
Abstract
Immigrants account for a significant proportion of the nursing workforce in the United States (U.S.). Although different cultural backgrounds may affect immigrant nurses’ perceptions of work and occupational health risks, little research has been conducted. Defining immigrant nurses as those who received initial nursing education in foreign countries, this study examined the differences in work-related perceptions and experiences of musculoskeletal (MS) symptoms and injuries between U.S.-educated and foreign-educated nurses. We analyzed data from a cross-sectional study using a statewide random sample of 419 California registered nurses. Foreign-educated nurses reported a more positive safety climate (p = .017) and perceived their jobs as less demanding (p = .008) than did U.S.-educated nurses. The prevalence of work-related MS symptoms was significantly lower in foreign-educated nurses than in U.S.-educated nurses (p = .044), but the difference was not significant in the multivariable analyses. Positive safety climate was significantly associated with a decreased risk of work-related MS symptoms and injuries, and this relationship was greater among U.S.-educated nurses than among foreign-educated nurses. Our findings suggest that immigrant nurses may have different perceptions about safety climate and job demand, which may modify their occupational health risks.
Keywords
Background
The international migration of health care workers, including nurses, has emerged as a global phenomenon over the past several decades (Organisation for Economic Co-operation and Development, 2010). In the United States (U.S.), there are approximately 3 million registered nurses, a significant portion of whom (14.6% in 2014) are immigrants (Hohn, Witte, Lowry, & Jose, 2016). States with the highest percentages of immigrant nurses include California (36.5%), New York (29.4%), and Florida (27.2%) (Altorjai & Batalova, 2017). Immigrant nurses in the U.S. are predominantly from developing countries such as the Philippines, the Caribbean, and South Africa (Li, Nie, & Li, 2014).
Immigrant nurses may experience positive and negative aspects of work environments in the U.S. and such differences may affect their perceptions about their work and related health and safety risks (Goh & Lopez, 2016; Li et al., 2014; Moyce, Lash, & de Leon Siantz, 2016; Xu, 2007). Studies have found that U.S. hospitals generally offer higher salaries and lower workloads and are better staffed than hospitals in immigrant nurses’ home countries, which may possibly contribute to immigrant nurses’ positive work experiences (Li et al., 2014; Magnusdottir, 2005). However, immigrant nurses can encounter increased occupational stress due to difficulties in communication and interpersonal relationships with patients and other workers from different cultural backgrounds. Difficulties may also stem from differences in the scope of nursing practice in the U.S. compared to their home countries (Callaghan, Tak-Ying, & Wyatt, 2000; Goh & Lopez, 2016; Jose, Griffin, Click, & Fitzpatrick, 2008; Xu, 2007, 2010).
Many reports have addressed health disparities and inequities for immigrants in general (Edward, 2014; Schenker, 2010). Studies have reported an increased risk for occupational injury among immigrant workers, generally those in occupations that require less education and job training, offer lower wages, and necessitate more physical labor, such as agricultural workers and construction workers (Kosny et al., 2012). Although these employment features do not reflect the general characteristics of the nursing population, the association between immigration status and work-related health might apply to nurses. However, some studies using national survey data reported lower occupational injury rates among foreign-born workers than among U.S.-born workers (Xiang et al., 2012; Zhang et al., 2009). Studies have indicated that immigrants are less likely to report work-related injuries due to language barriers, different perceptions about injury severity, and fears about job security (Kosny et al., 2012).
There is little information available on the impact of immigration on occupational health disparities among nurses, despite the large number of immigrant nurses in the nursing workforce. In general, U.S. nurses are at high risk for work-related injuries. In a survey by the American Nurses Association, over 40% of nurses reported experiencing at least one work-related injury in a 12-month period (American Nurses Association, 2011). Among various work-related health problems, musculoskeletal (MS) injuries are the most common, with the prevalence of MS problems in the nursing profession ranging from 26% to 55% depending on body region (e.g., lower back, shoulder, neck, upper extremity) (Davis & Kotowski, 2015). However, little is known about the relationship between immigration status and work-related injury incidence among nurses. Research is needed to fill this knowledge gap and to address the needs of the growing immigrant nursing workforce. The aim of this study was to examine differences in the perceptions of work environment and work-related MS symptoms and injuries between U.S.- and foreign-educated nurses and to examine whether immigration status moderates those relationships.
Method
Data and Study Sample
This study was a secondary analysis of cross-sectional survey data of 419 California registered nurses. The 2013 California Nurses Safety Survey was conducted using postal and online survey formats among a random sample of 2,000 actively licensed nurses selected from the 2012 California Board of Registered Nurses list (Lee, Lee, & Gershon, 2015). Sampling was stratified by nine regions in California (Northern counties, Sacramento region, central five-county San Francisco Bay Area, remainder of San Francisco Bay Area, Central Valley and Sierra, Central Coast, Los Angeles, Inland Empire, and Border counties) using the method by Spetz, Keane, Chu, and Blash (2013). Samples were selected proportionately by the registered nurse population density in each region. Detailed information about the survey methods is available elsewhere (Lee, Lee, & Gershon, 2015).
