
Abstract
In the United States, approximately one half of individuals with chronic hepatitis C virus (HCV) are not aware of their status. Current HCV treatment is highly successful and is associated with a decrease in all-cause mortality. Occupational health nurses (OHNs) are often the sole health care providers at worksites and have a unique opportunity to provide HCV education, screening, and linkage to care. This project measured changes in OHN HCV competency and outreach, and identified barriers to screening. In June 2017, Survey 1 was emailed to 3,414 American Association of Occupational Health Nurse (AAOHN) members. For HCV competence, HCV knowledge and confidence in educating and counseling employees regarding HCV were assessed. HCV outreach and barriers to screening were identified. The HCV educational campaign launched in October 2017 with a webinar, a webpage/toolkit, and educational emails. Survey 2 was emailed in January 2018 to assess for changes in HCV competency and outreach. A total of 445 OHNs responded to Survey 1, and 111 completed both surveys, and participant demographics represented AAOHN membership base (95% female, mean age 56.4). The average HCV knowledge pretest score was 76% and posttest score was 77%. Confidence in educating/counseling employees about HCV increased from 2.6 to 2.9 (on a 1-5 scale; p = .052). Higher pretest scores were associated with bachelor’s degree (BS/BA) education or above, greater confidence in HCV education/counseling of employees, and HCV education participation within the prior 12 months. There are ongoing HCV learning needs for OHNs and greater opportunities for HCV outreach in worksites.
Introduction
In the United States, it is estimated that there are 3 to 4 million individuals infected with chronic hepatitis C virus (HCV), and that approximately half of those are unaware of their HCV infection (Denniston et al., 2014). The prevalence is highest in people born between 1945 and 1965 and individuals with a history of injection drug use, blood transfusions before 1992, and HIV infection (Centers for Disease Control and Prevention, 2015). Chronic HCV infection can result in cirrhosis, liver failure, hepatocellular carcinoma, and an increase in all-cause mortality (American Association for the Study of Liver Diseases and Infectious Diseases Society of America [AASLD and IDSA], 2018). Successful HCV treatment has many proven benefits including decreasing all-cause mortality and reducing the incidence of hepatocellular carcinoma (Ghany, Strader, Thomas, & Seeff, 2009). Current HCV treatment regimens are highly efficacious (95%-100% sustained virologic response) and have very few side effects. The AASLD and the IDSA recommend that HCV treatment be offered for all chronically infected HCV persons, except those who have less than a 12-month survival due to nonliver-related conditions (AASLD and IDSA, 2018). In the United States, only 13% to 18% of chronic HCV patients received HCV treatment (Spradling et al., 2018).
Occupational health nurses (OHNs) are often the sole health care providers at worksites, and have an opportunity to provide HCV education to all employees, with outreach for testing and linkage to care for at-risk employees. It is unknown if OHNs are current in their knowledge of HCV risk factors, testing, and treatment, and if they are providing employees with HCV education, screening, and linkage to care. It is also unclear if there are organizational factors influencing the extent of HCV outreach in worksites.
In May 2017, the American Association of Occupational Health Nurses (AAOHN) Foundation was awarded a grant from the National Viral Hepatitis Roundtable (NVHR). The purpose of this funding was to advance OHN HCV competency and share best practices to improve HCV knowledge of employees, and to increase HCV screening and linkage to care for at-risk employees at the worksite. OHNs often have long-term relationships with employees and have opportunities to coach and support workers with evidence-based recommendations for screening and treatment of chronic health care conditions, including HCV.
The aims of this AAOHN HCV Outreach project were to measure baseline levels and degree of change in HCV knowledge and confidence (i.e., competency) in AAOHN members after providing a comprehensive HCV educational campaign. Current outreach strategies used by OHNs to provide HCV screening, and any identified barriers that may limit HCV screening in the workplace were assessed by two surveys.
Background
HCV Screening Recommendations
In 1998, the CDC recommended HCV screening based on specific risk factors for contracting HCV, such as intravenous (IV) drug use and those who have received blood products before 1992. The CDC published the first major update in Hepatitis C screening guidelines in 2012. This update recommended additional screening of all persons born between 1945 and 1965 to improve HCV screening rates (Al-hihi, Shankweiler, Stricklen, Gibson & Dunn, 2017). This age cohort is known as the baby boomer generation, and, of those diagnosed with HCV in the United States, 75% are in this age cohort (Smith et al., 2014). Of deaths from HCV between 1999 and 2007, 73.4% were baby boomers (Davis & Roberts, 2010). Despite risk factor screening efforts, approximately one half of HCV cases remain undiagnosed (Yehia, Schranz, Umscheid, & Lo Re, 2014).
HCV Knowledge
At the outset of this project, knowledge about HCV risk factors, diagnosis, or treatment among OHNs was unknown. McGowan et al. (2013) reviewed physician knowledge about the updated hepatitis C treatment guidelines on a global scale. The study evaluated knowledge of 697 physicians who specialized in HCV treatment or who were general practitioners who actively treated patients with HCV. There were knowledge gaps identified in the treatment of HCV, with higher knowledge scores in hepatologists compared with general practitioners. Overall, 20% to 54% of respondents felt that health care providers had sufficient knowledge of the updated hepatitis C treatment guidelines. However, only 29% of U.S. physician respondents (n = 102) agreed to the statement that providers in the United States had sufficient knowledge of the HCV guidelines, 18% agreed that the general public was aware of HCV, 16% agreed that patients understood the consequences of untreated HCV, 7% agreed that patients were aware that HCV is curable, and 17% agreed that patients in the United States had adequate access to HCV providers in their communities (McGowan et al., 2013). These results indicate that a majority of health care providers in the United States, including OHNs, may benefit from ongoing HCV screening and treatment education.
Work-Related HCV Risk
In the occupational health setting, health care workers are an at-risk population targeted for hepatitis C screening. The Bloodborne Pathogens Standard (29 CFR 1910.1030), which was passed in 1991 by the Occupational Health and Safety Administration (OSHA), raised awareness regarding the risk of contracting hepatitis C, among other viruses, when a worker is exposed to blood or specific body fluids. Although baseline HCV screening and serial HCV testing for at least 6 months after potential HCV exposure through a blood-borne pathogen exposure is the usual standard of care, there is a very low risk of contracting HCV after a work-related exposure, and currently there is no recommended postexposure prophylaxis (AASLD and IDSA, 2018; Orland, Wright, & Cooper, 2001).
HCV Screening Strategies
Several studies have documented increased HCV screening of the 1945-1965 birth cohort using electronic medical record (EMR) reminder prompts in primary care clinic settings. Al-hihi et al. (2017) found an EMR prompt in Epic™ increased one-time HCV screening from 30% to 55% over a 9-month period. Konerman et al. (2017) also used an EMR reminder in Epic™ emphasizing the birth cohort, and HCV screening increased from 7.6% to more than 72% in one year.
Prior to implementing HCV screening EMR prompts, providers based HCV screening decisions on race, gender, and insurance type rather than on current screening guidelines (Konerman et al., 2017). While this study ultimately found EMR prompts to be effective, another study found that despite EMR prompts, providers who had not received integrated education on updated HCV screening guidelines frequently overrode the prompts and failed to screen at-risk patient populations (Nitsche, Miller, Giorgio, Berry, & Muir, 2018).
While EMR reminders are valuable, focused efforts including reminder tools, staff education, and performance reporting for improving clinician behavior led to increased birth cohort testing for HCV and initiation of curative therapy (Nitsche et al., 2018).
Known Barriers to HCV Screening and Treatment
Barriers to hepatitis C screening can be divided into several levels: provider, patient, payer, and/or government. Clinician competence in HCV and perceived health system barriers of time and cost of screening may reduce screening. McGowan et al. (2013) found physicians feel the general public is unaware of HCV and does not know HCV is curable. Only 35% of providers believe patients have adequate access to HCV treatment providers with the lowest rate in the United States (17%) and the highest in the Nordic countries (62%). McGowan et al. (2013) also found that providers have insufficient training to manage HCV treatment and a limited referral base to specialist providers that have the ability to provide HCV treatment.
