
Abstract
Background: The transition into shift work represents a critical and challenging time point in a nurse’s career. The purpose of this study was to describe nursing students’ sleep patterns and perceptions of safe practice during their first semester of clinical rotations. Method: Repeated measures pertaining to the sleep patterns of 19 full-time junior undergraduate nursing students were measured before, during, and after their first clinical rotations. Sleep was measured using wrist activity monitors and sleep diaries for seven consecutive days at each time period. Students’ “self-efficacy” or belief in their ability to provide safe practice was measured for (a) patient care (preventing adverse events to patients) and (b) occupational health (preventing occupational injuries to themselves) using Bandura’s self-efficacy scales. Associations between students’ sleep, sleepiness, and their perceptions of safe practice were explored. Results: Nursing students’ self-efficacy scores regarding patient care (preventing adverse events) improved across the three time periods (from 80% before clinical rotation, to 84% during clinical rotation, to 87% after clinical rotation). Although lower overall, students’ self-efficacy scores regarding occupational health (preventing occupational injuries to themselves) also improved across the three time periods (from 71% before clinical rotation, to 76% during clinical rotation, to 77% after clinical rotation). Furthermore, increased sleepiness significantly predicted lower self-efficacy scores for both patient care and occupational health. Conclusion/Application to Practice: Sleepiness can impair nursing students’ confidence in their ability to practice safely.
Introduction
Shift work and associated sleep loss can impair cognitive performance; promote workplace accidents, such as needle sticks, and errors, such as medication miscalculation; and degrade long-term health (Satterfield & Van Dongen, 2013; Williamson & Lombardi, 2011). Within the health care system, between 24% and 45% of nurses report sleep disturbances (Waage et al., 2014) that have been associated with patient medication errors and occupational health risks for nursing staff (Asaoka et al, 2013; Rogers, 2008; Shao, Chou, Yeh, & Tzeng, 2010). A considerable body of research has focused on the relationship between sleep, shift work, and long-term health outcomes in practicing nurses. An example is the Nurses’ Health Study that began in 1976 with an initial focus on cancer, in which more than 238,000 U.S. nurses had participated (Hankinson, 2015). Findings from this study revealed associations between night shift work and multiple risks for chronic disease such as obesity, cancer, hypertension, and cardiovascular mortality (Gangwisch, Feskanich, Malaspina, Shen, & Forman, 2013; Gu et al., 2015; Ramin et al., 2015).
Occupational health studies addressing sleep and safe practice around patient care provide a complementary perspective to those addressing health risks to nurses. For example, a study on nursing error rates found that night shift nurses were over 40% more likely to make errors than day shift nurses (Niu et al., 2013). Given that medical errors are currently the third leading cause of death in the United States, sleep restriction and fatigue among nurses are clearly of major concern, so much so that the American Nursing Association (ANA, 2014) has stressed the importance of reducing fatigue and sleepiness in nurses to help address this national problem. Similarly, The Joint Commission—a U.S.-based, independent, health care accrediting organization that focuses on enhancing quality of care and patient safety—identified drowsiness, fatigue, and sleep deprivation as hazards for both patient safety and health care workers’ personal safety and well-being (The Joint Commission Sentinel Event Alert, 2011). There is compelling evidence that health risks to both workers and patients increase when nurses’ sleep patterns are outside the norm.
Although the risks of sleep restriction and fatigue for nurses and their patients have been a topic of great interest, very little research has focused on nursing students as they prepare to face the rigors of the health care workforce. More than 150,000 new nursing graduates join the U.S. workforce each year (Health Services and Resources Administration, 2015). This workforce has approximately 2.9 million workers and serves a critical function in the health care system and society at large (Hankinson, 2015). During their education, nursing students make an abrupt transition from traditional classes into clinical rotations and shift work, a challenging time where fears of medical errors and adverse patient events abound. Qualitative research has shown that nursing students fear being negligent, administering incorrect medications, or mislabeling something (Noland & Carmack, 2014). Another qualitative study exploring nursing students’ fears as they transitioned to the workforce found that their anxiety about making mistakes impaired their ability to sleep, resulting in a negative spiral of stress, sleep disturbance, and more stress (Postma, Tuell, James, Graves, & Butterfield, 2017). Postma and colleagues reported the following quotations from nursing students who characterized this cycle: “. . . I think for a lot of us it felt like drinking out of a fire hose. . . Then that adds to the isolation, and the anxiety, and—the stress. . . and then you don’t sleep” (p. 3); “You may fall asleep, but then you’re sleeping, and then all of a sudden, you’re like—You’re having a dream that you’re just messing up something in clinical, which I’ve done” (p. 3).
