
Abstract
Background:
Spain hosts the fourth largest number of immigrants in Europe, resulting in a large proportion of migrant workers. To date, few studies have examined the working conditions of immigrants in Southern Spain who are known to be at risk for adverse working conditions. This study aimed to investigate the patterns of work and working conditions of immigrants living in southern Spain and to understand how these factors may affect their health.
Methods:
A qualitative study using semi-structured interviews was conducted throughout 2019 and included 93 immigrants. Transcription, literal reading, and theoretical categorization were performed and a narrative content analysis was carried out.
Results:
Three themes emerged on working conditions of this study population, including social and labor-related characteristics, working conditions, and occupational health issues. Four employment sectors were most commonly occupied by these immigrants, including caregiving and food service for women and agriculture and construction for men. Most immigrants were from Latin America, unemployed or working part-time jobs, and not hired under an employment contract. Most worked in low-qualified jobs, and were exposed to occupational hazards such as falls from heights, manual handling of materials, and psychological strain. The lack of training on occupational risk prevention and labor rights was related to a low identification of work situations having a negative impact on the health of immigrants.
Conclusions/Application to Practice:
These findings should be taken into account by the government and public health managers to provide better assistance to immigrant workers in Europe.
Keywords
Background
Since the global economic crisis in 2007, the economic insecurity and the lack of job opportunities have led to an increase in international migration to countries with higher income levels (Valero-Matas et al., 2014), resulting in countries from the European Union having received a large number of immigrants. Within this context, Spain hosts the fourth largest number of immigrants in Europe, representing 7% of its population (Eurostat Statistics Explained, 2019). The Spanish regions with the highest foreign population are Catalonia (20%), Madrid (16%), Andalusia (14%), and Valencia (14%; Economic and Social Council Spain, 2019).
In recent years, some changes have been noted concerning migration characteristics in Spain. The use of the Strait of Gibraltar is still one of the most important routes for “forced” migrations due to conflict situations (e.g., Syrian refugees; CEAR Spanish Refugee Assistance Commission, 2016). Conversely, middle- and high-income individuals, aiming to live in a country with better socioeconomic situations, are attracted by investment migration programs in Spain (Hombrados et al., 2019).
Immigrants tend to contribute positively to the labor force of Spain, with 80% in the active working age range (i.e., 16–65 years of age), and help mitigate the aging population and the low birthrate in Spain. Likewise, concerning the economic role of immigrants in Spain, it is important to note that only 0.6% of the Spanish Gross Domestic Product (GDP) is directed to foreign currency remittances; therefore, its negative impact on the Spanish economy is minimal (Economic and Social Council Spain, 2019).
Different studies have reported that the working conditions of immigrants are characterized by precariousness, low qualification, and more hours of work than the native population (Akhlaq, 2020; Arici et al., 2019; Moyce & Schenker, 2018). This is a result of a policy requiring immigrants to seek employment to obtain a residence permit (Agudelo-Suárez et al., 2009; Rosemberg et al., 2019). Immigrants usually are selected for the toughest and most difficult jobs for certain sectors such as agriculture, eating establishments, small businesses, construction and domestic services without proper economic compensation (García et al., 2009).
In addition to an insufficient salary (Agudelo-Suárez et al., 2009), immigrant populations are exposed to workplace hazards; experience higher rates of workplace injuries, illnesses, and fatalities; and are more prone to suffer from vacation deprivation (Agudelo-Suárez et al., 2009; Ministry of Labor Migration and Social Security, 2019). Despite these workplace challenges, previous research has reported high rates of job satisfaction among immigrant populations. These findings could be the result of an improved quality of life through employment, the main goal of migrating for most immigrant individuals (Rinken, 2005).
In the past 5 years, few studies have investigated the association between working conditions and occupational health (Agudelo-Suárez et al., 2019; Arici et al., 2019; Benazizi et al., 2018; Cayuela et al., 2018; Conway et al., 2016) and even fewer studies have addressed this literature gap with qualitative methods (Ronda-Pérez et al., 2016; Zapata-Villa et al., 2018). To our knowledge, this is the first study among a Spanish immigrant working population that also examines occupational health and safety (OHS) training, as it is a factor that influences the perception of occupational risks and better health care for workers. Aiming to bridge this gap, the objective of this study was to employ qualitative methods to investigate the association of work patterns and work conditions with the health of the immigrant population living in southern Spain.
