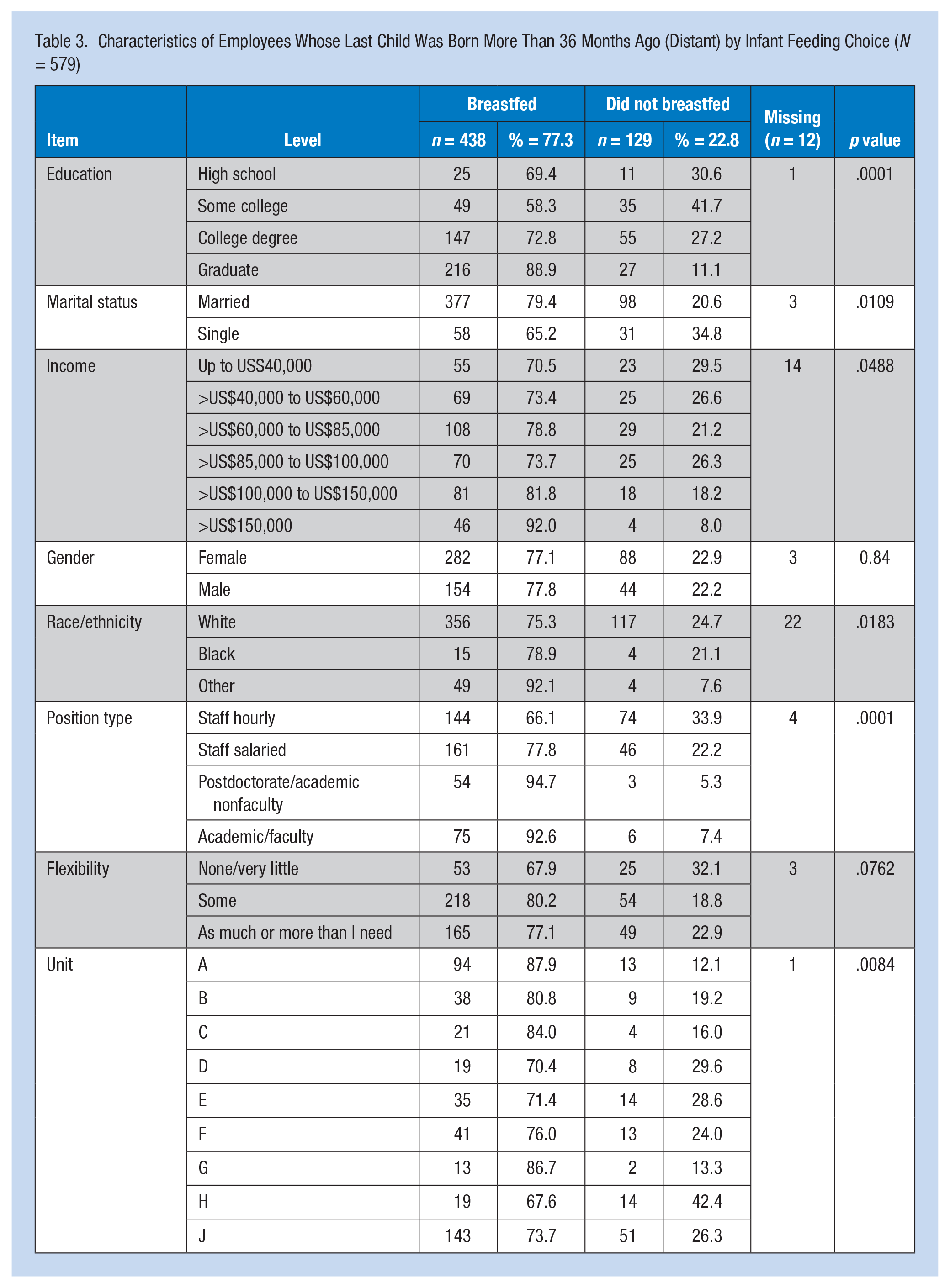
The Distant group was predominantly White (85%). Breastfeeding was lowest among Whites (75.3%), and highest among “Others” (92.1%). Breastfeeding was highest among Unit A respondents at 87.9%, and lowest among the Unit H group at 67.7%. The profile of breastfeeding respondents in the Distant group by breastfeeding status after returning to work is listed in Table 4; of these respondents, 71.3% breastfed after returning to work. Those infants who were breastfed after the parent returned to work were significantly more likely to have a graduate degree compared with a high school diploma, and have academic faculty versus hourly positions.
