
Abstract
Background:
Rotating shift work is common in high-hazard industries, despite documented associations with sleep disturbance and impairment. In the oil industry, where rotating and extended shift schedules are used to staff safety-sensitive positions, work intensification and increasing overtime rates have been broadly documented over the last few decades. Research on the impacts of these work schedules on sleep and health has been limited for this workforce.
Methods:
We examined sleep duration and quality among rotating shift workers in the oil industry and explored associations between schedule characteristics, sleep, and health outcomes. We recruited hourly refinery workers from the West and Gulf Coast oil sector members of the United Steelworkers union.
Findings:
Impaired sleep quality and short sleep durations were common and associated with health and mental health outcomes common among shift workers. Shortest sleep durations followed shift rotations. Early rise and start times were associated with shorter sleep duration and poorer sleep quality. Drowsiness and fatigue-related incidents were common.
Conclusion/Application to Practice:
We observed lower sleep duration and quality and increased overtime in 12-hour rotating shift schedules. These long workdays with early start times may reduce available hours for quality sleep; here they were associated with reduced exercise and leisure activity which correlated with good sleep. This safety-sensitive population appears severely impacted by poor sleep quality, which has broader implications for process safety management. Later start times, slower rotation, and a reconsideration of two-shift schedules are interventions to consider for improving sleep quality among rotating shift workers.
Background
Hourly refinery workers commonly work rotating shifts to accommodate 24/7 production. Since the 1990s, the majority of refineries have staffed their process operations with two 12-hour shifts; these rotate (change from night to day) every 2 to 4 days. Prior to this, three rotating 8-hour shifts were common, with a slower rotation frequency. Although rapid rotations have been found to be less disruptive by some (Costa, 1996; Knauth et al., 1980), there is substantial evidence that rapid rotation adversely affects sleep quality and quantity (Asaoka et al., 2013; Fischer et al., 1997; Pilcher et al., 2000). Actual work schedules have been observed to vary from nominal ones in the oil industry, with frequent overtime shifts interrupting recovery (Aguirre & Moore-Ede, 2014; Bourdouxhe et al., 2000). Long work hours are associated with short sleep duration (Harma, 2003; Knauth, 2007). In the healthcare industry, a comparison of 8- and 12-hour shifts found a greater prevalence of shift work sleep disorders (Asaoka et al., 2013) and shorter sleep duration (Geiger-Brown et al., 2012), increased fatigue, decreased performance, and increased errors reported on the 12-hour shift, particularly in hours 9 to 11 (Trinkoff et al., 2006). For industrial workers, short sleep duration, sleep disruptions, and decreased alertness have been documented on extended shifts (Fischer et al., 2000; Knauth, 2007), although some research has shown few differences (Smith et al., 1998). A review by Nachreiner (2001) identified increasing accident risk after hour 9 in four studies. A comparison of different schedules found that the 12-hour shift consistently produced the highest fatigue scores in transportation (Dawson & Fletcher, 2001) and nursing (Chen et al., 2014; Szczurak et al., 2007).
Shift workers experience disturbed sleep and increased sleepiness (Costa, 2015). Shift work sleep disorder, defined as the presence of primary insomnia and/or excessive sleepiness in relation to work schedules, is associated with gastrointestinal (GI) disorders, depression, anxiety, and fatigue (Åkerstedt et al., 2002; Flo et al., 2012). Because work schedules conflict with social and biological circadian rhythms, rotating shift workers experience chronic circadian misalignment. Social jet lag, defined as the discrepancy between mid-sleep hours on work days versus free days, has been used to illustrate this (Wittmann et al., 2006). Large individual differences have been observed among shift workers in adapting to work schedules (Saksvik et al., 2011). Older workers tend to have shorter and more disrupted sleep (Miles & Dement, 1980), and both circadian phase (Monk & Folkard, 1992) and chronotype (Fischer et al., 2016) have been shown to advance with age. Aging can also slow adjustment to circadian rhythm disruption from rotations (Bonnefond et al., 2006), reduce sleep after night shifts (Blok & De Looze, 2011; Sallinen et al., 2003), and increase insomnia (Harma et al., 1998).
For these safety-sensitive positions in a high-hazard industry, the impact of extended, rapidly rotating shifts concurrent with work intensification has not been well studied. Despite fatigue being identified as a root cause in several catastrophic refinery accidents, oil industry fatigue guidelines are voluntary and have been implemented inconsistently (Aguirre & Moore-Ede, 2014). The American Petroleum Institute (API) developed Recommended Practice 755, Fatigue Risk Management Systems for Personnel in the Refining and Petrochemical Industries (RP755) in response to a directive from the U.S. Chemical Safety Board and Hazard Investigation Board (CSB) following a catastrophic refinery accident in 2005 that identified fatigue as a causal factor (API, 2010; CSB, 2007). The CSB ultimately called RP755 “unacceptable” and issued a request for public comment in 2013 in an effort to revise it. However, in 2019, a second edition of RP755 was published that allowed for longer work sets (an increase from 84 to 92 hours) and shorter rest breaks (a decrease from 36 to 34 hours) for 12-hour shifts during normal operations (API, 2019). Now, as this skilled workforce ages, job demands have intensified alongside a volatile oil market. A better understanding of work schedules that impair sleep and impact overall health has the potential to increase job performance, improve process safety, and impact long-term worker health. This study evaluated recent work schedules among hourly refinery workers and explored associations between work hours and sleep quality and duration.
Methods
A self-reported questionnaire was administered to voluntary participants recruited from oil sector members of the United Steelworkers (USW) West and Gulf Coast districts to assess hours worked, shift rotations, sleep history, and current health and mental health status (including job stress). Participants were recruited through a roster of oil sector members of the USW union, as part of a larger survey administered to evaluate the effects of extended, rotating shifts on employee health and quality of life. The focus was on associations between hours of work, sleep duration and quality, and health outcomes associated with shift work. The survey included a job history questionnaire and questions about current staffing levels. The survey tool was developed and pilot tested among two focus groups of refinery members, who provided input on industry terminology, work schedule configurations, and schedule management.
