
Abstract
The purpose of this study was to investigate the influence of work environments and occupational hazards on smoking intensity by occupation type in Korean workers. This study used the data from the Fourth Korea National Health and Nutrition Examination Survey in 2009. The sample of this study included 3,769 adults who were aged 18 years or older and had an occupation of office work, sales, or manufacturing. After controlling for sociodemographic characteristics, the generalized linear models revealed that office workers and the sales force who had smoking co-workers at the workplace were more likely to smoke than those who did not. A dirty workplace and exposure to occupational noise were significant factors increasing the smoking intensity for manufacturers. A smoking cessation program considering physical work environments and co-workers’ support should be developed for Korean workers.
Keywords
It is well established that smoking is associated with a high prevalence of occupational injury. Active smokers without a history of occupational noise exposure are more likely to have a hearing impairment than non-smokers (Nakanishi, Okamoto, Nakamura, Suzuki, & Tatara, 2000). Smoking is also associated with reduced vision in the dark (Havelius & Hansen, 2005) and sleep disorders (Nakata et al., 2005), which can cause job-related injuries. Furthermore, for employees who smoke, additional financial costs may be incurred due to absenteeism, less productivity (Tsai, Wen, Cheng, & Huang, 2005), and health care expenditures (Yang, Fann, Wen, & Cheng, 2005).
Many workplaces in Korea have now prohibited smoking, provided smoking cessation programs, or at least introduced smoking policies. These measures and a range of community-based initiatives have significantly decreased smoking prevalence rates. Although smoking prevalence among men in Korea was 42.1% in 2012, it has been declining over the past two decades (Korean Statistical Information Service [KOSIS], 2012). In contrast, the smoking prevalence among Korean women was only 6.2% in 2012, but it has been increasing over the past two decades (KOSIS, 2012). Thus, smoking is a significant issue for many Korean workers as it is for workers in other countries, and it is important to identify ways in which the workplace, work environment, and organization of work might contribute to smoking behavior.
This study used the social ecological theory (McLeroy, Bibeau, Steckler, & Glanz, 1988) as a theoretical framework to identify the association between work environments, occupational hazards, and smoking intensity. A contention within the social ecological theory is that an individual’s health is influenced by physical aspects (e.g., ergonomic design of jobs, exposure to toxic substances), social aspects (e.g., shift work, hours worked per week), and psychological aspects (e.g., decision latitude, work demands) of workers’ jobs as well as their dispositions, resources, and characteristics (Chin, Hong, Gillen, Bates, & Okechukwu, 2013; Ettner & Grzywacz, 2001). Based on a literature review and theoretical framework, we selected variables from individual, health, behavioral, psychological, interpersonal, and occupational aspects that influence smoking intensity among Korean workers.
Work environmental factors and occupational hazards other than psychosocial factors have received only limited attention in previous research. Many studies have focused on assessing the relationships between current smoking status and psychological stress as indicated by models of job strain (Fujishiro & Heaney, 2009; Heikkila et al., 2012; Kouvonen, Kivimaki, Virtanen, Pentti, & Vahtera, 2005; Kouvonen et al., 2007; Li et al., 2010; Ota et al., 2010; Radi, Ostry, & LaMontagne, 2007). Some studies have examined the association of smoking and work environment in terms of work shift, perception of one’s work (Sanderson, Ekholm, Hundrup, & Rasmussen, 2005), physical workload (Albertsen, Hannerz, Borg, & Burr, 2004), peer smoking at the worksite (Honjo, Tsutsumi, Kawachi, & Kawakami, 2006), or social support (May & West, 2000; Steptoe, Wardle, Pollard, Canaan, & Davies, 1996). However, these studies have not produced consistent findings. The main reason for inconsistent results may be that sample sizes were too small to detect effects (Albertsen et al., 2004). There might be an association between smoking and occupational hazards such as dust, chemicals, or noise, but relatively few studies (Albertsen et al., 2004; Chin, Hong, Gillen, Bates, & Okechukwu, 2012) have investigated such associations.
It is important to identify significant workplace factors related to smoking so that occupational health nurses can develop and implement more effective workplace strategies to impact smoking behavior. Therefore, the purpose of this study was to assess the influence of work environments and occupational hazards on smoking intensity by occupation type after adjusting for sociodemographic characteristics of a large sample of Korean workers.
Method
This secondary data analysis used data from the Fourth Korea National Health and Nutrition Examination Survey (KNHANES VI-3) conducted by the Korea Centers for Disease Control and Prevention (KCDC). The KNHANES VI-3 data were publicly available and provided only de-identified data, and the researchers did not contact the participants.
Setting and Sample
The KNHANES VI-3 is a large, population-based, cross-sectional survey of Korean non-institutionalized civilians. The survey used a systematic stratified cluster sampling design based on geographic area, gender, and age. The sampling frame was based on the 2009 Korean National Census Registry. Weights indicating the probability of being sampled were assigned to each respondent, enabling the results to represent the entire Korean population (KCDC, 2010).