Patient-related barriers such as fear of stigma, lack of appreciation of risk, and the incorrect belief that they had been vaccinated for HCV have been found to affect birth cohort screening (Nitsche et al., 2018). Patients may not be aware of the need to be tested, and may not be able to afford the costs associated with treatment.
Payer-related barriers include costs to the patients and costs to the insurance companies. Patients may have high out-of-pocket expenses or their private or government-sponsored health care insurance does not cover the expense of treatment. Government barriers include restriction of treatment due to costs or availability of medications, lack of country-wide education regarding HCV prevalence and need for screening, and insufficient funds for public health initiatives (McGowan et al., 2013).
Project Aims
The AAOHN HCV Outreach Project aimed to determine OHN competency (knowledge and confidence) in HCV and the number of HCV outreach activities before and after an intervention educational campaign. It also aimed to identify the demographic, professional, and organizational factors associated with higher baseline HCV knowledge in OHNs and to describe any reported barriers to HCV screening in the work site. The long range goal of the AAOHN HCV Work Group is to increase one-time HCV screening of employees/retirees born between 1945 and 1965.
Method
Project Team
AAOHN is the largest U.S. organization of nurses providing health care to workers in the workplace. AAOHN created an HCV Work Group of AAOHN members from a variety of work settings with experience and/or interest in hepatitis C, which included three OHNs from the health care industry and one OHN from a large global manufacturing company, co-led by one hepatitis C advanced practice nurse practitioner and one nurse researcher. The AAOHN director of education and AAOHN education manager were additional members of the HCV Work Group. This team was responsible for reviewing the literature, developing pre- and posttest surveys, pilot testing the surveys, conducting data analysis, reviewing survey results, developing and/or evaluating educational materials for the AAOHN HCV webpage, previewing educational sessions (i.e., webinar, concurrent sessions), presenting the webinar/concurrent sessions, and drafting the final manuscript.
Project Overview
The AAOHN HCV Work Group met monthly, via conference call, beginning in May 2017 to guide this one-year HCV Outreach Project. In May 2017, the Work Group leaders communicated with the University of California, San Francisco, Committee on Human Research (CHR), and determined that a CHR review was not required due to the quality improvement nature of the HCV Outreach Project. A pretest survey was developed and pilot tested with the HCV Work Group members in May 2017, and, in June 2017, all AAOHN members (excluding students and retirees) were invited via email to participate in this survey. At the beginning of this first survey, members were informed their email would be used for a second survey in January 2018, and their de-identified survey data would guide an educational toolkit/webpage and HCV webinar, which launched in October 2017. An additional method to build HCV awareness and knowledge included periodic email blasts (sent from September 2017 through January 2018).
The Intervention
The intervention for this quality improvement project was the “AAOHN Cares About HCV” outreach education campaign, which included a webpage/toolkit, a webinar, and email blasts (http://aaohn.org/page/hepatitis-c-resources). The start of the campaign was announced by the AAOHN president to all AAOHN members via email. A new HCV webpage was designed and posted on the AAOHN website and included HCV information, HCV screening guidelines, a health coaching packet, the latest treatment information, links to HCV resources for referrals, and member testimonials regarding HCV outreach activities. Email blasts provided information on the campaign, the AAOHN HCV webpage, HCV risk factors, common HCV myths, and why baby boomers should be screened for HCV. A free 1-hr HCV webinar was offered to all AAOHN members; this webinar was then posted on the AAOHN Academy website for all members to view free of charge.
Data Collection Method
In June 2017, the first survey link was emailed to all active AAOHN members (n = 3,414), excluding student and retiree members. The survey link was open for 14 days, and two email reminders were sent. Email addresses of respondents were kept in a separate, confidential file and used for sending the second survey. In January 2018, the second survey was emailed to 437 AAOHN members who had completed the first survey. The second survey was open for 21 days, and three email reminders were sent.
First Survey
A 36-item web-based survey tool was developed, pilot tested, and revised. For pilot testing, the survey items were reviewed by HCV Work Group members for clarity and comprehension.
Survey 1 had five items that assessed OHN demographic and professional details including gender (male vs. female), age (in years), birth year (those born between 1945 and 1965 vs. all others), race/ethnicity (White vs. all others), and highest level of education (bachelor’s degree [BS/BA] and above vs. all others). Six items assessed OHN occupational and role details including job title (collapsed into three categories: clinical [licensed practical/vocational nurse, registered nurse/OHN, clinical nurse leader, nurse practitioner/advanced practice registered nurse], management roles [case manager, manager/supervisor, chief executive officer/chief], and other [faculty, consultant, or other]); OHN certification (certified occupational health nurse [COHN] vs. all others and certified occupational health nurse specialist [COHN-S] vs. all others); OHN experience (in years); if the current OHN role included providing health care maintenance/preventive services not related to work (Yes–No), ordering of diagnostic labs/tests (Yes–No), and prescribing of medications (Yes–No).
Six questions asked about organization characteristics, including type of industry (working in the health care industry vs. all others [Yes–No]), practice region (Northeast, Midwest, South, and West per U.S. Census designation, analyzed via six contrasts), number of employees (eight categories from less than 500 employees to greater than 50,000 employees), the provision of blood-borne pathogen training at the worksite (Yes–No), if the OHN had attended an HCV continuing education workshop or webinar in the prior 12 months (Yes–No), and if they were currently providing HIV-AIDS awareness education at the worksite (Yes–No).
HCV competence was evaluated by confidence and HCV knowledge. One item assessed how confident the OHN felt in providing HCV education/counseling about HCV risk factors, diagnosis, and treatment to employees (as measured on a 1-5 scale with 1 being “not at all confident” to 5 being “extremely confident”). For purposes of testing their knowledge, 15 questions (with multiple subcomponents, each equal to one point for a total pretest score of 30) assessed the OHN’s current knowledge of HCV; for data analysis, these items were categorized into three subscales: HCV risk factors (14 items), pathophysiology/diagnosis (six items), and treatment (10 items). Items included true–false answers, or multiple choice options. For the risk factor subscale, HCV risk factors were assessed as being true, such as being born between 1945 and 1965, sharing of needles for drug use, receiving blood transfusions before 1992, sharing razors, and vertical transmission, or false, such as sharing food, sitting on toilets, or kissing. For the Pathophysiology-Diagnostics subscale, items assessed, for example, whether HCV is an RNA virus (true), HCV has different genotypes (true), and chronic hepatitis C often has no symptoms (true). For the Treatment subscale, items assessed, for example, whether there is a cure for HCV (true), whether levofloxacin was an HCV treatment (false), that direct acting antiviral medications had very few side effects (true), and that there is no current vaccine to prevent HCV (true).
HCV outreach activities at the work site were assessed with one item (with eight subcomponents, Yes–No), including whether the OHN conducted employee education on HCV (such as offering a class, email alert, newsletter item, etc.), included HCV risk factors in a voluntary health profile questionnaire, ordered HCV testing after a work-related blood-borne pathogen exposure, referred at-risk persons to their primary care provider for HCV testing, advocated for insurance coverage for HCV treatment at the pharmacy benefit level, added an HCV screening prompt to the EMR, referred positive HCV results for further testing and/or linkage to care, and/or counseled employees about HCV results.
Two items assessed if the OHN perceived barriers to HCV screening (Yes–No), and if yes, if there were any of the six barriers to HCV screening (Yes–No), including if HCV risk factors were perceived to be personal, with challenges in maintaining privacy; the OHN did not feel comfortable asking about HCV risk factors, such as IV drug use; overall concerns about maintaining confidentiality in their worksite; there are treatment cost concerns from their employer; their organization does not permit them to screen for HCV; and/or the OHN needed more information about HCV to feel comfortable doing outreach.
Second Survey
The second survey included the 36 items from Survey 1, including the pretest, with one added item measuring the OHN’s participation in the AAOHN HCV Educational Campaign. This item, with four subcomponents (Yes–No), assessed whether the OHN in the prior six months had attended the October 2017 HCV webinar, attended any other HCV education, viewed the AAOHN HCV Webpage, and, if yes, which HCV resources did they access. The additional items were developed and pilot tested by the HCV Work Group for clarity and comprehension.
