
Abstract
This study measured the daytime sleepiness (DS) and work safety of fathers during the first 12 weeks of their babies’ lives (i.e., early fatherhood). A questionnaire was developed using the Epworth Sleepiness Scale (ESS), the Safety Behaviour at Work Scale, a self-reported sleep history, and a work-related incident history. Of the 221 participants, the vast majority reported they experienced less than 6 hours of interrupted sleep per night during the 12 weeks of the study, and an increasing frequency and severity of DS. The study also revealed an inverse correlation between ESS and Safety Behaviour at Work scores; fathers were 14% more likely to report a near-miss accident at work at 12 weeks. This study posits that antenatal classes and assessment of fathers’ sleepiness at work by occupational health practitioners could assist fathers in reducing daytime sleepiness and mitigating the risk of workplace incidents.
Keywords
More and more, society is demanding that Americans sacrifice sleep for the sake of family and work (Caldwell & Caldwell, 1998), yet little is known about men during early fatherhood. Demographically, dual earner couples outnumber couples for which the male is the breadwinner (Broomhill, & Sharp, 2004; Flood, 2003; Pocock, 2003); yet during early fatherhood (e.g., fathers with babies), the traditional role remains influential and reinforces the gender stereotype (Etaugh & Folger, 1998; Fuegen, Biernat, Haines, & Deaux, 2004). This situation exists because during early fatherhood, fathers fulfill the provider role so that the family has income while mothers are on leave (Battles, 1988; Eggebeen & Knoester, 2001). Although the breadwinner role remains salient for men during this time, it has also been shown that fathers also wish to care for their babies (Anderson, 1996; McVeigh & St John, 2003; Mellor & St John, 2012; Rustia & Abbott, 1993). For example, a baby’s sleep pattern over a 24-hour period is intermittent, lasting from a few minutes to a few hours (Cole & Cole, 2001), and consequently, parents spend 16% of their time holding their babies during sleeping or soothing; this percentage only drops to 13% at 13 weeks (Baildam et al., 2000). Thus, the outcome for working men during early fatherhood can be sleep deprivation due to repetitive sleep disturbances (Mellor & St John, 2010, 2012), which might ultimately affect work performance (Long & Johnson, 2001).
One salient consequence of a lack of sleep is daytime sleepiness (DS). DS is the “propensity to doze or fall asleep when intending to remain awake” (Johns & Hocking, 1997, p. 844), and research has shown that a minimum of 6 hours of uninterrupted and consecutive sleep is needed to prevent sleepiness during the day (Dinges, Rogers, & Baynard, 2005; Roehrs, Carskadon, Dement, & Roth, 2005). The phenomenon of DS appears to be commonplace. In the general and working population, DS has ranged from 10% to 25% (Johns & Hocking, 1997; Philip, Taillard, Niedhammer, Guilleminault, & Bioulac, 2001; Roehrs et al., 2005).
The prevalence of DS is of concern and might have grave consequences for workplace and public safety. DS has been shown to have deleterious effects on work performance, including decreased vigilance and task performance (Dinges et al., 1997; Leonard, Fanning, Attwood, & Buckley, 1998), increased fatigue and exhaustion (Edell-Gustafsson, 2002), and disorientation (Puvanendran, Venkatramani, Jain, & Farid, 2005). Several studies have also revealed an increased likelihood of work accidents in sleep deprived workers (Gold et al., 1992; Melamed & Oksenberg, 2002; Smith, Horswill, Chambers, & Wetton, 2009) and an increased likelihood of traffic accidents (Connor et al., 2002; Smiley, 1998).
It is commonly held that newborn care is a taxing experience for parents especially for mothers; however, fathers are now expected to become active parents (Anderson, 1996; McVeigh & St John, 2003; Rustia & Abbott, 1993). Yet, little research, description of the early fatherhood experience, and the pressures men face in balancing work and care responsibilities have been published (Mellor & St John, 2010). Furthermore, although general research on DS and its adverse consequences for workplace and traffic safety exists, at present, no study has specifically investigated the frequency, severity, and duration of DS in working men during early fatherhood or whether at this time in men’s lives DS results in greater risk to their safety at work.
