
Abstract
Nurses often struggle with maintaining a healthy lifestyle. While nurses are often assumed to have the knowledge to participate in health-promoting behaviors, this knowledge may not translate into sustainable change in behavior. The purpose of this descriptive study was to compare nurses’ health behaviors with residents in the community where the nurses were employed. Participants (N = 166) completed the Health Promoting Lifestyle Profile–II survey (HPLP-II) along with a demographic survey. The HPLP-II consists of six dimensions of a health-promoting lifestyle: (a) spiritual growth, (b) health responsibility, (c) physical activity, (d) nutrition, (e) interpersonal relations, and (f) stress management. Both groups scored the highest in spirituality followed by interpersonal relations. However, scores for the other HPLP-II dimensions ranked differently between the two groups. Nurses scored higher in health responsibility while the community participants scored higher on nutrition. Both groups scored the lowest on stress management and physical activity. Significant differences between groups were found only on the health responsibility dimension of the HPLP-II survey with nurses scoring higher. While nurses overall did not do any better than the general population in participating in a healthy lifestyle, patient stakeholders feel strongly that nurses should role model healthy behaviors. Employers need to be better prepared to support nurses to participate in a healthy lifestyle. Success can come from even small incremental changes (e.g., walking groups, team challenges, taking stairs) within the work environment. Furthermore, evidence-based practice teams that include administration, management, and staff are positioned to contribute through education and development of innovative workplace wellness programs.
Keywords
Introduction
Stressful work environments (e.g., shift work with long hours, high patient acuity, and lack of organizational support) have been cited as significant factors affecting health-promotion behaviors in nurses (Buss, 2012; Kim et al., 2013; Kurnat-Thoma, El-Banna, Oakcrum, & Tyroler, 2017; Ross, Bevans, Brooks, Gibbons, & Wallen, 2017). Ineffective coping mechanisms to this stress may result in behaviors such as unhealthy eating and decreased physical activity (Hensel, 2011, as cited in Kurnat-Thoma, El-Banna, Oakcrum, & Tyroler, 2017) leading to obesity and the development of chronic diseases such as diabetes and cardiovascular disease (Kurnat-Thoma et al., 2017; Phiri, Draper, Lambert, & Kolbe-Alexander, 2014). Historically, nurses have been expected to role model the behavior they promoted with patients. However, more recently, the ability to meet this expectation has come into question. While the benefits of behaviors such as healthy eating and physical activity are well documented, nurses may struggle just as much if not more than many in the general population (Ross et al., 2017).
Background
Based on education and experience, nurses are often assumed to be knowledgeable regarding the importance of health-promoting behaviors such as healthy eating, physical activity, and stress management. However, this knowledge may not translate into sustainable change (Ross et al., 2017). Several research studies support that nurses do not practice positive health behavior and that a large percentage of nurses are overweight or obese (Nahm, Warren, Zhu, Minjeong, & Brown, 2012; Zitkus, 2011). For example, Nahm et al. (2012) reported a mean body mass index (BMI) of 28.2 kilograms (kg)/meters (m)2 and a 59.2% prevalence of overweight/obesity in a sample of 183 nurses. In a recent literature review by Ross et al. (2017), prevalence of overweight nurses (nurses with a BMI of 25 kg/m2 to 30 kg/m2) ranged between 30% and 53%, similar or higher than the 33.1% prevalence of overweight people in the general population. Buss (2012) showed that the prevalence of overweight and obesity varied according to the country of origin, race and ethnicity, and the age of nurse participants. In the United States, studies reported a range of obesity from 23% to as high as 61.4%.
Blake and Harrison (2013) found incongruity between attitudes toward being role models for patients versus nurses’ health behaviors. While participants endorsed the belief that nurses should be role models for their patients, many did not engage in healthy lifestyle practices themselves. Out of 540 nurses, 24% were overweight/obese, 47% were physically inactive, 73% did not meet recommendations for healthy eating, 40% reported binge drinking, and 17% were smokers (Blake & Harrison, 2013). Proper nutrition and physical activity are considered the first line of defense to combat obesity and to prevent cardiovascular disease (American Heart Association, 2016). A sedentary lifestyle can be deadly, and even if an individual participates in high levels of physical activity, it does not mitigate the effects of prolonged sitting on mortality risk (Matthews, George, & Moore, 2012). Research supports that nurses who maintain a physical activity program and get adequate sleep are at lower risk for obesity even amid a stressful workplace (Han et al., 2012).