Data Analysis
All analyses were completed with SPSS version 23. For both surveys, no missing data replacement was conducted. Participants had to have completed at least 33% of 30 HCV knowledge test items in both the pre- and posttest to be included in the analyses.
In this project, using a pre- and posttest design, the HCV knowledge composite score was used to determine competence, in addition to the self-assessed confidence in counseling and educating employees about HCV. Both variables were analyzed as continuous variables.
For descriptive variables from Survey 1 and Survey 2, raw numbers, means, standard deviation, medians, and ranges were calculated. For Survey 1, bivariate analyses were conducted, using one-way analysis of variance or Pearson’s r correlations, comparing sociodemographic, OHN role, and organization factors with composite pretest HCV knowledge scores, to determine whether there were significant differences in pretest scores by variable. The HCV pretest results were analyzed by the three subscales (risk factors, pathophysiology, and treatment), calculating the proportion of correct answers at baseline, with a baseline mean confidence score. A multivariate linear regression model was conducted to determine which factors were associated with higher HCV composite pretest scores at baseline. Sociodemographic, OHN role, and organization variables were included in the linear regression model if they were significantly associated with the HCV pretest score in the bivariate analysis with a p value of .10 or below.
To determine any change in HCV competence between the pre- and posttest, a matched paired t-test was conducted using the pre- and posttest change score for both the knowledge and confidence scores. For HCV knowledge, an item analysis of each test item was additionally conducted, comparing which items did or did not significantly improve over time.
Data on outreach activities from both surveys are compiled as proportions, and a paired sample crosstab analysis was conducted, using the McNemar Test, to determine whether there were any significant increases in outreach activities after the educational intervention. Additional analyses were done to determine whether there was a significant increase or decrease in conducting HCV outreach over the prior 6 months, by those who (a) did not report any outreach activities in their baseline surveys and (b) in those who did report HCV activities in their baseline surveys in June 2017. Data on barriers to HCV screening ascertained from both surveys were also analyzed.
Results
For the first survey, there were 489 responses (13% response rate); 445 completed the HCV knowledge pretest, and 437 completed the pretest and provided their email addresses for the follow-up survey. There was a 25.4% response rate to the second survey with 111 OHNs completing both surveys with pre- and posttest HCV test scores.
OHN Competency in HCV and Factors Associated With Greater Competence
Table 1 describes the sociodemographic and work factors of this baseline sample in the bivariate analyses with HCV pretest scores. The sample was primarily female, averaging 56 years of age, in a role title of OHN, with an average of 17 years of OHN experience, working in either health care or manufacturing settings; 75% of respondents were born in the baby boomer years: 1945-1965. A wide range of industries were represented from across the United States, with 24% working with fewer than 500 employees. Factors significantly associated with higher HCV pretest scores included education (bachelor’s degree [BS/BA] or above), ordering diagnostic tests, prescribing medications, having attended an HCV continuing education program in the prior 12 months, and having higher levels of HCV confidence in educating and counseling employees about HCV. Nurse practitioners and faculty/professors had higher HCV pretest scores, as did those prepared at the Doctorate in Nursing Practice level (data not shown). Those who practiced in the West additionally had higher scores. Those who were certified as a COHN had significantly lower pretest scores; when stratified by type of industry, there were no significant differences in test scores (data not shown). Years of experience were also negatively correlated with HCV pretest scores, that is, more OHN experience was not associated with higher pretest scores.
Sociodemographic, Role, and Industry Characteristics and Mean HCV Pretest Scores
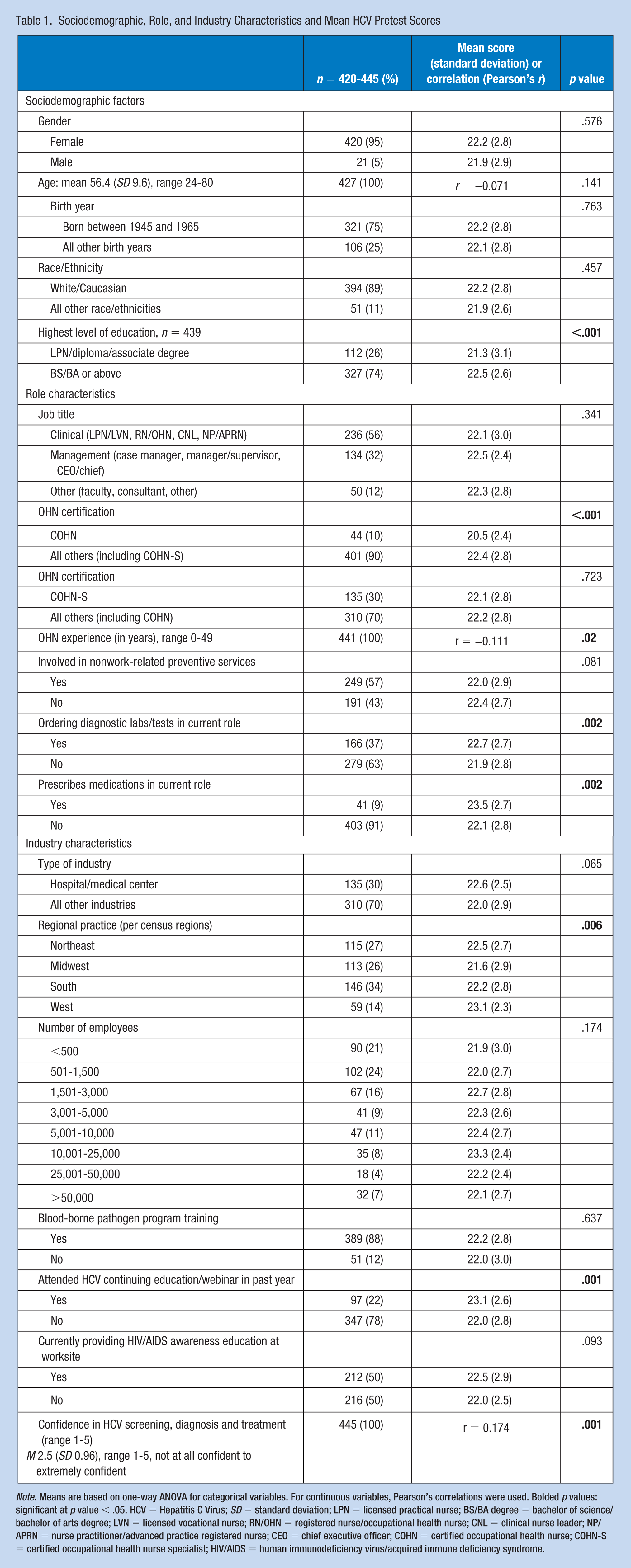
Note. Means are based on one-way ANOVA for categorical variables. For continuous variables, Pearson’s correlations were used. Bolded p values: significant at p value < .05. HCV = Hepatitis C Virus; SD = standard deviation; LPN = licensed practical nurse; BS/BA degree = bachelor of science/bachelor of arts degree; LVN = licensed vocational nurse; RN/OHN = registered nurse/occupational health nurse; CNL = clinical nurse leader; NP/APRN = nurse practitioner/advanced practice registered nurse; CEO = chief executive officer; COHN = certified occupational health nurse; COHN-S = certified occupational health nurse specialist; HIV/AIDS = human immunodeficiency virus/acquired immune deficiency syndrome.
Table 2 describes HCV competency at baseline. For the HCV knowledge pretest, the average test score was 22 of a maximum 30 points, representing 74% correct. There were higher knowledge scores in the HCV risk factor subscale (81%), and lower scores in HCV treatment strategies subscale (68%). For confidence in counseling and educating employees about HCV risk factors, diagnosis, and treatment, the mean score was 2.5 (SD 0.96) on a 1-5 scale, ranging from 1 (not at all confident) to 5 (extremely confident).