Recruitment for the study began in late 2014, and the survey was administered in early 2015. Active or former USW members with current or previous experience in the oil sector who were at least 25 years of age were invited to participate. Participants were recruited by sending an informational flyer about the study to a large (17,000) member mailing list of current and former West and Gulf Coast oil sector members, of which an unknown proportion may have worked shifts. From the initial informational mailing about the study, we received 656 requests for surveys (a 3.9% response to recruitment); of these, 552 met eligibility requirements, 418 surveys were returned to the research team, and 384 of these were complete (a 69.6% response to contacts made). A small fraction of respondents (23) were retired or on leave when the survey was administered; these respondents were excluded from comparisons to recent hours worked. Participation in the study was entirely voluntary, and participant identities were not shared with the USW. Two incentives of US$1,000 each were awarded to one participant from each District, randomly selected using a sweepstakes drawing.
Survey
The 60-question survey included questions on demographics and work history, and validated measures for job stress, staffing, physical and mental health, and sleep quality. Data were collected on hours of work in the previous 4 weeks, including shift type (day, swing, or night) and overtime quantity (noted as additional shifts). Participants logged hours slept and hours worked for 1 week using a 24-hour log. A less detailed weekly work schedule log tracked day, night, and evening/swing shifts, and days off for the 3 weeks prior. This 4-week string of shifts worked was used to examine schedule patterns and tally hours worked. Hours spent commuting were requested.
Sleep quality was assessed using the Pittsburgh Sleep Quality Index (PSQI), a 19-item questionnaire that assesses subjective sleep quality over the past month using a composite of seven component scores (subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medications, and daytime dysfunction). Global PSQI scores range from 0 to 21 (higher scores representing worse sleep quality), with a cut-off of greater than 5 considered indicative of a clinical sleep disorder. Internal validity was tested using Cronbach’s alpha: the PSQI instrument resulted in an alpha of .72. Chronotype was estimated using the mid sleep time on work-free days (MSF), found to be an accurate assessment of the clinically measured chronotype (Wittmann et al., 2006). MSFs were calculated from the average mid-point between sleep onset and waking on free days (days off), if at least 36 hours of time off (two sleep events) were logged, using the guidelines for chronotyping shift workers published by the Munich Chronotyping Questionnaire (Roenneberg et al., 2003). Because we observed shorter sleep durations rather than oversleeping on the first sleep event, the suggested correction for sleep debt compensation was not applied.
Health outcomes were measured using questions from the National Health and Nutrition Examination Survey (NHANES), assessing GI discomfort (a self-report of heartburn, acid reflux, indigestion, constipation or diarrhea) and conditions associated with shift work. A self-report of systolic and diastolic blood pressure was requested. NHANES questions were also used to collect information on general health behaviors (frequency of smoking, alcohol, caffeine consumption, exercise, and leisure activity).
Questions on job stress were drawn from the National Institute for Occupational Safety and Health (NIOSH) Quality of Work Life Questionnaire (QWLQ) (U.S. Centers for Disease Control and Prevention [CDC], National Institute for Occupational Safety and Health [NIOSH], 2010). Ten questions were selected from the following domains: work demands (pace of work, physical exertion), co-worker support (co-worker competence and help/resources), supervisor support (promotional opportunity and concern for safety), skill discretion, decision latitude, justice, and overall job enjoyment. Responses were recorded on a 4-point Likert-type scale: 1 = not at all true, 2 = not very true, 3 = somewhat true, 4 = very true. Job stress variables were summed to create a global job stress score, which ranged from 0 to 30 (Cronbach’s alpha: .66). Negative answers were reversed so that a higher score indicated more support and lower job stress.
A truncated mental health questionnaire was assembled using five questions from the Patient Health Questionnaire (PHQ) 9-item scale for depression (Kroenke et al., 2001) and three from the Generalized Anxiety Disorder (GAD) 7-item scale for anxiety (Spitzer et al., 2006). Questions that would trigger mandatory reporting (suicide ideation) and those that overlapped between the two questionnaires were removed for brevity. A 4-point Likert-type scale rating was assigned to each symptom based on its frequency over the last month: 1 = not at all, 2 = several days, 3 = more than half the days, and 4 = nearly every day. A standardized score for depression and another for anxiety were created from the individual PHQ and GAD questions, respectively; these two subscales ranged from 1 to 4. The anxiety subscale had a Cronbach’s alpha of .69 and depression, .86. Higher scores indicated a higher frequency of adverse symptoms (poorer mental health).
Participants were asked about a history of incidents that they attributed to fatigue at any time in their career. Data were collected on four adverse outcomes: a reportable incident, a serious error, a near miss, or a car accident while commuting. Binary responses to each incident type were summed for a maximum count of four incident types per individual.
Statistical Analysis
Descriptive statistics were calculated for all variables of interest and tested for normality. Pearson’s correlation coefficients were calculated to assess associations between normally distributed linear sleep variables (chronotype, sleep duration and quality, rise and start times) and age, years of experience, job stress, and mental health scores. Differences between mean sleep durations and PSQI scores were tested for significance using a one-tailed Student’s t test (for two groups) or (for more than two groups) a one-way analysis of variance (ANOVA) with Tukey’s test for honestly significant differences (HSD) for post hoc pairwise comparisons. Logged sleep durations during 12-hour work sets and rest breaks of 48 hours or more were averaged and compared using a Student’s t test. Rise and start times were tested as a predictor of sleep duration and quality using linear regression. Multivariate linear regression was used to test predictors of sleep duration. Ordinal logistic regression was used to examine the effect of PSQI scores as a continuous predictor on the probability of fatigue-related incidents. Statistical analyses were generated using SAS 9.4 (copyright 2013, SAS Institute, Inc., Cary, NC, USA). The study received approval from the UCLA Institutional Review Board and informed consent was obtained in writing from all participants.