Characteristics of Employees Whose Last Child Was Born More than 36 Months Ago (Distant), Who Continued to Breastfeed After Returning to Work
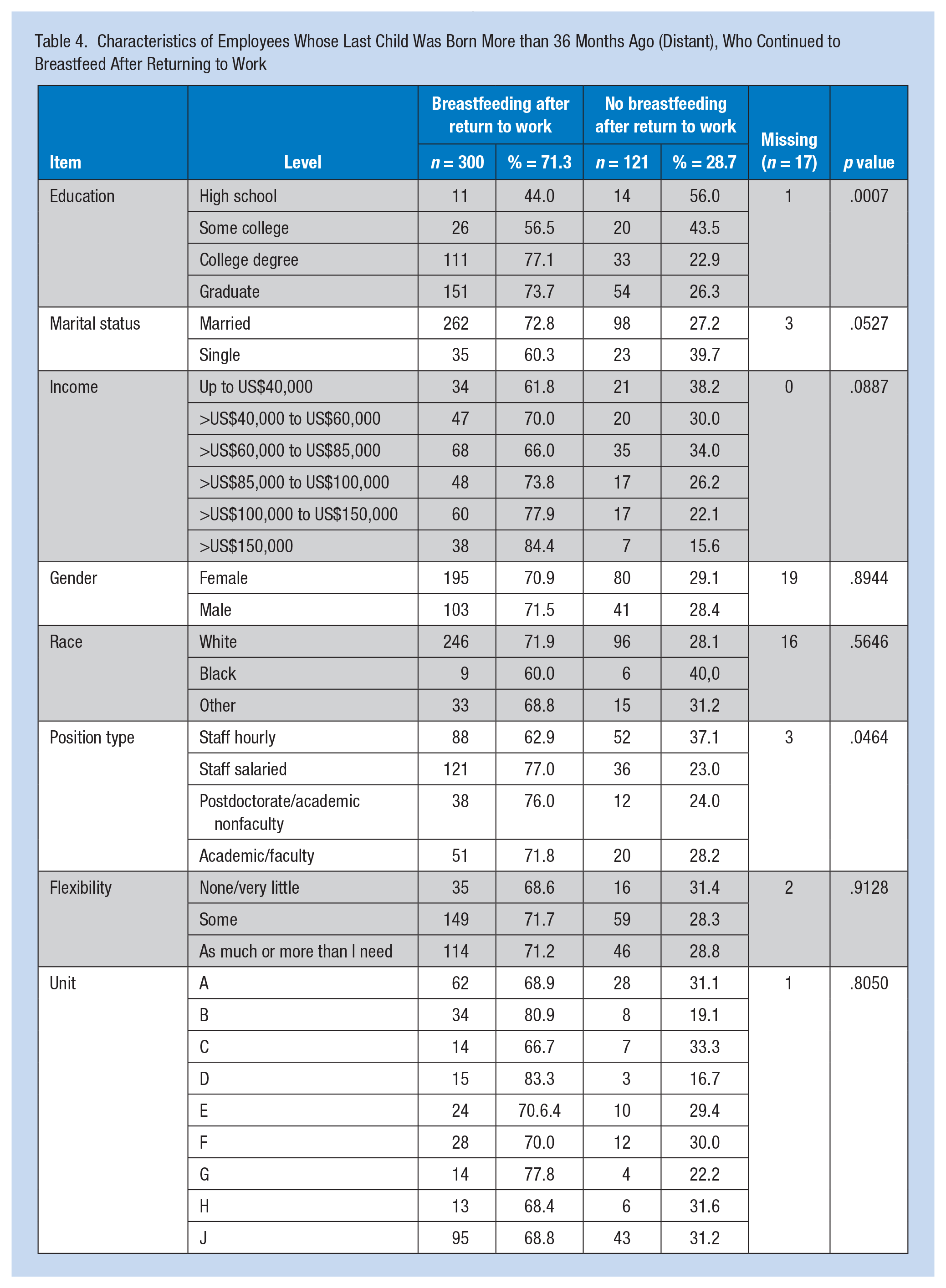
Among the Distant group, education, marital status, race, income, position type, and unit were positively associated with breastfeeding behavior. For the group of Distant employees that continued to BFRW (Table 4), education and position type were significantly associated with continuing to BFRW. Multiple logistic regression was run with significant variables. Position was a significant predictor of breastfeeding, and education remained as a predictor of BFRW.
Characteristics of the Recent group are shown in Table 5 by breastfeeding choice: 86.6% of the Recent group breastfed their last children. Breastfeeding increased significantly with increasing education from 62.5% for those having earned a high school diploma to 92.3% for those parents with graduate degrees.