Methods
A qualitative, exploratory, and descriptive design was employed and data were analyzed using a phenomenological approach. This approach seeks to describe and understand experiences (i.e., the study phenomenon) from each participant based on the analysis of specific discourses and themes, aiming to build a collective perspective (Hernández-Sampieri et al., 2010). Data collection consisted of semi-structured interviews with immigrants living in southern Spain in 2019. This research followed the criteria of the Consolidated Criteria for Reporting Qualitative Studies–COREQ (Tong et al., 2007).
Setting and Sample
The study was conducted in Andalusia, the southernmost region of Spain and Europe, where, according to the Spanish National Institute Statistics (2019), there are 8,427,000 inhabitants and 653,146 immigrants.
Participants were recruited through contacts with five nongovernmental organizations (NGOs) from five Andalusian cities (Seville, Cádiz, Málaga, Huelva, and Córdoba). These NGOs offer social and labor support to immigrants of different nationalities, such as orientation to employability, the advice in getting the appropriate documentation, English as a Second Language course, and OHS training. However, training in the care sector is the course most attended by the immigrant population, ensuring better job interviews in the future.
Eligibility criteria for participants included adults who were at least 18 years of age, migrated to Spain, able to communicate in fluent Spanish or English, received or participated in any of the NGO services, and were trained in OHS.
Sampling was intentional, and the number of informants was completed when the interviews did not provide any new information. A series of sociodemographic variables were ascertained (gender, age, job, country of origin, and years living in Spain) to ensure heterogeneity of profiles and perspectives. The intention was to increase the relevance of our findings within the Andalusia areas and their generalizability to other Spanish areas. Based on these inclusion criteria, our study sample included 93 participants.
Data Collection
The interviews were carried out face-to-face by two qualified researchers inside the NGOs (n = 80) or by phone (n = 13) in 2019. Interviews lasted approximately 50 minutes and were audiotaped and transcribed sverbatim. Data collection continued until data saturation was reached as previously mentioned.
