
Abstract
Background:
Nearly half of U.S. workers have access to workplace wellness programs (WWPs), 58% of workers with access participate. The aim of this study was to assess interest in WWP participation and identify reasons for lack of interest among workers with work-related permanent impairments—a population at elevated risk of adverse health outcomes.
Methods:
Workers who returned to work after a work-related permanent impairment were interviewed 11 to 15 months after workers’ compensation claim closure. Qualitative content analysis methods were used to code open-ended responses.
Findings:
Of 560 respondents, 51.4% expressed interest in WWP participation. Numerous adverse health and economic characteristics were associated with WWP interest, for example, interest was expressed by 63.3% of workers reporting fair/poor health status versus 47.1% reporting good/excellent; 56.9% of workers reporting moderate/severe pain versus 41.4% reporting mild/no pain; 64.7% of workers without health insurance versus 50.1% with health insurance; 69.0% of workers reporting depression versus 47.2% without depression; 70.4% of workers reporting obesity versus 48.0% without obesity; and 63.2% of workers often worried about expenses versus 46.9% reporting sometimes/never worried. Specific participation barriers were described by 34.2% of the 272 workers who were not interested.
Conclusions/Applications to Practice:
A majority of workers with work-related permanent impairments—particularly those with adverse health and economic characteristics—were interested in WWPs. Many workers who reported no interest cited participation barriers. Further research is needed to determine whether addressing such barriers would enhance equitable access. Those undertaking WWP planning, implementation, and outreach should ensure that WWPs are inclusive and serve workers with disabilities.
Background
Upon returning to work, workers with work-related permanent impairments, who account for roughly 10% of all injured workers, face elevated risks of further injury and work interruption related to unstable health, disability, and workplace factors (Sears, Fulton-Kehoe, & Hogg-Johnson, 2021; Sears, Schulman, et al., 2021a, 2021b). Nearly, half of U.S. workers have access to workplace wellness programs (WWPs), which hold potential to improve health and employment outcomes, yet only 58% of workers with access choose to participate (Tsai et al., 2019). WWPs can play a key role in the Total Worker HealthTM strategy that was launched by National Institute for Occupational Safety and Health in 2011 (Schill & Chosewood, 2013). The Total Worker HealthTM strategy advocates integration of workplace safety and workplace health promotion programs, as well as broader consideration of multiple factors that influence health and quality of life, to more comprehensively improve and support worker well-being (Chari et al., 2018; Schill & Chosewood, 2013).
Muir et al. (2019) suggest that workers who are healthier and more physically active are more likely to participate in WWPs. However, to enhance equitable access to WWPs, it is important to identify strategies to effectively engage all workers, including those with work-related permanent impairments and other disabilities. A small exploratory study of inclusive worksite wellness for workers with disabilities found that individual, social, and organizational factors all influence participation (Cook et al., 2016). Interest levels and barriers specific to workers with work-related permanent impairments are unknown. The aim of this study was to assess interest in WWP participation and identify reasons for lack of interest among injured workers with work-related permanent impairments. Understanding the factors associated with interest in and barriers to WWP participation can inform the design of inclusive, equitable, and accessible WWPs.
Methods
Study Design and Data Sources
The Washington State Department of Labor and Industries administers the workers’ compensation (WC) system, which includes (a) the State Fund, covering about 70% of workers, and (b) self-insured employers, covering the remainder. If, after completing treatment, injured workers are able to work but have suffered permanent impairment (i.e., permanent anatomic or functional abnormality or loss of function), their impairment may be rated for a permanent partial disability (PPD) award. Washington State workers with work-related permanent impairments were potentially eligible for this study if they had an accepted State Fund or self-insured WC claim that closed with a PPD award between January 1, 2018, and April 30, 2018. Workers were excluded if they had never worked after claim closure. Telephone interviews were conducted 11 to 15 months after claim closure, between February 6, 2019, and April 20, 2019. In total, 582 complete and 17 partial interviews were conducted, with a response rate of 53.8%, and negligible nonresponse bias. Further details regarding survey development, survey administration, detailed exclusion criteria with numbers of ineligible workers excluded for specific criteria, response rate calculation, and nonresponse bias assessment are available elsewhere (Sears, Schulman, et al., 2021b).
