
Abstract
Transitioning into independent professional practice may be a difficult and trying process for newly licensed nurses, who may be at risk for burnout and quitting their jobs. Issues related to new nurses’ well-being at work may also impact their personal lives. Using thematic analysis within the framework of Total Worker Health, this study examined factors related to the overall work, safety, and health of newly licensed nurses that should be addressed in work environments to promote well-being and prevent burnout and attrition. The main component of Total Worker Health is to find and understand the relevant issues that lead to safety and health risks in the workplace and affect workers’ well-being at work and home. The overarching concept of Balance between Work and Life included three main themes: Health, Work Environment, and Learning to Be (a nurse). These themes with their subthemes described the difficulties participants had in balancing the complex interactions of work conditions and social life changes during the transition from student to professional nurse. Participants identified new physical health problems, mental health challenges, physical violence, lack of support structures at work, and alterations in family and friend relationships. However, they also developed protective factors from new connections with coworkers. These findings showed that new nurses are vulnerable to many factors at home and work that affect well-being and may lead to burnout and attrition. Implications include interventions at work that focus on health promotion, group support, and safety risk prevention through occupational nurse management.
With a looming nursing shortage and a current registered nurse (RN) vacancy rate of 8.2% and growing, U.S. nursing education programs have committed to educating more nurses (American Association of Colleges of Nursing [AACN], 2017). In 2017, 230,000 RNs were newly licensed (National Council of State Boards of Nursing, 2018; NSI Nursing Solutions Inc., 2018). The large number of novice RNs in workplaces generates concern regarding occupational health and safety. Previous studies provide evidence that occupational injuries and fatalities are greater in newly licensed nurses, whose inexperience, limited training, and erratic work schedules may contribute to them being at increased risk (Breslin & Smith, 2006; Stimpfel, Brewer, & Kovner, 2015).
Background
In the workplace, RNs face high levels of stress, low levels of control, challenging work climates, and burnout impacting performance, safety, and work-life balance (Hanna & Mona, 2014; Mark & Smith, 2012; Wu, Fox, Stokes, & Adam, 2012). Among newly licensed nurses, an imbalance in work-life stems from poor job fit and work demands that interfere with their personal life, which in turn contributes to poor or unsafe work performance, emotional exhaustion, family conflicts, burnout, and attrition (Boamah & Laschinger, 2016). These issues have been attributed, in part, as to why almost 20% of newly graduated nurses quit within their first year of employment, and up to 33% quit by their second year. This attrition costs employers up to US$82,000 per nurse (Kovner, Brewer, Fatehi, & Jun, 2014; NSI Nursing Solutions Inc., 2018). These high dollar figures do not account for workflow disruption and impact on staff morale.
The demands facing new nurses in balancing work and life encompass physical, biological, and psychosocial health, and appropriately relate to the Total Worker Health (TWH) program, recently introduced by the National Institute for Occupational Safety and Health (NIOSH). The underlying tenet of the TWH program is to “integrate protection from work-related safety and health hazards with promotion of injury and illness prevention efforts to advance worker well-being” (NIOSH, 2015), with a purpose to develop a healthier workforce in all areas of employment. TWH is an approach to link all health-related services within a place of employment, and to find strategies to improve worker health and decrease employee loss by including factors related to the workplace (such as safety), employment issues (such employment patterns, demographics), and the worker (including the social environment and work-life balance) (Shill & Chosewood, 2013).
With increased rates of safety issues and burnout, there is a need to discover how the process of transitioning from school to work affects newly licensed RNs. The purpose of this qualitative descriptive study was to examine and describe the transition of newly licensed nurses in to practice within the context of TWH.
Method
We conducted a descriptive qualitative study, using thematic analysis, to explore the experiences of newly licensed novice RNs and their transition to practice, while working in health care facilities in Washington and Oregon. The targeted population were the RNs who received their nursing license and graduated within 2 years of the start date of the study. Focus groups and key informant interviews were conducted from September 2015 to August 2016.