Health care behaviors of providers affect both personal health and their provision of health promotion services to patients. Zhu, Norman, and While (2011) reported that healthy weight doctors and nurses were more likely than those who were overweight to provide overweight or obese patients with advice and strategies to achieve weight loss. Lobelo, Duperly, and Frank (2009: as cited in Chiou, Chiang, Huang, & Chien, 2014) argued that there is compelling evidence that the health of doctors matters and that the doctors’ personal physical activity habits influence their clinical attitudes and counseling of patients regarding physical activity. General practitioners who smoked themselves were less likely to engage in smoking cessation for their patients (Stead et al., 2009 as cited in Chiou et al., 2014). These findings suggest that one of the most important things that nurses can do is maintain their health and well-being, thereby encouraging patients to do the same.
Among many other findings, the landmark Nurses’ Health Study supports (Belanger, Hennekens, Rosner, & Speizer, 1978; Morabia, 2016) the vital role that lifestyle factors play in the prevention of chronic disease. Findings from this study indicated that most of the heart attacks in their participants were preventable through regular physical activity; maintaining a healthy weight; making dietary changes such as reducing saturated fats and increasing fiber, fruits, and vegetables; and not smoking (Manson, 2000). Findings from the Nurses’ Health Study II showed a significant association between nonsmoking, a healthy BMI, physical activity, and healthy eating with lower cardiovascular heart disease (CHD) risk. A prospective analysis of lifestyle factors was conducted among 88,940 female nurses, ages 27 to 44 years, following them from 1991 to 2011. Approximately 73% of CHD cases were attributable to poor adherence to a healthy lifestyle (Chomistek et al., 2015).
Recent studies (within the last 10 years) examining the differences between nurses’ health behaviors and the general population are lacking. The most recent related study found was the National Health and Nutritional Examination Survey (NHANES) published in 2007. Data revealed that registered nurses were more obese (31%) compared with the general population (27%) (National Institutes of Health, 2007). An even older study examined nursing students’ health-promoting behaviors with other college students and the general population. Clément, Jankowski, Bouchard, Perreault, and Lepage (2002) found that nursing students demonstrated more health-promoting behaviors (i.e., women’s health screenings, non-smoking) than the general population. However, no significant differences were found for most of behaviors examined. The purpose of this study was to contribute to the recent body of knowledge regarding nurses’ health behaviors and how they compare to a community population in southern New Mexico.
Theoretical Framework
The current work was based on Pender’s (1996) Health Promotion Model (HPM). Pender based the HPM on the Health Belief Model originally developed in the 1950s. She added to this model by proposing that individuals may adopt lifestyles and patterns of behavior aimed at attaining a higher level wellness and health state, not just the avoidance of illness. The HPM consists of three major concepts: (a) individual characteristics and experiences, (b) behavior-specific cognitions and effects, and (c) behavioral outcomes. Individual characteristics and experiences include prior-related behavior and personal factors. Prior-related behavior is the frequency of the behavior in the past. Personal factors include biological, sociocultural, psychological, and general characteristics that may influence behavior such as age, ethnicity, health status, and socioeconomic status (Pender, Murdaugh, & Parsons, 2010). Behavior-specific cognitions and effects include perceived benefits and barriers, self-efficacy, activity-related affect, and interpersonal and situational influences (Pender et al., 2010). Included in the assessment are benefits (e.g., healthy weight) and barriers (e.g., costs) associated with undertaking a health behavior. Activity-related affect is the subjective feeling connected to the behavior. Examples of interpersonal influences are family’s, peers’, and role models’ support of the health activity. Situational influences refer to the environmental factors that can increase or decrease the commitment to the behavior (Pender et al., 2010).
The hypothesis for this study was that nurses would participate in less health-promoting behaviors than the community population as measured by the Health Promoting Lifestyle Profile–II (HPLP-II; Walker & Hill-Polerecky, 2005).