HCV Pretest Total and Subscale Scores, n = 445
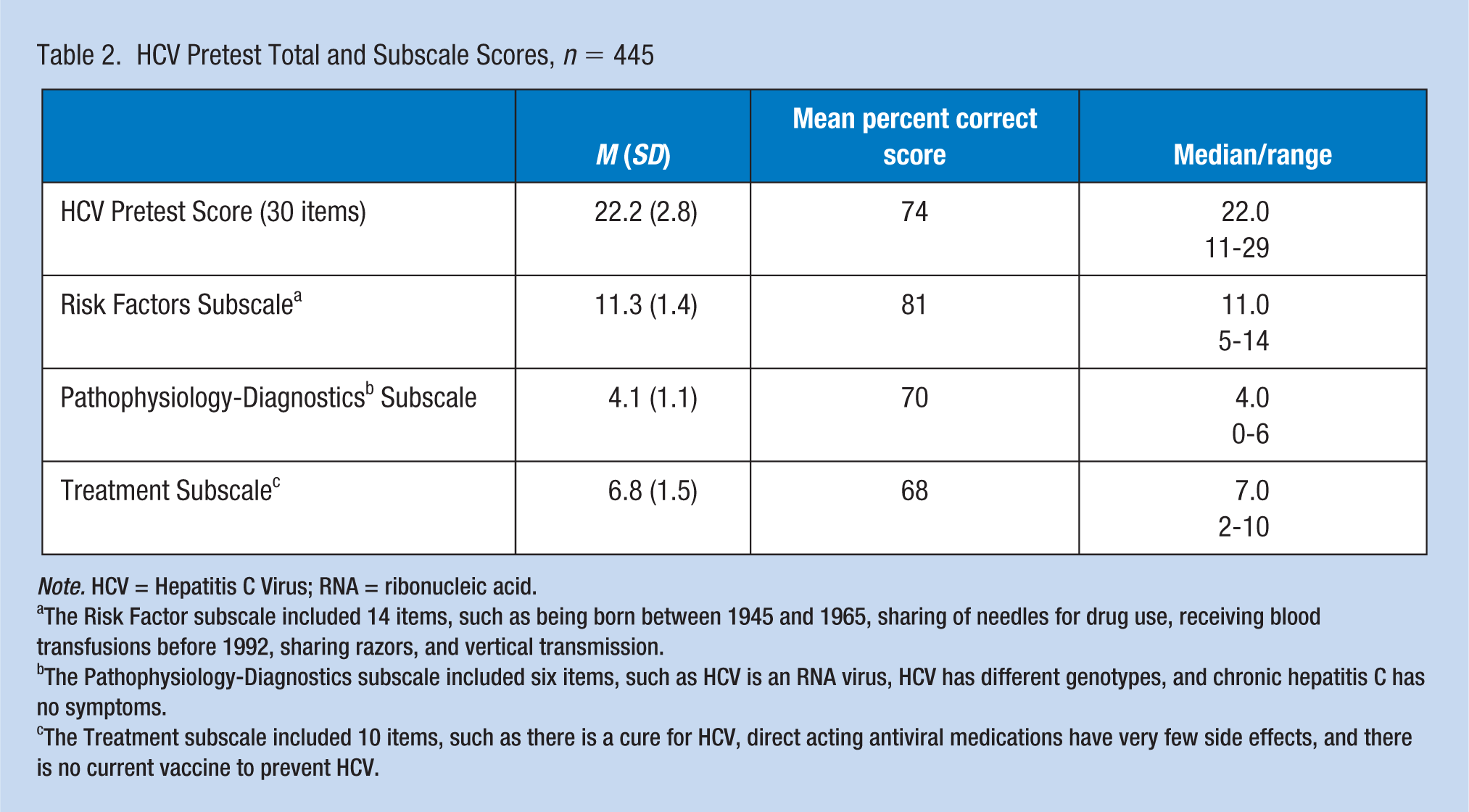
Note. HCV = Hepatitis C Virus; RNA = ribonucleic acid.
The Risk Factor subscale included 14 items, such as being born between 1945 and 1965, sharing of needles for drug use, receiving blood transfusions before 1992, sharing razors, and vertical transmission.
The Pathophysiology-Diagnostics subscale included six items, such as HCV is an RNA virus, HCV has different genotypes, and chronic hepatitis C has no symptoms.
The Treatment subscale included 10 items, such as there is a cure for HCV, direct acting antiviral medications have very few side effects, and there is no current vaccine to prevent HCV.
Table 3 identifies factors associated with higher HCV pretest scores. Eleven factors, which were significant at a p value < .10 in the bivariate analysis, were included in the multivariate regression model: HCV confidence, nursing education, having COHN certification status, working in the health care industry, years of OHN experience, providing nonwork-related health care maintenance/preventive services, ordering diagnostic tests, prescribing medication, having attended an HCV continuing education session in the prior 12 months, providing HIV-AIDS awareness education at their worksite, and practice region. The overall model was significant (p value = .028), with 16.5% of model variance explained by the model. After controlling for other factors in the model, higher HCV confidence (on a 1 to 5 scale), higher nursing education (bachelor’s degree [BS/BA] or above), and if the respondent had attended an HCV education class in the prior 12 months were three factors associated with higher pretest scores, scoring from 0.42 to 0.83 points higher on a 1-to-30 test scale. After controlling for other factors in the model, respondents with COHN certification scored 1.2 points, on average, lower on the HCV pretest (note: COHN-S certification was not significantly correlated with HCV pretest scores).
Linear Regression: Factors Associated With Higher or Lower HCV Pretest Scores, n = 406
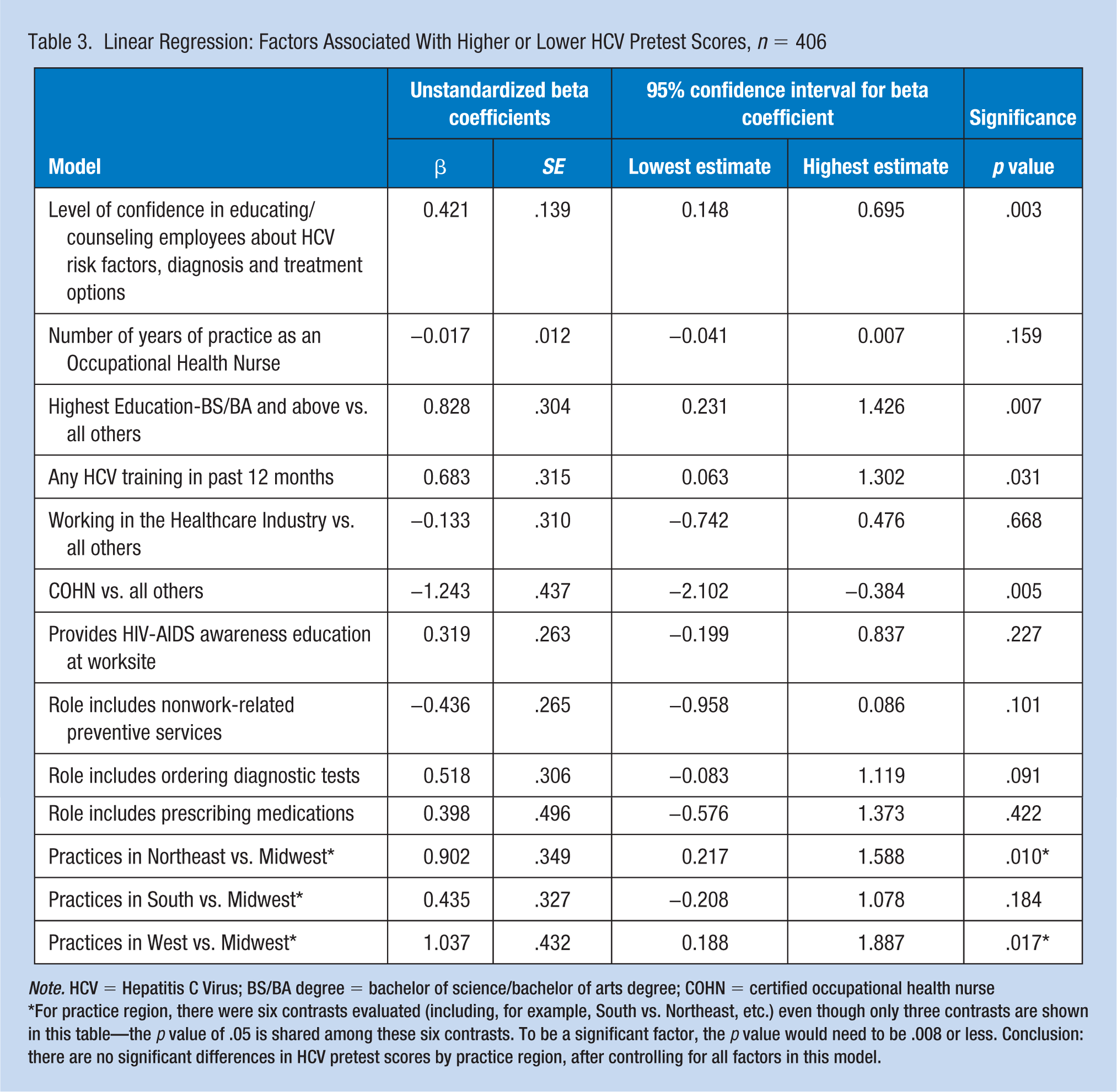
Note. HCV = Hepatitis C Virus; BS/BA degree = bachelor of science/bachelor of arts degree; COHN = certified occupational health nurse
For practice region, there were six contrasts evaluated (including, for example, South vs. Northeast, etc.) even though only three contrasts are shown in this table—the p value of .05 is shared among these six contrasts. To be a significant factor, the p value would need to be .008 or less. Conclusion: there are no significant differences in HCV pretest scores by practice region, after controlling for all factors in this model.