The KNHANES VI-3 consisted of three questionnaires: Health Interview Survey (HIS), Nutrition Survey, and Health Examination Survey. The authors extracted data from approximately 10,078 HIS, which included sociodemographic and health-related behavior (i.e., physical activity, cigarette smoking, and alcohol use as well as information about work environments) data (KCDC, 2010).
The sample for this study included adults aged 18 years or older working in offices, sales, or manufacturing. Unemployed individuals, including housewives and students, were excluded. Participants who did not respond to the question about occupation were also excluded. Consequently, 3,769 respondents were selected for the final analysis. Figure 1 illustrates the screening process for selecting the study sample.
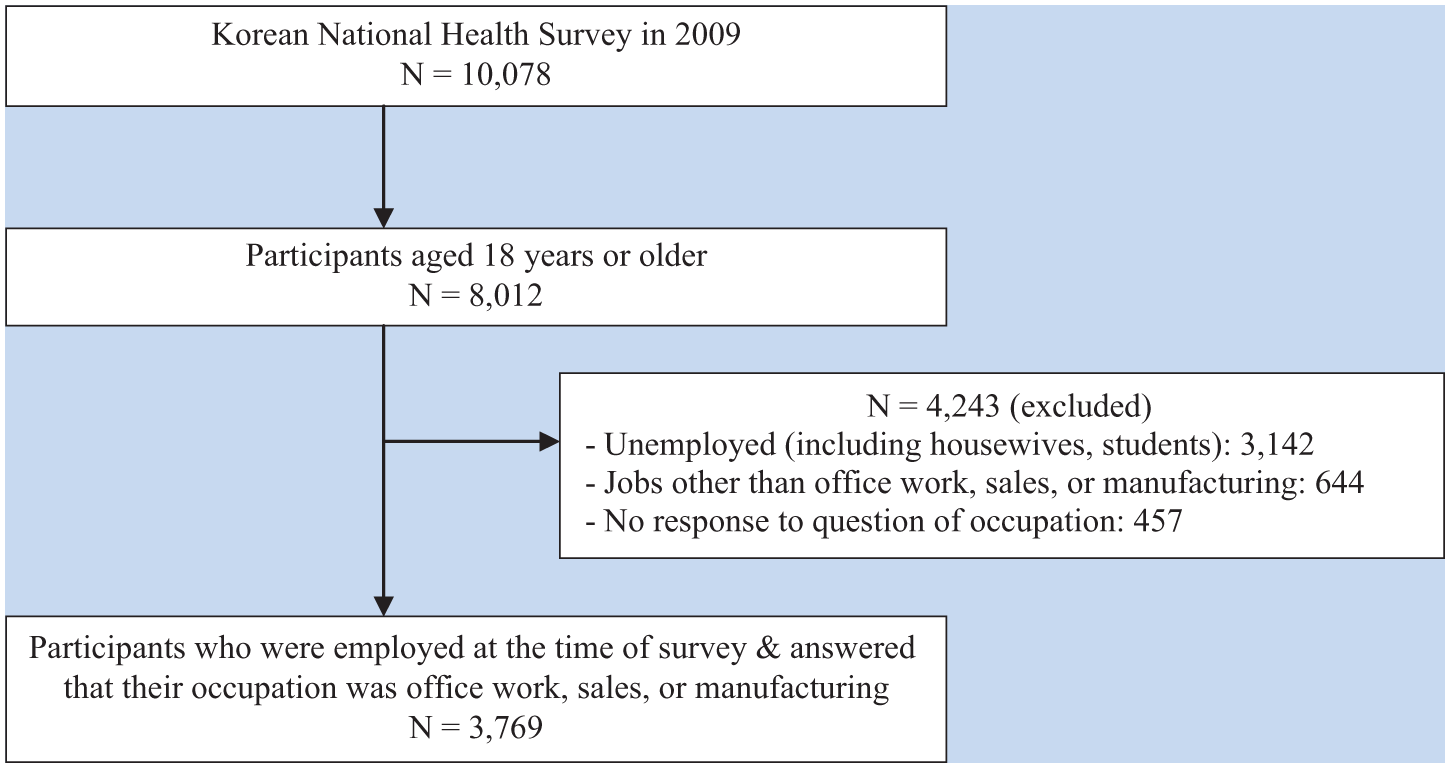
Screening process used to select the study sample.
Measures
Sociodemographic variables included age (i.e., 18-24, 25-34, 35-44, 45-54, 55-64, ≥65 years), gender (male, female), marital status (married, divorced/separated/widowed, never married), education (elementary school graduate or less, middle school graduate, high school graduate, college graduate or higher), household income (lower, lower-middle, upper-middle, upper), and living arrangement (living alone, living with others).