Pender’s model (Pender, 1996) provided the framework for this study. Healthy lifestyles involve a multi-dimensional pattern of self-initiated actions that serve to maintain or enhance the level of wellness, self-actualization, and fulfillment of the individual. To measure health-promoting behaviors, the HPLP-II was developed. Derived from Pender’s HPM, the HPLP-II includes six dimensions of a health-promoting lifestyle: (a) spiritual growth, (b) health responsibility, (c) physical activity, (d) nutrition, (e) interpersonal relations, and (f) stress management. The HPM provided the foundation for the development of the HPLP-II used to assess healthy behaviors in this study.
Method
A descriptive study was employed to examine the differences in health-promoting behaviors between nurses and residents of the surrounding community population. Nurse participants were recruited from two hospitals in southern New Mexico. Participants from the community population were recruited from the community that these two hospitals serve. Participants were recruited by word of mouth and flyers posted at the hospitals and local businesses and organizations. Based on a power analysis using an alpha of .05, a power of .80, and an effect size of .50, a minimum of 63 participants per group were required.
Human Subjects Approval
Approval to conduct the study was obtained through the Institutional Review Board at New Mexico State University. Written informed consent was obtained and stored in a locked filing cabinet only accessible to the researcher. Participants were informed that their participation was voluntary and they could withdraw at any time. No names or personal information were collected on the demographic and survey data forms. A unique identifier was used to connect the participant’s demographic questionnaire to their survey responses.
Measures
Participants were asked to complete a one-page demographic questionnaire and the HPLP-II survey. Example items on the demographic survey included age, gender, ethnicity, perceived health status, and presence of chronic diseases such as diabetes, hypertension, and asthma. For perceived health status, participants were asked to rate their health on a scale of 1 to 4 (1 = poor, 2 = fair, 3 = good, and 4 = excellent). The HPLP-II, developed by Walker and Hill-Polerecky (2005), was used to measure health-promoting actions. Modified from the original HPLP (Walker, Sechrist, & Pender, 1987), the HPLP-II is a 52-item, 4-point (1 = never, 2 = sometimes, 3 = often, 4 = routinely) Likert-type scale that assesses the frequency with which individuals report engaging in activities directed toward maintaining or enhancing their levels of well-being, self-actualization, and fulfillment.
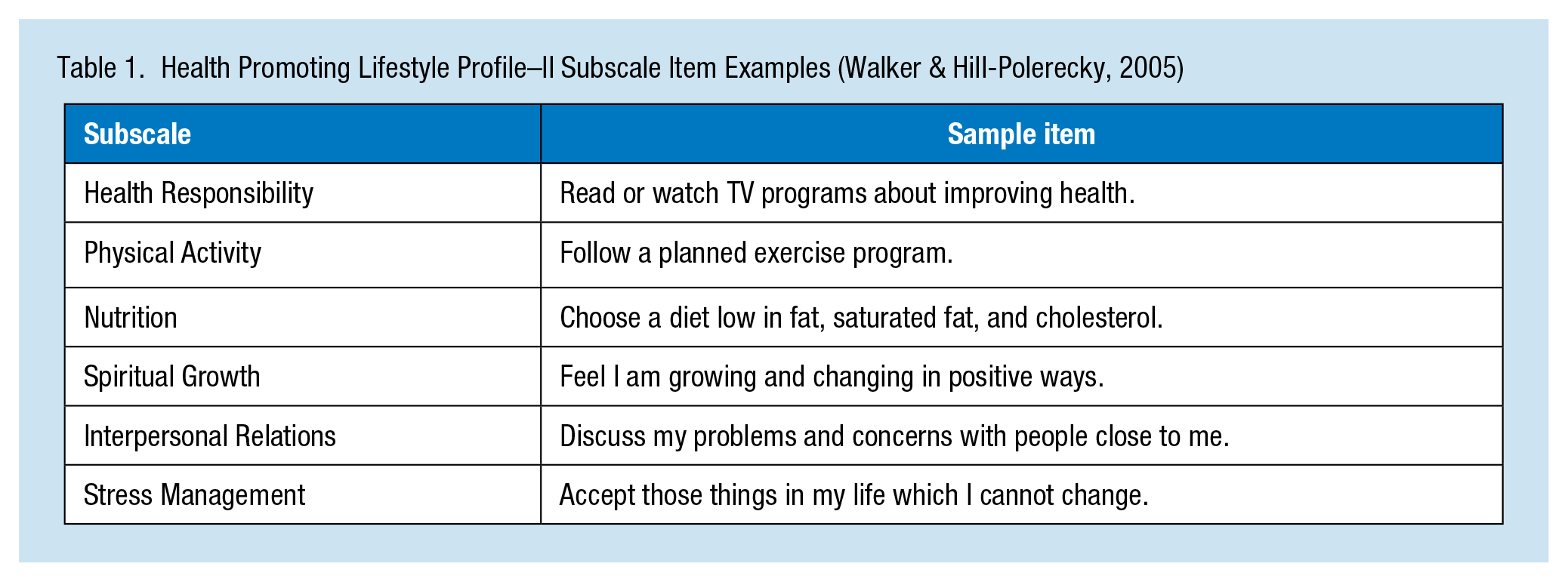