Method
As part of a larger research project (approved by a university Human Research Ethics Committee and relevant participating health agencies) investigating working men during the first 12 weeks of fatherhood, a compelling need was identified to investigate the possible relationship between DS and work safety. A convenience sample was chosen from antenatal and postpartum services in the Gold Coast region of Queensland and Northern New South Wales in Australia. A required sample size of 197 was calculated (p < .05, B = .80, and an effect size of .30); however, to overcome attrition, a larger sample size of 241 was chosen. The final sample size for the study was 221 participants.
Instruments
A self-administered questionnaire regarding fathers’ sleep history, DS, safety behavior at work, and fathers’ work-related incident history was sent to the participants at 6 weeks (T1) and 12 weeks (T2) after their babies’ births. Those potential participants who failed to return their questionnaires within 1 week of posting were sent a reminder notice and another questionnaire. Each participant’s responses were anonymous; code numbers were attached to each pair of questionnaires but, after data analysis, all identifiable data were deleted from the database leaving only code numbers on the questionnaires.
DS was measured using the Epworth Sleepiness Scale (ESS), eight items (situations) reflecting activities of everyday life. Participants used a 4-point Likert-type scale of 0 to 3 to estimate the likelihood of falling asleep (0 = never doze, 1 = slight chance of dozing, 2 = moderate chance of dozing, 3 = high chance of dozing) with a total scale score range from 0 to 24. ESS scores are representative of the DS experienced by individuals with obstructive sleep apnea syndrome (OSAS); scores of less than 10 indicated non-DS, scores greater than 10 and less than 16 indicated mild OSAS, and scores greater than 16 indicated moderate to severe OSAS (Johns, 1991). The ESS has been used extensively in sleep research, and the validity, stability, and internal consistency of the scale has been demonstrated in many studies (Beaudreau et al., 2012; Bloch, Schoch, Zhang, & Russi, 1999; Chen et al., 2002; Cho et al., 2011; Johns, 1992, 1994; Kendzerska, Smith, Brignardello-Petersen, Leung, & Tomlinson, 2014; Knutson, Rathouz, Yan, Liu, & Lauderdale, 2006; Miletin & Hanly, 2003). In this study, the data from the ESS were used to measure the frequency, severity, and duration of DS. In addition, a paired-sample t test was used to identify any differences in the mean scores for ESS at 6 weeks (T1) and 12 weeks (T2).
This study also measured the work safety behavior of men during early fatherhood. Safety behavior is the actual behavior that individuals demonstrate at work, adhering to safety procedures to maintain a safe workplace (Griffin & Neal, 2000; Neal & Griffin, 2002). Griffin and Neal (2000) developed the Safety Behaviour at Work scale, which includes six statements that measure worker safety compliance (three items) and worker safety participation (three items). Participants used a 5-point Likert-type scale to estimate how much their work behavior corresponded to the item statements on work safety (1 = strongly disagree, 2 = disagree, 3 = not sure, 4 = agree, and 5 = strongly agree) with a score range of 0 to 15 for both Safety Compliance and Safety Participation subscales. Item scores are summative with a low score indicating unsafe behavior. The safety behavior scale has shown acceptable internal consistency (Griffin & Neal, 2000; Machin, 2005; Neal & Griffin, 2002, 2006; Neal, Griffin, & Hart, 2000; Pousette, Larsson, & Torner, 2008). A correlation coefficient (Pearson’s r) was used to identify the direction, strength, and statistical significance of the correlations between ESS and the Safety Behaviour at Work Scale scores at T1 and T2. Cronbach’s alpha coefficient was used to examine the reliability of the items within each scale. According to Polit and Beck (2012), an acceptable standard of reliability for the Cronbach’s alpha coefficient should be at least .70. In this study, the Cronbach’s alpha scores for the ESS and Safety Behaviour at Work scale were above .70 (see Table 1).