Health-related behavioral characteristics included frequency of alcohol consumption (none or <1 time per month, 1-4 times per month, 2-3 times per week, ≥4 times per week) and perceived stress level (high, moderate, low).
Working conditions were assessed by determining employment status (employed full-time, employed part-time), weekly working hours (≤40, >40 hours per week), working time of the day (day shift, night shift), and co-workers’ smoking at workplace (yes, no).
Work environments were assessed using eight questions: “Is your worksite clean and pleasant?” (Clean worksite); “Is your work so dangerous that you are at a high risk of an accident?” (Risk of accident); “Is your workload so demanding that you are always short of time?” (Psychological demand); “Do you have power in deciding working time or process?” (Decision authority); “Are you respected or trusted by your co-workers?” (Respect/trust); “Does your work require that you are in an uncomfortable posture for a long time?” (Uncomfortable posture); “Does your work require that you lift or move a heavy object?” (Physical strain); and “Do you have to hide your emotions at work?” (Hiding one’s emotion). All these questions were originally measured by using four scales: to a high degree, to some degree, to lesser degree, or no degree. In this study, responses were dichotomized into high (high and some degree) or low degree (low and no degree).
Occupational hazards were measured using six single questions: “Are you exposed to risky chemical substances such as organic solvents, heavy metals, or agricultural chemicals?” (Chemical substance); “Are you exposed to air pollution such as dust, fumes, or humectants?” (Air pollution); “Do you handle dangerous equipment or machinery?” (Dangerous equipment); “Are you exposed to fire or electrical shock?” (Fire/electrical shock); “Are you exposed to noise so high that you have to raise your voice to talk with others?” (Noise); and “Do you handle infectious specimens or microorganisms?” (Infection). Responses for these questions were categorized as either not exposed or exposed to each hazard.
Smoking intensity, as a dependent variable, was measured by a question asking the average number of cigarettes smoked per day. If respondents reported that they were ex-smokers or lifetime non-smokers, smoking intensity was recorded as zero.
Data Analysis
For the study results to represent the entire Korean population, the complex sample analysis which included strata, cluster, and sample weight was used. A bivariate analysis using t test (a test to compare the means of two groups) or analysis of variance (a test to compare the means among more than two groups) compared the average number of cigarettes per day by sociodemographic and work environment characteristics. A generalized linear model (GLM) was used to identify the impact of work environment and occupational hazards on smoking intensity. The GLM is a flexible generalization of ordinary linear regression that allows response variables to have error distribution models other than a normal distribution. A two-tailed, p < .05 level of significance was used. All analyses were conducted using SPSS version 21.0 (IBM Corp., Armonk, NY).
Results