Six dimensions of a health-promoting lifestyle have been identified through principle axis factor analysis (Walker & Hill-Polerecky, 2005). Except for the physical activity and stress management dimensions, there were nine items within each dimension with scores ranging from 9 to 36. For the physical activity and stress management dimensions, there were eight items each with scores ranging from 8 to 32. Mean subscale scores were obtained by summing the responses for each item and dividing by the number of items for that subscale (either 8 or 9). The overall HPLP-II scale score is calculated by summing the responses for all 52 items (ranging from 52 to 208). Total scale mean scores were calculated by summing item responses for all 52 items and then dividing by 52. Higher scores are indicative of more health-promoting behaviors in general or within a specific subscale. Cronbach’s alphas for the current study were all in the acceptable range: health responsibility (.77), physical activity (.87), nutrition (.74), spiritual growth (.85), interpersonal relations (.83), stress management (.77), and for the total HPLP-II scale (.93). Example items from each subscale are found in Table 1.
Health Promoting Lifestyle Profile–II Subscale Item Examples (Walker & Hill-Polerecky, 2005)
Data Analysis
Descriptive statistics were performed on the demographic information. To assess differences between the nurse and community population groups on demographic variables (e.g., gender, ethnicity, and education), Cramer’s V was used. For purposes of describing the study population and their behaviors, independent-sample t tests for between-group (nurse vs. community population) differences on the six HPLP-II subscales and overall score were conducted. Independent-samples t tests were also used to examine the effects of gender, ethnicity, and education on HPLP-II scores for the two groups. ANOVA was used to examine the effects of perceived health status and age on HPLP-II scores. Data were analyzed using the Statistical Package for Social Science (SPSS) version 25.
Results
Of the 200 questionnaires distributed to volunteer participants, 166 were returned resulting in a response rate of 83%. Of the 103 nurses and 63 adults from the community population, most were female (77%) with a mean age of the total sample being 42 years (range = 23-63 years). A total of 105 participants were White (67%), 46 (29%) were Hispanic, one (0.6%) was African American, one (0.6%) was Asian, one (0.6%) was Native American, and seven (4.4%) claimed “other” ethnicity. Much of the sample had a college degree (91%) and were married (72%). Participants stated they had one or more of the following chronic diseases: hypertension (15%), diabetes (6%), arthritis (6%), asthma (11%), and other (14%).
When differences between the groups were examined, very few significant differences were found between groups on their demographic characteristics (Table 2). Significant differences were found between nurses and the community population for education, gender, and presence of asthma. Significantly, more nurses were college educated (Cramer’s V = .284, p ≤ .0001), female (Cramer’s V = .183, p = .025), and reported more asthma (Cramer’s V = .234, p = .011).