Despite some qualitative research on this topic, the extent to which nursing students’ sleep affects their ability to provide safe clinical practice is unknown. Quantitative associations among sleep, sleep problems, and safe practice in student nurses have yet to be fully explored. The goal of this study was to address this gap in the research literature by monitoring nursing students’ sleep patterns (quantity and quality) and sleepiness during their first semester of day and night shift clinical rotations, a critical juncture in their professional development. During this same time frame, we also measured students’ safe-practice self-efficacy (both for patient care and for occupational health) to investigate associations between sleep, sleepiness, and confidence in their ability to provide safe patient care.
Method
Study Design
Using a repeated measures design, the sleep quantity and quality of 19 full-time nursing students were monitored before, during, and after their first clinical rotations in the second semester of their junior year. Sleep quantity (calculated based on minutes of sleep per 24 hours) and quality (calculated based on degree of movement during sleep) were measured objectively using wrist activity monitors (actigraphy), and sleepiness was measured using sleep diaries for seven consecutive days at each time period. During these same time periods, perceptions of patient care safe practice (preventing adverse events to patients) and occupational health safe practice (preventing occupational injuries to self) were measured using Bandura’s self-efficacy scales.
Theoretical Framework
Social ecological theory formed the foundation for the research; key concepts were organized according to the Ecological Model of Disaster Management, a nested systems model developed by Beaton, Butterfield and colleagues to frame different levels of organizational response during public health emergencies (Beaton et al., 2008). This model informed the study due to its focus on the individual within the organizational context, making it a holistic way to view nursing students’ occupational health and subsequent patient care consequences. For the current study, the model was adapted to focus on levels of concepts addressing student health (e.g., sleep patterns), student attributes (e.g., household situation influencing sleep patterns), organizations (e.g., university, hospital), and organizational attributes (e.g., shift expectations). This adaptation of the model focused on personal and organizational antecedents of safe nursing practices. In this case, safe-practice self-efficacy in patient care (preventing adverse events to patients) and occupational health (preventing occupational injuries to themselves) was used as a proxy for safe clinical practice
Participants
A convenience sample of 19 nursing students were recruited into the study. Inclusion criteria were full-time student status and assigned to clinical rotations as part of their junior year. The clinical rotations were designed to expose students to shift work and allow them to gain valuable insight into the nursing workforce. Clinical rotations included three shifts per week, and shifts ranged from 6 to 8 hours. Students were assigned to day, evening, or night shifts. Some students remained on the same shift throughout their clinical rotations, and others experienced more than one shift type. Recruitment procedures included providing a 10-minute in-class briefing to junior year students, as well as posting fliers and social media alerts. Students were assured that decisions to participate (or not) would in no way affect their grades or academic standing. No members of the research team were in a teaching or evaluation role for junior year students. The study was approved by the Washington State University’s Internal Review Board (IRB) prior to participant recruitment.
Study Measures and Procedures
Data were collected for seven consecutive days at three time points: Week 1 of the semester (prior to clinical rotations), Week 7 of the semester (during rotations), and Week 14 of the semester (following rotations, but prior to final exams). Thus, the data collection period took place over the course of 14 weeks. The primary study measure/independent variables were sleep quantity, sleep quality, and subjective sleepiness. Sleep quantity and quality were measured physiologically using wrist actigraphy, specifically using the Readiband V3™ actigraph by Fatigue Science. Actigraphy has been validated for the estimation of sleep quantity and quality across age groups (Driller, McQuillan, & O’Donnell, 2016). Actigraphy data were scored as “sleep” when the algorithms detect minimal activity over a period of time. Data are recorded for each day the Readiband is worn and are represented as a graph from midnight to midnight. The software converted these data into information about sleep through the use of scientifically validated algorithms. The more activity recorded, the lower the quantity and quality of sleep during that time. Sleep quantity was expressed as minutes of sleep across a 24-hour period. Sleep quality was expressed as a percentage that was calculated as the inverse of the percentage of movement recorded during sleep. For example, if 25% of a participant’s sleep was disturbed through movement, their sleep quality measurement for that night would be 75% that was not disturbed. We further calculated the average sleep quantity (minutes of sleep) and quality (percentage undisturbed sleep) over the seven-night period at each time point (prior, during, and after clinical rotations). Clinical comparison of Readiband sleep scoring versus polysomnographic sleep scoring indicated an accuracy rate of 92% (de Souza et al., 2003). Students were instructed to keep the actigraph on for the seven consecutive days during each data collection period. These devices are waterproof and Food and Drug Administration (FDA) approved for research use in hospital settings.