Workplace wellness program interest was assessed by asking: “Would you be interested in participating in workplace-based programs or activities aimed at maintaining or improving your health and function?” The subset of workers who were not interested were then asked the open-ended question, “Why is that?” Trained interviewers recorded workers’ narrative responses.
Administrative data included age, gender, WC coverage (State Fund vs. self-insured employer), and residence county, which was classified using the six-level 2013 National Center for Health Statistics Urban–Rural Classification Scheme for Counties (Ingram & Franco, 2014). All other covariates were obtained from the survey, and their collection and construction have been described in detail elsewhere (Edmonds et al., 2021; Sears, Edmonds, et al., 2021; Sears, Schulman, et al., 2021b, 2021c).
Data Analysis
We excluded 22 workers who did not answer the question about WWP interest (3.8% of 582 completed interviews). Bivariate associations between each covariate and WWP interest were tested using Pearson’s chi-square test (binary or categorical variables) or unequal variances t-test (ordinal scales or continuous variables), at a p < .05 significance level. All analyses were conducted using Stata/MP 15.1 for Windows (StataCorp LLC; College Station, TX).
Qualitative content analysis methods were used to code responses to the open-ended question regarding reasons for lack of interest. Following a content analysis approach (Hsieh & Shannon, 2005), and using Dedoose qualitative software (Dedoose Version 8.3.35, 2020), two coders (A.T.E. and J.M.S.) began the code development process by independently coding one-third of the responses. Codes were developed inductively, rather than by approaching these data with a priori frameworks. Each person’s response could be assigned more than one code. We then compared our code assignments and came to consensus on an initial coding scheme and codebook. The remaining responses were independently coded using this schema; discordant codes between coders were reviewed, and consensus on final codes was reached.
All survey participants gave informed consent. This study was approved by the University of Washington Human Subjects Division.
Results
Of the 560 included respondents, 51.4% expressed interest in WWP participation (n = 288), while 48.6% were not interested (n = 272). Of all respondents, 88.2% were working for pay when interviewed, 91.0% were born in the United States, and 62.3% were covered by the State Fund (vs. a self-insured employer) for the injury resulting in permanent impairment; none of these characteristics varied notably or significantly by WWP interest. Respondents’ mean age was 49.2 (SD: 11.7); workers who expressed interest in WWP participation were about 2 years younger on average than those not interested (mean difference: 2.1; 95% CI: [0.2, 4.1]; p = .032). Table 1 presents further descriptive characteristics for the overall sample, along with bivariate associations with WWP interest. Most of these characteristics did not significantly differ by WWP interest; however, workers in the lowest income categories (<40,000 USD) were significantly more likely to express interest in WWP participation (Table 1).