Characteristics of Employees Whose Last Child Is Less Than 36 Months Old (Recent) by Infant Feeding Choice (N = 362)
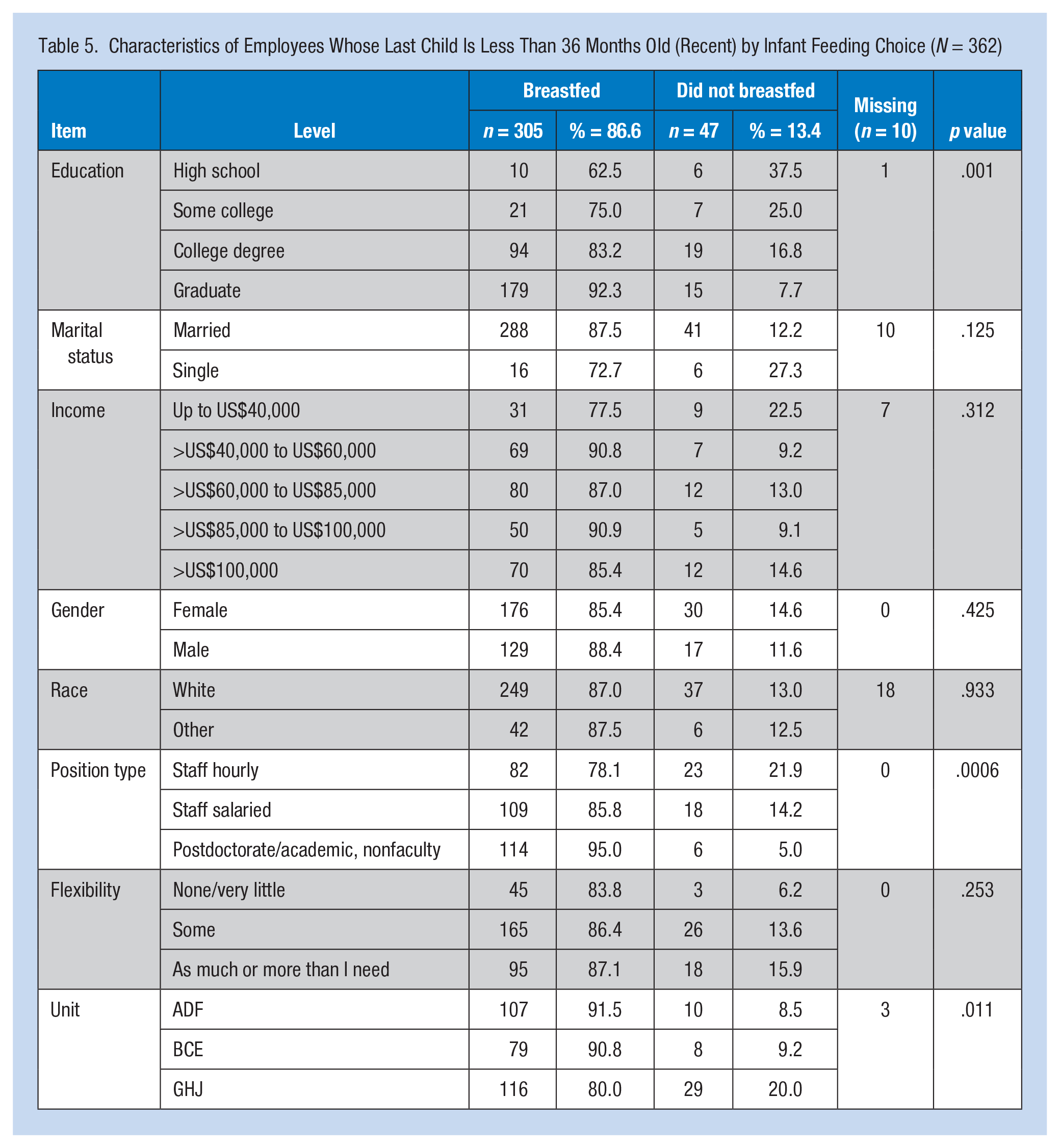
Breastfeeding was significantly associated with position type. It was lowest among those employees with hourly positions (78.1%) and highest among those with academic faculty positions (98.1%). Breastfeeding initiation was similar across the three job flexibility responses. Breastfeeding was highest among Unit D respondents (100%), and lowest among Unit J (71.4%).
Characteristics of the Recent group who breastfed after returning to work are listed in Table 6. Among this group, 78.6% continued to BFRW. Breast-feeding practices were similar across racial groups. Breastfeeding rates were not significantly associated with income. Breastfeeding was significantly associated with position type, lowest among hourly employees. Breastfeeding was not significantly associated with job flexibility, but varied; breastfeeding was lowest among those employees with very little or no flexibility (65.9%) and highest among those employees with the most flexibility (81.3%).