Subjective sleepiness was measured via sleep diaries that participants filled out for the seven consecutive days of each study measurement period. Subjective sleepiness was measured by asking students whether (on average) they felt sleepy or alert throughout the day. Additional questions were asked in the sleep diaries such as the following: “What time did you go to bed?” “How long did it take you to fall asleep?” “How many times did you wake up in the night?” “What time did you wake up?” Although this information was all collected with a greater degree of reliability from wrist actigraphy, these data were important for instances when wrist actigraphy data were incomplete (e.g., due to lack of compliance wearing the Readiband). 1 Student health, student context (e.g., whether they slept with a bed partner), organization, and organizational context data (e.g., housing situation, children, evening vs. night shift) associated with sleep were also collected.
The primary outcome measure was safe-practice self-efficacy. This concept was measured by having students indicate (on a scale from 0 to 100, where 0 = cannot do at all, 50 = moderately certain I can do, and 100 = highly certain I can do) the degree of confidence they had in (a) safe patient care (preventing adverse events to patients) and (b) occupational health (preventing injuries to themselves). In total, 24 items were included. Fifteen of these addressed patient care (e.g., “administer injections”) and nine addressed occupational health (e.g., “use safe lifting practices”). Scores were converted to percentages (maximum 100%) for ease of interpretation. We did not select a cutoff point to determine “confident” versus “not confident” in ability to provide safe practice. The research team has previous experience using Bandura’s (2001) Guide for Constructing Self-Efficacy Scales, and the 24 items we selected were based on those developed by Ryan and colleagues (2013). Internal reliability for these items is high (Cronbach’s α = .94 for patient care self-efficacy items and .83 for occupational health self-efficacy items). Students were e-mailed the safe-practice self-efficacy scales to complete each day.
Analytical Approach
Descriptive statistics (means and standard deviations for continuous variables, sample sizes, and frequencies for categorical variables) were examined. Sleep quantity (minutes of sleep per 24 hours), sleep quality (expressed as a percentage of time in bed actually sleeping, based on actigraphy algorithms measuring movement during sleep), and subjective sleepiness (measured by sleep diary responses) were then tested for their ability to predict students’ self-efficacy (expressed as a percentage from 0% to 100%) addressing (a) adverse events involving patients and (b) occupational injuries to themselves. Student context (e.g., sleeping with a bed partner) and organizational context (e.g., shift type) were also examined in the model. Generalized linear multilevel modeling (MLM) with fixed effects was used to account for repeated observations across participants overtime to reduce the likelihood of a Type I error and to account for potential clustering of data. This statistical technique provides equivalent output to a linear regression analysis, while estimating fixed effects to account for the possible violation of the assumption of independence among data points. Significance levels were set at .05. SPSS 24.0.0.0 software was used for all analyses.
Results
Table 1 depicts that in our sample of 19 students, most of them were female (84%) and Caucasian (95%). The average age of students was 25 years (range = 19-44 years), 16% were married, and 11% lived with children in the home.
Demographic Characteristics of the Nursing Student Sample (N = 19)
Table 2 shows that, overall, student sleep quantity and quality (measured by actigraphy) did not vary greatly across the data collection periods. During the first round of data collection (prior to clinical rotation), students received on average 427 minutes (SD = 8.4 minutes) or 7.1 hours of sleep per 24 hours, and their average sleep quality was 85% (range = 69%-98%). During the second round of data collection (during clinical rotations), students received on average 434 minutes (SD = 7.0 minutes) or 7.2 hours of sleep per 24 hours, and their average sleep quality (percentage of undisturbed sleep) was 86% (range = 72%-98%). During the third round of data collection (after clinical rotation, but prior to finals), students received on average 423 minutes (SD = 8.6 minutes) or 7.1 hours of sleep per 24 hours, and their average sleep quality was 85% (range = 70%-95%).