Reliability of the Study Instruments
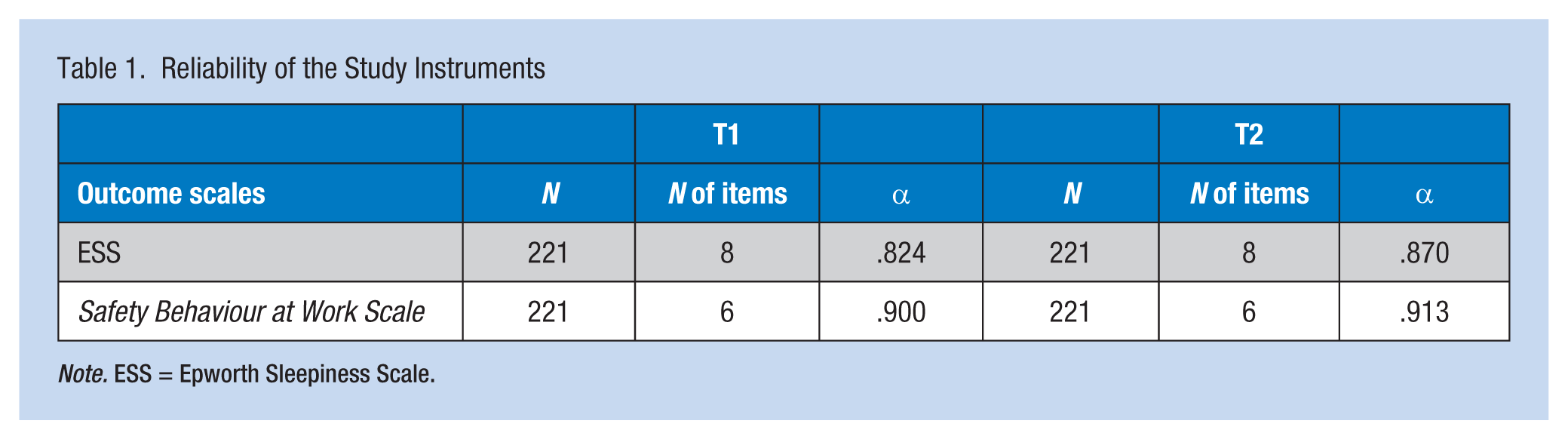
Note. ESS = Epworth Sleepiness Scale.
The duration and fragmentation of sleep has been shown to predispose individuals to DS (Dinges et al., 2005; Roehrs et al., 2005). Therefore, a brief sleep history was included in the questionnaire with two items asking participants to estimate how many sleep interruptions occurred per night and the hours of aggregated sleep (total sleep minus interruptions) they were receiving. A correlation coefficient (Pearson’s r) was used to identify the direction, strength, and statistical significance of the correlation between the ESS and sleep history scores at T1 and T2.
At both T1 and T2, participants were asked to report whether they had experienced work accidents or near-miss work accidents as well as road accidents and near-miss road accidents driving to and from work. A standard logistical regression analysis was used to assess the effect of DS on the likelihood that fathers would report a work or traffic incident at T1 and T2.
Results
Of the 221 participating fathers, the vast majority (85.4%; 182/213) indicated that they were experiencing interrupted sleep at T1, with an average of 2.4 interruptions per night (SD = 1.18; 0-7). The average aggregate sleep at T1 was 5.5 hours (SD = 1.20; 1-8 hours). At T2, the same percentage of fathers reported less sleep interruptions (M = 1.80, SD = 1.14, 1-6) and a corresponding slight increase in aggregated sleep (M = 5.9 hours, SD = 1.18; 1-8 hours). A paired t test revealed a statistically significant decrease in sleep interruption mean scores, t(217) = 7.26, p < .001, and a statistically significant increase in aggregated sleep mean scores, t(210) = −4.65, p < .001, from T1 to T2 (see Tables 2 and 3).