Measures
Work-related MS symptoms and injuries
The outcome variables for this study were binary measures of work-related MS symptoms and injuries in the past 12 months. MS symptoms were defined as pain, aching, stiffness, burning, numbness, or tingling in the lower back, neck, shoulder, or wrist/hand. MS symptoms were measured using questions modified from a valid and reliable instrument, the Nordic musculoskeletal questionnaire by Kuorinka et al. (1987), and the modified questions were used in other studies (Lee, Faucett, Gillen, Krause, & Landry, 2013; Lipscomb, Trinkoff, Geiger-Brown, & Brady, 2002). Work-related symptoms were identified if the respondent answered that the symptom was caused or made worse by work. For work-related injuries, the respondents were asked whether they had experienced any injuries or health problems at work in the past 12 months. For the respondents who experienced a work-related injury or health problem, subsequent questions were given to ask about the type of injury or problem (strains/sprains, sharp injuries, exposure to blood or body fluids, exposure to chemicals, exposure to violence, and other) and whether they had sought health care, missed work, or reported the injury to their supervisor.
Immigration status
The primary independent variable was immigration status, as defined by the country of initial nursing education. The sample was divided into U.S.-educated nurses and foreign-educated nurses.
Demographic and job characteristics
Demographic characteristics included age (years), gender (female/male), race/ethnicity (non-Hispanic White/African American/Hispanic/Asian/Other), body mass index [BMI] (kg/m2), and highest level of education (diploma or associate/bachelor’s or higher degree). Job characteristics included work area (urban/suburban/rural), work setting (hospital/ambulatory/nursing home/other), schedule (full-time/part-time or per diem), average hours worked per shift, average hours worked per week, work status (full-time/part-time or per diem), job title (staff nurse/nurse manager/nurse practitioner/other), job tenure in nursing (years), and patient handling duty (yes/no).
Perceptions about work and work environment
The Job Content Questionnaire (JCQ; Karasek et al., 1998) was used to assess how nurses perceived their work, including psychological job demand, job control, job satisfaction, and intent to leave current job. Job demand (five items) and job control (nine items) were measured using a 4-point Likert-type scale (1 = strongly disagree to 4 = strongly agree), and we calculated the scale scores using the formulas by Karasek et al. (1998). The job demand score ranged from 12 to 48, and higher scores indicate higher psychological workload or effort required for the job. The job control score ranged from 24 to 96, and higher scores indicate that they exert greater control over their work through the use of their skills and decision-making authority. Job strain was derived as the ratio of job demand to job control and ranged from 0.125 to 2. Higher job strain scores indicate higher job demand combined with lower job control. Job satisfaction was measured using a single question on a 4-point Likert-type scale (1 = not at all satisfied to 4 = very satisfied). Intent to leave current job was measured on a 3-point Likert-type scale (1 = very likely to 3 = not at all likely).
Safety climate and people-oriented culture were measured using the Organizational Policies and Practices (OPP) questionnaire (Amick et al., 2000). Safety climate refers to the employee’s shared perceptions about workplace safety and the management’s leadership related to safety policies, processes, and practices (Zohar, 2008). Safety climate (seven items) and people-oriented culture (four items) were measured with a 5-point Likert-type scale (1 = strongly disagree to 5 = strongly agree). Safety climate and people-oriented culture scores were calculated as the average of the scale’s item scores, ranging from 1 to 5. Higher scores indicate more favorable perceptions about safety climate and people-oriented culture. The validity and reliability of the JCQ and the OPP questionnaire have been well-documented in previous studies (Bonneterre, Liaudy, Chatellier, Lang, & de Gaudemaris, 2008; Karasek et al., 1998; Tang, MacDermid, Amick, & Beaton, 2011).
For perceived risk of injury, this study used the following item: “How likely is it that you will experience a musculoskeletal injury within a year related to nursing work in general?” (Lee et al., 2013). Six response categories (1 = extremely unlikely to 6 = extremely likely) were used.
Data Analyses
Descriptive statistics were used to summarize the study variables. The 12-month prevalence of work-related MS symptoms was calculated for each four-body region and overall; the prevalence of work-related injuries was calculated for each type of injury and overall. Categorical variables of demographics, job characteristics, work-related perceptions, MS symptoms and injury were compared between U.S.-educated and foreign-educated nurses using Chi-square or Fisher’s exact tests. Continuous variables were compared using the student’s t or Mann–Whitney tests (for job strain variables, safety climate, and people-oriented culture). Logistic regression analyses were performed to examine the associations of immigration status with work-related MS symptoms and injuries. In multivariable models, the analysis controlled for demographic and job characteristics and work perception variables that were significant (p < .05) in the bivariate analyses, and odds ratios (OR) with 95% confidence intervals (CI) were calculated. We also examined the interaction effects of immigration status with safety climate and job demand and calculated the probabilities of experiencing work-related MS symptoms and injuries separately for U.S.-educated and foreign-educated nurses. The interaction term in nonlinear models (i.e., logistic regression) is the ratio of two ORs, which makes the interpretation challenging (Karaca-Mandic, Norton, & Dowd, 2012). Therefore, we calculated the predicted probabilities of experiencing work-related MS symptoms and injuries from the models with interactions using the Margins command in STATA. All statistical tests were two-sided using a significance level of p < .05, and were performed using STATA version 14.1 (StataCorp, College Station, Texas).