Participants
Using purposive sampling, focus group participants and key informants were recruited through nursing education alumni offices using email invitations, word of mouth from faculty through researchers’ professional contacts in health care, and social media advertisements. Interested nurses were asked to contact the study coordinator, who provided information about the study. Potential participants who were interested, but could not attend a focus group were offered the option to participate in a key informant telephone interview. Inclusion criteria included novice RNs who graduated from a nursing program and received their RN license within 2 years of the focus group or interview, the ability to speak English, and the ability to attend a focus group in select cities in Oregon or Washington or participate in a telephone call as a key informant. Washington State University’s institutional review board determined that this study was exempt from human subjects review; however, verbal group consent was obtained for focus groups and individual consent from key informants was obtained to enhance trust and provide a means to ask questions about the study.
Data Collection
Prior to conducting the focus groups and key informant interviews, participants were given an explanation of the study, they provided verbal consent to participate, and completed a short demographic form. Descriptions of possible work-related issues such as fatigue or safe staffing that related to personal health during transition from a student to a professional nurse were described as topics for discussion as found in the TWH graphic: “Issues Relevant to Advancing Worker Well-being Through Total Worker Health” (NIOSH, 2015). Experienced qualitative researchers interviewed focus groups and key informant participants which were digitally recorded and notes were taken as backup. Audio recordings were professionally transcribed and de-identified. Focus groups interviews took 60 to 90 min and key informant interview telephone calls took 45 to 60 min. All participants received a US$40 gift card for participation in the study.
Semi-structured interview questions were developed from concepts found in the TWH graphic that aligned with those in new nurse transition literature. The TWH graphic lists areas of concern to worker health and safety including, (a) factors found within work places, and (b) factors that can be affected by work (NIOSH, 2015). Issues listed in the graphic include control of hazards and exposures, work organization, leadership, workforce policies, demographics, compensation and benefits, employment patterns, and environmental and community supports. Questions developed for the focus groups included defining health in general, health at work, and health outside of work. Although other questions regarding workplace policies and leadership, organization, and social support were developed, they were not used since those issues came up spontaneously in all of the focus groups using the three health questions. The first general question was “How do you describe health?” with probes that asked for clarification or further explanation. The follow-up question asked was “What is health at work?” with probes to ask about the term occupational health as well as safety, and risks. The final question of “What is health outside of work?” included probes to ask about relationships and home life.
Key informant interviews were conducted after the focus groups, guided by subthemes from the analysis from the focus groups, to elicit additional information and validate the developing patterns. Field notes were taken throughout focus groups and interviews and used to help develop codes and sub-themes. Data collection continued until no new data were obtained and no new codes identified, indicating data saturation.
Data Analysis
Transcripts were analyzed using teams and deductive thematic analysis according to Braun and Clarke (2006), which allows for exploration of descriptions and meanings of participants while situating findings in a broader social context (TWH). Deductive thematic analysis uses a predetermined framework to analyze data; in this case, concepts from the TWH graphic were used to inform the coding process, in addition to the interview questions (NIOSH, 2015). Although a list of possible TWH issues are listed in the graphic, it is recognized that not all issues are identified. As an example, the theme “Learning to Be” contained new elements not found in the graphic.
Transcripts and notes taken during interviews were read and reread, and ideas noted about possible codes related to framework concepts. Using initial ideas for possible codes, transcripts were then individually coded. Codes were entered into a codebook, created for code definitions and theme development (Saldaña, 2009). Although codes mostly aligned with concepts from the framework, subthemes, and later themes were allowed to emerge on their own to be able to capture any issue not found in the TWH graphic. Codes from each transcript were linked to quotes and field notes, and kept together as nodes using QSR NVivo 11©. Nodes were compared and sorted into potential themes with subthemes, and thematic maps made to examine relationships. Themes were compared with each other to ensure that each theme reflected distinct meanings, and reviewed with data from the texts for identification of patterns. Rigor was shown by using member checking with individual key informants, inclusion of multiple members on the research team to ensure agreement of themes, and utilization of decision and audit trails.