Differences Between Nurses and Community Population on Selected Demographic Characteristics
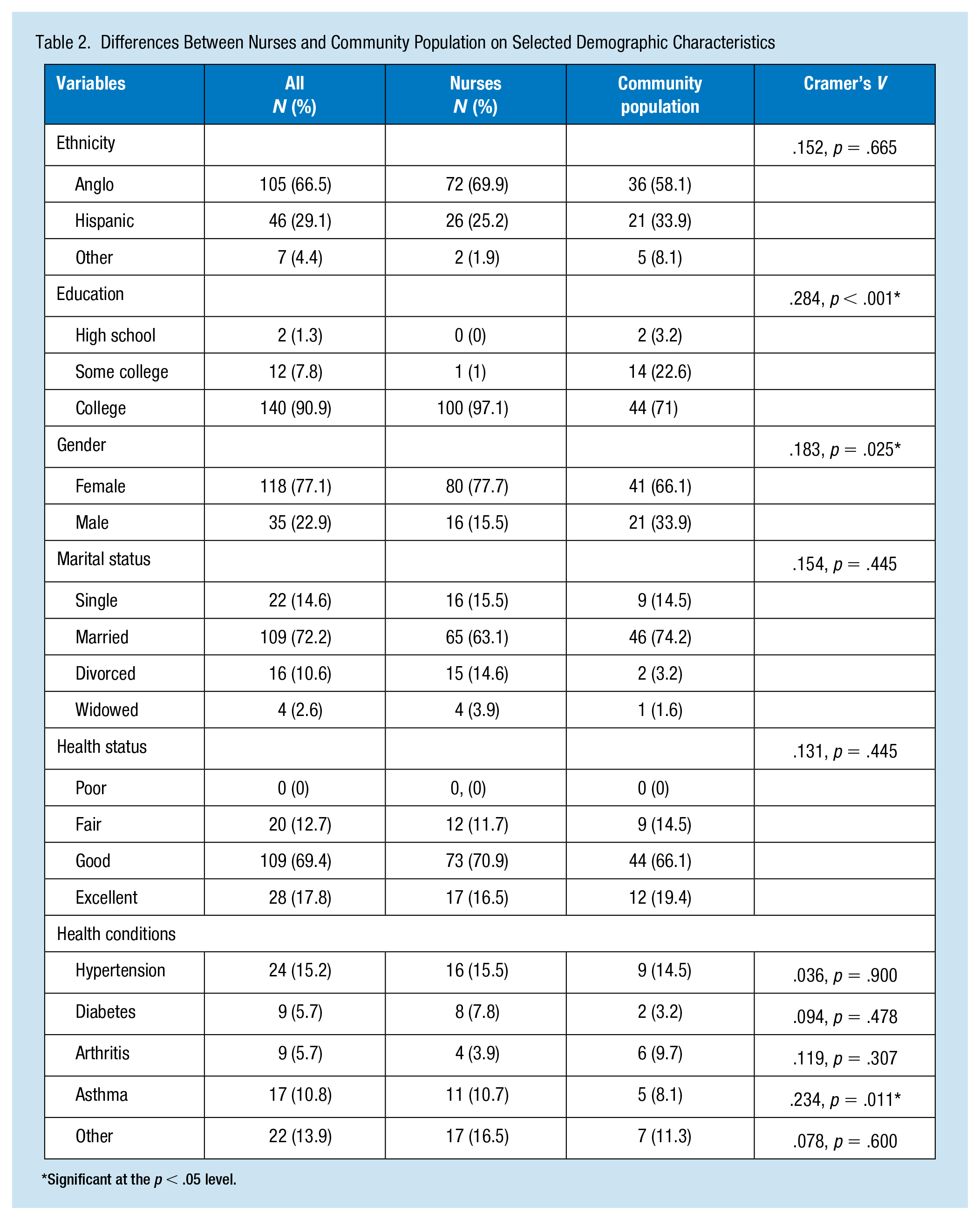
Significant at the p < .05 level.
Nurses scored the highest in spirituality (M = 25.77, SD = 4.15) followed by interpersonal relations (M = 25.28, SD = 4.32), health responsibility (M = 22.10, SD = 4.10), nutrition (M = 21.34, SD = 4.29), stress management (M = 18.04, SD = 3.95), and physical activity (M = 17.40, SD = 5.35), respectively. For the community sample, participants also scored highest in spirituality (M = 25.75, SD = 4.15), followed by interpersonal relations (M = 24.92, SD = 4.79), nutrition (M = 20.59, SD = 4.56), health responsibility (M = 19.74, SD = 4.56), stress management (M = 18.16, SD = 4.18), and physical activity (M = 17.43, SD = 5.14), respectively.