Patient Care and Occupational Health Self-Efficacy Across Time 1 (Preclinical Rotation), Time 2 (During-Clinical Rotation), and Time 3 (Postclinical Rotation)
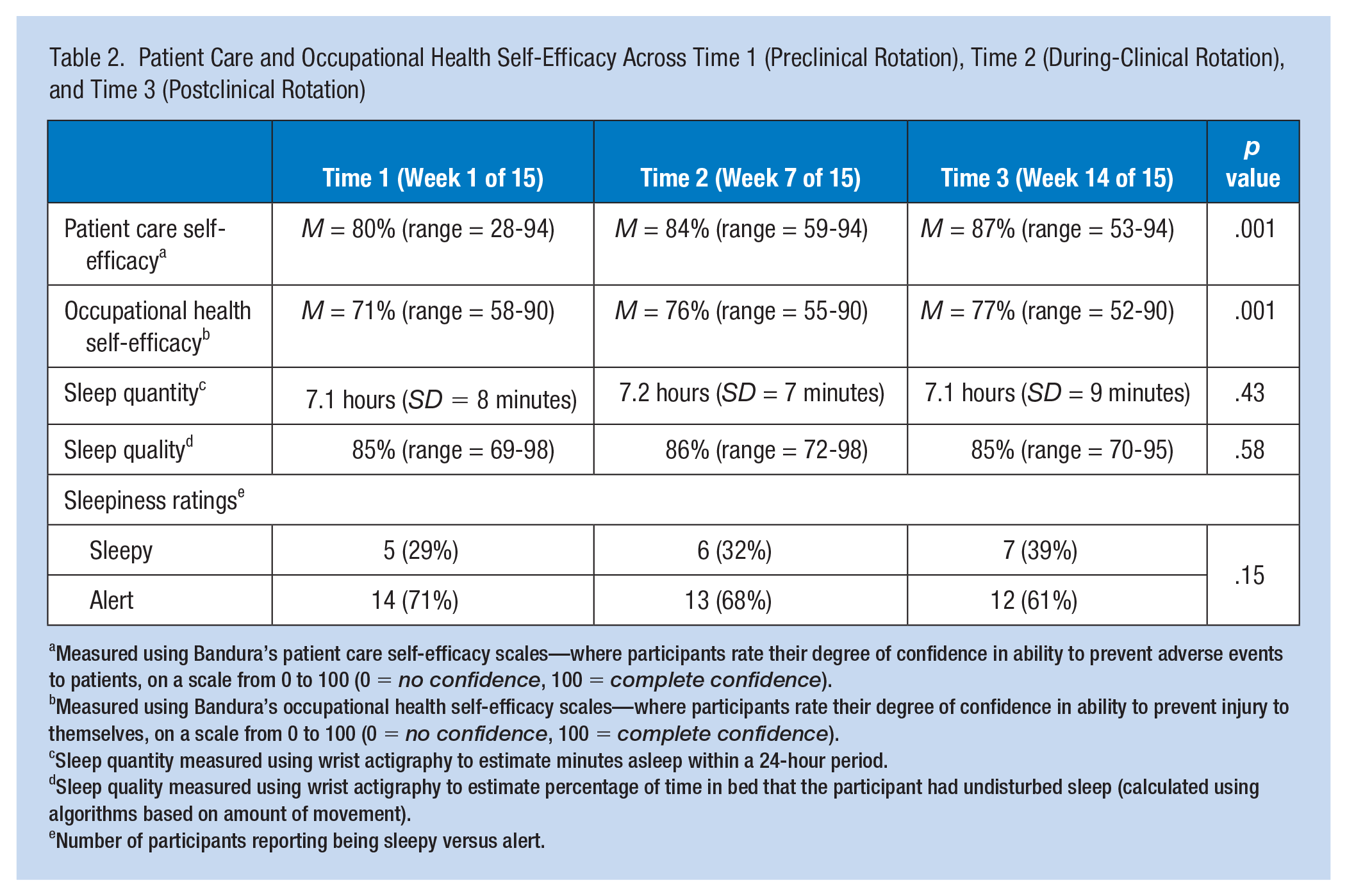
Measured using Bandura’s patient care self-efficacy scales—where participants rate their degree of confidence in ability to prevent adverse events to patients, on a scale from 0 to 100 (0 = no confidence, 100 = complete confidence).