HCV Education Campaign Participation and HCV Knowledge Changes
Of the 111 who participated in posttest Survey 2, in the prior 6 months, 22% had attended the AAOHN HCV webinar, 9% attended another HCV update, and 36% had accessed the HCV webpage resources on the AAOHN website (Table 4). The Frequently Asked Questions resource was accessed most frequently on the HCV webpage.
HCV Educational Activities Since June 2017,n = 111
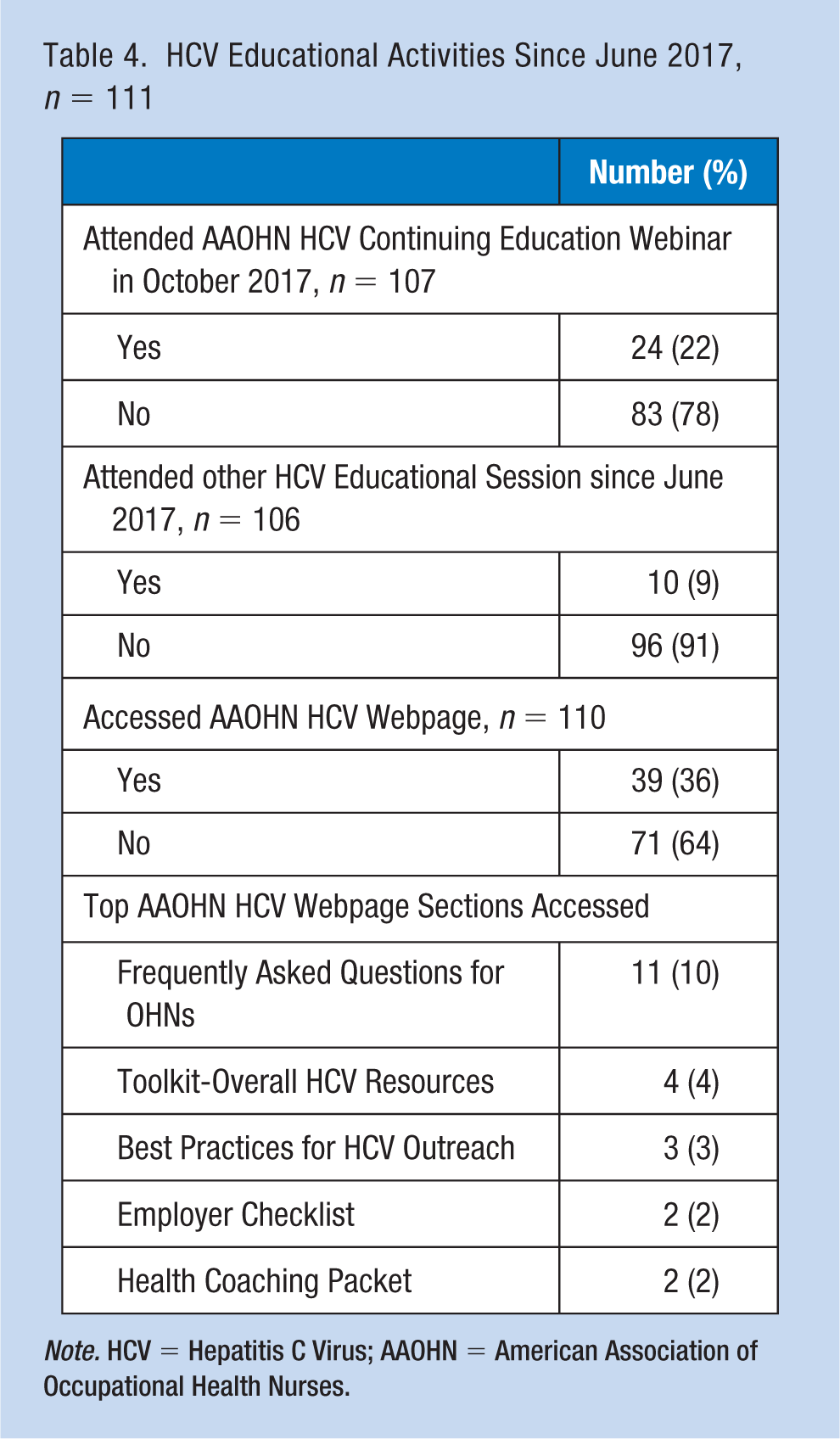
Note. HCV = Hepatitis C Virus; AAOHN = American Association of Occupational Health Nurses.
The sociodemographics of Survey 2 participants are summarized in Table 5; these Survey 2 respondents were not significantly different from the other participants at baseline (data not shown). For pre- and posttest changes in HCV knowledge, there were no significant changes in test scores (Table 6), even after controlling for participation in the AAOHN webinar (data not shown). For subscale scores, there were modest improvements in subscale scores (1 percentage point improvement in the risk factor subscale, and 2 percentage point improvements in treatment strategies), but these were not significant changes. Of note, two test items significantly improved in this sample: (a) the need to screen baby boomers for HCV, correctly answered by 95% in the pretest, moved to 100% in the posttest (p = .025), and (b) there is a cure for HCV, correctly answered by 64% in the pretest, improved to 74% in the posttest (p = .027; data not shown). Confidence in educating and counseling employees about HCV increased from a baseline mean of 2.6 to 2.9 (on a 1-5 scale), almost reaching statistical significance (p = .052).
Participants in Surveys 1 and 2: Sociodemographic, Role, and Industry Characteristics, June 2017, n = 111

Note. LPN = licensed practical nurse; BS/BA degree = bachelor of science/bachelor of arts degree; LVN = licensed vocational nurse; RN/OHN = registered nurse/occupational health nurse; CNL = clinical nurse leader; NP/APRN = nurse practitioner/advanced practice registered nurse; CEO = chief executive officer; COHN = certified occupational health nurse; COHN-S = certified occupational health nurse specialist; HCV = Hepatitis C Virus.