Findings
Overall, 34 newly licensed RNs participated in this study. Twenty-nine RNs participated in 4 focus groups, ranging from 4 to 12 members, held in Spokane, Tri-Cities, and Portland. Five additional newly licensed nurses in the Puget Sound region of Washington were contacted and participated in individual key informant interviews. A total of 27 (84%) participants fully completed the demographics forms. Among the participants who shared demographics, most were 18 to 25 (44%) or 26 to 35 (31%) years of age, female (79%), and Caucasian (91%) (Table 1). Most participants worked in urban acute care hospitals (84%) and held bachelor of science in nursing (BSN) degrees (72%).
Self-reported Demographic and Employment Characteristics of Focus Group and Key Informant participants. (N = 34)
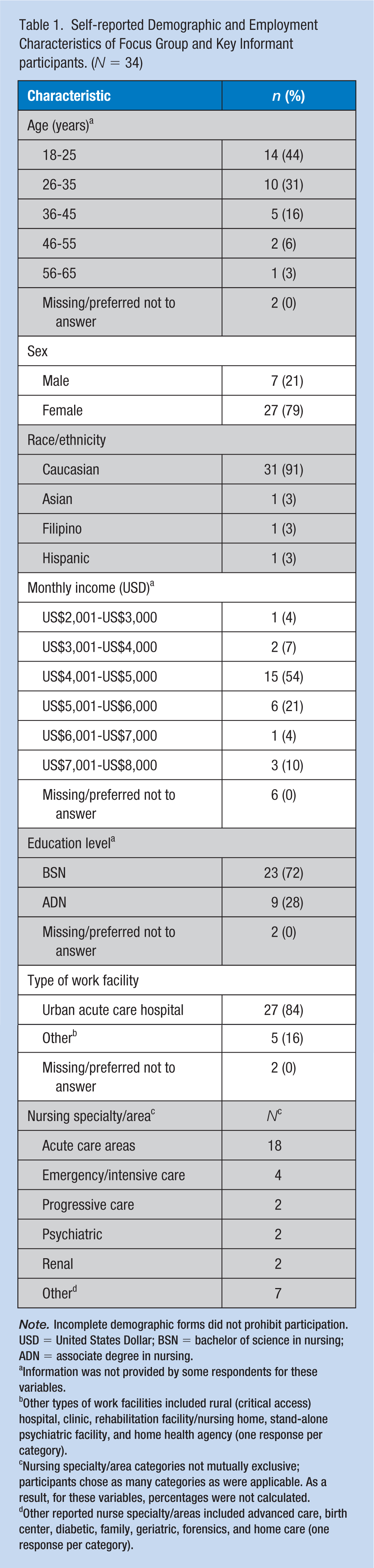
Information was not provided by some respondents for these variables.
Other types of work facilities included rural (critical access) hospital, clinic, rehabilitation facility/nursing home, stand-alone psychiatric facility, and home health agency (one response per category).
Nursing specialty/area categories not mutually exclusive; participants chose as many categories as were applicable. As a result, for these variables, percentages were not calculated.
Other reported nurse specialty/areas included advanced care, birth center, diabetic, family, geriatric, forensics, and home care (one response per category).