Results
Population
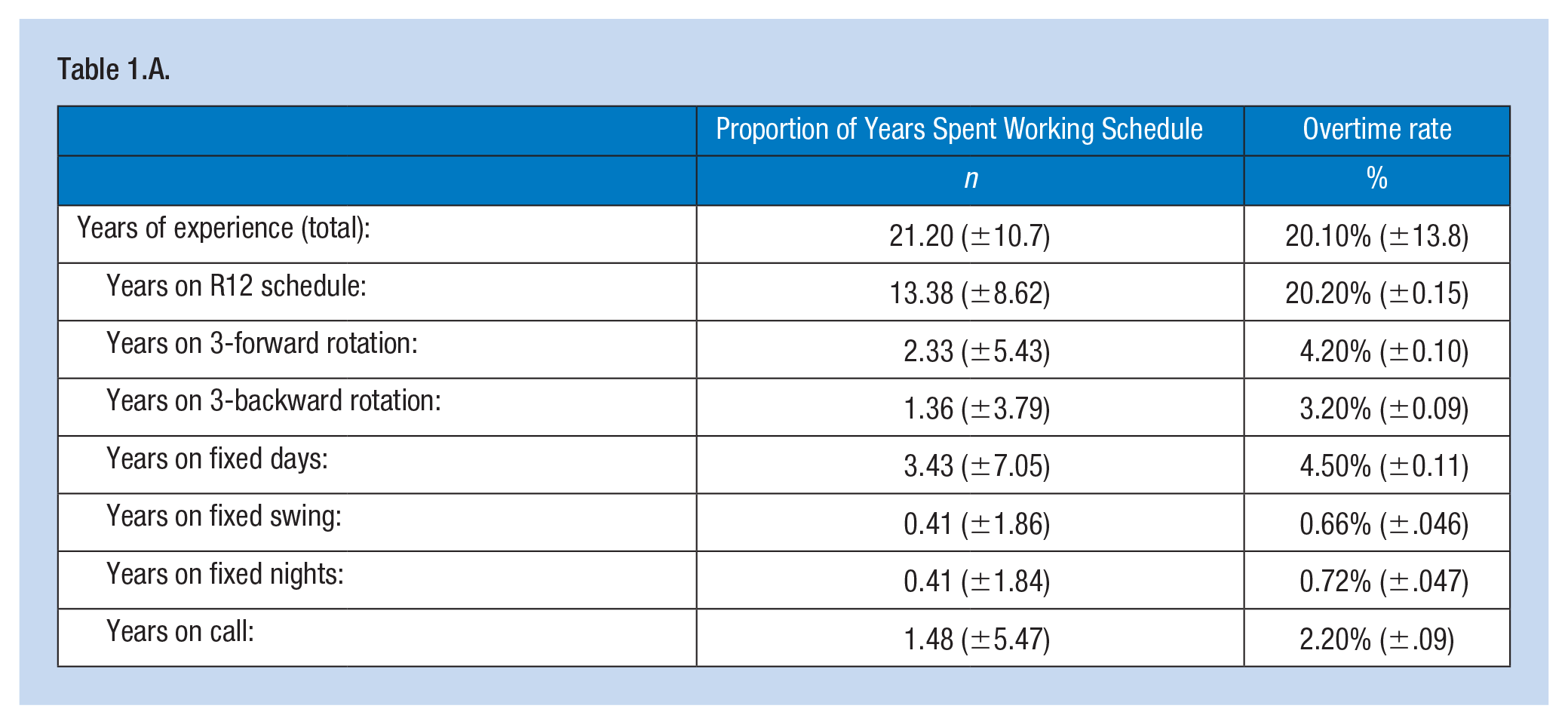
Characteristics of the study population are summarized in Table 1. The majority of study participants were male, worked as operators, had some college education, were older, married with children, and experienced. Sample demographics were comparable to available demographic data for this sector nationally (U.S. Bureau of Labor Statistics, 2014). The majority of the study population (91.7%, n = 351) was currently working 12-hour shifts and had for some time: 85.6% of their work history comprised rotating shift work, and of that, 68.3% comprised rotating 12-hour shifts (R12s). Participants had complex work histories, with a mix of rotating, fixed shifts, and on-call work that could not be easily grouped for analysis. The proportion of years spent working different schedules is summarized in Table 1.A.
Study Population Demographics
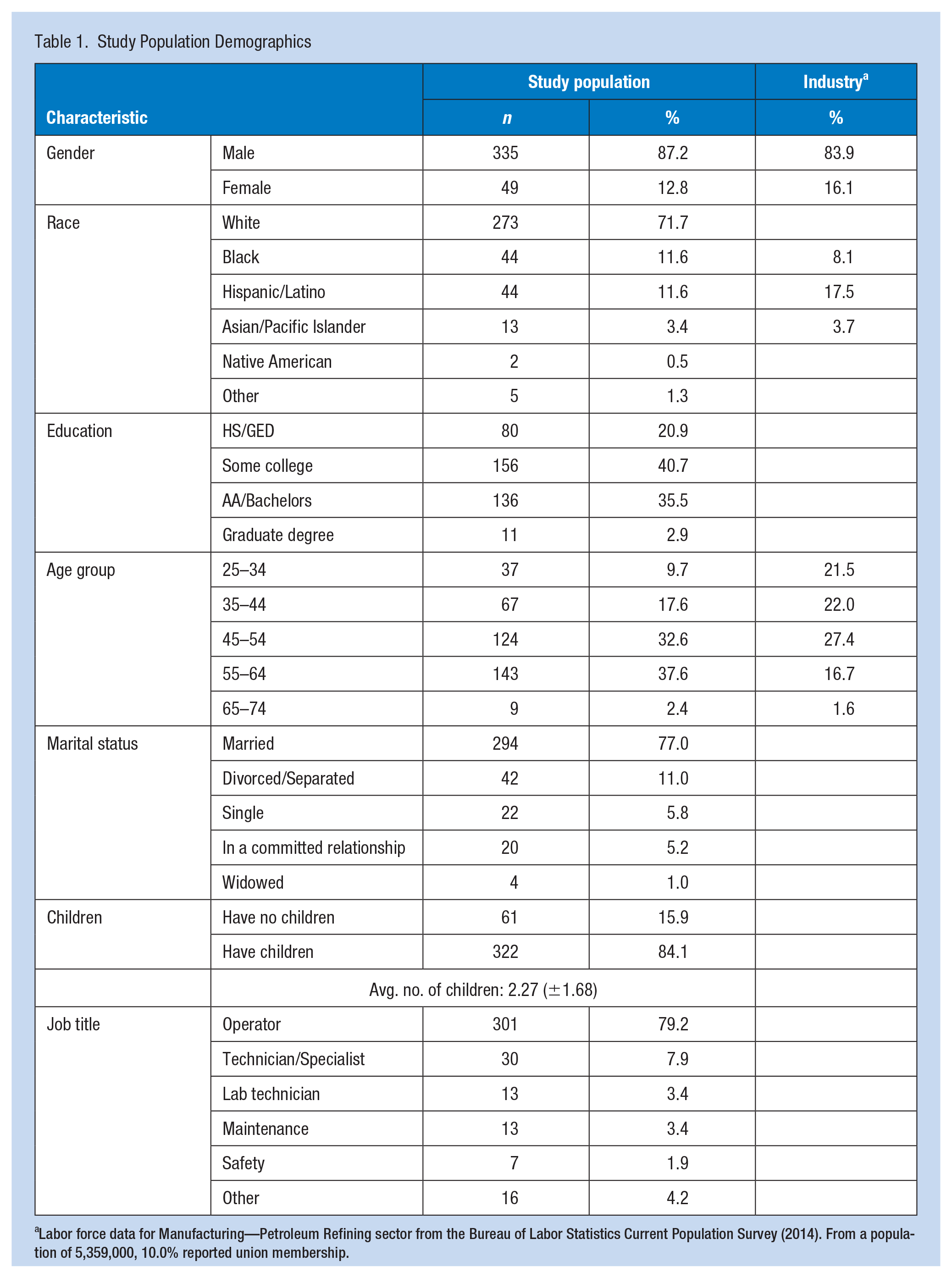
Labor force data for Manufacturing—Petroleum Refining sector from the Bureau of Labor Statistics Current Population Survey (2014). From a population of 5,359,000, 10.0% reported union membership.