Father’s DS Frequency and Percentages Based on OSAS Scale Scores
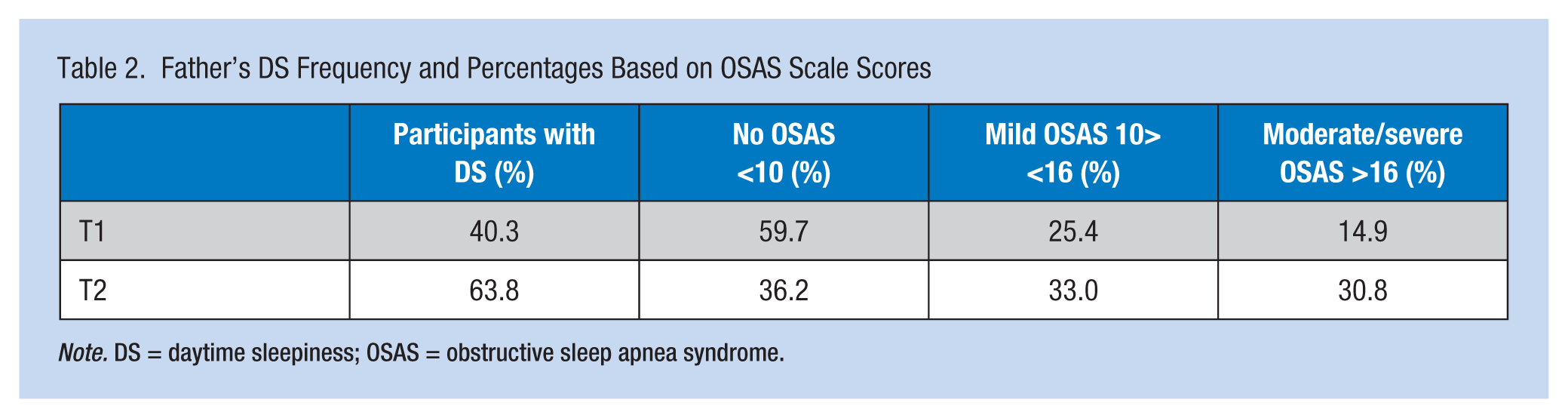
Note. DS = daytime sleepiness; OSAS = obstructive sleep apnea syndrome.
Paired t Test: Father’s DS at T1 and T2
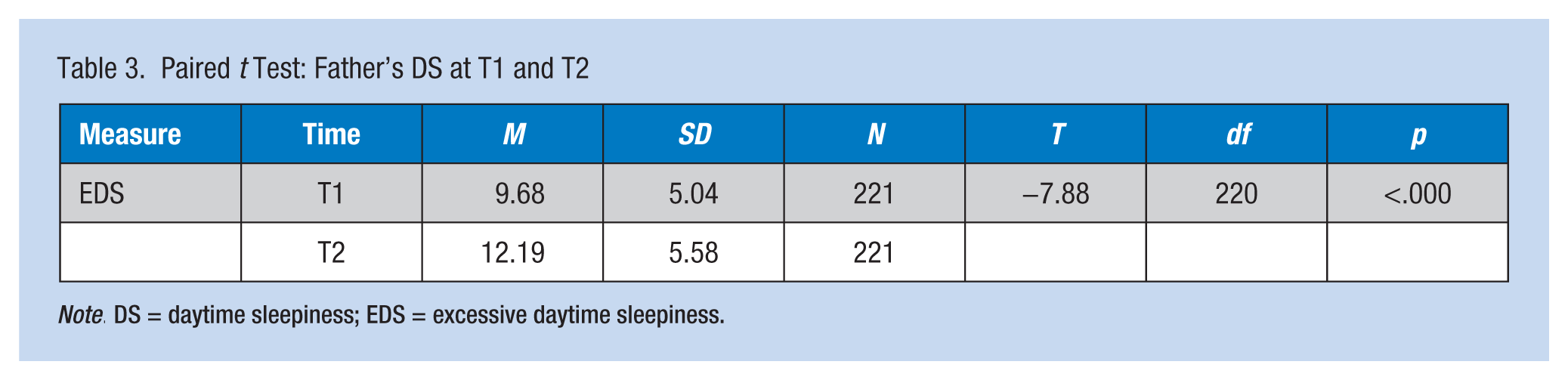
Note. DS = daytime sleepiness; EDS = excessive daytime sleepiness.