Associations Between Sociodemographic Characteristics and Interest in Workplace Wellness Program (N = 560)
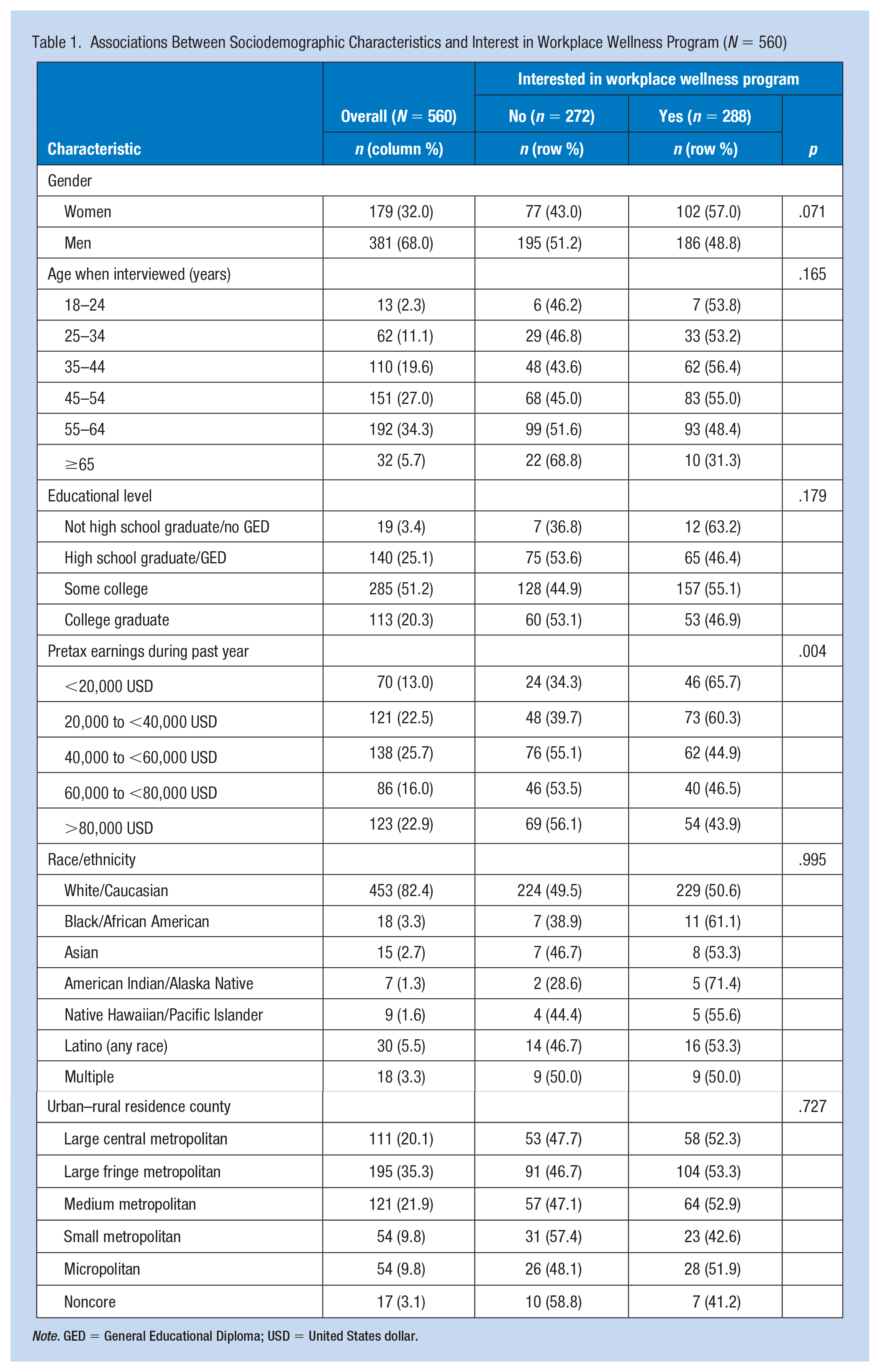
Note. GED = General Educational Diploma; USD = United States dollar.