HCV Pretest and Posttest Scores and Level of Confidence Changes
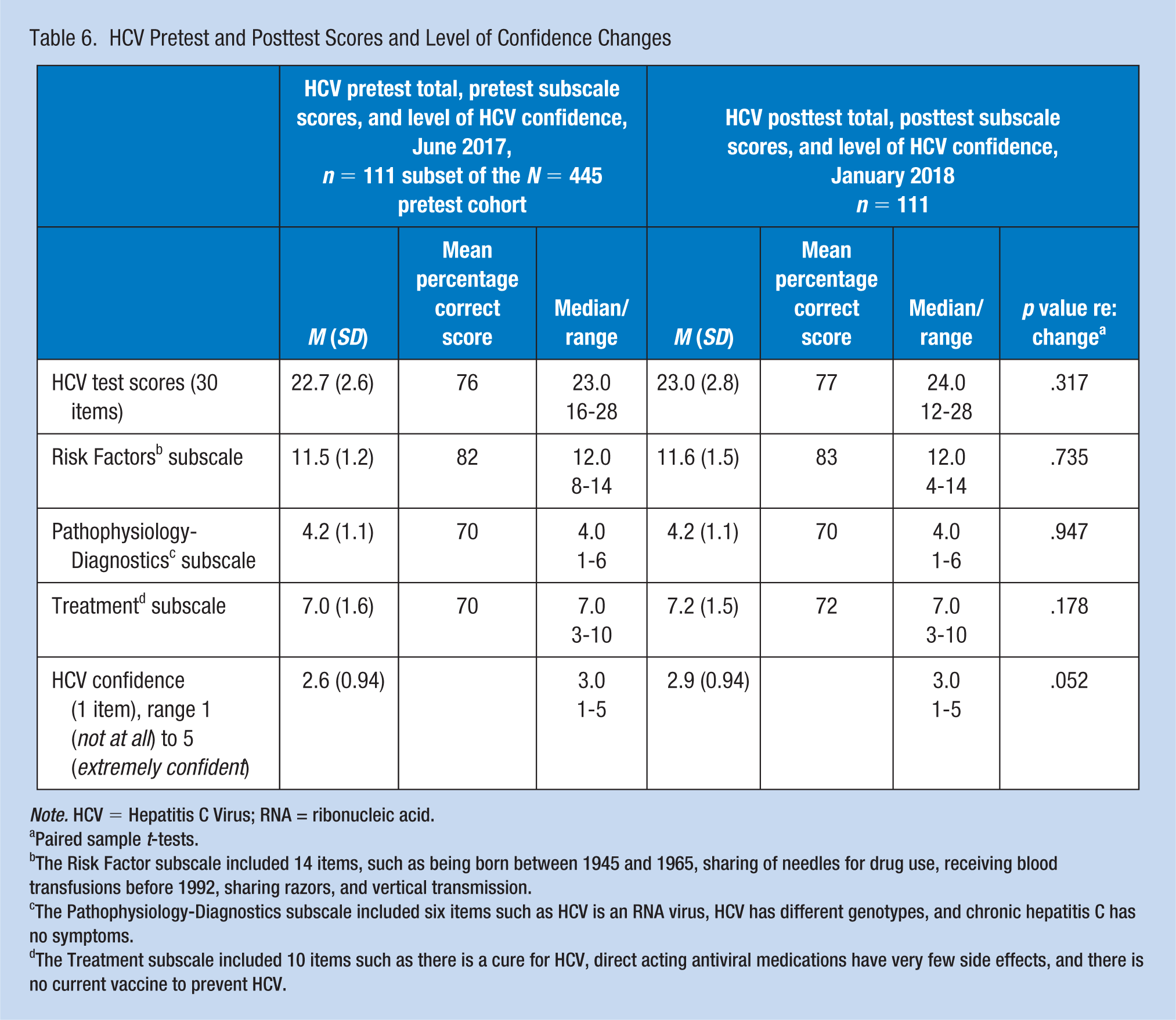
Note. HCV = Hepatitis C Virus; RNA = ribonucleic acid.
Paired sample t-tests.
The Risk Factor subscale included 14 items, such as being born between 1945 and 1965, sharing of needles for drug use, receiving blood transfusions before 1992, sharing razors, and vertical transmission.
The Pathophysiology-Diagnostics subscale included six items such as HCV is an RNA virus, HCV has different genotypes, and chronic hepatitis C has no symptoms.
The Treatment subscale included 10 items such as there is a cure for HCV, direct acting antiviral medications have very few side effects, and there is no current vaccine to prevent HCV.
HCV Outreach Activities and Impact of HCV Education Campaign
At baseline, 59% of the respondents reported at least one HCV outreach activity at their organization within the prior 12 months (Table 7). The most common outreach activities were (a) ordering HCV testing after a work-related blood-borne pathogen exposure (30%), (b) referring at risk employees to their primary care providers for HCV screening (23%), (c) employee education regarding HCV (23%), and (d) counseling for HCV results (22%). At postsurvey, 55% of the sample reported HCV outreach activities in the prior 6 months (i.e., since June 2017 Survey 1) including (a) ordering HCV testing after a work-related blood-borne pathogen exposure (29%), (b) employee education for HCV (23%), (c) counseling for HCV results (22%), and (d) referral of at-risk employees to their primary care providers for HCV screening (14%). Overall, those who completed Survey 2 had greater HCV outreach participation at baseline, when compared with the whole cohort (60% vs. 42%; data not shown). The majority of those who conducted outreach completed from one to three outreach activities (data not shown). Of the 111 who had completed pre- and posttest surveys, 44 (40%) had not reported any outreach activities in their baseline surveys, but 10 of these respondents reported new HCV outreach in their January 2018 surveys. Sixty-seven (60%) of the 111 reported HCV outreach in their baseline surveys; 51 of them reported continued outreach in their January 2018 surveys. These changes in HCV outreach activities were not statistically significant (p = .327; data not shown).
HCV Outreach Activities
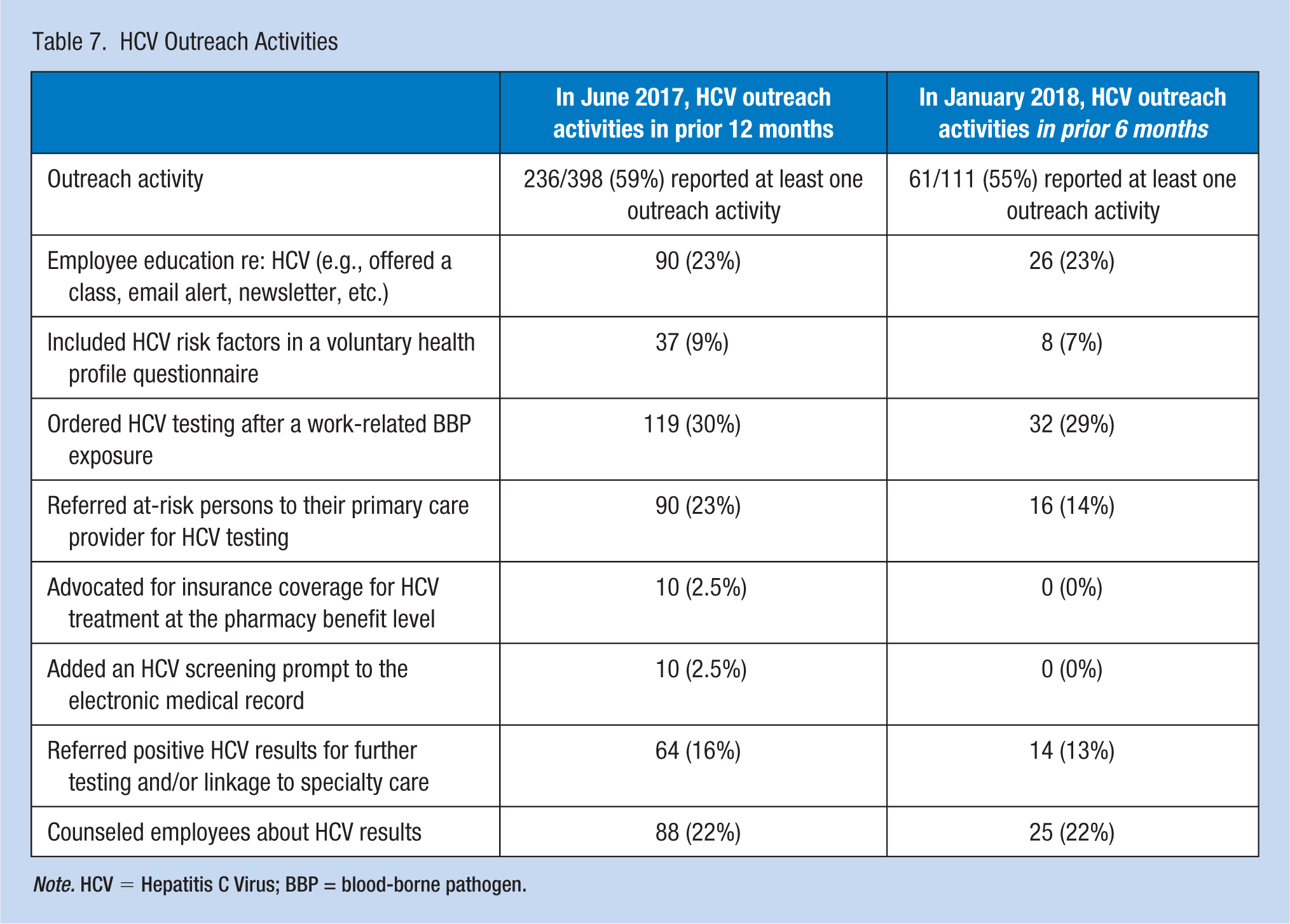
Note. HCV = Hepatitis C Virus; BBP = blood-borne pathogen.