Table 1 illustrates the bivariate comparisons of smoking intensity by sociodemographic variables, health-related behavioral characteristics, and working conditions among the three occupational groups (i.e., office workers, sales force, and manufacturing workers). The number of cigarettes per day differed significantly by age, gender, education, and frequency of alcohol consumption. Long work hours, full-time employment, and co-workers’ smoking were related to higher smoking intensity for all occupations. Day shift work was associated with higher smoking intensity in office workers, whereas evening shift work was associated with higher smoking intensity in manufacturing workers.
Comparisons of Smoking Intensity by Sociodemographic Characteristics Among Occupations
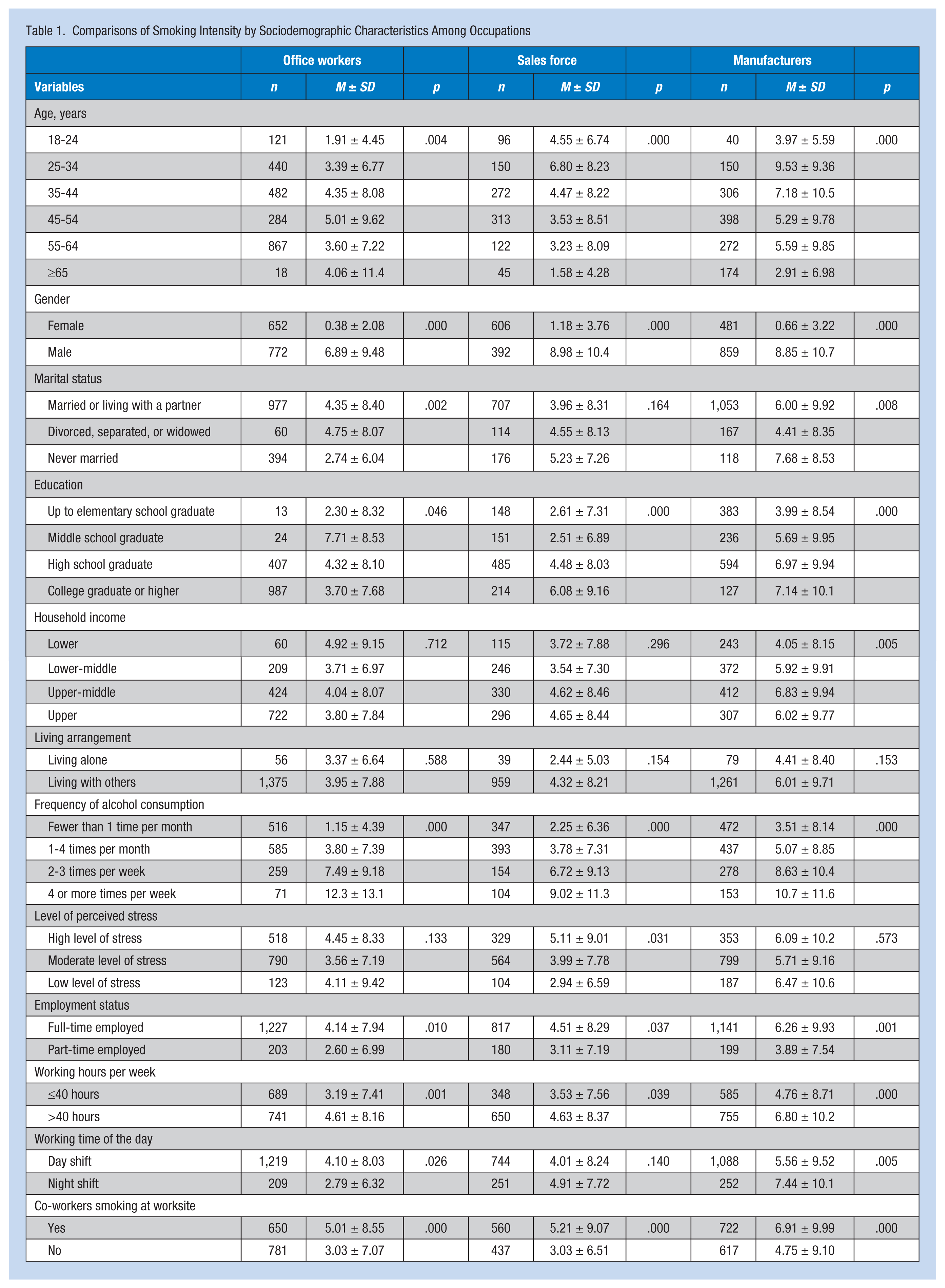
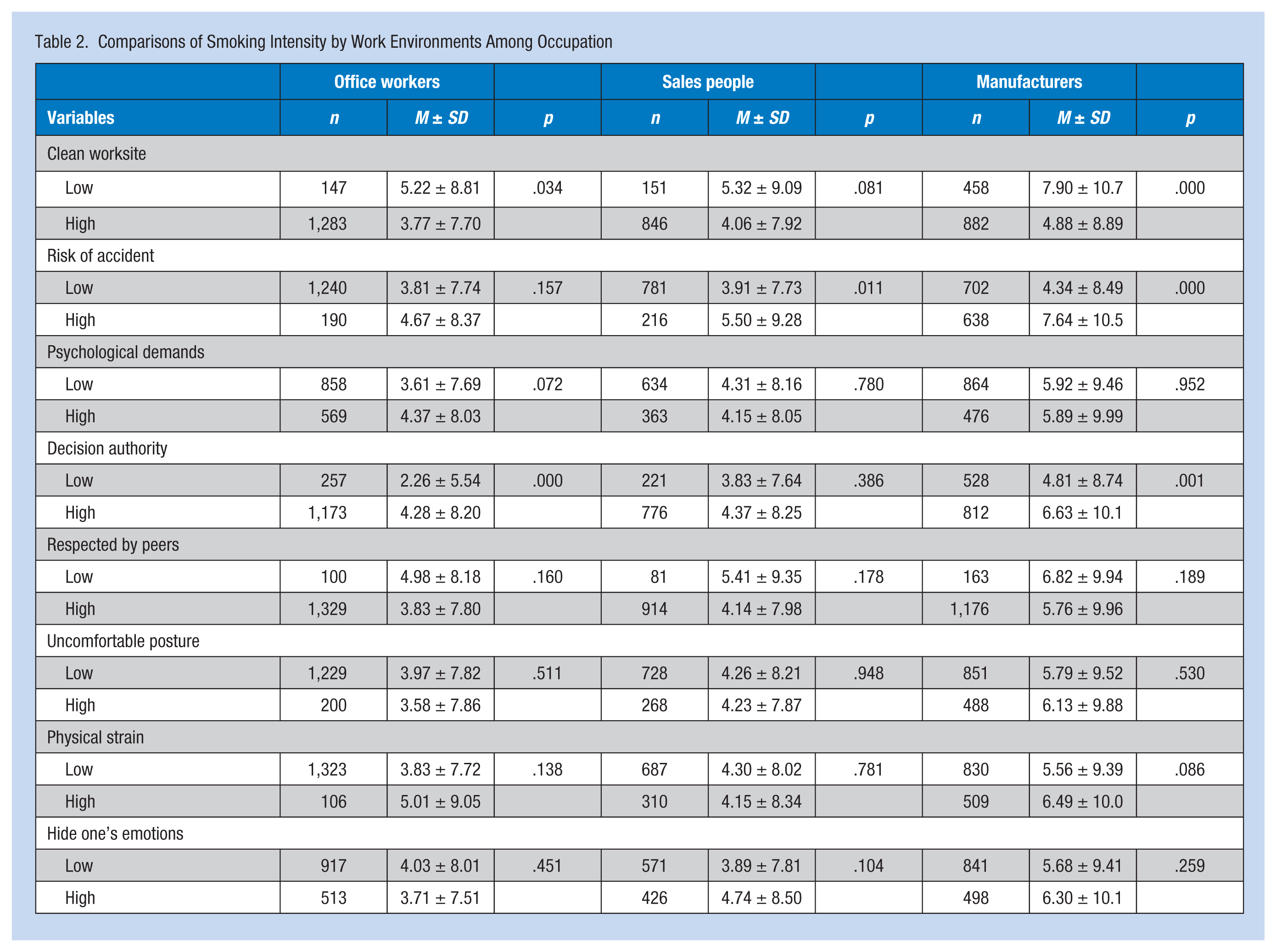
Table 2 shows the smoking intensity according to type of work environment. For office workers, a clean worksite and lower level of decision authority correlated significantly with a lower average number of cigarettes smoked per day. For the sales force, a significant relationship was found between a higher risk of accidents and more intense smoking. For manufacturing workers, a clean worksite, lower risk of accidents, and lower decision authority correlated significantly with less smoking intensity.
Comparisons of Smoking Intensity by Work Environments Among Occupation
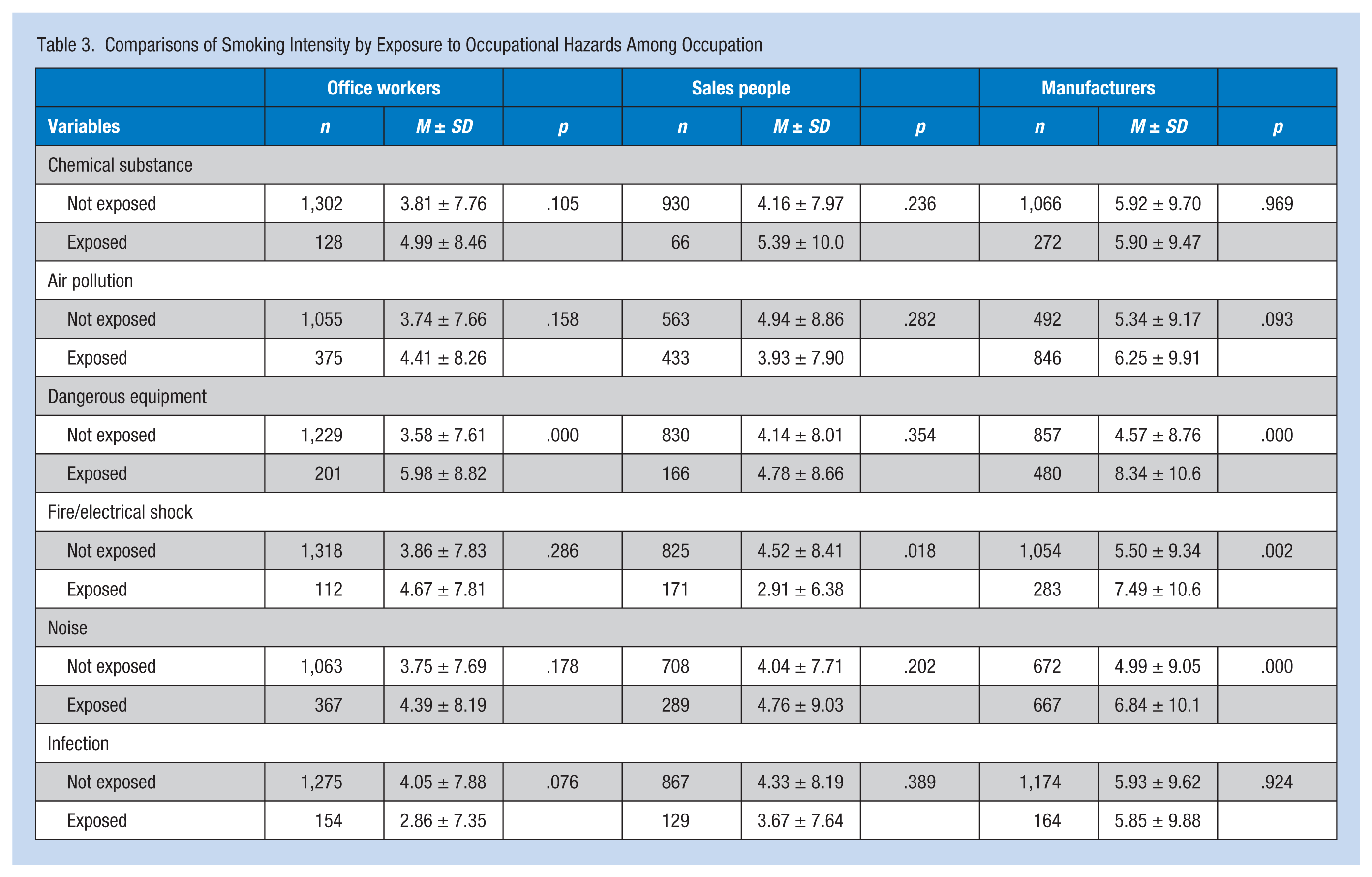
Office workers who handled dangerous equipment smoked heavily in comparison with officer workers who were not exposed to this risk (Table 3). Handling dangerous equipment and exposure to fire or electrical shock and noise significantly increased manufacturers’ smoking intensity.