For the HPLP-II, there was a significant difference in the scores for nurses (M = 22.09, SD = 4.06) versus the community population (M = 19.74, SD = 4.56) on the Health Responsibility subscale, t(150) = 3.30, p = .002 (Table 3). Even though not statistically significant, nurses also scored slightly higher than the community population on the Nutrition (M = 21.34 vs. 20.59) and the Interpersonal Relations (M = 25.28 vs. 24.91) subscales of the HPLP-II.
Differences Between Nurses and Community Population on HPLP-II Dimensions
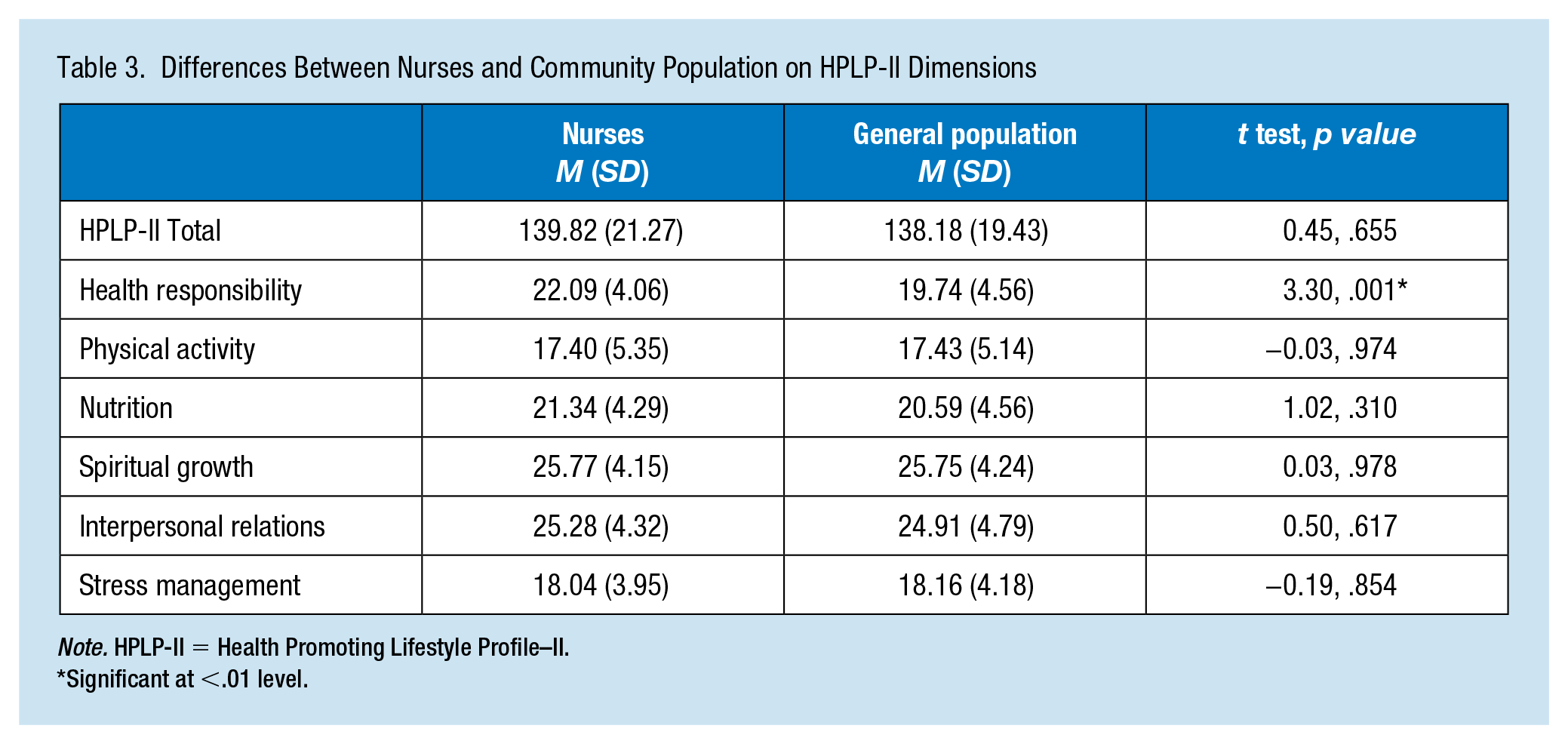
Note. HPLP-II = Health Promoting Lifestyle Profile–II.