Characteristics of Employees Whose Last Child Is Less Than 36 Months Old (Recent) Who Continued to Breastfeed After Returning to Work (N = 305)
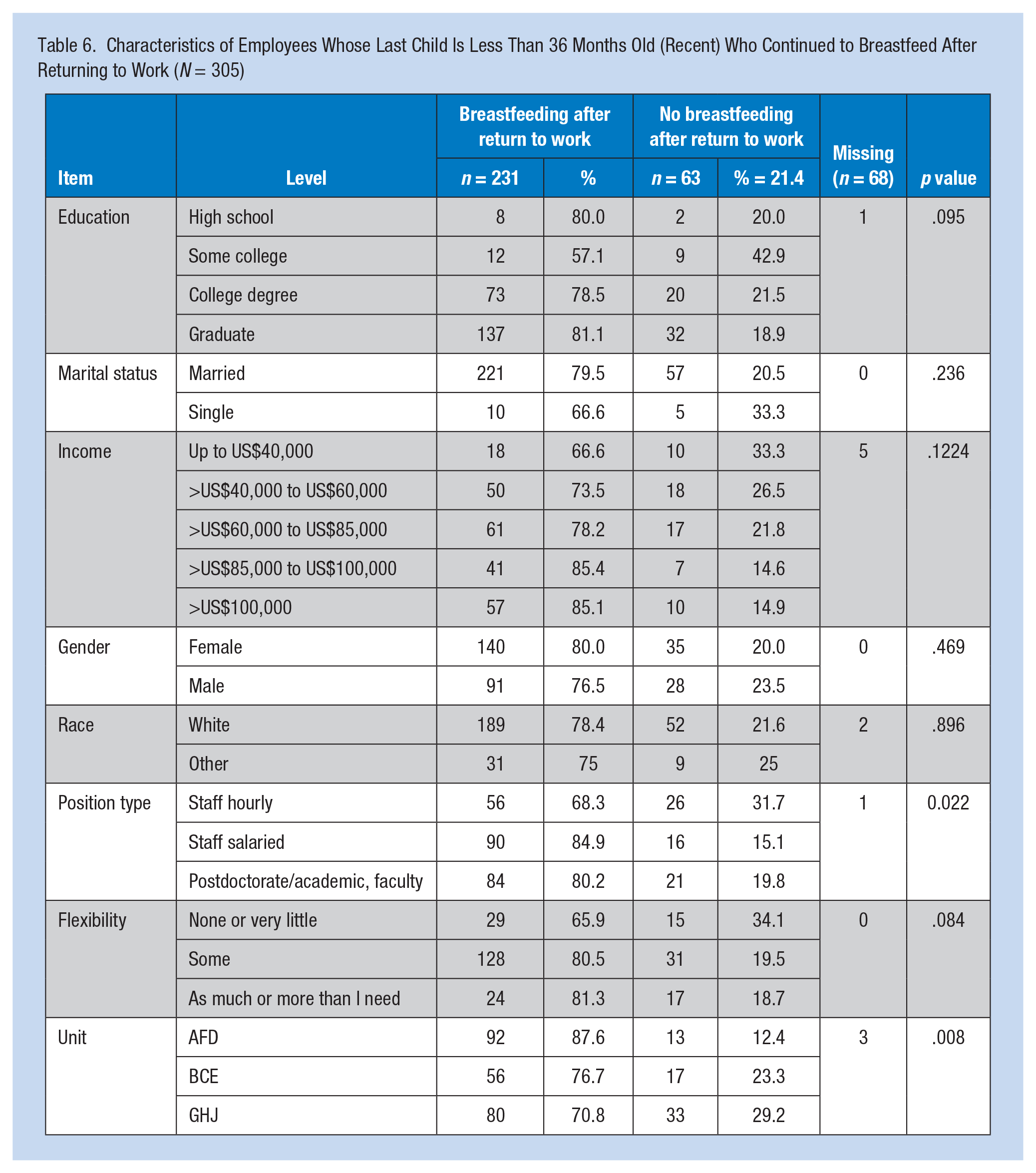
Among the Recent group, no differences in breastfeeding were found by marital status, race, income, or flexibility of their positions. Education, position type, and unit were the only independent variables associated with breastfeeding. Among the Recent group, only position type and unit were significantly associated with breastfeeding upon returning to work. Among units, Unit H was significantly different from all others. Based on separate multiple regression on the recent group, position was a predictor of breastfeeding, unit and position were predictors of BFRW.
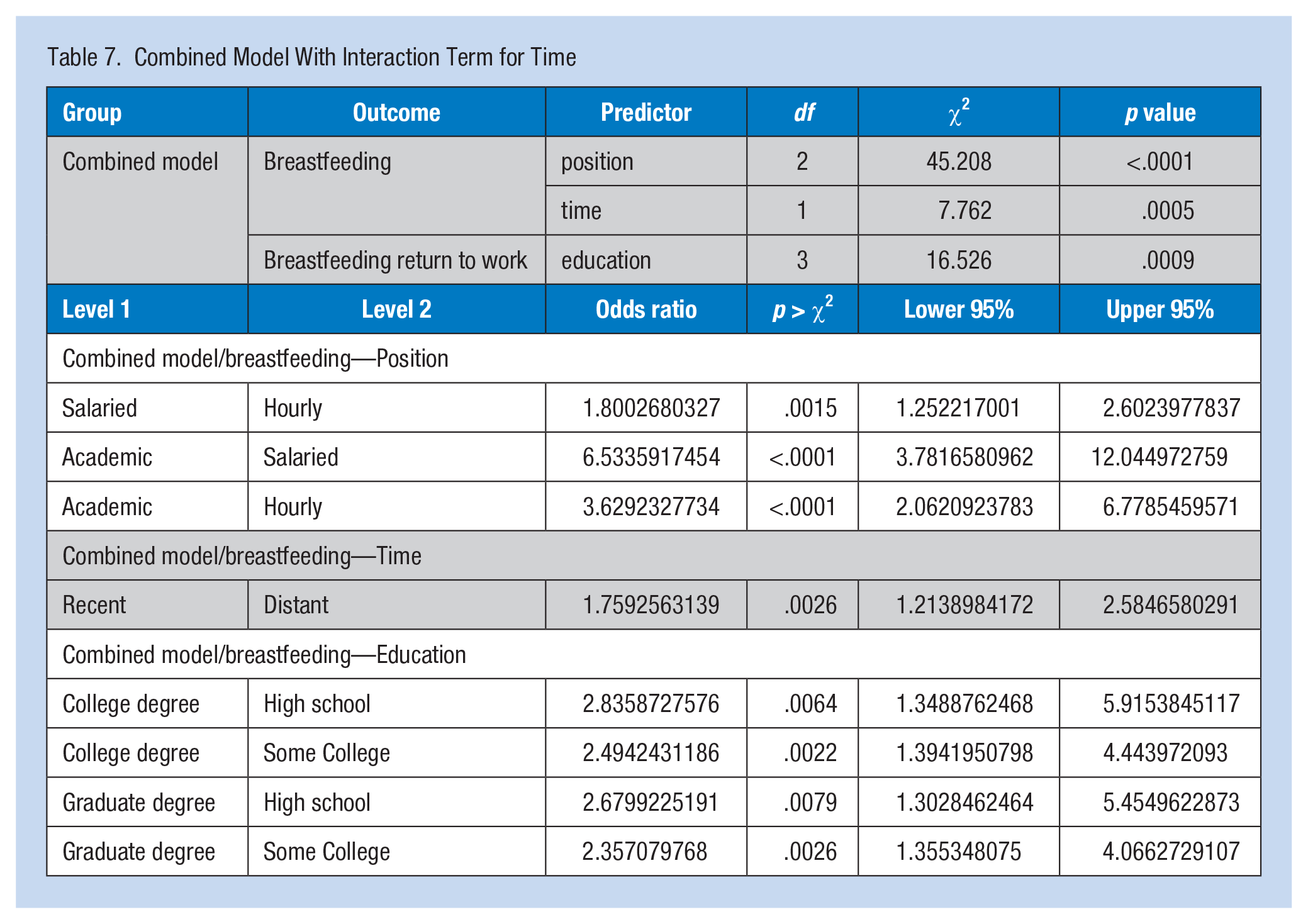
In the combined regression model for breastfeeding, position and the time associated term remained significant. The effect of job position on breastfeeding did not depend on time. In the combined model for breastfeeding on return to work, education was the only significant predictor of breastfeeding (Table 7).
Combined Model With Interaction Term for Time
Comments of Survey Respondents