Results
Among 526 respondents (response rate: 26.3%), 107 nurses were not eligible for this study; 102 were retired or not currently employed, three were on disability leave, and two had missing data for immigration status. The study sample (n = 419) consisted of 339 U.S.-educated nurses (80.9%) and 80 foreign-educated nurses (19.1%). The majority of foreign-educated nurses were Asians (n = 51, 64%), most commonly from the Philippines (n = 32). Other countries of origin for foreign-educated nurses included England, Ireland, Belgium, Germany, Netherland, Canada, Mexico, Korea, Taiwan, China, Thailand, Nepal, and Uganda. Of the participants, the majority were female (90.5%), non-Hispanic White (62.5%), staff nurses (68.2%), and worked in hospital settings (70.4%). U.S.-educated nurses and foreign-educated nurses in the sample showed some significant differences: Foreign-educated nurses were more likely to have a bachelor’s degree or higher (81% vs. 63%), a lower BMI (mean 24.6 vs. 25.9 kg/m2) and longer job tenure in nursing (24.7 vs. 19.0 years), work in urban areas (67% vs. 47%), and worked longer hours per week (40.7 vs. 36.7 hr) than U.S.-educated nurses (Table 1).
Sample Characteristics of California Registered Nurses Stratified by the Country of Initial Nursing Education.
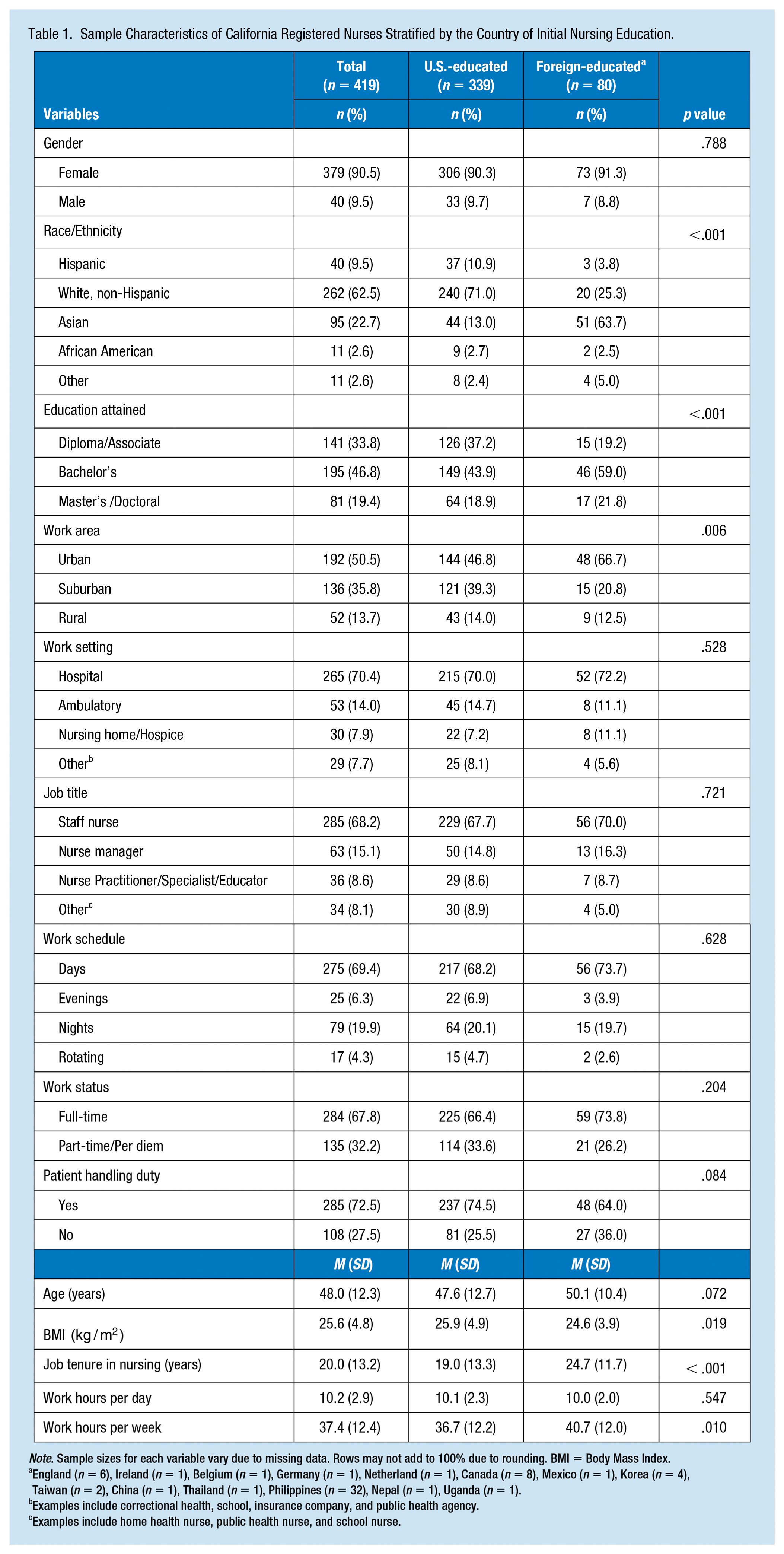
Note. Sample sizes for each variable vary due to missing data. Rows may not add to 100% due to rounding. BMI = Body Mass Index.
England (n = 6), Ireland (n = 1), Belgium (n = 1), Germany (n = 1), Netherland (n = 1), Canada (n = 8), Mexico (n = 1), Korea (n = 4), Taiwan (n = 2), China (n = 1), Thailand (n = 1), Philippines (n = 32), Nepal (n = 1), Uganda (n = 1).
Examples include correctional health, school, insurance company, and public health agency.
Examples include home health nurse, public health nurse, and school nurse.