Significant at <.01 level.
The community population did slightly better on the Physical Activity (M = 17.43 vs. 17.40) and Stress Management (18.16 vs. 18.03) subscales of the HPLP-II. Females (M = 21.79 vs. 19.56) scored significantly higher on the Health Responsibility subscale than males, t(145) = −2.65, p = .009. Nurses and the community population both scored significantly higher on the Physical Activity subscale based on health status. A one-way ANOVA showed that the effect of perceived health status on HPLP-II scores was significant for nurses, F(2, 88) = 8.77, p = .010, and for the community population, F(2, 51) = 8.03, p = .001. The better the health status, the higher the mean scores for nurses (excellent = 19.05; good = 17.90; fair = 13.31) and the community population (excellent = 22.01; good = 17.24; fair = 13.17).
Discussion
Nurses only scored significantly better than the community residents on the health responsibility dimension of the HPLP-II. This finding is not surprising when you examine the specific questions on the subscale. Items refer to things such as questioning health professionals, reporting signs and symptoms, and discussing health concerns with health professionals. As nurses are health professionals themselves, their comfort level and knowledge expertise would put them at an advantage over the community population. It was somewhat surprising that nurses had a significantly higher rate of asthma than the community population. Furthermore, nurses did not fare any better than the community population on all other chronic diseases assessed.
While not significantly different, nurses scored lower on physical activity and stress management. These findings support the current literature that being overweight is a significant problem for nurses. Reported lack of regular physical activity may contribute to this problem. It is also not surprising that health status played a significant role in health-promoting behaviors in this study. Findings from research studies overall support that nurses that rate their health poor report lower physical activity and higher rates of being overweight and obesity. For example, Choi and Sung (2013) examined the relationship between perceived health status and health-promoting behavior of 194 clinical nurses. Perceived health status showed a positive correlation with health-promoting behavior (r = .30, p < .001).
Results support that nurses share the same challenges as the community population in promoting a healthy lifestyle. Health education is only one aspect in adopting a healthy lifestyle. It is also important to reduce barriers and increase resources and support for participating in such behaviors. Barriers include lack of time, too tired, shift work, and lack of resources (Phiri et al., 2014). Workplace wellness programs have shown to be an effective approach to promoting employee health. Soldano (2016) discussed the following common themes across best practice programs: (a) commitment by the organization, (b) incentives for participation, (c) evidence-based interventions, (d) effective implementation strategies, and (e) program evaluation. Some of the qualities of the best performing programs included a focus on risk reduction, personalization, incentives, and including family.
For nurses, a promising 12-week program called “Nurses Living Fit” resulted in a significant decrease in BMI and waist circumference compared with a group that did not participate in the program (Speroni, Williams, Seibert, Gibbons, & Earley, 2013). Descriptively, participants indicated they had improved their overall lifestyle behavior including drinking more water, improved sleep, and better interpersonal relationships. Themes from the qualitative evaluation of the program revealed that participants wanted more education, personalized strategies, and for the program to be longer (Speroni et al., 2013).
Innovative longer term programs such as the Exercise Is Medicine (EIM; 2016) program has gained recognition in both professional and patient populations. EIM is a global health initiative co-launched in 2007 by the American Medical Association and the American College of Sports Medicine (ACSM). First, an initial assessment of current physical activity behavior is done. If not exercising according to the recommended guidelines of at least 150 minutes of moderate activity each week, physical and behavioral readiness to initiate or engage in more physical activity, brief counseling, and development of a tailored physical activity prescription is completed. The program includes a referral to a physical activity professional for extra education, support, and “filling” the exercise prescription if needed. Results have yielded better preventive care, improved health outcomes, and health care cost reductions (EIM, 2016; Gallegos-Carrillo, García-Peña, Salmerón, Salgado-de-Snyder, & Lobelo, 2017).