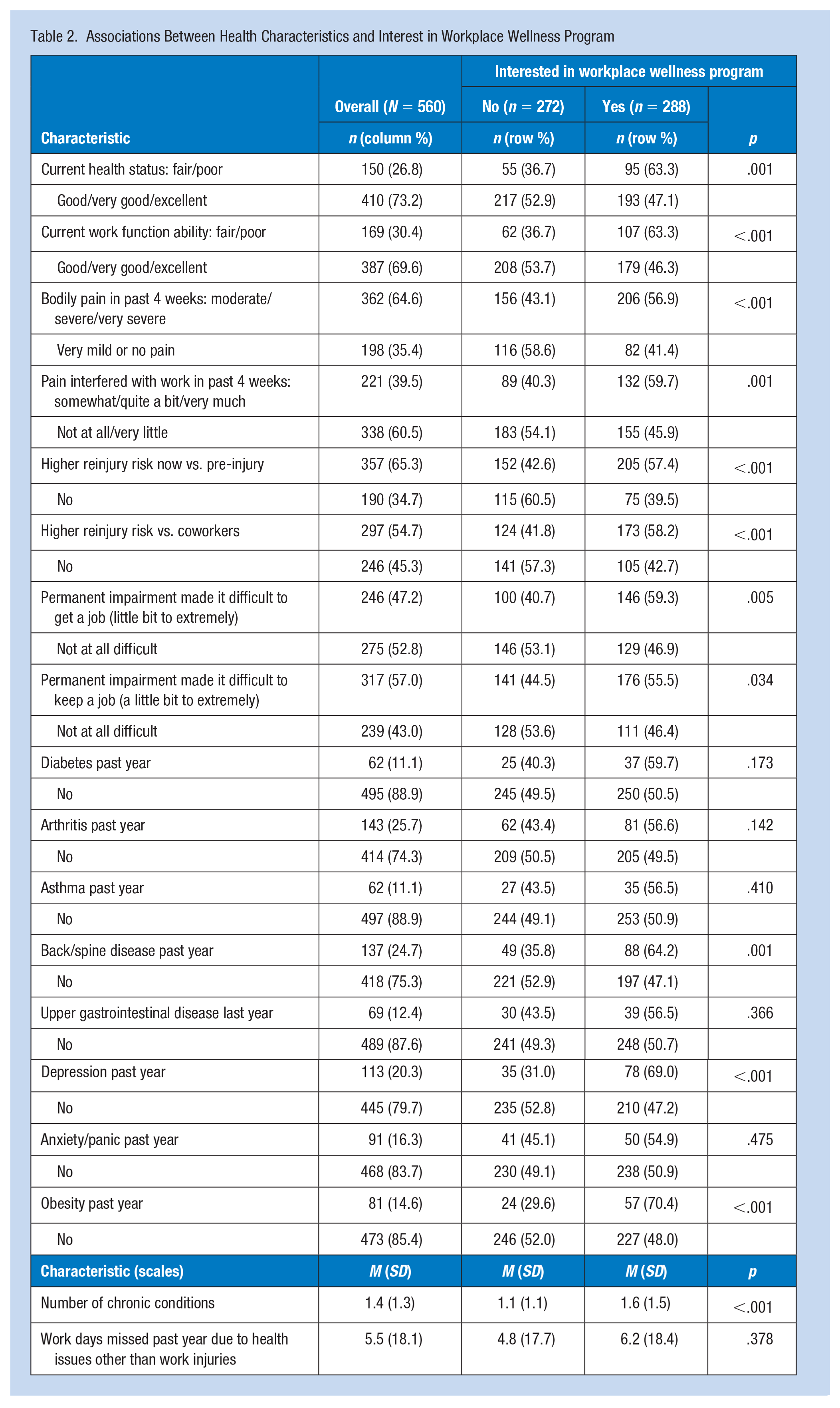
Respondents who reported poorer health status, poorer work functional status, more pain, more pain interference with work, higher perceived reinjury risk, and more difficulty getting or keeping a job due to their permanent impairment were substantially and significantly more likely to express interest in WWP participation (Table 2). Of the eight chronic conditions in the survey, three (back/spine disease, depression, obesity) were significantly associated with WWP interest. The direction of association was the same for all eight conditions, whether statistically significant or not. The number of chronic conditions ranged from zero to seven (M: 1.4; SD: 1.3); 31.3% reported none, 31.1% reported one, and 37.7% reported two or more. Workers with more chronic conditions were more likely to express interest in WWP participation (p < .001); however, number of work days missed due to health issues was not significantly associated with WWP interest (Table 2).