Table 2 shows perceptions about work compared between U.S.-educated and foreign-educated nurses. Foreign-educated nurses perceived significantly lower job demand (p = .008) and job strain (p=.026) and higher safety climate (p = .017) than U.S.-educated nurses. The proportion of nurses who were very satisfied with their jobs was slightly lower among foreign-educated nurses than among U.S.-educated nurses (41.8% vs. 45.6%), and nurses who were very or somewhat likely to leave their job were more common among foreign-educated nurses than U.S.-educated nurses (37.5% vs. 31.0%); but neither difference was statistically significant. Those who perceived the highest level of MS injury risk (extremely likely) were slightly less among foreign-educated nurses than among U.S.-educated nurses (16.0% vs. 20.1%; p = .662).
Perceptions About Work of California Registered Nurses: Comparison Between U.S.-Educated Nurses and Foreign-Educated Nurses. a
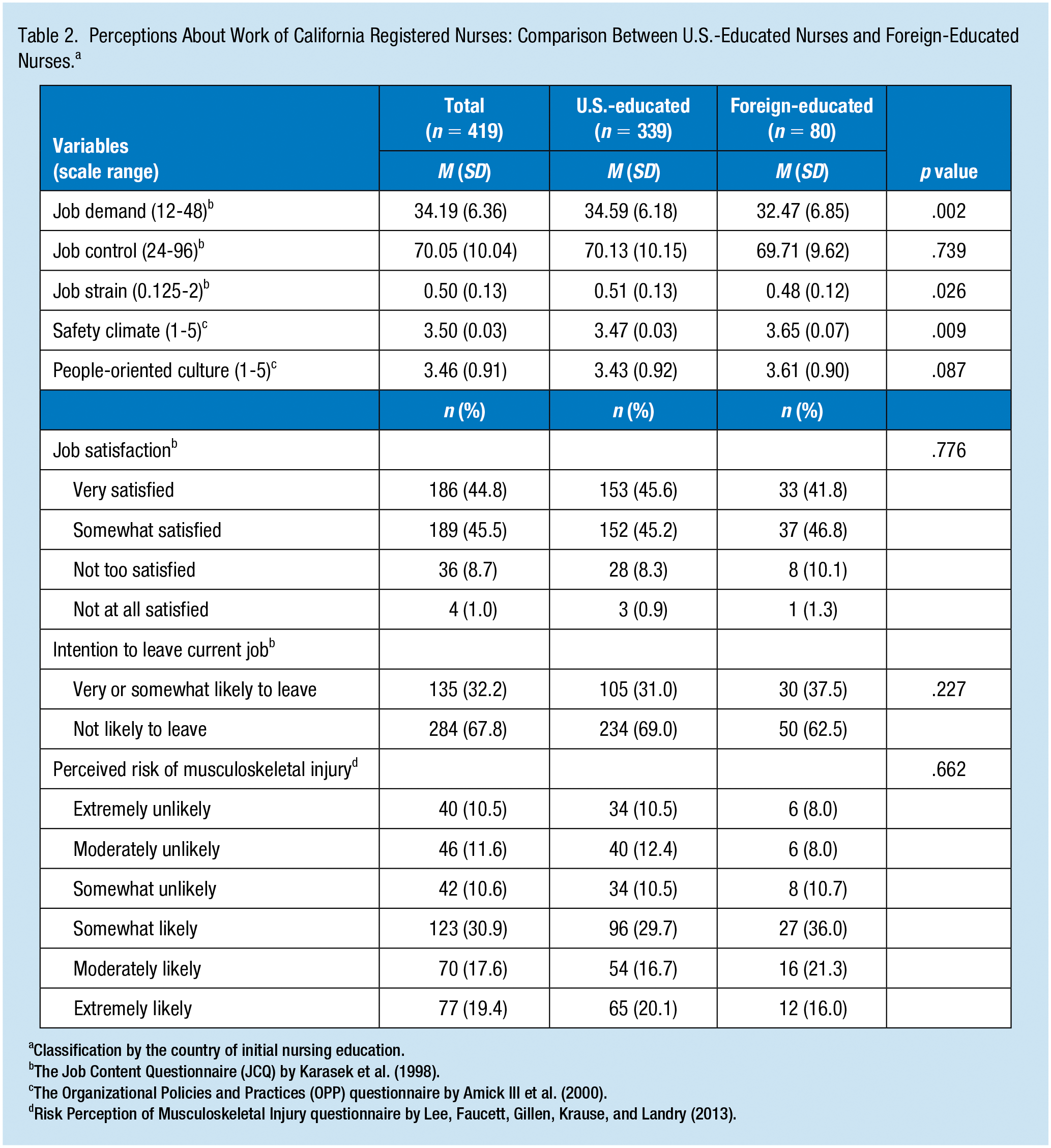
Classification by the country of initial nursing education.
The Organizational Policies and Practices (OPP) questionnaire by Amick III et al. (2000).
Table 3 presents the 12-month prevalence of work-related MS symptoms and the prevalence of work-related injuries for U.S.-educated and foreign-educated nurses. Overall, the prevalence of work-related MS symptoms was significantly lower in foreign-educated nurses than in U.S.-educated nurses (55.0% vs. 67.0%; p = .044); however, when evaluated by body region, none of the differences were significant. The prevalence of work-related injuries was not statistically different between U.S.-educated and foreign-educated nurses (24.8% vs. 21.3%; p = .507) and reporting of the injuries to supervisors was slightly more frequent among foreign-educated nurses than among U.S.-educated nurses (64.7% vs. 59.3%; p = .677).