Nurses are in a unique position to serve as role models for healthy lifestyles. Many in society, particularly patient consumers, believe that health care providers should “practice what they preach.” Behind this assumption is the belief that others are more likely to comply with advice about healthy behaviors if it is modeled by those giving it (Blake, Malik, Mo, & Pisano, 2011, in Chiou et al., 2014; Ross et al., 2017). However, results from a recent Delphi study (Kelly, Wills, Jester, & Speller, 2017) provides a controversial perspective on this expectation. A total of 25 participants drawn from a variety of stakeholders (e.g., nursing employers, patients, nursing students, and nurses) answered questions related to perceptions about nurses being role models of healthy behaviors for their patients. Both nursing students and practicing nurses believed that role modeling was an individual preference not a professional duty and agreed that it was more important to be viewed as “human” with the same challenges of others in maintaining a healthy lifestyle. Contrary to this finding was that patient stakeholders shared negative perceptions of visibly unhealthy health care professionals and felt that the nurses’ professional skills and credibility are influenced by their appearance (Kelly et al., 2017).
The benefits of a health-promoting lifestyle are well known. Research supports that people who maintain this lifestyle are happier, more productive, and tend to use less health care resources (Casselman, 2017; Hart, 2013). Nurses experience the same challenges that the general population face in maintaining a healthy lifestyle. A more realistic expectation may be to hold nurses to the same rather than higher standard of health-promoting lifestyle than the general population. An expanded meaning of “role modeling” that included sharing personal challenges and strategies for success may be more effective for both nurses and patients in maintaining a healthy lifestyle.
Rather than victim blaming nurses for not epitomizing the picture of health, employers of nurses need to be better prepared to support nurses to reach and maintain a healthy lifestyle. Development of an evidence-based practice team consisting of administration, management, and staff to focus on creative strategies/workplace wellness programs to support a healthy staff would be one such approach. Workplace wellness models such as the ones described here could be tailored to meet the specific needs of staff. Creative ways to encourage nurses to participate in such programs given the identified stressful work environments may be difficult but the returns are worth it in the long term.
Implications for Occupational Health Nursing Practice
Nurses experience the same challenges as the general population in maintaining a healthy lifestyle. Employers need to step up and work with nurses as an evidence-based practice team to focus on developing workplace wellness programs to support a healthy staff. While evidence-based programs such as the “Nurses Living Fit” or the “Exercise Is Medicine” have shown effectiveness, success can come from even incremental changes within the work environment.
Arena et al. (2013) shared some practical examples that include (a) creation of a safe walking path (both inside and outside), (b) developing creative team/personal challenges (e.g., highest average steps/day over a time period using wearables provided by employer), (c) integrating more physical activity in the workday (e.g., using stairs vs. elevator, parking car farther away, riding bicycle to work), (d) forming varying levels of walking groups with some including families, (e) healthy recipe contest, and (f) healthy choices with nutrition labeling at the point of purchase (e.g., cafeteria/vending machines). In addition to these ideas, Ross et al. (2017) provided other tips for increasing health-promoting behaviors in nurses. Examples include encouraging a culture of civility and support in the workplace, hold standing or walking meetings, hold in-service sessions on healthy behaviors, organizing healthy activities before and after shifts particularly for physical activity and use of an identified quiet space such as a sleep pod for a moment of relaxation/meditation. Nurses can be at the forefront in advocating for change needed to promote a culture of health and wellness in the workplace.
Applying Research to Practice
It is critical that employers and nurses work together as an evidence-based practice team to create novel strategies/programs that promote health in the nursing workforce. Incremental change such as using stairs vs. elevators and parking cars farther away may be the most successful, particularly at the beginning of such an adventure. Creating an infrastructure that promotes healthy behaviors (e.g., a safe walking path and healthy choices in the cafeteria and vending machines at work) is critical to facilitate change. Occupational health nurses can be the ones to lead the change through a combination of individual and team strategies and encouraging a culture of health and wellness in the workplace.
Footnotes
Conflicting of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Rebecca Keele is currently a professor within the College of Nursing at Texas Woman’s University. Prior to that, she was faculty at New Mexico State University for 20 years. Dr. Keele has been a public health/community health nurse (PHN/CHN) for over 25 years with experience working in all facets of PHN/CHN. Her research interests have primarily centered on promoting a lifestyle, particularly healthy eating and physical activity with underserved populations.