Associations Between Health Characteristics and Interest in Workplace Wellness Program
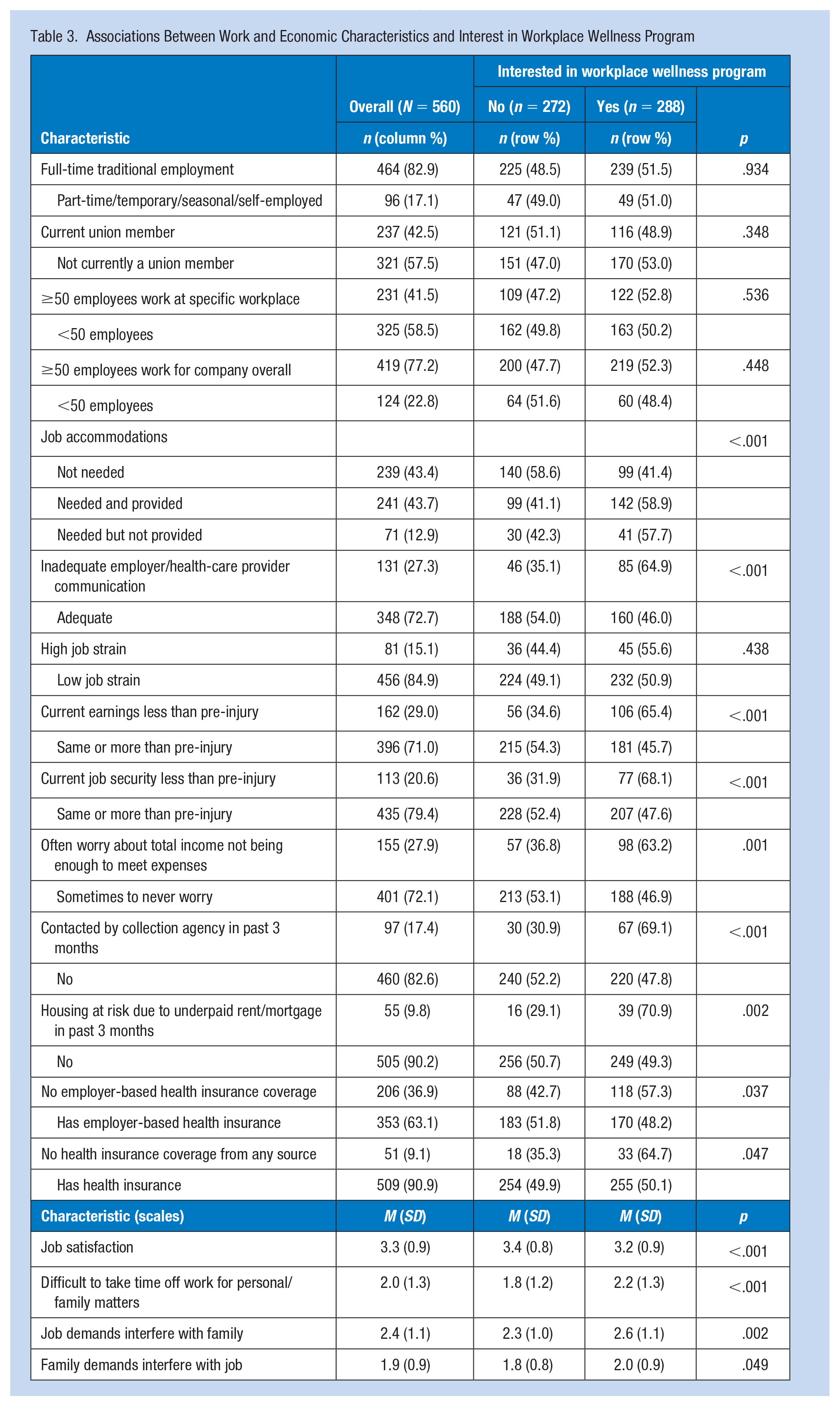
Employment type, union membership, employer size, and job strain were not significantly associated with WWP interest (Table 3). In contrast, workers reporting more economic stress consistently expressed more WWP interest, as did workers reporting lower earnings or less job security compared to pre-injury. Inadequate employer/health-care provider communication and lack of health insurance were also significantly associated with more WWP interest. Workers who needed job accommodations, regardless of whether they were provided, were significantly more likely to express interest in WWP participation compared to workers who did not need accommodations (Table 3). Workers reporting more work–family conflict consistently expressed more WWP interest. We also assessed several other workplace factors not included in Table 3 (i.e., social support, supervisor support, coworker support, organization-level and group-level safety climate), and found no noteworthy or statistically significant associations with interest in WWP participation.