Work-Related Musculoskeletal (MS) Symptom or Injury Experiences in the Past 12 Months Among California Registered Nurses: Comparison Between U.S.-Educated Nurses and Foreign-Educated Nurses.
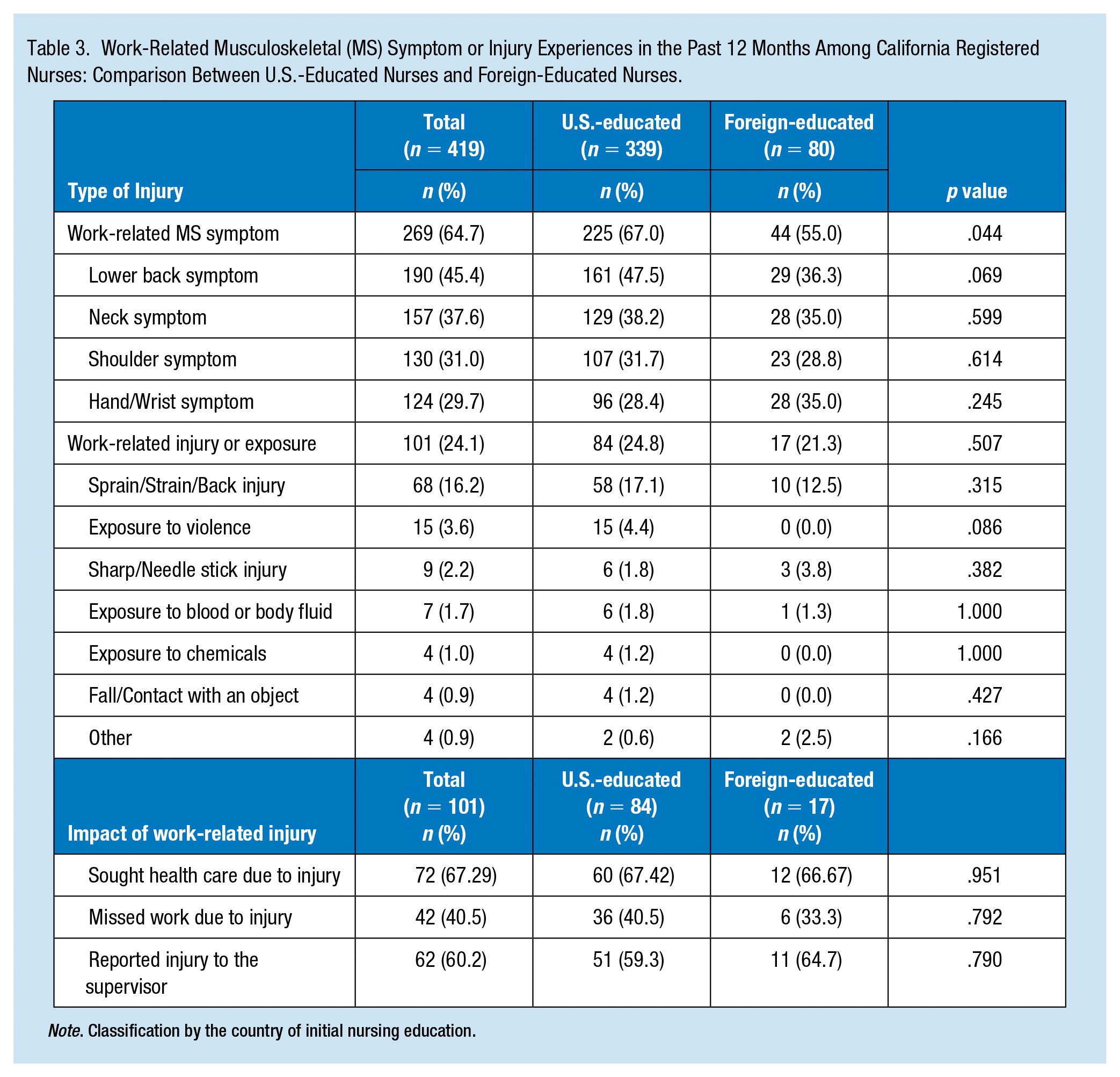
Note. Classification by the country of initial nursing education.
Factors Associated With Work-Related MS Symptoms and Injuries
Table 4 presents the results of multivariable models that examined the relationship between work-related MS symptoms or injuries and immigration status. Immigration status was significantly associated with work-related MS symptoms in the bivariate analysis (OR =0.60, 95% CI [0.37, 0.99]), but the statistical significance did not persist in the multivariable model (OR = 1.03, 95% CI [0.51. 2.09]). Instead, BMI, performing patient handling tasks, safety climate, and job demand were significant factors for work-related MS symptoms. A higher BMI was associated with an increased risk of experiencing work-related MS symptoms (OR = 1.06, 95% CI [1.00. 1.11]). The odds of experiencing work-related MS symptoms increased by approximately twofold among nurses who performed patient handling tasks (OR = 1.79, 95% CI [1.03. 3.11]). A stronger safety climate was associated with a decreased risk of experiencing work-related MS symptoms (OR = 0.49, 95% CI [0.31.0.76]). Conversely, higher job demand was associated with an increased risk of experiencing work-related MS symptoms (OR = 1.08, 95% CI [1.04. 1.13]).