Comparisons of Smoking Intensity by Exposure to Occupational Hazards Among Occupation
Multivariate Analysis
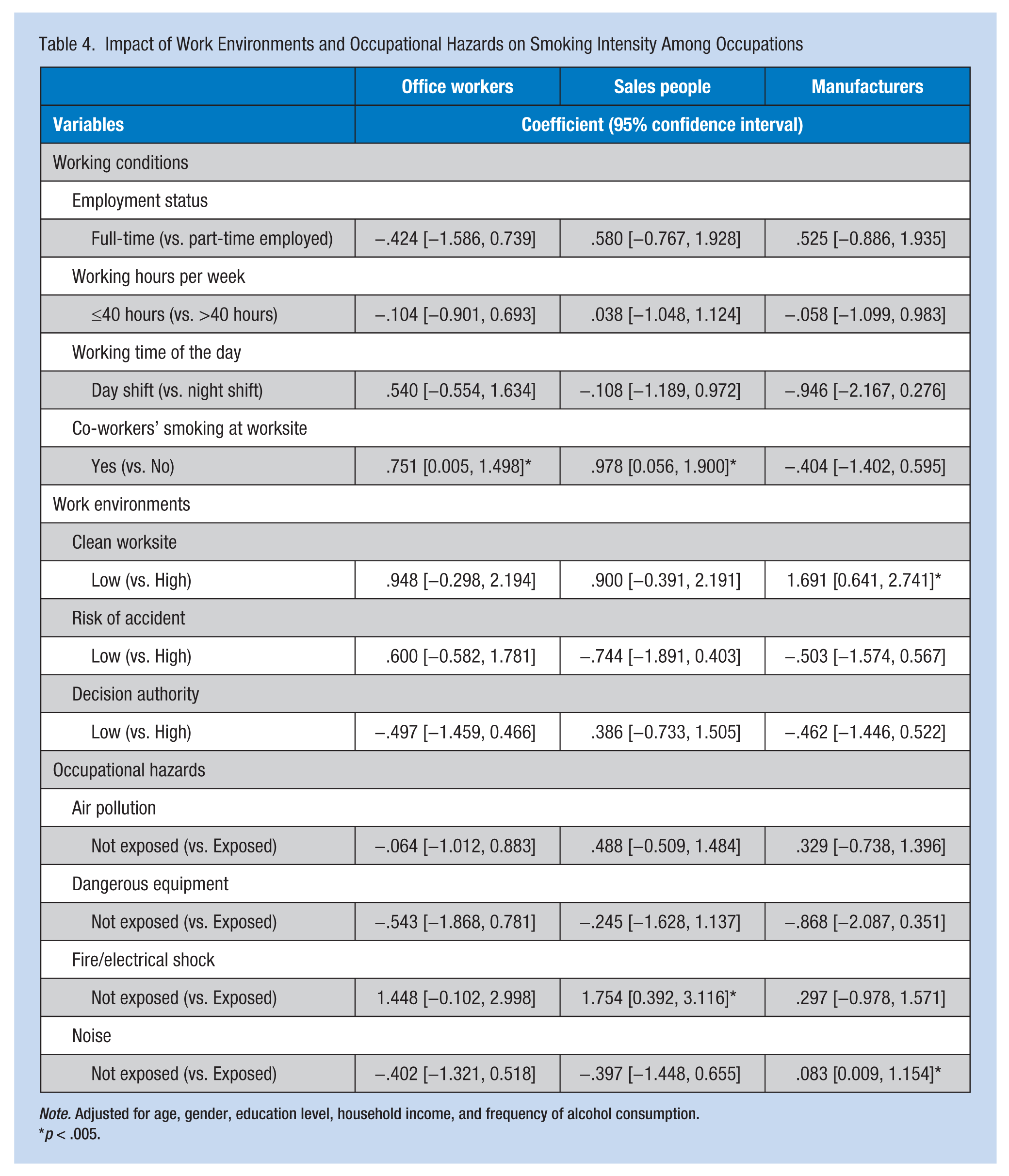
The impact of work environments and occupational hazards on smoking intensity among the three occupational groups is presented in Table 4. All GLM statistics were controlled for age, gender, education, household income, and frequency of alcohol consumption. Office workers who had smoking co-workers were more likely to smoke than those who did not have smoking co-workers (β = 0.751, 95% confidence interval [CI] = 0.005-1.498). Sales force who had smoking co-workers (β = 0.978, 95% CI = [0.56, 1.90]) and had not been exposed to fire or electrical shock risk (β = 1.75, 95% CI = [0.39, 3.11]) were significantly more likely to smoke compared with sales workers who had been exposed to fire or electrical shock hazards and did not have smoking co-workers. A dirty workplace (β = 1.69, 95% CI = [0.64, 2.74]) and exposure to occupational noise (β = 0.83, 95% CI = [0.09, 1.15]) correlated significantly with increased smoking intensity for manufacturing workers.