Sleep Quality
Our mean global PSQI score was 8.97 (SD: 3.97) for the study population; this did not differ among the R12 schedules. A global PSQI score greater than 5 (a threshold for sleep disorders) was calculated for 78.2% of respondents; a global PSQI over 10 (a threshold for severe sleep disorders) was calculated for 34.8%. Participants rated their own sleep quality (one component of the PSQI) as very bad (9.6%), fairly bad (45.0%), fairly good (41.5%), and very good (4.0%). Sleep quality improved with age (r: −.20, p < .01) and years of experience in refining (r:−.16, p < .01), but was not associated with age at career start (age minus years of work experience) (r: −.06, p: .25). A linear association was also observed between decreased sleep quality scores and increased anxiety (r: .58; p < .01), depression (r: .54; p < .01), and job stress scores (r: .31; p < .01), in addition to GI symptoms (r: .28; p < .01)
Characteristics of those with good (PSQI ≤5) and poor (PSQI >5) sleep scores were examined (Table 2). Significant differences between the groups were found for certain lifestyle characteristics (good sleepers had greater exercise frequency and leisure activities, and shorter commute length); work factors (good sleepers had more years of work history, greater staffing availability, ease of taking time off, and lower job stress); and health outcomes (good sleepers had fewer GI symptoms, and less anxiety and depression) (p < .05). Differences in age, caffeine and alcohol consumption, and smoking were not significant between the groups, nor were work histories or recent hours worked (p > .05).
Comparison of Characteristics of Those With Good Sleep Quality and Poor Sleep Quality
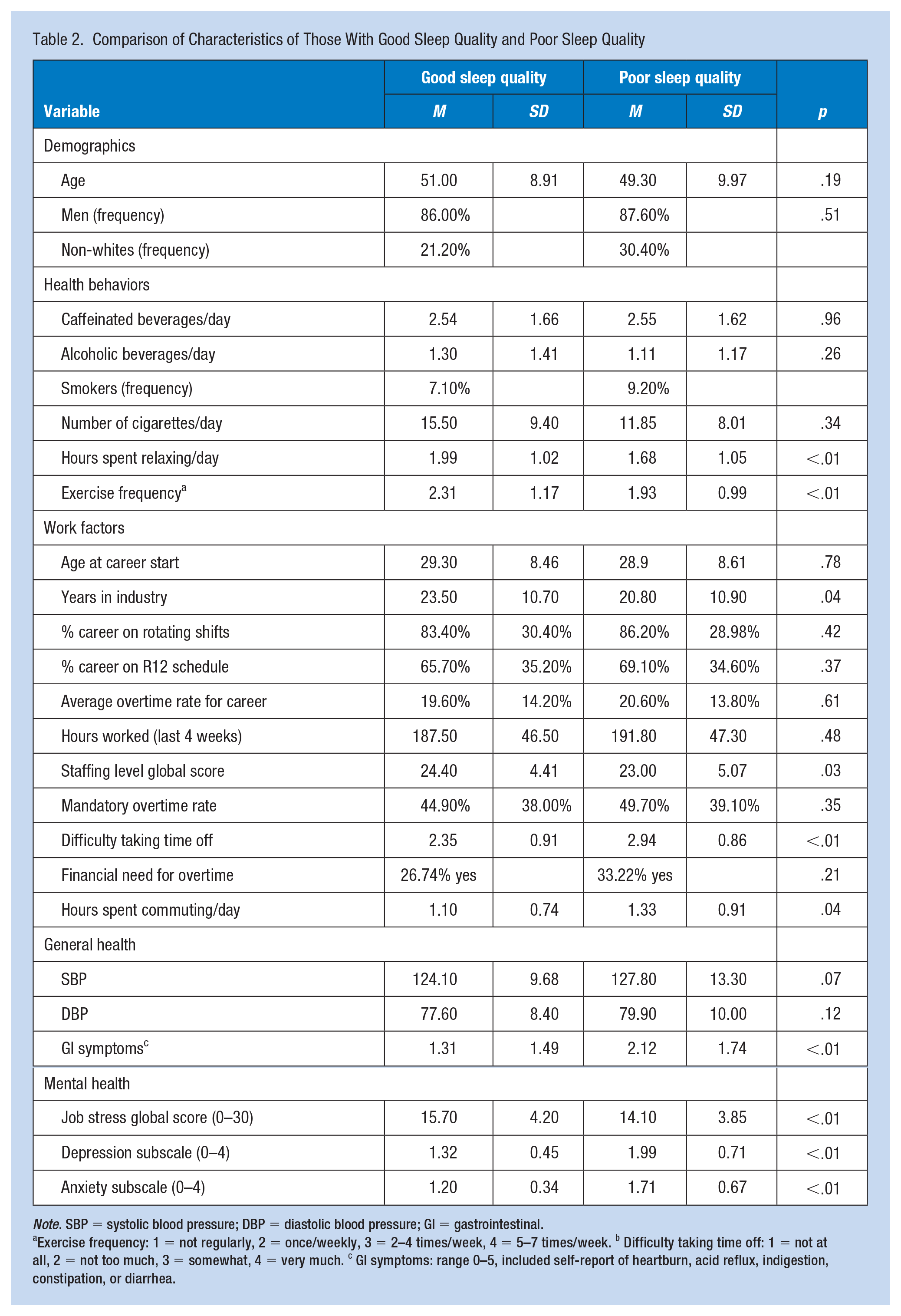
Note. SBP = systolic blood pressure; DBP = diastolic blood pressure; GI = gastrointestinal.