Key Themes
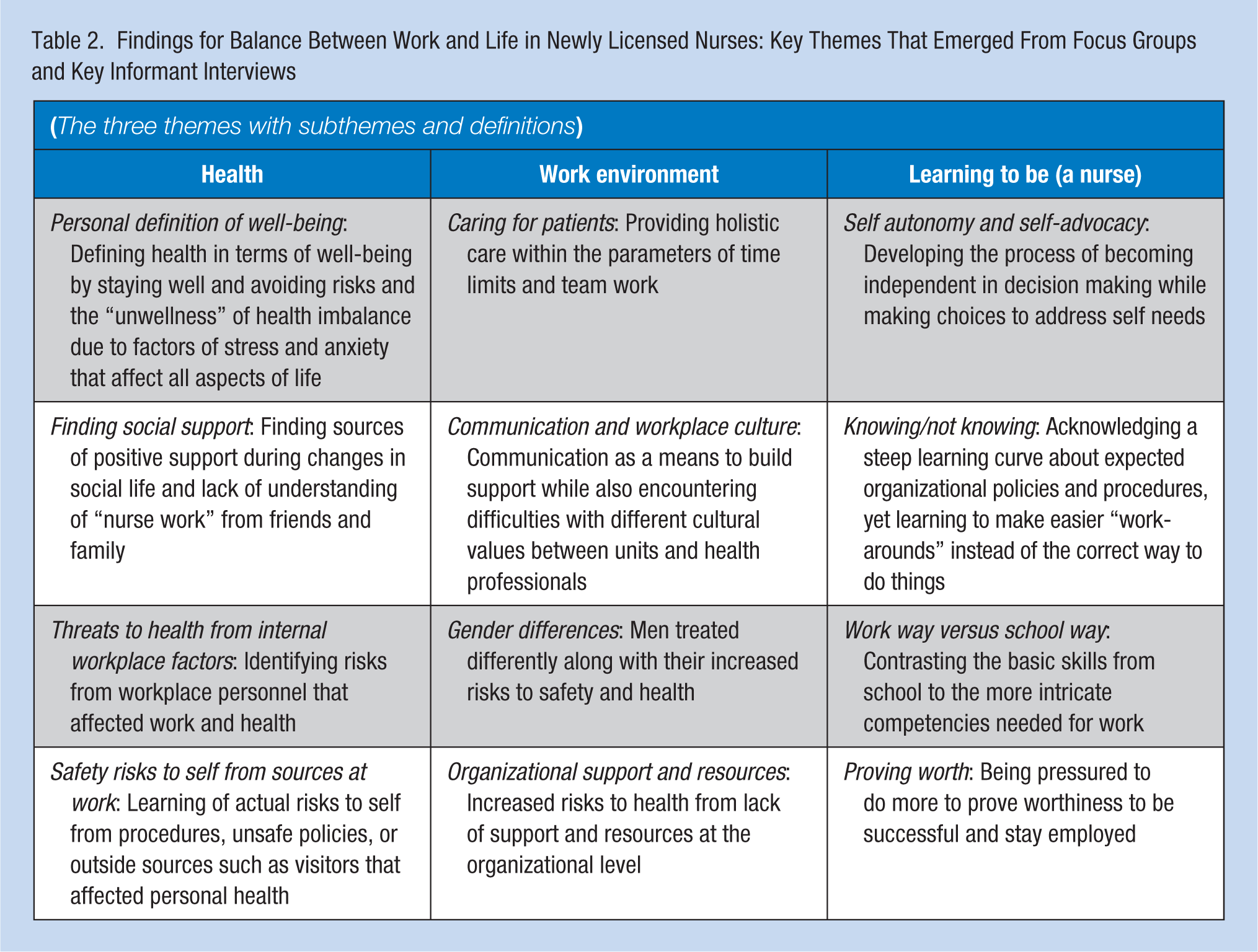
The overarching concept of Balance between Work and Life in Newly Licensed Nurses described the participants’ experiences and health perceptions of transition into practice. Three areas were identified as key themes with subsequent subthemes: Health, Work Environment, and Learning to Be (knowledge transition) (Table 2).
Findings for Balance Between Work and Life in Newly Licensed Nurses: Key Themes That Emerged From Focus Groups and Key Informant Interviews
Health
The key theme, “health,” included participants’ overall personal and social health. This theme encompassed the following four subthemes: (a) personal definition of well-being, (b) finding social support, (c) acknowledgment of occupational threats to health from internal personnel workplace issues, and (d) safety risks to self from sources at or due to work.
Personal Definition of Well-Being
Holistic balance in well-being was important to participants as they recognized the many dimensions of personal health and occupational health: physical, mental, psychological, emotional, and spiritual. Personal health was positively defined as being well and able to do what a person wanted to do. In contrast, occupational health was defined as avoiding risks: “Whenever I hear occupational health, I think of on-the-job injuries.” For a few participants, well-being implied finding time for self-care outside of work and learning new healthy habits. However, participants more frequently talked about “unwellness,” a state of health imbalance, than well-being. Unwellness included disrupted sleep patterns, exhaustion, stress, anxiety, poor nutrition, physical conditions, or burnout, all of which affected work performance and home life. Sleep issues were the most problematic, and participants reported using some type of sleeping agent or alcohol to sleep, or stimulants to stay awake at work. One participant shared, “I’ve never been a drinker, ever. Once a month maybe. I drink more since I got this job.” On-the-job stress caused many participants to feel anxiety and burnout, such as one nurse discussing having to give herself a pep talk on the way to work, “I’m not saying that I ever have like suicidal ideations or anything, but I just remember thinking-I could turn my car into the barrier and then I wouldn’t have to go to work.” However, all the participants agreed that personal well-being was affected by their occupation: “I think as nurses, we tend to take care of others more than we do ourselves.” To help regain work-life balance, another stated, “It’s important to keep your own health in mind, and not just be solely focused on your patient all the time 24/7. It’s a hard balance to find sometimes.”