An open-ended question at the end of the survey invited respondents to add any other comments on any aspect of work life and family concerns: “If you have ideas on how Cornell University could help you manage with elder care and child care responsibilities, please share.” Forty individuals mentioned breastfeeding; of these, seven comments were not directly relevant and included such responses as: my spouse actually breastfed and I adopted my child and did not breastfeed. The remaining 33 comments were made by 31 women who breastfed their last child (39.3% Distant, 60.6% Recent) and breastfed after returning to work; and two women who did not breastfeed their last child. The comments were grouped into categories related to structural challenges to breastfeeding (child care, parking, pumping rooms), influence of colleagues (supervisors and coworkers), and comments on the University policy (Table 8).
Qualitative Comments
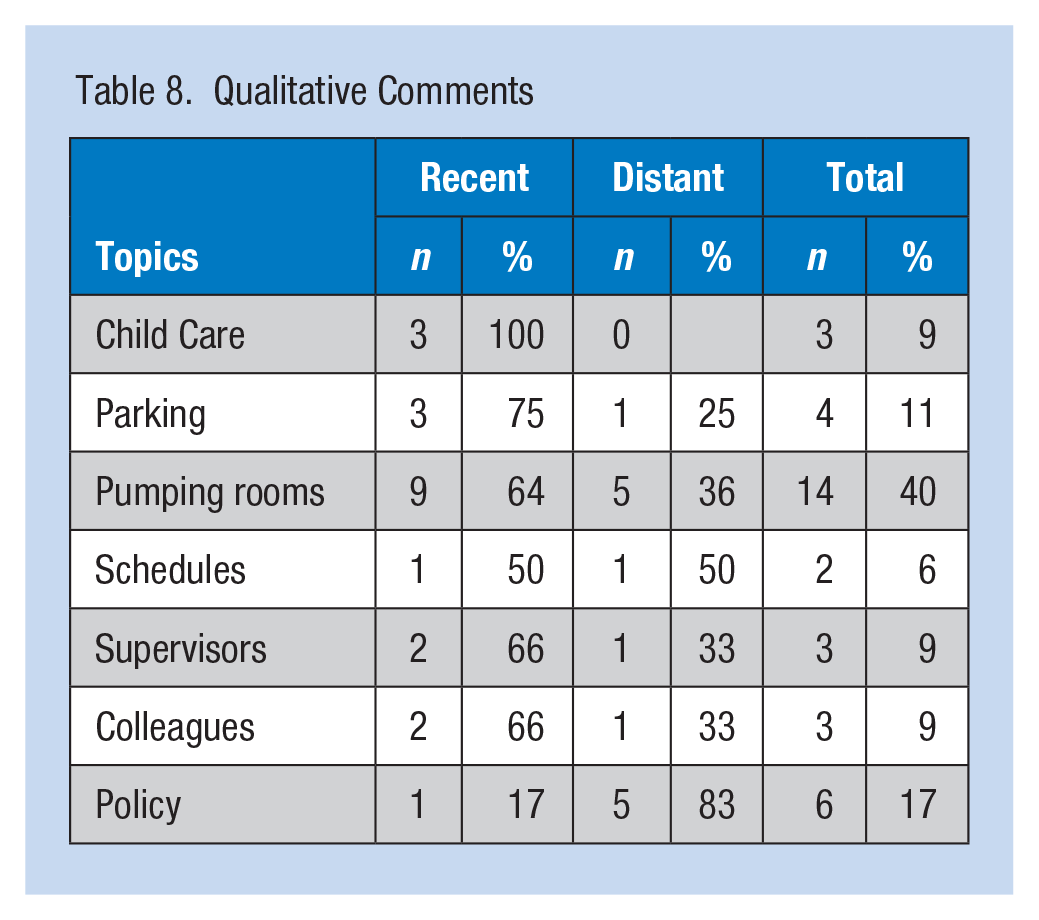
Practical concerns and considerations of working parents dominated the responses. More comments addressed issues with pumping rooms than any other topic. Examples are below:
Lactation rooms should be easier to access and remain unlocked. When I returned to work there was no lactation room for privacy. It was very uncomfortable to express milk in front of students. Lactation rooms are a must! Please continue to offer the child care grant, promote workplace flexibility, and preserve the lactation rooms (I pumped in a storage room . . . private, but not comfortable or conducive to long-term use).