Participants were recruited in the NGOs where they received job guidance and were interviewed after they had completed 20 hours of OHS training. At the beginning of the training, they were informed of the objectives of the study and were invited to participate voluntarily. The interviews were carried out at the end of the training in the NGO facilities or other locations, according to the participants’ preferences or by telephone. Those who agreed to participate signed a consent form or gave verbal consent when the interview was carried out by phone. The study was approved by the Andalusian Research Ethics Committee in Spain. All participants received written and oral information about the study, including the right to withdraw and the guarantee of confidentiality.
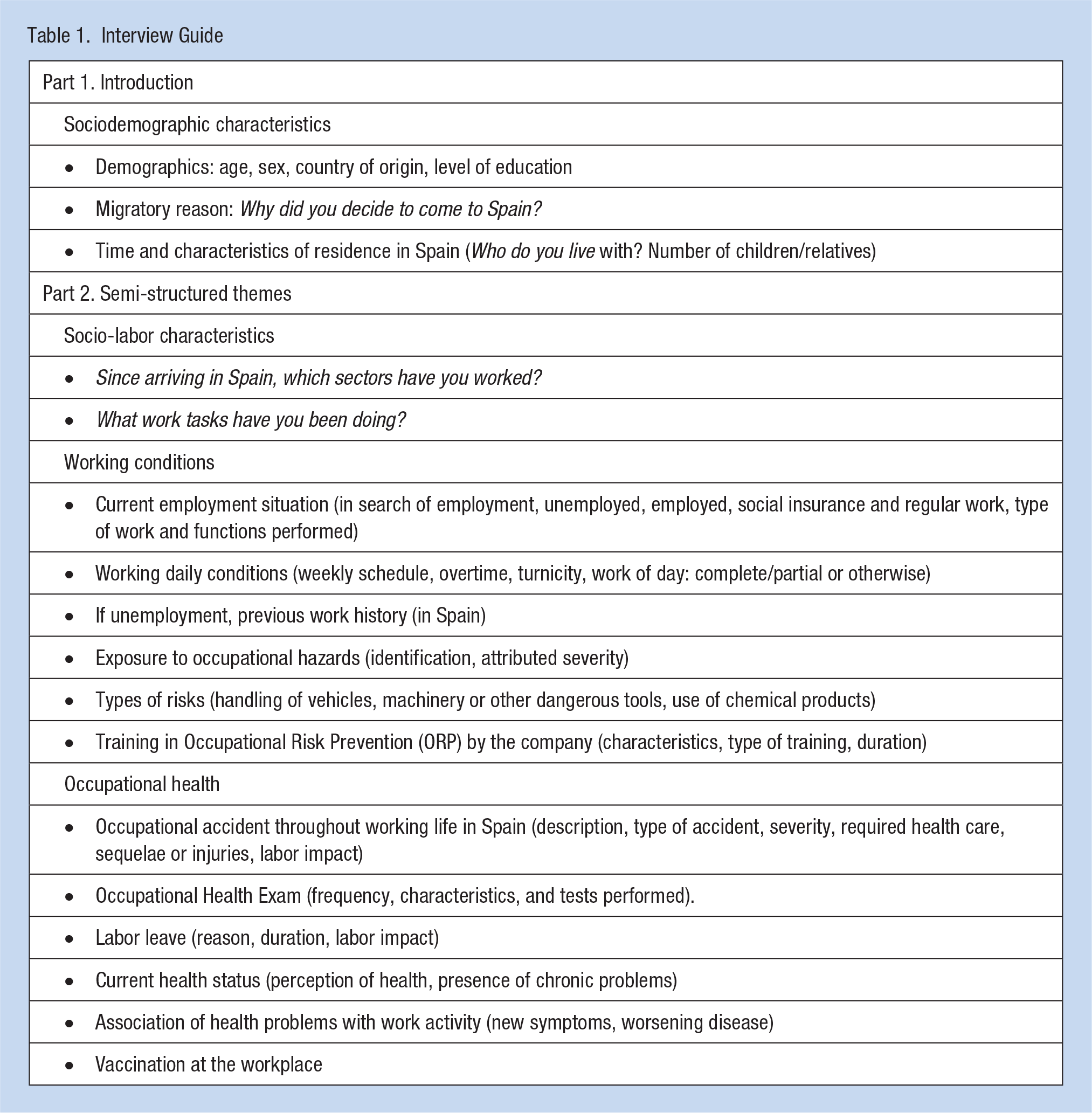
The interview script was based on the project called “Immigration, Work and Health,” a nation-wide study collecting information on the working conditions of immigrant workers and their relationship with health. A group of experts in occupational health (n = 9), migrations (n = 6), and two NGO users carried out an analysis of the content of this script to assess its adequacy. Finally, the script was improved and expanded, incorporating issues such as driving or handling of dangerous vehicles, machines or tools, use of chemical products, health care received due to work activity, and occupational vaccination status.
The interview script was made up of two parts, including questions about sociodemographic characteristics and details about workers’ labor characteristics. Details for the interview script are outlined in Table 1. In brief, workers were asked about work characteristics, daily work conditions and schedules, types of occupational hazards, occupational training, occupational health events and issues (injury and/or illness), and need for work leave.
Interview Guide
Data Analysis
Data were captured through audio recording. Transcription, literal reading, and thematic categorization were performed. Data analyses started with individual repeated readings to get an overview of respondents’ experiences. The research staff read all field notes and interview transcriptions several times to gain an overall understanding of the content. The analysis continued by organizing descriptive labels, focusing on emerging or persistent concepts and similarities/differences in participant’s behaviors and statements. The coded data from each participant were examined and compared with the data from all the other participants to develop categories of meanings.
A narrative analysis of the transcript content was carried out, following methods proposed by Taylor and Bogdan (1998). To ensure the quality of the data, triangulation with the research staff and informants was conducted. The data were analyzed using NVivo software (NVivo version 12; 2018; QSR International, Doncaster, Australia). A final report was prepared with the statements of each immigrant in the following way: “I, number, sex, age.” Descriptive analysis of the background information was carried out using numbers and percentages, as well as means and standard deviations.