Impact of Work Environments and Occupational Hazards on Smoking Intensity Among Occupations
Note. Adjusted for age, gender, education level, household income, and frequency of alcohol consumption.
p < .005.
Discussion
The researchers found that the impact of work environments and occupational hazards on smoking intensity differed by occupational type. Office workers and sales workers who had smoking co-workers were significantly more likely to smoke; this finding is consistent with previous studies (Chin et al., 2013; Perrine & Aloise-Young, 2004). Peer pressure is widely assumed to be a significant causal factor in the initiation of smoking. Perrine and Aloise-Young (2004) found that the likelihood of smoking was 4 times higher if one friend was a smoker and increased by up to 160 times if four friends were smokers. Yasin, Retneswari, Moy, and Koh (2012) found a strong association between co-workers’ support and smoking cessation. When attempting to quit, the effect of co-worker support may be enhanced when offered by non-smoking colleagues or ex-smokers.
According to social cognitive theory, individuals’ perceptions of the environment create behavioral norms, which in turn impact health behaviors. A social environment with many smokers creates a barrier for smokers to quit smoking because social norms that approve smoking are promoted (Honjo et al., 2006). Social support from co-workers is a critical factor for many workplace health promotion programs. As social support at work is associated with employees’ health risks and predictive of subsequent behavior change, workplace health promotion interventions could achieve desired outcomes by ensuring that the support of smoking partners and co-workers is integrated into the design and delivery of programs (Chin et al., 2013).
In this study, sales workers who reported no exposure to fire or electrical shock in their workplaces were more likely to smoke than those who were exposed to potential fire or electrical shock hazards in their workplaces. Lit cigarettes are the leading cause of unintentional residential fires in Korea. In 2010, 37.6% of a total of 1,432 residential building fires were unintentional, and 11.7% of these unintentional fires were caused by smoking (Life Safety, 2011). Using modeling, a 1% decrease in smoking corresponded to a 7% decrease in the residential fire mortality rate (Diekman, Ballesteros, Berger, Caraballo, & Kegler, 2008). Iacobelli et al. (2008) found that current smokers perceived that the risk of an accident while smoking was drastically lower than that perceived by the non-smoking public. This finding is consistent with current smokers’ tendencies to minimize the health impact of their own smoking behavior (Weinstein, Marcus, & Moser, 2005). Thus, knowledge of an elevated risk of accidents for smokers is not as common as knowledge of an elevated risk of health problems associated with smoking, such as cancer or respiratory disease (Iacobelli et al., 2008).
Cigarette smoking is a modifiable behavior at the individual level. However, efforts to change individual behaviors often have little effect at the population level (Diekman et al., 2008). Environmental influences at community and societal levels interact with individual-level human behavior (Ettner & Grzywacz, 2001). The adoption of nationwide fire-safe cigarette laws may be one example of the interplay between environmental and individual factors (Diekman et al., 2008). Successful efforts to reduce smoking and adhere to workplace fire protection recommendations may translate into a reduction in residential fire mortality rates.