Multivariable Logistic Regression Models: Factors Associated With Work-Related Musculoskeletal Symptoms and Injuries Among California Registered Nurse.
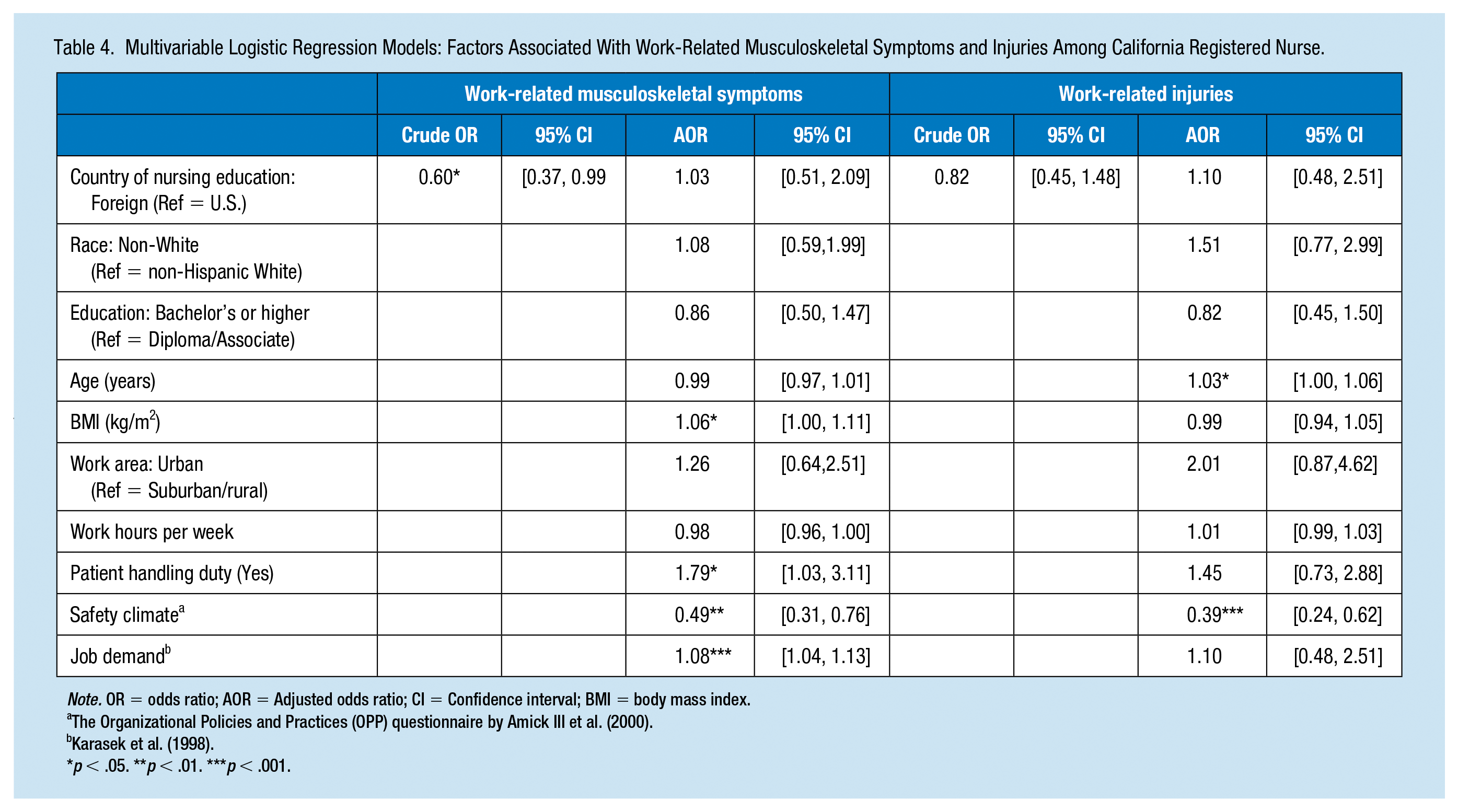
Note. OR = odds ratio; AOR = Adjusted odds ratio; CI = Confidence interval; BMI = body mass index.
The Organizational Policies and Practices (OPP) questionnaire by Amick III et al. (2000).
p < .05. **p < .01. ***p < .001.
The prevalence of work-related injury was not different by immigration status. Work-related injury among nurses was associated with safety climate, job demand, and age. Nurses who reported higher safety climate scores had lower risks of experiencing work-related injuries (OR = 0.39; 95% CI [0.24, 0.62]). In contrast, nurses who reported higher job demand were at increased risk of experiencing work-related injuries (OR = 1.10; 95% CI [1.05, 1.15]). In addition, older age was significantly associated with an increased risk of work-related injuries (OR = 1.03, 95% CI [1.00, 1.06]). The interaction effect between immigration status and safety climate on work-related injury was significant. Safety climate was associated with lower risk of work-related injuries for U.S.-educated nurses, but not for foreign-educated nurses (Figure 1).