Barriers to Implementing HCV Outreach Activities
Table 8 outlines respondent perceptions of barriers to HCV outreach in their organizations. Of note, approximately half of respondents reported no barriers to conducting HCV outreach in their organizations. Of those who reported barriers, the most prevalent (50%-53%) barrier chosen was “my organization does not permit Occupational Health to screen for HCV.” Additional barriers included “not assessing personal risk factors due to privacy concerns” and “needing additional knowledge about HCV to feel more comfortable in conducting HCV outreach.” “Maintaining confidentiality” and “costs of treatment” were more prominent barriers identified in the Survey 2 posttest responses. Potential OHN discomfort in assessing risk factors for HCV was rarely identified as a barrier to HCV outreach at baseline and in Survey 2 posttest respondents.
Perceived Organization Barriers to HCV Outreach
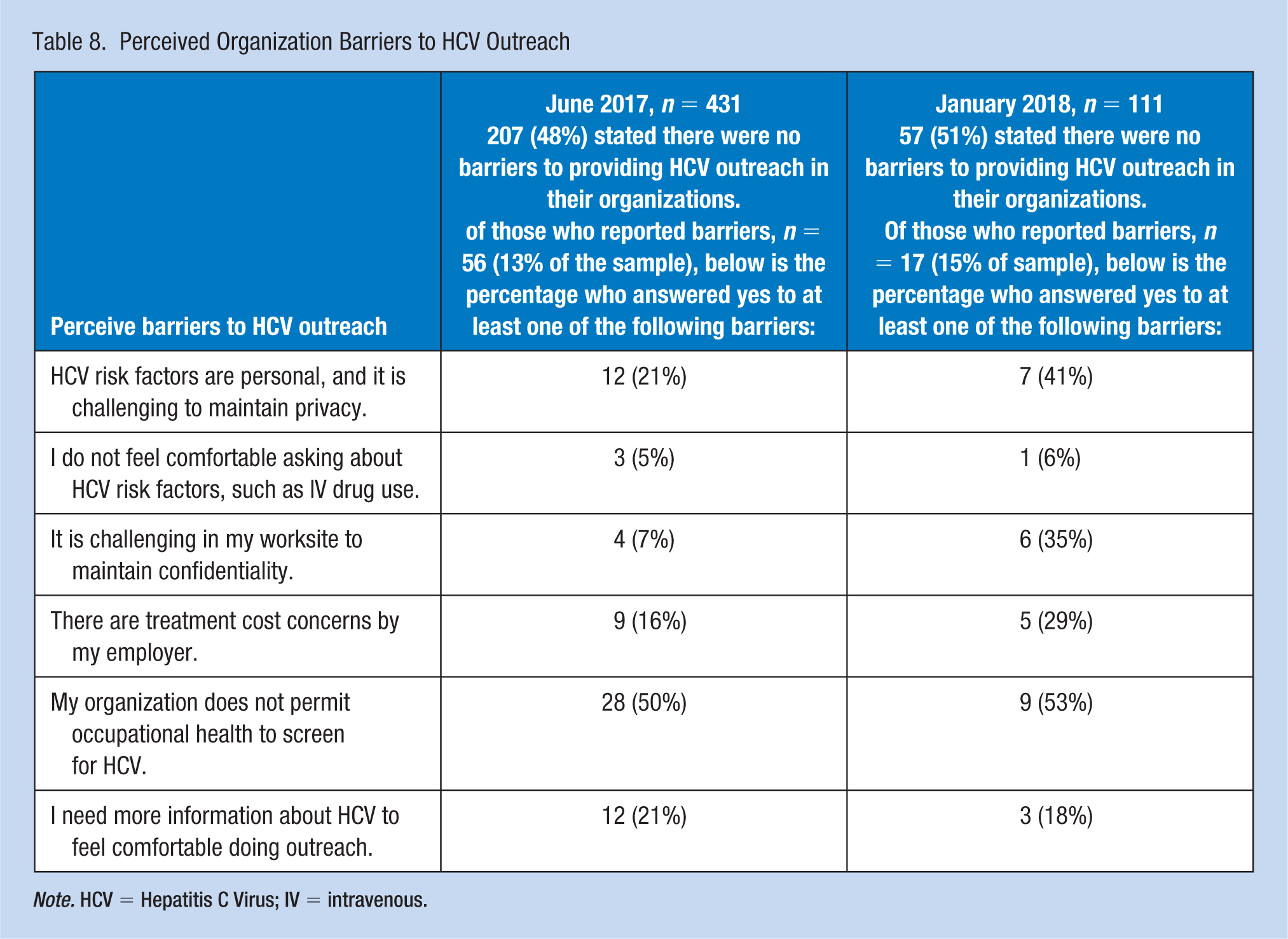
Note. HCV = Hepatitis C Virus; IV = intravenous.
Discussion
This is the first quality improvement project to assess and evaluate HCV knowledge within the OHN setting. Although total HCV knowledge scores did not improve significantly from pre- to posttest, there were 10 OHNs who reported no HCV outreach at baseline, but did report HCV outreach after HCV education. This is in addition to those who continued to be involved in HCV outreach activities. Furthermore, knowledge regarding HCV risk factors and HCV treatment improved in the posttest, although not statistically significant. HCV risk factor knowledge levels improved from 82% to 83%, and HCV treatment knowledge improved from 70% to 72%. In addition, OHNs felt more confident in their HCV knowledge after AAOHN HCV Education Outreach interventions. Pre- to posttest OHN HCV confidence level improved from 2.6 to 2.9 (1 to 5 Likert scale with 5 being extremely confident and 1 being not confident), which almost reached statistical significant (p = 0.52).
Limitations and Strengths
The main limitation of this study is generalizability to the larger AAOHN population. The baseline sample, although representative in terms of gender, age, education, and industry profile, represented only 13% of the membership. In addition, the large decrease in respondents from those who took both pretest survey (n = 445) and posttest survey (n = 111) is a limitation. Change in score from pre- to posttest can only be ascertained from 111 respondents, and only 31% had attended any HCV education between pre- and post-testing. With less attrition between surveys and greater participation in the webinar, the scores may have been different. The large decrease in respondents can be due to the release of our posttest survey in January after the holiday season. In addition, the limited amount of time between the launch of the HCV Outreach education intervention and the posttest (3 months) may have affected the outcome score of the posttest survey.
The primary strengths of this study include baseline assessment of OHN knowledge of HCV and evaluating gaps in this knowledge. It is imperative to recognize the importance of keeping up-to-date with HCV screening and treatment practices, and to highlight specific HCV knowledge areas to address in future HCV Outreach interventions. Knowledge gaps (with scores less than 80%) were seen in all three sections (risk factors/transmission, diagnostic testing, and treatment). For example, some of the questions with scores less than 80% include the following: Vertical transmission and sexual intercourse are HCV risk factors, HCV screening of pregnant women is not a current CDC recommendation, the HCV antibody test is the test to use for screening, and direct acting antivirals have a low side-effect profile.