Exercise frequency: 1 = not regularly, 2 = once/weekly, 3 = 2–4 times/week, 4 = 5–7 times/week. b Difficulty taking time off: 1 = not at all, 2 = not too much, 3 = somewhat, 4 = very much. c GI symptoms: range 0–5, included self-report of heartburn, acid reflux, indigestion, constipation, or diarrhea.
Sleep Duration
A slight majority of the study population (50.6%) reported short sleep durations, defined here as <6 hours per night, with sleep durations ranging from 2 to 8 hours (M: 5.49, SD: 1.14). Both age (r: .22, p < .01) and years of work experience (r: .18 p < .01) were significantly correlated with increased sleep durations, but age at career start (age minus years of work experience) was not (r: .04 p: .44).
A shift-dependent variation in sleep duration was observed among R12 schedules, which is discussed below. Shorter sleep durations correlated with increased anxiety (r: .30; p < .01), depression (r: .30; p < .01), job stress (r: .19; p < .01), and GI symptoms (r: .13; p < .01). A multivariate linear regression explained 14% of the variance in sleep duration based on a possible allocation of hours in the day (p < .01): commute length and overtime significantly predicted reduced sleep duration, and shift length had a weak association. Exercise and leisure activities significantly predicted increased sleep duration (Table 3).
Multivariate Linear Regression of Sleep Duration Onto Daily Activities
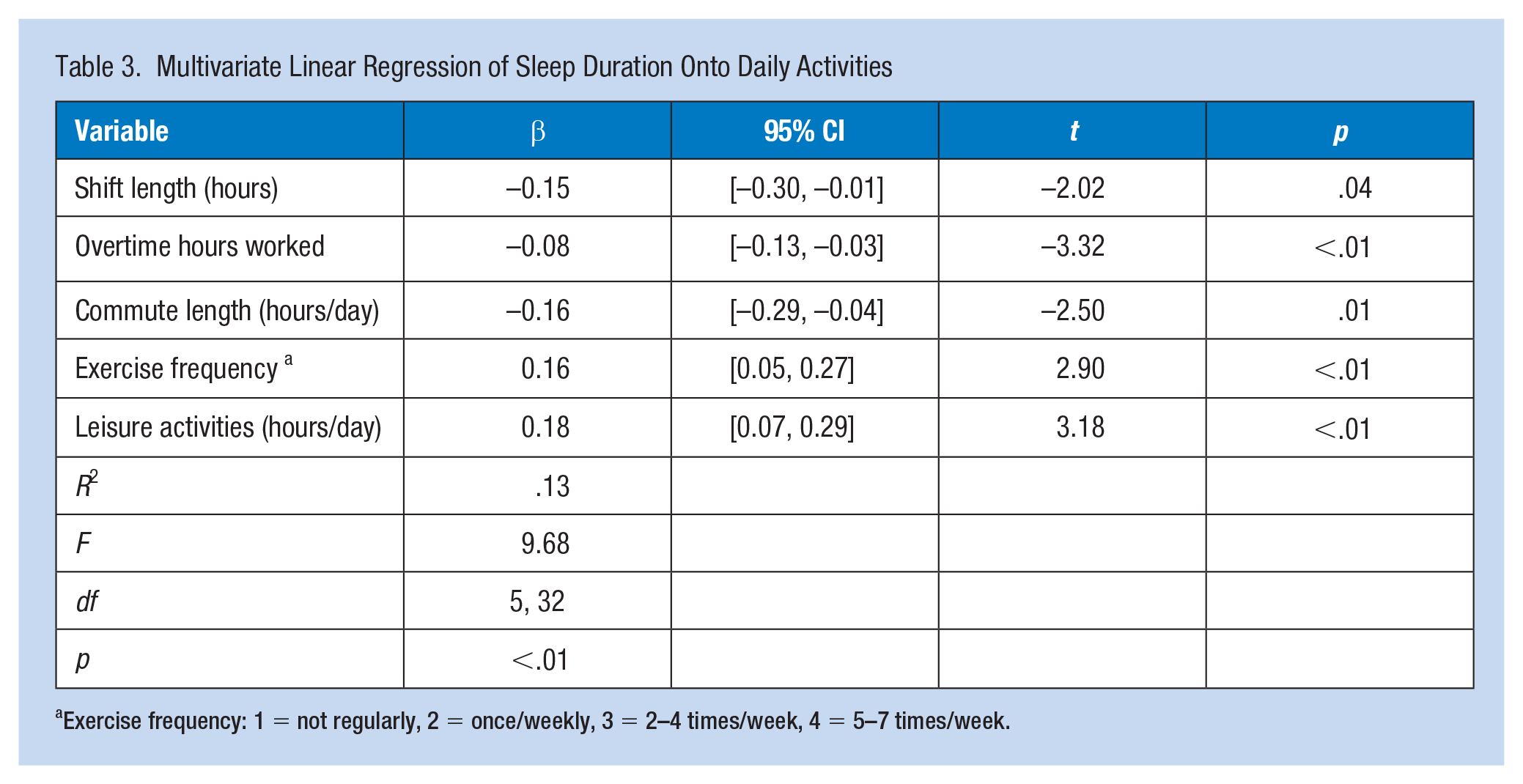
Exercise frequency: 1 = not regularly, 2 = once/weekly, 3 = 2–4 times/week, 4 = 5–7 times/week.
Work Schedules
Those with a history of rotating shift work had shorter sleep duration and poorer sleep quality scores than those who worked permanent day shifts (Table 4). Among shift workers, when a threshold of 15 years of shift work experience was applied to assess tolerance (as suggested by Costa, 2003), both sleep quality and quantity were lower in the group with less than 15 years of experience (p < .05). Sleep quality improved for those on leave or in retirement (p < .05). Sleep duration was longer during 8-hour shift work sets compared to 12-hour shift work sets (p = .05).