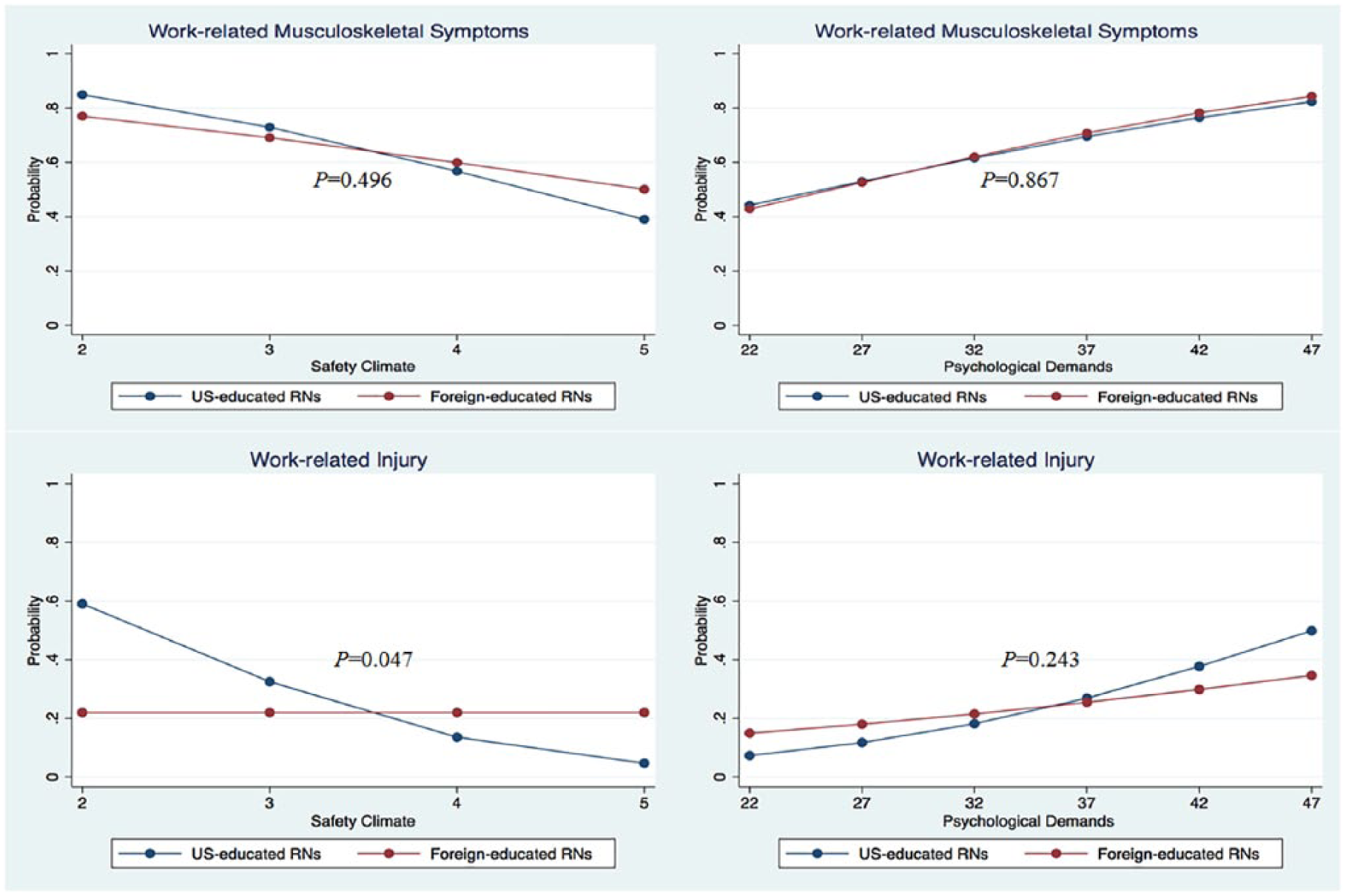
The relationship between work-related perceptions and musculoskeletal injury/symptoms between U.S.-educated and foreign-educated nurses.
Discussion
To explore the role of immigration in work perceptions and occupational health risks among nurses, we used a statewide random sample of California registered nurses and compared work perceptions and work-related MS symptoms and injuries between U.S.-and foreign-educated nurses. We did not find an independent association between immigration status and work-related MS symptoms and injuries, but there were significant differences in perceptions of workplace safety climate and job demand between U.S.- and foreign-educated nurses. Our findings were consistent with the findings of previous studies, demonstrating that a strong safety climate and low job demand are linked to decreased risks for work-related MS symptoms and injuries (Bailey, Dollard, McLinton, & Richards, 2015; Christensen & Knardahl, 2014; Clarke, Sloane, & Aiken, 2002; Lang, Ochsmann, Kraus, & Lang, 2012; Lee, You, Gillen, & Blanc, 2015; Mark et al., 2007). In addition, we found a significant interaction effect between immigration status and safety climate on work-related injuries, and the relationship between perceived safety climate and injury risk differed between U.S.-educated and foreign-educated nurses.
We found that immigrant nurses (i.e., foreign-educated nurses) were less likely to experience work-related MS symptoms or injuries than were U.S.-educated nurses, although the difference was significant in bivariate analysis only. As we noted earlier, the difference was no longer significant once work environment factors, such as safety climate and job demand, were taken into consideration. We also found no significant difference in injury reporting between U.S.-educated and immigrant nurses. Our findings extend prior research, indicating the dominant and crucial role of work environment factors for worker safety and health, which supersede individual worker-level risk factors. We found no significant relationship between immigration status and occupational health risks among nurses, in contrast with previous studies, which mainly focused on less skilled occupations and found immigrants had a higher risk of occupational injuries and reduced rates of injury reporting. Our finding indicates different industry characteristics may have different associations with occupational health risks.