The results further revealed that 40% of the participants experienced DS to some degree at T1; this percentage was higher at T2 (64%). Specifically, at T1, 25% of the participants reported ESS scores indicative of mild DS, and 15% reported scores equivalent to moderate to severe DS. However, at T2, the ESS scores indicative of DS were higher, with 33% reporting mild DS and 31% reporting moderate to severe DS. The ESS group mean score for participants at T1 was 9.68 (SD = 5.04, 0-22); this score was higher at T2 (M = 12.19, SD = 5.58, 0-24). A paired t test revealed a statistically significant increase in ESS mean scores from T1 to T2, t(220) = −7.88, p < .001. Furthermore, a correlation coefficient (Pearson’s r) revealed an inverse and statistically significant correlation between ESS and aggregate sleep scores at both T1 and T2, r = −.259, p = .019, and r = −.372, p < .001, respectively, and a positive and statistically significant correlation between ESS and interrupted sleep scores over the same timeframes, r = .181, p = .007, and r = .234, p < .001.
A descriptive analysis of the Safety Behaviour at Work scores has been described in a previous article (Mellor & St John, 2012), in which participants reported a decrease in safety behavior at work scores over the 12-week period. In this study, the results also revealed statistically significant correlations between ESS and Safety Behaviour at Work subscales—in particular, an inverse correlation between ESS and safety compliance scores at T1 and T2 (r = −.242, p < .001, and r = −.348, p < .001, respectively); in relation to safety participation, an inverse statistically significant correlation (r = −.255, p < .001) was found at T2.
A standard logistic regression analysis assessed the effect of DS on the likelihood that fathers would report a work-related incident at T1 and T2. For work accidents, road accidents and near-miss road accidents, the overall model did not reliably distinguish between reporting and not reporting a work-related incident among participants with DS. However, DS was shown to significantly predict the reporting of a near-miss accident at work. Fathers who reported DS were 12% more likely to report a near miss at T1, χ2(5, n = 216) = 8.919, p = .004, 95% CI = [1.038, 1.216], and 14% more likely at T2, χ2(5, n = 216) = 25.46, p < .001, 95% CI = [1.038, 1.216].
Discussion
The study results point to a disturbing picture of DS and impaired safety among workers during early fatherhood. In this study, the frequency of DS was high at 6 weeks and 12 weeks (40% and 64%, respectively); these percentages were higher and in stark contrast to previous research that reported a DS prevalence in the working population of between 10% and 25% (Johns & Hocking, 1997; Philip et al., 2001; Roth & Roehrs, 1996). In addition, Johns and Hocking (1997) reported an ESS mean score of 4.6 and an aggregate sleeping period of 7.5 hours in the working population. In this study, fathers reported a mean score of approximately double the score of the working population and 2 hours less sleep at 6 weeks. Moreover, at 12 weeks, 64% of participants reported DS levels representative of the DS experienced by moderate to severe OSAS sufferers. Interestingly, although the number of sleep interruptions and aggregate sleep among study participants significantly improved from 6 to 12 weeks, sleep interruptions and aggregate sleep did not buffer participants’ DS. One explanation for this finding might be that interrupted sleep plays a role in maintaining DS regardless of improved aggregate sleep. The positive correlation between ESS and sleep interruption scores adds support to this assumption. Thus, the study results support the research findings of Dinges et al. (2005) and Roehrs et al. (2005) who found that 6 hours of uninterrupted sleep is needed to meet basic sleep requirements.
This study is the first to also identify the work safety implications of DS in men during early fatherhood. Previous research has demonstrated the negative affect DS has on vigilance, task performance, and work safety; this study adds to the literature regarding this proposition. Disturbingly, this study revealed a correlation between increasing DS and decreasing safety compliance and safety performance in early fatherhood during the first 12 weeks and that participants with DS were 12% more likely to report a near-miss accident at work at 6 weeks and 14% at 12 weeks. However, unlike other studies (Akerstedt, Fredlund, Gilberg, & Jansson, 2002; Heaton, Browning, & Anderson, 2008; Melamed & Oksenberg, 2002), this study did not reveal a correlation between DS and work accidents or traffic accidents. One reason for this finding may be a lack of statistical power in this study to capture relatively rare events. Regardless, high frequency and severity of DS scores, decreased safety behavior, and the increased likelihood of near-miss accidents lend support to DS during early fatherhood posing a potential risk to work and public safety.