Finding Social Support
Participants defined social support as encouragement, understanding, and assistance from family and friends. They did not anticipate that relationships would change once they moved into professional nursing practice. However, family and friends had difficulties dealing with participants’ long shift hours, lack of participation in social activities, and in listening to work issues. Participants commented about the lack of understanding of nursing work. Most participants talked about the need to find other relationships for support from friends made at work or with other health professionals; “Those are the people you see, you socialize with, and you’re working alongside with in your career. There’s just this kind of different level of a connection that you don’t get with other people.” Yet, as participants recognized the scarcity of understanding between their work and those close to them, they learned to value time spent with family and friends to stay connected.
Threats to Health From Internal Workplace Factors
Threats were identified as issues that affected health or well-being due to work from personnel, such as incivility, bad attitudes, or bullying, which were separate from safety risks at work. Many participants reflected on their learning the phrase “nurses eating their young” in school and subsequent experience as a new employee. One common premise in conversations about “eating our young” was summed by one participant: That has been said for a long time . . . we should be there to lift each other up and help each other out . . . we went into nursing is help others, not to tear ‘em down, whether it’s a coworker or not.
Several others affirmed that good role modeling and support from their mentors or experienced managers aided them in dealing with the internal threats at work.
Safety Risks to Self
Safety risks were actual risks to personal safety caused by work or due to the type of work conducted. These risks, as stated by participants, included ergonomic-related tasks such as lifting patients, aggressive or violent patients or families, guns, needle sticks, driving home “asleep,” and bad policies or systems. Several examples of bad systems were given, such as lack of security on-site or having to walk to or from unlit parking lots to work alone. Many participants worried about making it home safely after working the night shift.
Every participant talked about their lack of experience with aggressive patients and the situations in which they found themselves. Some shared experiences such as being hit or kicked, most often by patients with dementia, whereas others shared that they had seen guns brandished. Most agreed with this statement: “Aggressive patients. Or aggravated patients are always a risk and, you’re worried.” Several people talked about being confronted with angry relatives or friends of patients and of not knowing how to handle a truly angry person: “You get threats from their families, and I don’t feel safe in that situation.” Only a few participants felt they had enough training as new nurses to deescalate violent or potentially violent situations.
Work Environment
The second key theme that arose from the focus groups and interviews related to the “work environment.” This theme explained the influences, resources, and skills needed that affected how novice RNs did their jobs or that helped them transition from school to individual practice following education. This theme was broken down into four subthemes related to the occupational setting or circumstance of the nurses: (a) caring for patients, (b) communication and workplace culture, (c) gender, and (d) organizational support and resources.
Caring for Patients
The participants spoke of putting the patient first and providing safe care. They discussed taking a holistic view of the patient and taking pride in doing so: “We’re supposed to look at all of the aspects of the patient’s life.” Yet, often as new nurses, they didn’t have time to look at the broad picture because, as one person said, “It’s really hard to learn how to do that holistic care as you’re trying to learn and refine your skills at the same time.” Time management was critical and not easily attained, as this new nurse noted: “One of the things that was difficult for me is I wanted to do all of these things for my patients. And you just don’t have time.” However, a positive surprise for many participants was caring for patients from a team approach, in which they could more easily balance the workload when responsibility was shared.