Lack of convenient parking to facilitate timely trips home or to child care locations during lunch or other breaks was described as a barrier to breastfeeding.
It would be very helpful to dedicate some parking spots to primary care parents of infants (or give a handicap permit to breastfeeding mothers of infants). When my children were infants, I often had to leave work for short periods of time to nurse/pump . . . I would have trouble finding a parking spot on my return and hence these absences would be very costly on my already limited time at work. When I was breastfeeding, I paid for a J-lot permit so I could run home all the time to breastfeed. I think it would have been nice to have had some kind of arrangement that allowed me to do that more easily. Women who live far away will just not breastfeed, which is a real problem for the health of their infants. I am very disappointed with parking while I am breastfeeding. I commute 2 days a week from Canandaigua to BEEBE Hall. Thankfully, I get to work from home 3 days a week. At any rate, when I went to see what my options were for parking and pumping, I was told that the only thing I could do was pay 180 dollars UP FRONT and then I would get a temp pass to park near work. I just returned from maternity leave and could not afford this. There is no bus that goes ANYWHERE near my building and I have to walk from A LOT with my breast pump, and several other bags that I use for transporting my work back and forth from home. I feel that Cornell should be more respectful of moms who are breastfeeding and parking. I would have gladly paid the money as I have paid for parking in the past, out of my paycheck, but that was not an option.
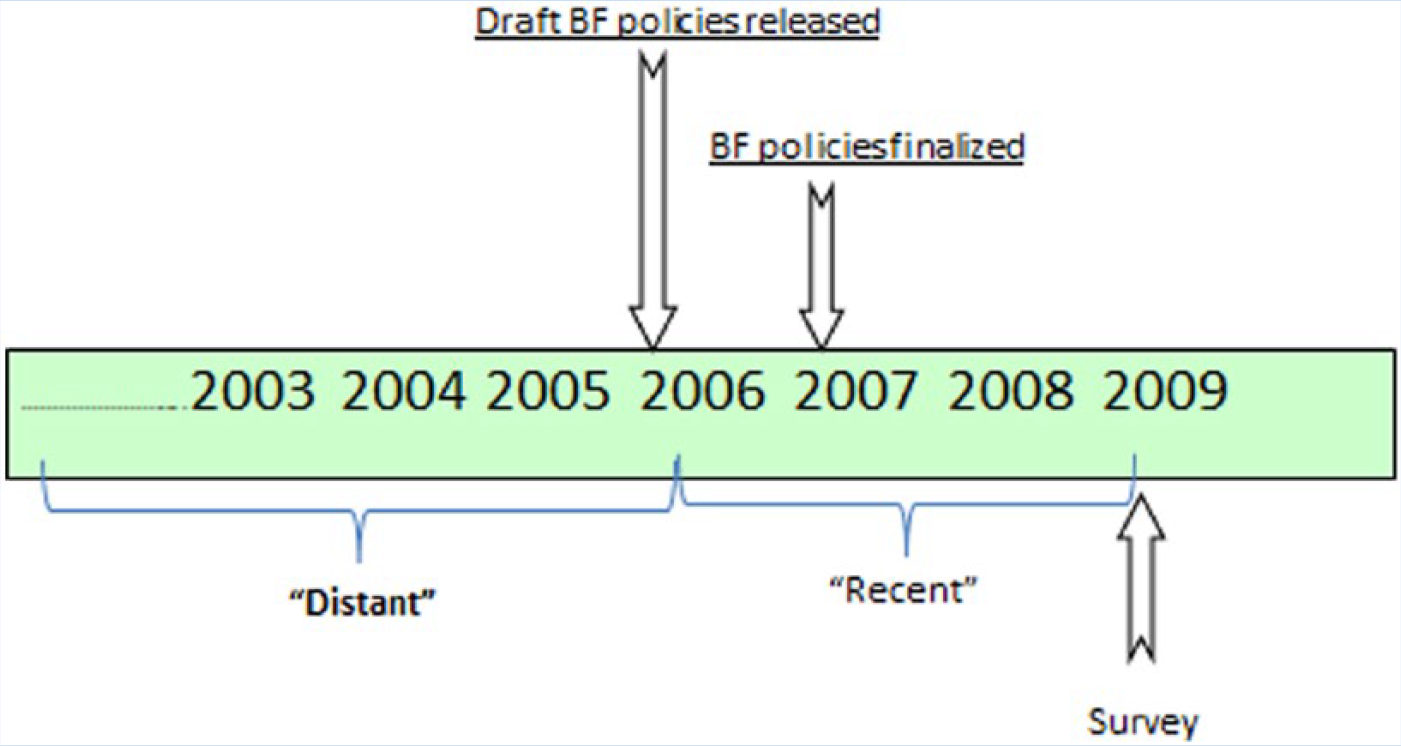
Timeline depicting policy implementation, survey distribution, and age groupings.