Mean Sleep Duration and Sleep Quality Scores for Study Participants, Grouped by Work History, Employment Status, and Shift Length
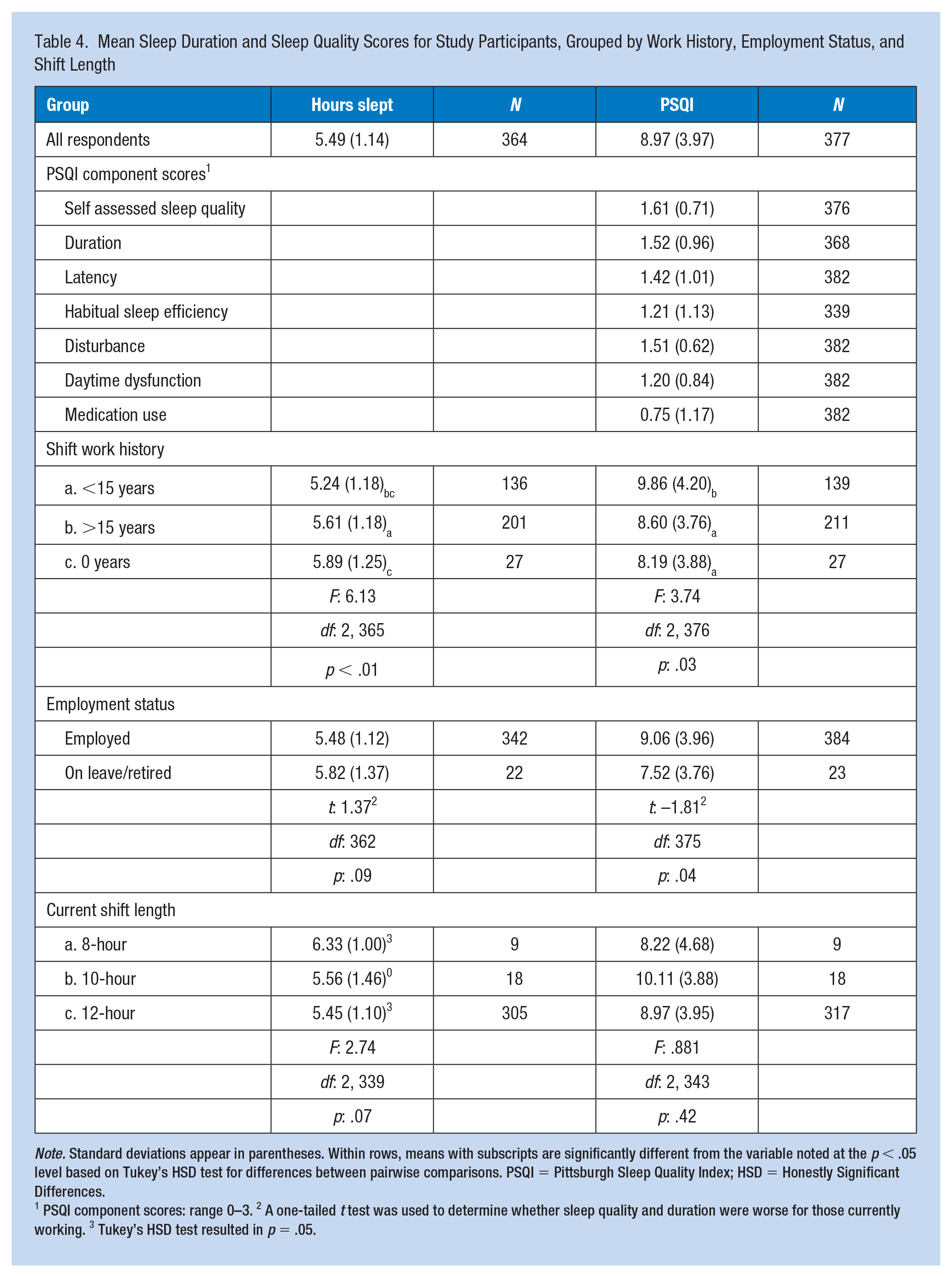
Note. Standard deviations appear in parentheses. Within rows, means with subscripts are significantly different from the variable noted at the p < .05 level based on Tukey’s HSD test for differences between pairwise comparisons. PSQI = Pittsburgh Sleep Quality Index; HSD = Honestly Significant Differences.
1 PSQI component scores: range 0–3. 2 A one-tailed t test was used to determine whether sleep quality and duration were worse for those currently working. 3 Tukey’s HSD test resulted in p = .05.
Shortest sleep durations were reported following shift rotation (4.89 hours), then during night shift sets (5.04 hours), during day shift sets (5.34 hours), and then following a day off (7.07 hours). Significant differences were found between all groups, except between night shift and post-rotation (Figure 1). Total hours slept for the week (including days worked and days off) were negatively correlated with total hours worked (r: −.18, p < .01).
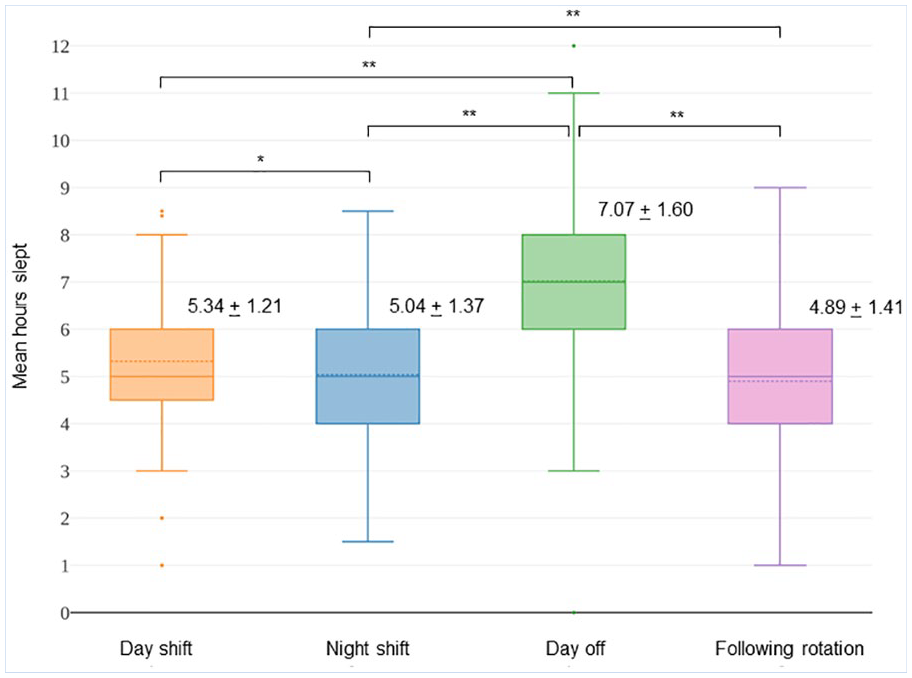
Mean Hours of Sleep Reported During Day and Night Shift Sets, Between Days Off, and Immediately Following a Shift Rotation.