Communication and Workplace Culture
Communication and the culture of the workplace were somewhat related. Culture affected how participants perceived unit support and how they interacted with others. Some participants spoke about socializing with work colleagues after shifts which lead to increased trust and shared values. Communication differences due to unit culture, such as different expectations regarding patient information when transferring patients, were noticed. Participants voiced the need for clear communication to facilitate their transition to safe practice. Communication, specifically, was discussed in several ways. First, interprofessional issues were addressed, especially between medical staff and nurses. Many examples were given by participants, including provision of unclear orders, following orders that required a call to report results that were subsequently dismissed by the medical provider, or the lack of skill in reporting what was important. One person, noting he was still learning how to report to a physician, revealed his experience about communication and safety: That’s almost an area that I feel like, less safe, because often calling the doctor at night turns into getting yelled at-even if it’s for a good reason. So, it’s like you do everything you possibly can to not call them.
A second communication problem that interfered with work was between nursing staff. These issues were related to no communication between different shifts and different units, or lack of following protocols and not informing others of risks. However, one key informant found communication between staff was excellent in her workplace and proposed that it was because she worked in a highly specialized area, which echoed other participants’ experiences who worked in intensive or emergency care.
Gender Differences
Several focus groups had male participants, and two key informants were men. They identified several issues associated with gender that affected health and safety, which were readily endorsed by female participants. Men were perceived as having been treated “differently” by management and other health professionals. Both men and women asserted that men face more safety risks because men were often called upon to do extra lifting, intervene with aggressive patients, and take calls from health care providers, such as physicians, who were known to be verbally abusive. After a week of having to deal daily with a particularly aggressive patient as the only male nurse on the unit, one key informant shared the impact to his emotional health when he found himself crying on the way home from work due to the stress and fatigue.
Organizational Support and Resources
Lack of resources was a common thread in all focus groups and with key informants. Organizational resources included not only supplies, the right type of patient room, or equipment located on units, but also human resources, such as sufficient numbers of nurses or nurse aides. All participants perceived that their workplace orientation did not sufficiently prepare them to safely transition into practice. Irritation, as voiced by participants, was considerable, and they noted that without good support and time to learn protocols and policies, they felt lost and unsafe: “So there are days where I’m like: I don’t know where that is. I don’t know who to call to ask for it. I don’t know where to look. Help me.” Those few who completed a months-long nurse residency felt more at ease. Lack of support and resources were difficult to manage overall for the new nurses because, as one person put it: “It affects the health of the patient for sure, but I think it affects the work environment more than anything ‘cause we’re already stressed out and we don’t have some kind of assistance.”
Learning to be
The key theme of “learning to be” was used by some participants, and was driven by the concept of knowledge translation. This is the process and development of a professional nursing practice. This theme contained elements that involved learning “how to be” in a workplace, as one participant described, I think just trying to be—trying to know what I want it [my own nursing practice] to look like, and making it look that way . . . It just seems like something I have to figure out still.
Four subthemes arose within this theme, including (a) self-autonomy and self-advocacy, (b) knowing/not knowing, (c) work way versus school way, and (d) proving worth.
Self-Autonomy and Self-Advocacy
Self-autonomy and self-advocacy were discussed hand-in-hand as becoming independent and self-directing in practice while having to learn to advocate for themselves. One participant noted, “And that was my first introduction to being like, ‘I really need to do this (making decisions) on my own. You can be here as my resource person, but I’m going to teach myself here’.” Participants became aware of the need to advocate for themselves at work and home. Choosing where to work was important to self-growth and goal setting for some participants. Others found that they needed to advocate for themselves at home by dividing up chores and spending time with family members.
Knowing/Not Knowing
Many participants said they were very unsure on-the-job as new nurses, especially regarding the “right way” to do things. They felt overwhelmed with information (e.g., organizational policies) or felt unprepared when orientation was over. They described steep learning curves. One nurse said, “And I didn’t know what to do about it. I didn’t know what to do about it when everything went right, let alone when everything went wrong. So that just added to the stress.” Not only did participants talk about not knowing what to do correctly, they also related stories of tension between the “right way” but not following procedure, especially if more experienced nurses were role modeling that behavior: “I think maybe there’s a tendency to—maybe I’d call them, like, shortcuts—but doing things that work but maybe aren’t the best because it’s faster or easier or whatever, but in the long-run can harm you.”