Worksite cleanliness was found to be related to increased smoking intensity in manufacturing workers but not related for office or sales workers. Arguably, cleanliness of the workplace environment may be associated with worksite smoking policies; workplaces with full smoking bans are more likely to be clean compared with worksites with absent or less directive policies. In Korea, smoking has been prohibited inside major public buildings such as hospitals, schools, or theaters since 1995 and in all business offices since 2015 (Korean Ministry of Health and Welfare, 2015). Blue-collar workers such as manufacturers are less likely than office or service workers to be employed at worksites with restrictive smoking policies (Honjo et al., 2006). According to the study by Heloma and Jaakkola (2003), a long-term effect of the national smoke-free workplace law is less exposure to environmental tobacco smoke (ETS). Also, implementation of the law seemed to be linked to changes in employee attitudes favoring more restrictive workplace smoking policies. Reduction of ETS exposure and attitude change was strongest in industrial workplaces. The systematic review by Fichtenberg and Glantz (2002) revealed that totally smoke-free workplaces had about twice the impact on rates of smoking cessation as workplaces with less restrictive policies, such as smoking only in designated areas. As a clean workplace was shown to influence the amount workers smoked, maintaining workplace cleanliness with a strict non-smoking policy is strongly recommended to reduce workers’ exposure to ETS.
Noise is a common occupational hazard. Long-term exposure to noise damages the hair cells of the organ of Corti in the inner ear and eventually leads to noise-induced hearing loss (Mohammadi, Mazhari, Mehrparvar, & Atttarchi, 2009). Studies by Topplia, Pyykko, Starck, Kaksonen, and Ishizaki (2000) and Nakanishi et al. (2000) found that cigarette smoking was significantly associated with a higher likelihood of noise-induced hearing loss. After adjusting for cardiovascular events and risk factors, Blue Mountains Hearing Study participants demonstrated that current smoking was related to hearing loss (Gopinath et al., 2010). A more marked association between current smoking and hearing loss was observed for participants who did not report significant occupational noise exposure, thus indicating that noise exposure may mask the harmful effect of smoking (Gopinath et al., 2010). Data from a large community-based survey supported the growing body of evidence that ex- and current smokers have more hearing impairment than lifetime non-smokers, even after controlling for occupational noise exposures (Palmer, Griffin, Syddall, & Coggon, 2004). Moreover, the joint effects of smoking and exposure to noise significantly increased hearing impairment in young people aged 20 years to 40 years (Ferrite & Santana, 2005).
The authors found that workers who were exposed to occupational noise were more likely to smoke. Palmer et al. (2004) asserted that smoking workers should be encouraged to refrain from both smoking and exposure to noise. Smokers should periodically participate in smoking cessation programs.
Although Li et al. (2010) and Radi et al. (2007) found that smoking intensity was related to job strain and decision latitude, this study did not find any significant associations between smoking intensity and job strain or decision latitude in the occupational groups investigated. Possible reasons for these discrepancies could include differences in the intensity of job strain, the nature of work across different jobs, and varying social capital. Furthermore, smoking intensity may also be masked by the role of addiction and nicotine (Parascandola, 2011), which varies among individuals and was not assessed in this study.
This study has several limitations. One weakness was that workers may have under-reported data about work environments and occupational hazards. Therefore, the results may not be generalizable, and it may be difficult to reach definite conclusions. Clearly, longitudinal studies using both self-reported and objective measurements of work environment variables are needed. It is also necessary to investigate how smoking culture in various countries influences workers’ smoking. Although the researchers accounted for several confounding variables, other potential factors were not accounted for in the analyses. For example, self-belief in smoking cessation, motivation, or spousal support may influence smoking behavior. Furthermore, smoking intensity was not validated by any biochemical indicators.
Conversely, this study had several strengths. The study is one of the few to examine the impact of work conditions, psychological and physical work environments, and occupational hazards on smoking intensity. Several studies about smoking have focused on only one aspect of the work environment. Also, for most other studies, the sample included only a small number of workers from one workplace, whereas this study drew participants from three occupational groups within a large population-based sample.
Implications for Practice
The underlying impact of smokers’ individual characteristics and their work environments on rates of smoking must be better understood. These findings emphasize that supporting co-workers’ smoking cessation should be considered when implementing a workplace smoking cessation program for office and sales workers. Furthermore, a tailored smoking cessation program focused on the physical work environment (e.g., establishing clean worksites and reducing exposure to occupational noise) should be developed. Workers and health care providers should establish workplace support and tobacco control measures to improve success of workplace smoking cessation efforts. More research is needed to determine the precise associations between various aspects of work environments and smoking.
Applying Research to Practice
The study found that office workers and the sales force who had smoking co-workers at the workplace were more likely to smoke than those who did not. More importantly, exposure to occupational noise and dirty workplaces were significant factors increasing smoking intensity for manufacturers. These findings emphasize that supporting co-workers’ smoking cessation is an important factor to be considered when implementing a workplace smoking cessation program for office workers and sales force. A tailored smoking cessation program that focuses on physical work environments as well as co-workers’ support should be developed for Korean workers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Sungshin Women’s University Research Grant 2013-1-21-007.
Author Biography
Young-Ju Kim, RN, ACNP, PhD, is associate professor at the Sungshin Women’s University College of Nursing in Seoul, Korea. She is conducting research on community-based health promotion.