Measured using Bandura’s occupational health self-efficacy scales—where participants rate their degree of confidence in ability to prevent injury to themselves, on a scale from 0 to 100 (0 = no confidence, 100 = complete confidence).
Sleep quantity measured using wrist actigraphy to estimate minutes asleep within a 24-hour period.
Sleep quality measured using wrist actigraphy to estimate percentage of time in bed that the participant had undisturbed sleep (calculated using algorithms based on amount of movement).
Number of participants reporting being sleepy versus alert.
The number of students reporting being sleepy, however, went from 29% (five students) before rotations, to 32% (six students) during rotations, to 39% (seven students) after rotations, suggesting an increase in self-reported sleepiness (collected via sleep diary) during and following clinical rotations.
Nursing students’ self-efficacy scores regarding their ability to provide safe patient care (prevent adverse events to patients) consistently improved across the three time periods—from 80% at Time 1 (range = 28%-94%), to 84% at Time 2 (range = 59%-94%), to 87% at Time 3 (range = 53%-94%). This was a statistically significant difference (F = 33.41; df = 1,62; p < .001), indicating that the overall exposure to clinical rotations improved students’ belief in their own safe practice regarding safe patient care. This trend was also observed for self-efficacy regarding occupational health (preventing injuries to themselves)—from 71% at Time 1 (range = 58%-90%), to 76% at Time 2 (range = 55%-90%), to 77% at Time 3 (range = 52%-90%). Although self-efficacy scores for occupational health were lower overall than self-efficacy scores for patient care, the change in scores over time was statistically significant (F = 30.27; df = 1,56; p < .001), indicating that the exposure to clinical rotations also improved students’ belief in their own safe practice regarding occupational health.
Students assigned to night shift rotations had lower self-efficacy scores overall than students assigned to day shift rotations (82% vs. 87%), although this was not a statistically significant difference. Feeling sleepy significantly predicted both lower safe-practice self-efficacy scores (F = 42.55; df = 1,60; p < .001) and occupational health self-efficacy scores (F = 3.67; df = 1,58; p < .05). No other contextual variables entered into the models (e.g., sleeping with a bed partner) were significant.
Discussion
This study revealed that students’ safe-practice self-efficacy regarding both patient care and occupational health improved significantly with exposure to clinical rotations; however, occupational health self-efficacy was consistently lower than patient care self-efficacy. Furthermore, higher levels of self-reported sleepiness were significantly associated with students’ confidence in their ability to perform safe practice in both the patient care and occupational health domains.
Of particular interest, sleep quantity itself (per actigraphy) did not significantly impair self-efficacy scores—in fact, participants tended to receive similar sleep across the semester (just over 7 hours per night). Per current recommendations, this falls below the estimated 7.5 to 8.5 guidelines on sufficient sleep (Hirshkowitz et al., 2015). There are several possible explanations for our finding that sleep quantity did not vary, yet self-reported sleepiness both increased over the semester and predicted lower self-efficacy scores.
First, students consistently received slightly less than adequate sleep and thus were likely slightly deprived of sleep throughout the duration of the study. The increase in sleepiness seen across the study period could speak to a reduced ability to cope with this slight sleep restriction, especially when additional factors such as the stress of clinical rotations are considered. In other words, students who find it harder to cope with reduced sleep and the rigors of clinical exposure (evidenced by higher self-reported sleepiness scores) may also be less likely to feel confident in their ability to provide both safe patient care and practice in a way that promotes safety to themselves. The prior work of Postma et al. (2017) supports this possibility, as nursing students reported anxiety about coping with both sleep restriction and the uncertainty of shift work.
A second potential explanation for the fact that students’ sleep remained consistent over time and yet their sleepiness increased could be related to the timing of sleep. A proportion of the sample (37%) were assigned to evening and night shifts, requiring their sleep timing to be disrupted. Resulting circadian misalignment can result in sleepiness, even if sleep itself is not affected (Niu et al., 2013). That students assigned to night shifts tended to have lower self-efficacy scores (although not significantly so) lends some support to this possibility.
Another finding that requires discussion is that nursing student self-efficacy regarding occupational health was consistently lower than their self-efficacy regarding patient care. It is possible that this is an indicator of priority for nurses, whereby they are more concerned about the safety of the patient than their own well-being. Nurse self-care is critical however, both for the safety of nurses and for their provision of high-quality care to the patients. This speaks to a disconnect often speculated about within the nursing profession, where occupational health can be considered less important than patient care (Hankinson, 2015).