In regard to perceptions of work, we found that immigrant nurses had more positive perceptions about their jobs, reporting higher safety climate and lower job demand than did U.S.-educated nurses. Many immigrant nurses in the U.S. migrate from less developed or lower-income countries (Health Resources and Services Administration, 2010). If immigrant nurses worked in such foreign countries with fewer resources dedicated to job responsibilities and workplace safety, they may perceive the working conditions and environments of the U.S. in a more positive manner. This positive perception derived from relative comparison may occur regardless of the actual work environment conditions, some of which may be far from optimal and perceived as poor by the respondents’ counterparts, U.S.-educated nurses. This explanation may be supported by our findings on interaction effects. We found an inverse relationship between safety climate and work-related injuries only among U.S.-educated nurses, and injury risk did not change based on the level of perceived safety climate among immigrant nurses. We also observed a similar pattern of stronger relationships, although not statistically significant, between safety climate and MS symptoms and between job demands and work-related injuries among U.S.-educated nurses. These findings suggest that positively biased perceptions about work environments among some immigrant workers may not accurately reflect the occupational health risks of the objective work environment. To the best of our knowledge, this is the first study to have quantitatively examined differences in U.S. nurses’ perceptions of safety climate and psychological job demand by immigration status. Further research is needed to validate these findings with a larger sample of immigrant nurses.
The results of this study should be interpreted with caution because of several limitations. First, this study used cross-sectional data; therefore, a causal relationship between study variables cannot be established. Second, this study used a population-based random sample, but possible nonresponse bias and self-selection bias related to the low response rate may have limited the internal validity and generalizability of the study’s findings. However, as long as the tendency for nonparticipation did not differ between U.S. and immigrant nurses, this nondifferential bias would lead the result toward the null. Our study used a small sample size, particularly for immigrant nurses, and may have had limited statistical power to detect differences between the two groups. Third, in defining immigrant nurses, we used the country of initial nursing education as a proxy for immigration status. Although country of initial nursing education is presumably a good proxy for the immigration status of nurses (Schumacher, 2011), this approach could have misclassified U.S.-born nurses who received nursing education elsewhere as immigrants. In addition, the length of stay in the U.S. or the level of acculturation among immigrant nurses may play a role in the relationships examined, but those data were not available in this study. Finally, for MS symptoms, our variables were limited to back, neck, shoulders, and upper extremities in this secondary data analysis study. Thus, our findings may not fully address nurses’ experiences of work-related MS symptoms across the whole body.
Implication for Occupational Health Nursing Practice
Our study findings contribute a few important insights to the current occupational health nursing practice. While the nursing workforce includes a significant number of immigrant nurses, previous research has not assessed the role of immigration status in work-related perceptions and occupational health risks. Our findings demonstrate that there are significant differences in perceptions about workplace safety climate and job demand between immigrant nurses and U.S.-educated nurses where these factors may play significant roles in experience of work-related MS symptoms and injuries. Our findings also suggest that those factors may be linked with occupational health risks more strongly for U.S.-educated nurses than for immigrant nurses. Future research is needed to explain the reason for the greater impact on U.S.-educated nurses and to further elucidate differences in work-related perceptions and injury risk among nurses by immigration status. In practice, these differences should be considered in planning and providing injury and illness prevention programs in the workplace to identify effective strategies. As the population of immigrant nurses increases and immigrants become a substantial part of the U.S. nursing workforce, the impact of immigration on their work experiences and occupational health risks needs to be better understood. Understanding the factors that can promote occupational health for immigrant nurses is crucial to maintaining a healthy nursing workforce that plays a pivotal role in caring for the health of the U.S. population.
Applying Research to Practice
Immigrant nurses (foreign-educated nurses) make up a considerable portion of the nursing workforce in the U.S. This study found that foreign-educated nurses had more positive perceptions about workplace safety climate and psychological job demands than U.S.-educated nurses, despite possible additional sociocultural challenges. Positive safety climate and lower job demands were linked to a decreased risk of work-related musculoskeletal symptoms and injuries, and this relationship was greater among U.S.-educated nurses than among foreign-educated nurses. Nursing leaders and health care organizations should note the differences in work perceptions between U.S.-educated and foreign-educated nurses to protect the health and safety of nursing employees.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funding for the Nurses’ Safety Study was supported by the Southern California NIOSH ERC Pilot Research Grant (2T42OH008412-08).
Ethical Approval
The Nurses’ Safety Study was approved by the Committee on Human Research at the University of California, San Francisco. This secondary data analysis, using data without personal identification, received an exemption of review.
Author Biographies
Kyung Mi Kim, MS, PhD candidate, RN, CNOR, is a doctoral student at University of California, San Francisco, School of Nursing, and has a keen interest in delivering high-value care: economically viable high-quality care for patients and better health for the population at a reduced cost. Her research focuses on the evaluation of health policy’s impact on the quality and cost of care and health care disparities. Her research interests also include health care workforce issues (e.g., the occupational health of the health care workforce and the utilization of nurse practitioners).
Soo-Jeong Lee, PhD, RN is an associate professor at University of California, San Francisco, School of Nursing, whose research focuses on the health effects of occupational exposure and the prevention of occupational injuries and illnesses. Her interests include musculoskeletal disorders in health care workers, health effects from chemical exposure (pesticides, cleaning products), organizational and occupational factors, safe work practices, occupational health surveillance, and evaluation of the impact of interventions at the individual, organizational, and regulatory level.