Day shifts had early start times: rotating 12-hour shifts started between 3 and 7 a.m. (median: 5 a.m.). Night shift start times ranged from noon to 9 p.m. (median: 5 p.m.). Rise times prior to day shifts ranged from 2 to 6 a.m. (M: 3:44 ± 0:41 a.m.). Rise times prior to night shift varied widely (range: 5 a.m. to 5 p.m., M: 12:02 ± 2:04 p.m.). On their day off, participants typically slept till 8 a.m. (M: 7:59 ± 1:59 a.m.). During day shift sets, sleep duration increased by 28 minutes for each hour later participants woke (p < .01) and increased 19 minutes for each hour later their shift started (p < .01). For the night shift, hours slept increased 15 minutes with later rise times (p < .01), but not later shift start times (p = .83). Later rise and start times were a significant predictor of improved (lower) sleep quality scores for both shifts (p < .05), although explained variance was low.
Individual Sleep and Schedule Characteristics
Chronotypes (as MSF) were estimated for a subset of respondents who reported consistent work and sleep hours on the daily log (n = 237); these were examined for misalignment with their work schedules. MSFs calculated indicate a predominance of very early chronotypes (mean MSF: 2:12 ± 1:52 a.m., median 2:00 a.m.); a histogram also revealed a small cluster of very late chronotypes. No linear relationship was observed between MSF and sleep quality (r: −.02, p = .76) or duration (r: .07, p = .30). When grouped into five bins, MSFs around 3:30 a.m. had the longest sleep, F(4, 200): 2.41, p = .05, but sleep quality, F(4, 208): 1.00, p: 0.40, and drowsiness, F(4, 209): 0.72; p = .58, were not significantly different.
Differences between MSF and mid-sleep on work (MSW) days, or social jet lag, were much higher during night shift work sets (t: 14.09, p < .01). MSW during day shift sets (MSWD) were 12:30 ± 1:00, resulting in a social jet lag estimate for day shifts (MSFD−MSWD) of 1.79 (±1.66) hours. MSW during night shift sets (MSWN) were 9:04 ± 1:40 a.m.), yielding an MSFD−MSWN value of 6.80 (±2.34) hours. No associations were found between these social jet lag values and sleep duration or quality (p > .05).
Fatigue and Adverse Outcomes
Having trouble staying awake during engaged activities or drowsiness (PSQI component “daytime dysfunction”) increased as sleep duration, F(3, 364): 8.96, p < .01, and quality, F(3, 377): 36.84, p < .01, decreased. Drowsiness was reported by more than half the study population: 24% reported it monthly, 17.7% one to two times weekly, and 9.4% three or more times weekly. Those who reported frequent drowsiness (3 or more times a week [n = 36]) averaged 4.83 ± 1.32 hours of sleep per night; those who reported drowsiness 1–2 times per week (n = 57) averaged 5.22 ± 1.11 hours per night.
Our survey asked participants whether they had ever had an incident at work or while commuting that they attributed to fatigue. One third of the study population reported at least one type of incident, and 6.3% more than one type of incident. Nearly a fourth (24.6%) of respondents reported a near miss at work, 7.6% reported a vehicle accident while commuting, 4.7% a serious error, and 3.1% a reportable accident. Elevated PSQI scores were associated with a higher frequency of these incidents. For every one-unit increase in PSQI scores, increased odds of an adverse event were observed for: near miss odds ratio (OR) = 1.11 [1.05, 1.18], vehicle accident OR = 1.14 [1.03, 1.25], serious error OR = 1.12 [0.97, 1.29], and reportable accident OR = 1.09 [0.97, 1.23].
Discussion
We found that sleep duration, particularly sleep quality, was severely impacted in this safety-sensitive population. Early start times were widely reported, with evidence of earlier than average chronotypes among the population. Shorter sleep durations were reported following shift transitions, and the highest social jet lag values were found during night shift sets. Frequent drowsiness was reported, and fatigue-related incidents were fairly common. Health outcomes associated with shift work were prevalent, with the strongest associations found between poor sleep quality and anxiety and depression.
Although rotating shift work cannot be eliminated, these findings point to various schedule modifications that have the potential to improve sleep. Our study provided further evidence that early rise and start times may adversely impact sleep (Costa, 1996; Knauth et al., 1980). Åkerstedt et al. (2010) found that early rising times (to accommodate early start times) were not accompanied by earlier bedtimes, resulting in sleep debt. The very early start times reported here may be linked to the adaptation of the workforce toward morningness we observed, although morningness has been found to increase with age. Chronotypes estimated here were 2 to 3 hours earlier than those reported elsewhere for the general population (Wittmann et al., 2006), and 1 to 2 hours earlier than those reported previously for shift workers with a 6 a.m. shift start time (Fischer et al., 2016). Previous studies have found morningness to be associated with better sleep quality (Natvik et al., 2011). However, we found the longest sleep durations reported were by those with later MSFs (around 3:30 a.m.
Some have proposed that a flexible chronotype is beneficial for shift work adaptation, particularly for rapid rotation schedules (Reinberg et al., 2007). Despite an equally balanced shift assignment, we found a high prevalence of very early MSFs, a possible indicator of chronotype inflexibility. If this is the case, it could intensify the hardship of transitioning to night shift following rotations. Late chronotypes have been associated with depression in various studies (Levandovski et al., 2011; Selvi et al., 2010), suggesting social jet lag as a possible mechanism. We saw severe desynchrony (nearly 7 hours) and high social jet lag for the majority of those working night shift sets, but did observe a small cluster of late chronotypes. These could benefit from a permanent night shift schedule. As suggested by others, considering individual chronotype in the assignment of fixed or rotating shifts could prove beneficial. Finally, rapid rotation schedules have been associated with poor sleep in various studies. We saw sleep durations <5 hours following shift rotations, and responses to open-ended questions identified the shift change as a source of fatigue and hardship (data not shown). Rapid rotation schedules in the oil industry, such as the “every other weekend off” or 2-3-2 schedule, were designed to distribute weekend work equitably, but they lose their merit when overtime (we saw average rates of 20%) eliminates weekends at home. Reducing the number of shift transitions has the potential to improve sleep.
Our findings reveal greater levels of impairment and sleep deficit than have been reported elsewhere. Prevalence of sleep disorders (as PSQI global score >5) affected 78.3% of the study population compared to a general population prevalence of 71.3%, and severe sleep disorders (PSQI >10) affected 34.8% compared with 5.4% (Hinz et al., 2017). Previously published PSQI scores include 4.66 for the general population and 6.73 for other shift workers (van Mark et al., 2010), and 7.31 for rotating shift workers (Ruggiero, 2005); we measured 8.97. Our individual PSQI component scores were within the ranges of those previously reported for patients with clinically diagnosed sleep disorders, with the exception of daytime dysfunction; our scores for sleep duration (1.52 ± 0.96) were not significantly different from patients with primary insomnia (1.51 ± 1.20) and depression (1.71 ± 1.14); sleep latency (1.42 ± 1.01) was comparable to insomnia patients (1.42 ± 1.01); and sleep disturbance scores (1.51 ± 0.62) to patients with depression (1.47 ± 0.51), narcolepsy (1.53 ± 0.72), and insomnia (1.40 ± 0.62) (p > .05) (Buysse et al., 1989).