Two commented on scheduling: one was extremely positive; the other was highly critical regarding allowances for extended breaks and more frequent breaks.
For me, breastfeeding would have been too difficult because of my work schedule. I would have liked for it to have been easier. There was no one telling me I had rights and what to do, so I didn’t breastfeed. My office allows me to work at home and to have a flexible part-time (4.5 hours/day) schedule, so I was free to pump as much as I needed. I was able to continue to exclusively breastfeed twins until they were 1 year old. That is entirely due to the fact that I had an extremely flexible schedule and the privacy needed to pump (and a child care provider that was willing to work with me). Also, my managers relieved me from evening and overnight job responsibilities so that I could breastfeed my children.
There was feedback regarding insensitive comments made by coworkers, highlighting the need for more information sharing regarding university policies and breastfeeding rights.
Might be nice to have a support network for faculty moms of babies—we get some heat because our dinosaur colleagues assume that having a baby means we are “not serious” about science. I think it is helpful for you to know that many of our colleagues who are single, childless and not in a position to care for their elders resent these important initiatives. I’ve maintained a modest schedule for breast milk pumping, and was completely shocked when a colleague challenged my right to do so. Fortunately, my supervisor supports this. I guess it would be helpful for (The University) to continue publicizing the value of these initiatives. Thank you so very much for the progress with the lactation rooms. I hope information about them has become standard when employees inquire about maternity benefits. I still hear too many women say it would be too hard to continue breastfeeding when they return. I know it’s a very personal choice, and I think more outspokenness on Cornell’s part could be influential. I really benefited from the HR series on breastfeeding, I highly valued attending. I would welcome any additional sessions on balancing work and motherhood, parenting, and related topics.
Discussion
The creation of a supportive work environment is an integral part of the Career/Life Services mission. Establishing breastfeeding rooms for pumping became part of their strategy in 2005 to support working mothers. The first rooms were established in the University’s main administrative building, Day Hall; and in the School of Veterinary Medicine. At the time of the survey, 14 breastfeeding rooms were available across campus. Some were part of an existing lavatory as in Day Hall; others were uniquely designed for the needs of breastfeeding mothers as building renovations or new construction was planned. In addition, orientation of all new university staff by Career/Life Services includes information regarding work flexibility options and the responsibility of supervisors in facilitating employee requests for breastfeeding accommodations.
The creation of two employee groups, based on the age of the individual’s last child, was necessary to detect changes in breastfeeding behavior over time. The Recent group represented the breastfeeding experience of staff with children born 0 to 36 months prior to the survey. Development of the draft and posting of the final University breastfeeding policies occurred during this time period.
Over time, a positive trend in breastfeeding practices and behavior and the continuation of breastfeeding upon return to work was clearly demonstrated in the data set. The breastfeeding rate for the entire respondent group (80%), the Distant group (78%) and the Recent group (87%) surpasses the Surgeon General’s Healthy People 2010 target for breastfeeding initiation of 75%. The 2009 national rate for ever breastfed was 73.9%, the New York state rate was 76.4% (https://www.cdc.gov/breastfeeding/data/reportcard.htm); the respondent sample exceeded these rates as well. The increase in breastfeeding rate displayed by the Recent group above the Distant group (+ 9.35%), is greater than any improvements found during the same time period in national or state rates (+2% change). For example, the Recent group breastfeeding rate is higher than the rate reported in Tompkins County in 2009 (82%). Breastfeeding after returning to work was 71.3% for the Distant versus 78.6% for the Recent group. However, no comparable data for the county, region, or state on the rate of breastfeeding among women returning to work was available. Finally, differences in breastfeeding behavior by race and income levels disappeared in the Recent group.
According to national data, a “typical” breastfeeding mother has a middle to upper income, is White and married, and has some college education (Office of the Surgeon General, Centers for Disease Control and Prevention, & Office on Women’s Health, 2011). Conversely, women who choose not to breastfeed are more likely to be non-Hispanic Black, with low income, unmarried, and with less than a high school education. National data also indicate that low wage workers do not continue to BFRW due to the nature of their positions (Grummer-Strawn & Shealy, 2009). Workers earning a higher wage are far more likely to have greater flexibility and therefore, greater opportunities to continue to BFRW (Mills, 2009). The difference in breastfeeding behavior typically predicted from demographic descriptors disappeared after implementation of workplace breastfeeding support policies as evidenced in the Recent group.