Work Way Versus School Way
Participants contrasted what they were taught in school with their experiences in the workplace. Participants discussed learning basic skills needed for practice in their school programs and acknowledged the limitations of an academic program for teaching all necessary skills for practicing RNs. Yet, the transition from theoretical to practical was challenging. For example, participants noted that they received information in school about stress, anxiety, and burnout; however, they were surprised when they experienced this for themselves. Other participants discussed stress from expectations for perfection in school that subsequently followed them into their jobs, stating that, in practice, often the expectations were difficult to achieve.
Several participants felt the problem of balancing work expectations and what was taught in school was due to what was not taught in school. One key informant said she had a manager that used an evidence-based approach and was having staff learn the best and newest ways to do things. She noted she experienced difficulty in adjusting to her new position at work, due to her school program “being behind” in teaching evidence-based practice, including safety.
Proving Worth
Participants felt pressured to prove themselves to their peers and managers. They discussed wanting to fit in and not stand out: “As a new nurse and a new hire, you feel like you have to prove yourself and your worthiness almost, of your position.” Participants felt guilty if they took breaks, did not work extra shifts, or requested a day off, and some were scolded for calling in sick. Others felt pressure from managers to do more as the new staff person: “I had a manager tell me I wasn’t picking up extra shifts because I wasn’t loving it.” Pressure was especially intense during the probationary first months of hire: “I want to be really good . . . I feel like this ticking time clock kind of in the back of my head until my ninety days when I know, okay, I’m going to keep my job.” The pressure from proving themselves increased stress at work and at home, leading to health concerns and safety risks at work.
Discussion
The major concept of Balance between Work and Life in Newly Licensed Nurses with its three themes explained how the newly licensed nurses attempted to transition from student to a professional nursing role at a first nursing job. They reported experiencing a new awareness of occupational safety risks, listed new health problems such as hypertension and anxiety, referenced challenges adjusting to “normal life” after working several 12-hr shifts in a row, and difficulties finding time for self-care and relationships. Camaraderie, communication, and collegiality among coworkers were cited as protective factors in and outside the workplace: Non-nurses “just don’t get it.” Some participants discussed how factors within these themes have led to their own burnout and attrition. A serendipitous finding that emerged at the end of all focus groups was the relief felt by the participants from sharing their common experiences.
These findings resonate with many other studies that show the complex problems of transitioning into employment from student to a newly licensed nurse (Hoffart, Wadell, & Young, 2011; Kenny, Reeve, & Hall, 2016; Kramer, Brewer, & Maguire, 2011; Postma, Tuell, James, Graves, & Butterfield, 2017; Thomas, Bertram, & Allen, 2012; Wang & Tsai, 2014). Most of the problems identified in this study and in the literature reinforce components of the TWH program. A key component of TWH is evaluation of issues that are relevant and impact the well-being of the worker, as well as families and communities (NIOSH, 2015). The overarching theme for this study, Balance between Work and Life in Newly Licensed Nurses, includes factors that are attributable to occupation health and safety of newly licensed nurses at the workplace or within their social environments, as found in TWH. Psychosocial factors, safety issues, employee engagement, health behaviors, and “just being a new nurse” are just a few of the issues that lead to success or burnout and attrition (Bradley, Grossman, Hubbard, Ortega, & Curry, 2016).
This study had limitations. First, participants were predominantly women, Caucasian, and worked in mostly urban areas in the northwest, potentially limiting the generalizability of findings to diverse populations of nurses. Future research should explore perspectives of nurses in multiple settings and populations. Second, in focus groups, some participants may have been hesitant to freely contribute their experiences; however, all focus group participants for this study volunteered information throughout each session. Furthermore, key informant interviews confirmed themes and concepts introduced in focus groups.
Implications for Occupational Health Nursing Practice
The TWH program has brought to light the fact that there are now known risk factors related to work that have not been identified in the past. Studies have shown that new nurses have high rates of burnout and anxiety. Hospitals have instituted interventions to allow for learning over time, such as nurse residency programs. However, there are more factors in play than just giving new employees a longer time to be comfortable with skills in the job setting. In this study, participants, including some in residency programs, described challenges of transitioning to work that included encountering or witnessing violence, bullying from nursing and medical staff, long shifts, change in social support, inadequate or broken equipment, unsafe policies, lack of security, and even poor meal availability. These factors were found to affect health and contributed in some way to the more profound “unwellness” described by participants.