We found that as PSQI scores worsened, odds of a past fatigue-related incident increased. Although current sleep quality lacks temporal significance with these past events, poor PSQI scores have been measured in former shift workers, lasting into retirement (Monk et al., 2013), suggesting this tool could be used to detect long term sleep disorders. We did not measure performance in our study, but others have found correlations between clinically measured function and attention deficits and PSQI component scores. Benitez and Gunstad (2012) found that poor subjective sleep quality was associated with reduced executive function, and short sleep duration was associated with a lower attention span in healthy young adults, while Nebes et al. (2009) found sleep latency and habitual sleep efficiency associated with impaired reasoning, attention, and memory in older adults. We saw both sleep quality and duration improving with age, possibly because of an industry trend to provide older workers the option for permanent day shifts as a result of either seniority or health conditions that contraindicate rotating shift work. Older workers also tended to work less overtime.
Average sleep durations reported here were in the range of those documented in the incident investigation that initiated the fatigue risk management guidelines for the petroleum industry (CSB, 2007). Shortest sleep durations were associated with more frequent episodes of drowsiness. More than one fourth of the study population reported weekly (or more frequent) episodes of drowsiness during engaged activities. A meta-analysis of 36 shift work studies that analyzed only three 8-hour shift rotations (N = 4,375) conducted by Pilcher et al. (2000), reported average sleep durations of 6.62 hours during the day, 8.03 hours during the evening/swing, and 5.85 hours during night shift sets in three shift systems. In contrast, we observed an average of 5.26 hours during day shift sets and 4.99 hours during night shift sets, when restricting our sample to only the R12 shifts. Although Pilcher’s meta-analysis was not limited to the manufacturing sector and confounders cannot be controlled for, it provides a crude comparison that implicates the 12-hour shift as adversely impacting sleep duration. This also suggests that the loss of the swing shift (which averaged sleep durations of 8.03 hours in the Pilcher et al. study) may have eliminated an opportunity for recovery. We also observed decreased frequency of exercise and leisure activities for those working 12-hour shifts; these activities were positively correlated with improved sleep.
Both sleep quality and sleep quantity were correlated with health outcomes that have been associated with shift work, including anxiety, depression, and GI discomfort. A study of 12-hour shifts in the petroleum industry in Iran identified increased risk of GI and psychological disorders as weekly hours worked increased (Choobineh et al., 2012), and Parkes (2002) found that neuroticism, anxiety, and negative affect were associated with lower shift work tolerance in refining. Self-reported data collected from nurses on 12-hour shift rotations showed strong associations between shift work disorder and both anxiety and depression (p < .001) (Flo et al., 2012). The extremely strong correlation we saw between global PSQI scores and depression and anxiety measures has not been replicated elsewhere. Associations between depression and sleep disorders have been studied extensively, but the causal mechanisms are poorly understood, with many comorbidities acting as mediators. The association between PSQI scores and depression was examined as part of the instrument validation (Buysse et al., 1989). Later, Grandner et al. (2006) suggested that the subjective measures of the PSQI may better detect negative affect, but Nebes et al. (2009) found higher PSQI scores associated with functional aspects of depression (motivation, concentration, decision making) rather than mood. Social jet lag has been proposed as a risk factor for depression and anxiety, but this has been disputed. Reduced sleep efficiency, increased latency, and short sleep duration have been associated with generalized anxiety disorder in a clinical study (Benca et al., 1992). We also sleep quality improving with reduced job stress, increased ability to take time off, and higher staffing; associations with individual job demands are examined further elsewhere (McNamara, 2018).
Refinery workers are an understudied population, and by administering our survey directly to employees through union rosters, we were able to capture unique dimensions of their work characteristics, including schedule irregularities, overtime, staffing levels, and job stress, alongside sleep patterns, and health behaviors. However, the data contain potential inaccuracies inherent in self-reported data, and the sample has limited power from a small data set and low response to recruitment. The issue of overtime is controversial among the workforce, as many rely on the added income overtime provides. Efforts by the union to strengthen industry fatigue guidelines and alleviate job demands have had limited success. These efforts culminated in a national strike in the USW oil sector in January and February 2015 during study recruitment, which may have impacted participation. All of this presents the potential for selection bias among participants. Furthermore, because recruitment materials advertised a health study on rotating shift work, interested participants may have been motivated by a concern about health complaints, which could limit generalizability. Limited funding restricted the use of incentives for all participants and follow up mailings. Despite this, the demographics of the study population (gender, race, and age) were comparable to those published for this workforce nationally. Trends in our data (such as shift work tolerance) have been replicated elsewhere. Complex work histories of different schedule configurations limited retrospective exposure assessment or evaluations of distinct schedules.
Applications to Professional Practice
Self-reported survey data indicated that a sample of oil refinery operators exhibited impaired sleep quality and short sleep durations. Long shifts (12 hours or more with holdovers) were reported; these predicted shorter sleep durations when combined with long commutes and overtime. Poor sleep quality scores were associated with gastrointestinal symptoms, as well as anxiety and depression; sleep quality improved with exercise and leisure activities. Inexperienced shift workers exhibited diminished sleep quality and quantity. The shortest sleep durations reported were following shift transitions; these averaged less than 5 hours. Opportunities to improve sleep in this safety-sensitive workforce include later start times, fewer rotations, eliminating holdovers (particularly for extended shifts), and accommodating inexperienced shift workers by acknowledging individual chronotypes and social and family demands. These recommendations are applicable to all industries that employ rotating shifts.
Footnotes
Acknowledgements
The authors thank David Campbell from USW Local 675 for his leadership during the study inception and the USW Health, Safety and Environment Program (Mike Wright and Kim Nibarger) and the USW Tony Mazzocchi Center (John Scardella) for their support of the project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by NIOSH SCERC traineeship and Pilot Research Grant no. 5 T42 OH008412-9. Mailing costs for the survey were supported in part by the United Steelworkers Charitable and Educational Fund.