Associations Between Work and Economic Characteristics and Interest in Workplace Wellness Program
Of the 272 workers who expressed no interest in WWP participation, 19.5% (n = 53) did not think they needed a WWP; 16.9% (n = 46) reported that they were already engaged in their own health or wellness activities; 4.0% (n = 11) did not think it would be helpful; and 8.8% (n = 24) did not think it would be relevant to their employment circumstances because they were retired, about to retire or leave their job, or were self-employed. Eight workers (2.9%) said they would need more information about WWPs. Specific participation barriers were described by 34.2% (n = 93). More than half of this subset described being too busy or having no time to participate, in general terms (n = 52), related to work demands (n = 8), or related to family demands (n = 8). Other convenience-related barriers included wanting to avoid extending the workday (n = 7), length or timing of commute (n = 3), night shift (n = 2), and general inconvenience (n = 1). Barriers with a more individual/personal focus included: (a) preferring solitary activities/privacy (n = 5), (b) health/injury status (n = 4), and (c) age (n = 1). Notably, few workers cited negative perceptions of their employer (n = 5) or negative perceptions of WWPs (n = 4). Finally, 16.9% (n = 46) did not provide any further information or gave vague/uncodable responses. (Note: Percentages summed to slightly over 100% because several responses were assigned more than one code.)
In a post hoc analysis motivated by the bivariate and qualitative findings above, we took a closer look at the subgroup whose stated reason for not being interested in WWP participation was that they were already engaged in their own health or wellness activities. The associations found between WWP interest and both lower income and lack of health insurance (Tables 1 and 3) suggested that one mechanism driving WWP interest might be lack of access to health/wellness activities outside the workplace. To assess this potential mechanism, we divided the sample into three groups: (a) no WWP interest, because already engaged in health/wellness activities; (b) no WWP interest, but gave other reasons (or no reason); and (c) WWP interest. Workers with no WWP interest due to engagement in health/wellness activities had: (a) higher incomes (36.4% of this group were in the >80,000 USD category, compared to 24.2% of those with no WWP interest for other reasons and 19.6% of those with WWP interest; p = .013) and (b) a higher prevalence of employer-based health insurance (76.1% compared to 65.8% and 59.0%, respectively; p = .048). Health insurance coverage from any source had the same pattern, although not statistically significant (95.7% compared to 92.9% and 88.5%, respectively; p = .116).
Discussion
A majority of respondents (51.4%) expressed interest in WWP participation. Expressing interest in WWP participation was significantly associated with having or being exposed to the more adverse condition for a number of health, work, and economic characteristics, including health status, work function, pain, pain interference with work, perceived reinjury risk, job security, work–family conflict, earnings, and economic stress. Workers expressing interest were less likely to have health insurance, yet were more likely to have certain chronic health conditions (i.e., back/spine disease, depression, obesity). Workers who needed job accommodations (vs. those who did not) were significantly more likely to express interest in WWP participation. These findings contrasted with previous research suggesting that healthier and more physically active employees were more likely to participate in WWPs (Muir et al., 2019). Reported interest may not necessarily result in actual participation (Ott-Holland et al., 2019), and our findings point to the need to assess and address participation barriers for this population to ensure equity and inclusion. For example, interest in WWP participation was associated with higher levels of work–family conflict, which in turn might affect ability to participate outside working hours.
Specific participation barriers were described by 34.2% of the workers who expressed no interest. These barriers most often related to issues that could potentially be addressed by offering WWPs during working hours and making workload adjustments. This echoes previous qualitative research among low-wage workers (Parrish et al., 2018). Notably, few workers cited negative perceptions of their employer or of WWPs as their rationale for lack of interest. Further, many workers expressing no interest gave reasons that might be amenable to educational and motivational strategies. For example, among those not interested (n = 272), 19.5% did not think they needed a WWP, 4.0% did not think a WWP would be helpful, and 2.9% needed more information.
Workers who reported lack of interest in WWP participation due to being engaged in their own fitness/wellness programs (vs. other reasons) had higher incomes and a higher prevalence of employer-based health insurance. These characteristics may facilitate access to wellness activities such as gym memberships, fitness classes, physical therapy, and personal trainers, thus potentially less need for employer-provided WWPs.