Occupational health nurses promote the health and safety of work and workplace communities including health care facilities and serve as experts in developing wellness programs, promoting safe work practices, preventing injuries, and mitigating hazards (American Association of Occupational Health Nurses [AAOHN], n.d.). Occupational health nurses’ role of managing risk reduction and health promotion (AAOHN, n.d.) aligns with TWH and the findings in this study. Workplace interventions seek to improve worker well-being while also protecting their health, such as (a) the Centers for Disease Control and Prevention (CDC; 2016) Work@Health program, that can be used to develop organization health strategies, (b) the Association of Occupational Health Professionals in Health care (AOHP) safe patient handling for health care workers and workplace violence prevention programs designed to protect nurses and others (AOHP, 2018), and (c) tools available from NIOSH TWH to assess worksite employees’ health and well-being and learn best practices (CDC, 2015). Occupational health nurses can use resources such as these to advocate for change and address challenges facing nurses, especially newly licensed nurses.
Work-based support groups for newly licensed nurses at work were endorsed by participants as a means to improve emotional and psychological health, and align with the types of suggested interventions for TWH. Having occupational health nurses as the experts to evaluate and recommend changes, such as support groups, has been endorsed by the Robert Wood Johnson Foundation (2015). In addition, development of tools to evaluate risks to work and life balance of new nurse employees is a research need that can be filled by occupational health nurses and lead to the best interventions to enhance health and safety at work and at home.
Conclusion
This study designed through the lens of the TWH model illustrates the necessity of linking occupational health and safety risks, work-life balance, and transitions to the workplace to the prevention of attrition and promotion of health and safety for newly licensed RNs. Much more work is needed to prevent new nurses from saying, “I am working five days a week, and it sucks my soul out.”
Applying Research to Practice
This study reports themes related to work, health, and safety of newly licensed nurses as found in the TWH framework, an initiative designed to improve the overall health and well-being of the U.S. workforce and reduce employee loss. Uncovering factors related to the TWH of newly licensed nurses transitioning into nursing practice provides occupational nurses and others the details needed to develop interventions that offer work-life balance, such as support groups for new nurses, assessments of new nurses’ health and safety risks at various time points during their first year with appropriate referrals as needed, more time for orientation and social support, and policies that encourage a culture of safety and work engagement.
Footnotes
Acknowledgements
We wish to acknowledge all of the newly licensed nurses who participated in this study and to Halle Schultz, student nurse, who assisted with recruitment.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Oregon Healthy Workforce Center pilot grant. U19OH010154, National Institute for Occupational Safety and Health, Center PI: WK Anger, Pilot PI: PG Graves.
Author Biographies
Gail Oneal, PhD, RN, is a population health nurse with research expertise in the areas of risk messaging, occupational and environmental health, and qualitative methodology. She is a clinical associate professor in the College of Nursing at Washington State University.
Janessa M. Graves, PhD, MPH, is a health services researcher with expertise in occupational health services and pediatric injury prevention and treatment. Her research focuses on equity in access, costs, and quality of injury care. She is an associate professor in College of Nursing at Washington State University.
Tullamora Diede, PhD, RN-BC, CNL, is qualitative researcher with expertise in nursing workforce issues and philosophical hermeneutic phenomenology methodology. She is an assistant professor at the Washington State University, College of Nursing.
Julie Postma, PhD, RN, is an occupational and environmental health nurse with expertise in community based participatory research. She is the Assistant Dean for Research in the College of Nursing, Washington State University.
Celestina Barbosa-Leiker, PhD, is a nursing researcher with expertise in psychological health and nursing workplace issues. She is the Associate Dean for Research in the College of Nursing at Washington State University.
Patricia Butterfield, PhD, RN, FAAN, is an occupational and environmental health nurse with expertise in the area of risk reduction. She is the Associate Dean for Research in the Elson S. Floyd College of Medicine at Washington State University.