Differences in breastfeeding remained after implementation of workplace breastfeeding policies when examined by position type. Position type may embody characteristics of the job situation that are not mitigated by policy changes. This finding could be a reflection of the demands of hourly workers whose positions are part-time and inherently have time sensitive tasks during work hours; for example, breaks are not required for those employees who work less than 4 hours. Likewise, the environment of most academic appointments (private offices, support staff, independent nature of work assignments) provides a positive advantage for academic staff who are breastfeeding.
Surprisingly, flexibility was not a significant work factor for either group. Employees from both groups reported a fairly high level of flexibility regardless of other factors. This high rating could be a manifestation of the supportive family-friendly work environment that has garnered the university so much recognition and awards, and may explain why this factor was not significant.
Unit or work location was a significant factor for the Recent group only. This finding could be the result of uneven policy implementation, staff turnover, supervisor training, and the ability of supervisors to offer support. The resourcefulness of individual supervisors to accommodate staff requests may also be at play. The following comments from staff shed light on the individual accommodations made in their work locations:
My supervisors are incredibly supportive and continue to do their best to provide me with private places to pump but not having an officially designated area is stressful. Fortunately, my office found a place for me to pump that was within the building; if I’d had to pack up my things and walk several blocks to a Designated Pumping Station, I would have been far less likely to continue breastfeeding. Encouraging individual building managers to find little spaces (doesn’t take much) would be a good idea, even though I appreciate the existence of pumping stations.
Suggestions for improving additional structural barriers to breastfeeding were provided. The distance and time involved in walking to and from assigned parking lots, limited short-term parking for dropping off and picking up passengers, and very few short-term parking spaces for women to use if going home during the day were mentioned as barriers. The limited number of pumping rooms, and rooms that did not lock were additional concerns. Even when pointing out barriers, respondent comments were predominantly positive: thanking administration for setting aside space, even if not ideal space for pumping.
Study Limitations
Several limitations may have affected study results. First, all of the data were self-reported. Second, the child age categories used to create employee groups were not discreet. Third, the experiences of employees in the Distant group could be up to 11 years prior to implementation of the survey. Respondents’ memories of prior events could be subject to their interpretations and not verifiable through other sources. Fourth, no recorded information on length or exclusivity of breastfeeding was available which could have affected data accuracy. A respondent’s interpretation of “breastfeeding” can also vary dramatically, from exclusive breastfeeding to feeding from the breast once a day. Fifth, no data were available on the hospitals where these women delivered which could influence breastfeeding initiation. The length of maternity leave was not determined, which has been shown to influence breastfeeding duration and exclusivity. The length of employment was also not ascertained and may have affected employee comfort with policies and supervisors. Secular factors, not explored in this study, could also have influenced breastfeeding initiation and duration. Health care provider, health department and lay group activities, and mass media campaigns could have affected responses. Finally, the data only allow examination of associations, not cause and effect.
Implications for Occupational Health Nurses
Given the number of working women of childbearing age in the workforce, employer supports for family health are imperative if this segment of the workforce is to remain productive. Occupational and environmental health nurses are critical advocates for the health of all employees. Ensuring current breastfeeding policies are understood and implemented, and reinforcing the health benefits of breastfeeding for women and infants when new policies are being considered is an additional strategy for advocating for family-friendly workplace policies.
Conclusion
The introduction of institutional policies for breastfeeding, and training to increase supervisors’ awareness of the need for such accommodations is an essential step in creating a family-friendly work environment. Many institutional changes were realized during the 36 months prior to the survey, including changes in university policies, supervisor training, staff orientation, and establishment of breastfeeding support groups.
The influence of institutional supports for breastfeeding was assessed by grouping employee data by the age of their youngest children. It appears that employees’ patterns for initiating breastfeeding and then continuing to BFRW have improved over time. The data on the Recent group versus the Distant group indicate higher breastfeeding rates overall and higher rates of breastfeeding after returning to work. This finding indicates that the efforts of Career/Life Services to institute family-friendly policies which include breastfeeding-specific support strategies have had a positive influence on employees’ breastfeeding behavior.
Although these data were self-reported, an increase in breastfeeding overall and an increase in the number of employees who continued to BFRW is both positive and encouraging. Still, additional work is warranted to better understand the relationships between employer policies regarding breastfeeding at the workplace and employees’ breastfeeding choices.
Applying Research to Practice
Limited paid maternity leave and pressure to return to work present tremendous challenges to breastfeeding for even the most motivated women. Where established, workplace polices that address employee needs result in longer breastfeeding duration. Workplace breastfeeding policies, coupled with education of all employees and reinforced by supervisors, have potential to improve the health and well-being of employees and their children. Although women working at all levels of an organization benefit when a supportive atmosphere is fostered, low wage and hourly workers may benefit most.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Joan D. Paddock is a senior extension associate in the Division of Nutritional Sciences, Cornell University.