Factors associated with higher HCV knowledge pretest scores included being prepared with a BS/BA degree or above, having attended an HCV continuing education class/webinar in the prior 12 months, and perceiving higher confidence in educating/counseling employees about HCV risk factors, diagnosis, and treatment options. Ongoing professional education about HCV is critically important, and will continue to be an AAOHN priority going forward. Additional subsequent HCV education interventions included two concurrent sessions on HCV offered at the annual AAOHN conference in April 2018.
Being a COHN was associated with lower pretest scores. This was not a finding of those certified as occupational health nurse specialists, which requires a BS/BA degree or above (in addition to other requirements) to be certified as a COHN-S. In addition, there were no significant differences in mean test scores for COHN respondents by industry (health care industry vs. all others). Therefore, being a COHN serves as a proxy variable for the different educational requirements for these two certifications; those prepared as a COHN were significantly more likely to be educated with less than a BA/BS degree (p = .000). There were only 44 COHN respondents, representing 10% of the sample; therefore, this finding may not be generalizable to other COHNs.
Besides identifying HCV knowledge gaps, this study identified current HCV Outreach activities by AAOHN members. The HCV Outreach activities ranged from general HCV education to more specific activities, such as counseling employees about their HCV test results. Underutilized outreach strategies are EMR prompt reminders for HCV screening in occupational health clinical settings.
Multiple factors contribute to whether or not a person at risk for HCV will be screened. At baseline, 13% of respondents identified barriers to conducting outreach in their worksites. Identified barriers included not being permitted to screen for a nonwork-related health condition, such as HCV, due to their primary focus on occupational health, and a lack of HCV knowledge. Additional barriers included discomfort with asking employees questions related to personal risk factors, privacy, and confidentiality, and treatment costs. These findings may be based in the OHN’s knowledge of Federal standards protecting employees, families, and retirees, an organization’s priority on focusing only on job-related risks, a lack of knowledge regarding direct and indirect costs associated with not screening and treating HCV, or the OHN’s personal values and comfort with discussing risk factors. Yet in this study, 48% of respondents stated specifically that there were no HCV outreach barriers in their organizations. The fact that many AAOHN members do not see barriers to HCV screening in their organizations provides a future opportunity for enhanced HCV outreach to employees, retirees, and dependents.
Implications for OHN Practice
OHNs have a unique opportunity to educate thousands of employees and retirees in the importance of HCV screening for those people at risk, and for those born between 1945 and 1965 to have at least one baseline screening HCV antibody test. OHNs routinely provide employee education regarding the need for health screening and prevention of chronic disease, and therefore an education seminar on HCV screening and advances in treatment would be a great addition to their wellness/health promotion educational program schedule. These types of seminars could be done in conjunction with celebrating World Hepatitis Day. If OHNs’ organizations are already providing preventive health screening of employees, then OHNs could encourage inclusion of HCV antibody screening for at-risk employees. The OHN must have a screening process that maintains the privacy of personal health information including consents for confidential release of records and referral of positive findings to an employee’s personal health care provider for further evaluation and follow-up. OHNs can add HCV education posters and pamphlets to OH clinic waiting areas and add hepatitis screening questions to their current health risk profile questionnaires. Adding an EMR prompt to remind OHNs to review HCV risk factors during employee OH visits will prompt OHNs to counsel workers to pursue HCV screening with the OH clinic or their primary care providers. OHNs can also enhance the HCV content in current annual blood-borne pathogen trainings and ensure that HCV screening is on the list of health care maintenance recommendations for baby boomers. OHNs can identify opportunities to influence their organization’s leaders to include HCV screening and treatment during employee and family health plan benefit design, and advocate for full drug treatment coverage to cure HCV.
OHNs need to additionally understand the regulatory differences related to a health savings account (HSA) and a health reimbursement arrangement (HRA) and other tax-incentive health plan programs to guide the development and scope of primary care worksite services such as HCV screening and consultation (Pollitz & Rae, 2017; Sherman & Click, 2007). For example, if an employee is covered by a health plan, which is combined with an HSA, the employer cannot provide free personal health care services at the worksite (Sherman & Click, 2007). Although HCV screening is considered a preventive service, to comply with Internal Revenue Service (IRS) regulations, OHNs should determine the scope of an HCV screening, counseling, and referral program in consultation with their employer’s benefits organization and attorneys.
Worksite Personal Health Care Services, Nondiscrimination, and Privacy Laws
Compliance with Federal standards to prohibit employment discrimination based on health status and to protect the privacy of personal health information need to be considered when planning for a worksite HCV education/counseling, screening, and referral program. The Americans With Disabilities Act (ADA) and the Genetic Information Nondiscrimination Act (GINA) protect employees and their families from employment discrimination based on health status when asked to disclose personal health information, including genetic information, as voluntary participants in workplace wellness programs (Pollitz & Rae, 2017). The Health Insurance Portability and Accountability Act (HIPAA) standards protect the privacy of an employee’s personal health information; the ADA and GINA also include certain privacy protections (Pollitz & Rae, 2017). The OHN role in protecting privacy of personal health information is of paramount importance in worksites.
Conclusion
The HCV Education Outreach study to assess and evaluate OHN HCV competence and outreach activities is the first of its kind. Differences in OHN HCV competence (knowledge and confidence) were evaluated. Factors such as being educated at a bachelor’s degree or above, having attended a continuing education/webinar on HCV in the prior 12 months, and having confidence in HCV counseling/education were associated with higher HCV knowledge pretest scores. Although the HCV education campaign intervention did not result in significant overall test score improvements, there were gains in confidence and certain knowledge areas, for example, that a cure for HCV exists. The majority of OHN respondents (59%) conducted at least one HCV outreach activity in their organizations, and approximately half did not identify current organizational barriers to conducting HCV outreach. In addition to ongoing education on HCV disease, screening, and treatment, it is imperative that OHNs understand their employer’s health plan, including benefit coverage for HCV treatment and management, and the regulatory and legal influences that may create barriers when recommending worksite HCV screening, counseling, and referral to primary care providers and specialists.
The case has been made for early intervention in the screening and treatment of HCV as it decreases HCV-related health care costs, patient morbidity, and mortality (Surjadi, 2018). Based on an employer’s interpretation and legal consultation related to Federal nondiscrimination and privacy laws and regulations, OHNs HCV outreach efforts may include employee education and awareness through confidential and voluntary worksite screening, consultation regarding HCV test results, and/or primary care or specialty referral. With continued HCV education, OHNs are uniquely positioned to influence business and employer benefits leaders of the importance of workplace HCV education, screening, and treatment referral, and the provision of health insurance plans that cover HCV treatment.
Footnotes
Acknowledgements
The authors wish to thank and acknowledge funding from the National Viral Hepatitis Roundtable (NVHR), and the support of Tina Broder (NVHR). In addition, the authors wish to acknowledge and thank Kathleen Buckheit, Jessica Scott, Nicholas Wade, and Jennifer Beining for their work on the American Association of Occupational Health Nurse (AAOHN) hepatitis C virus (HCV) Work Group, and Steven Paul, PhD, for statistical consultation.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Miranda Surjadi is part of the Speakers Bureau at Gilead Sciences.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Miranda Surjadi is an associate professor at the University of California, San Francisco, School of Nursing Adult-Gerontology Primary Care Nurse Practitioner Program.
Beverly Nuchols is a nurse practitioner at Sutter Health Bay Area specializing in Employee Health/Occupational Medicine.
Denise Souza, MSN, ANP-BC, FAAOHN, received her graduate education from the University of California San Francisco in 1994, and has worked in manager, clinician, and faculty roles in manufacturing, university and hospital occupational health settings, including working as a nurse practitioner in primary care settings as well. Her interests include global and environmental health, in addition to hepatitis C.
Lori Wolfe is a nurse practitioner at Corteva Agriscience.
Barbara Burgel is a fellow of AAOHN and the American Academy of Nursing, and is professor emeritus at the University of California, San Francisco, School of Nursing Occupational and Environmental Health Graduate Nursing Program.