Strengths and Limitations
The open-ended approach enabled the description of WWP interest/participation barriers to emerge from the standpoint of the workers surveyed, rather than relying on a priori frameworks. Another strength was that the survey was focused on the first year after claim closure—a time period which is high risk for reinjury and job loss, and crucial for successful work reintegration (Sears, Fulton-Kehoe, & Hogg-Johnson, 2021; Sears, Schulman, et al., 2021a). Finally, this study involved a large population-based sample of workers with work-related permanent impairments, and the nonresponse assessment revealed no consequential bias. Our inclusion of workers with any type of permanent impairment enhances generalizability to a broad range of injuries and conditions. Limitations to generalizability include: (a) the survey being conducted only in English and (b) a high prevalence of union membership (42.2%), more than double the estimated 19.8% for Washington State in 2018 (Bureau of Labor Statistics), which may indicate relatively low job precarity among this sample (Edmonds et al., 2021). This was an exploratory study; more research is needed to replicate and extend these findings.
Conclusion
This study provides evidence that a majority of workers with work-related permanent impairments—particularly those at higher risk of adverse health outcomes and with fewer economic resources—are interested in participating in WWPs. Our findings point to the need to determine whether existing WWPs adequately serve this population, and whether adjustments are needed to support access and inclusion.
Implications for Occupational Health Practice
Implementation of a Total Worker HealthTM strategy at the workplace often includes a WWP as a key feature. Some studies have suggested that WWPs are primarily used by healthier workers. In this study, we identified that many workers with work-related impairments reported interest in WWPs, which was promising and worth further exploration. Workers with work-related permanent impairments, and disabled workers more generally, represent a substantial share of the workforce. In addition, some workers with work-related impairments reported barriers to participating in WWPs as the reason for their lack of interest. Efforts to address these barriers could ensure equitable access to WWPs by workers who may have the most to gain from these programs. Occupational health nurses and others undertaking WWP planning, implementation, and outreach should ensure that WWPs are inclusive and serve workers with disabilities.
Applying Research to Occupational Health Practice
Workers with work-related permanent impairments, and disabled workers more generally, represent a substantial share of the workforce. This study suggests that a majority of workers with work-related permanent impairments—particularly those at higher risk of adverse health outcomes and with fewer economic resources—are interested in participating in WWPs. In addition, some workers with work-related impairments reported barriers to participating in WWPs as the reason for their lack of interest. Efforts to address these barriers could ensure equitable access to WWPs by workers who may have the most to gain from these programs. Occupational health nurses and others undertaking WWP planning, implementation, and outreach should ensure that WWPs are inclusive and serve workers with disabilities.
Footnotes
Acknowledgements
We thank all survey participants for their time and input. We thank Research and Data Services personnel at the Washington State Department of Labor and Industries, specifically Lisann Rolle, program manager, and Sarah West, data analyst, for facilitating access to the necessary administrative data and providing extensive data documentation.
Author Contributions
J.M.S., A.T.E., and P.A.H. participated in the conception and design of the work, J.M.S. and D.F.-K. participated in acquisition of data, J.M.S. and A.T.E. conducted the analysis, and J.M.S. and B.A.S. drafted the work. All five authors participated in interpretation of data and revising the work critically for important intellectual content, and provided final approval of the version to be published.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Grant sponsor: National Institute for Occupational Safety and Health (NIOSH) (Grant numbers: R21OH011355 and T42OH008433). The findings and conclusions in this report are solely the responsibility of the authors and do not necessarily represent the official views of NIOSH.
Data Availability Statement
The data that support the findings of this study are not available for data sharing due to privacy and third-party restrictions.
Ethical Approval
All procedures followed were in accordance with the ethical standards of the institutional review board (University of Washington IRB Committee J; IRB00005647; FWA No: 00006878) and with the 1964 Helsinki declaration and its later amendments. All survey participants gave their informed consent prior to their inclusion in the study.