This study highlights a serious situation that cannot be ignored by employers; and, of further concern are research findings that have shown men during early fatherhood work longer hours than prior to the births of their children (Eggebeen & Knoester, 2001; Mellor & St John, 2012; Tanaka & Waldfogel, 2007). Therefore, employers must be cognizant of early fatherhood as a time when fathers have increasing exposure and engagement in work; at the same time, these men are potentially experiencing DS and impaired work safety. Previous studies have highlighted the lack of consideration given to work-family balance and family leave by managers (Holter, 2007; Nepomnyaschy & Waldfogel, 2007; Ortega, 2009; Wolcott, 1991); the results of this study posit the need for managers to see leave as an occupational health and safety measure to reduce DS rather than a work entitlement or privilege.
Although employers have an obligation to provide workplace safety measures, fathers also have an obligation to be safe at the workplace for themselves and their colleagues. Thus, the onus is also on men during early fatherhood to sleep and rest in readiness for work. Measures to prevent or mitigate DS can occur prior to babies’ births. Antenatal programs can help fathers identify and clarify DS issues. The discussion of sleep as a specific health issue for working fathers has received only scant attention in previous health and social literature (Mellor & St John, 2010), and thus, it can be assumed that it is also given minimal acknowledgment as an issue for fathers in antenatal education. The results of this study support the need for antenatal programs to assist fathers in preparing for changes in work–life balance commonly expected during early fatherhood. For example, antenatal programs are a timely venue for men to receive information about and encouragement to plan for balancing care requirements of the newborn and work demands, and to maximize uninterrupted sleep (McVeigh & St John, 2003).
Occupational health and safety professionals should offer care to fathers during the early months of their babies’ lives (McVeigh & St John, 2003; Mellor & St John, 2012). In relation to DS, occupational health practitioners, and in particular occupational health nurses, can better understand the health and safety of men during early fatherhood by using the ESS to identify fathers with DS, measure DS severity, and implement measures to meet the needs of their specific work. Previous literature has shown the importance of health surveillance, health promotion, and injury prevention programs as part of the occupational health nurse’s role (Mellor & St John, 2007; Mellor, St John, & McVeigh, 2006). Therefore, occupational health nurses can directly impact work safety for new fathers. For example, occupational health nurses should regularly assess the work of men during early fatherhood because new fathers may not be able to assess their own safety or decision-making processes. Occupational health nurses can identify fathers at risk of DS and collaborate with supervisors to modify fathers’ work environments or processes as necessary.
This study is the first to quantitatively measure DS in men during early fatherhood and provides a foundation for further research on their health and safety at work. However, caution is warranted when generalizing the study findings because a randomized sample of new working fathers was not possible and the sample was drawn from within a distinct geographical region. Furthermore, while standardized measures were used, the study asked participants to provide data over a 12-week period; in light of the assumption that men in early fatherhood suffer DS, their recall accuracy might be an issue. As a result of these limitations, this study should be replicated with a larger sample over a wider geographical area and a longer time frame. Longitudinal studies greater than 3 months are needed to measure the persistence of DS in new fathers, which could confirm or refute these study results and the validity and reliability of the scales.
Conclusion
Fatherhood is a significant life event for men, and this study found that it is common for new fathers to experience DS during the first 12 weeks of their babies’ lives. The results of this study also revealed the negative impact DS has on new fathers’ workplace and traffic safety. This study posits that antenatal classes and the assessment of fathers at work might be needed to reduce DS and mitigate the risk of workplace and traffic incidents. Employers, midwives, and occupational health practitioners could use the ESS scale to identify DS in this high risk group and subsequently implement and monitor interventions to help these workers stay healthy and safe while they make the transition to fatherhood.
Applying Research to Practice
Daytime sleepiness has an impact on the safety behavior and thus the workplace safety of men with babies.
Occupational health nurses must be prepared to assess and monitor the levels of sleep deprivation and safety behavior in fathers during the first 3 months of early fatherhood.
Simple survey tools such as the ones described can be adapted and used for this purpose.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Gary Mellor is a registered general nurse and academic with clinical experience in primary health and remote occupational health nursing. His research has centered primarily in work safety, early fatherhood, and men’s health.
Stephen Van Vorst is a registered general and a registered psychiatric nurse with clinical experience in medical-surgical, mental health, and developmental disability nursing. His research interests include mental health nursing education, preparation for practice, and fatherhood—in particular, the support of fathers with babies.