Implications for Occupational Health Nursing Practice
Our findings have implications for interventions designed to prepare nursing students for safe entrée to the workforce and for occupational health nurses working in the health care system. It is arguably easier to increase mental resilience to sleep restriction and stress than it is to increase total sleep time and reduce stressors. For example, shift work will always result in less than optimal sleep—especially for evening and night shift workers (James et al., 2017). Educating nursing students on how to optimize their sleep and promote sleep hygiene is of course important, but perhaps equally important is teaching them about sleepiness countermeasures such as light exposure, caffeine management, exercise, and hydration. Similarly, the nursing profession will always face stressors, particularly for new nurses. Reducing the number of stressors new nurses are exposed to is likely less feasible than promoting nurses’ belief in their ability to handle those stressors. As such, interventions and education that seek to (a) provide fatigue and sleepiness countermeasures and (b) promote resilience to stress may result in safer nursing practice—both in patient care and in occupational health.
This education could happen within nursing colleges or in the hospital setting. Qualitative research on nursing students preparing to enter the workforce suggests that students would be highly receptive to education on fatigue/sleepiness countermeasures and sleep hygiene promotion (Postma et al., 2017). Within the hospital setting, several options for this type of education exist, including the National Institute of Occupational Safety and Health (NIOSH) training “NIOSH training for nurses on shift work and long work hours,” DHHS (NIOSH) Publication No. 2015-115. Preliminary research suggests that this training could be effective at enhancing nurse safety and wellness, which could have consequent effects on patient care outcomes (Caruso, 2014). Of particular importance in light of our study findings, the NIOSH training places just as much importance on occupational health as it does on patient care, with key information on taking breaks, safe lifting practices, and so on, which can hopefully bring to light the importance of nurses taking care of themselves with the same commitment that they take care of their patients.
Study Strengths and Limitations
A strength of the study was the use of biopsychological sleep measurement via wrist actigraphy. Many studies rely solely on sleep diaries or other self-reported sleep measures, which tend to be less accurate (de Souza et al., 2003). Actigraphy is currently considered the most reliable method for investigating sleep outside using polysomnography in a laboratory setting (Driller et al., 2016). Another strength was the longitudinal design, allowing data collection at critical times during the nursing student’s professional formation. In addition, no participant attrition or missing data throughout the study were observed. This was particularly beneficial given the small sample size, which is a limitation of the study. The small convenience sample precludes generalization to the nursing student population. Future research needs to test larger samples to fully explore the impact of sleep and sleepiness on nursing student self-efficacy in safe practice. The current study findings do provide justification, however, for conducting a larger study on this topic. Another limitation, related to the small sample, was the lack of diversity (racial, ethnic, and gender) among the students, which also limits the generalizability. Finally, subjective sleepiness was measured with a single item, and future research should consider a more comprehensive examination of sleepiness.
Conclusion
This work begins to address a gap in the total worker health (TWH) research by examining a critical period in the professional development of nurses and helps to guide occupational interventions—particularly those targeted toward reducing nursing student sleepiness. Understanding student nurses’ initial sleep patterns in response to clinical rotations can yield insights into opportunities for occupational interventions at the university and hospital level. With approximately 2.9 million licensed and registered nurses, they make up the largest professional group in the U.S. health care workforce. 2 We owe it to them to ensure that new nurses joining this workforce feel fully confident in their ability to practice safely and take care of themselves and their patients.
Applying Research to Practice
This study addresses a gap in the total worker health (TWH) research by examining a critical period in the professional development of nurses and can inform the development of future occupational interventions. Of particular importance are interventions targeted toward reducing nursing student sleepiness and promoting resilience to shift work, stress, and sleep restriction. Our research adds to the body of research literature informing promotion of patient care and occupational health safe practice, and maximizing the health, safety, and productivity of the nursing workforce.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by NIOSH U19 OH010154, Oregon Healthy Workforce Center.
Notes
Author Biographies
Lois James is an assistant professor at the College of Nursing, Washington State University.
Patricia Butterfield is the Associate Dean for Research at the Elson S. Floyd College of Medicine, Washington State University.
Erica Tuell is a research coordinator at the College of Nursing, Washington State University.