Results
The study sample included 93 participants (77.4% females and 22.6% males), with a mean age of 41.3 (SD = 10.3) years and 37.6% had at least high school education. Participants were from Seville (32%), Malaga (23%), Cádiz (19.5%), Huelva (14%), and Córdoba (11.5%). The NGOs included a wide number of nationalities with most immigrants from Latin America (25.8% from Nicaragua, 10.7% from Peru, 10.7% from Colombia, and 10.7% from Bolivia) and their average length of stay in Spain was 5.5 years (Table 2). A total of 73.1% of participants did not have a job during the interview.
Spanish Immigrant Characteristics (N = 93)

The lack of job opportunities in the country of origin was pointed out as the most common reason for migration, followed by political asylum. In general, migrations were based on individual reasons and had a strong desire to return to the home country. However, this desire remained in the background, as one of the main objectives to be fulfilled by immigrant workers is sending remittances to relatives outside Spain. Three main themes emerged from the discussions, namely, socio-labor characteristics, working conditions, and occupational health.
Social and Labor–Related Characteristics
Four employment sectors were the most commonly occupied by study participants and differed by gender, including informal/formal caregivers and food and beverage establishments (for females) and agriculture and construction (for males).
Females reported an overload of functions during their work, usually assigning tasks not specifically outlined in their job description and exceeding working hours. For example, “although I was hired to accompany an older person, I could rarely be with her because I also had to cook for the whole family and clean the house” (I42 female, 45 years). It was common for women to carry out housework and care for both children and the elderly, some of them with chronic diseases, as described by one participant, “Caregiving for diabetes patients . . . also dependent with Alzheimer, dementia, cerebrovascular accident . . . besides cleaning the house, cooking, ironing, shopping, accompanying the doctor, going to the pharmacy . . .” (I62 female, 50 years).
In most of the cases, a clear difference was noted between the job qualifications in Spain (i.e., lower qualification) as compared with their country of origin (i.e., higher qualification). A female said, “I have worked as a waitress and saleswoman in Nicaragua, but here in Spain, I was working only picking oranges, and they call me to work from time to time, whenever they want” (I2 female, 37 years). Another Colombian participant has switched from working in a bank offering loans, to occupying a waiter position in a bar in Spain (I22 male, 32 years).
The participants reported that this lower job qualification was justified by the bureaucracy and the challenges needed to validate academic degrees. However, the need to send remittances to the country of origin and the desire to quickly occupy a job that allows economic maintenance were also important reasons for this low qualification. As a participant refers, “I have some validated documents, but they are not enough. Some of them have to be sent by our universities, so we are caught between the slow bureaucracy of our country and the demands of the Spanish law” (I14 male, 28 years old).
Working Conditions
Although almost three quarters of the immigrants interviewed were currently unemployed (72.37%), most of them had worked in Spain in the past. Nevertheless, among those employed, most were recruited for part-time or seasonal jobs. It was also frequent to find people who work without a work permit (e.g., picking olives in the field, I66 male, 23 years), and situations in which the employer failed to formalize the situation of the employee, such as not paying governmental social security taxes: “In my previous job, I have worked 25 months giving care to a dependent person without contributing to social security” (I27 female, 42 years): I have worked in an air conditioning installation company from 2005 to 2007, and he [the boss] told me he would hire me but he didn’t. Since he didn’t pay me for a week, I quit my job and I’m currently looking for a regulated job (i.e. to be hired under an employment contract). (I4 male, 51 years)
Other common complaints related to the working conditions, including the duration of the working day, which usually surpassed 8 hours. Some respondents reported a 12-hour workday (I69 male, 42 years; I70 female, 48 years) or even living with the person they care for, working as internal staff: “My workday is [never] complete as an internal worker, there is no rest. I have to take care of her [dependent person] day and night” (I11 female, 40 years). They also mention having no expectation of ongoing work or guaranteed hours of work per week, which does not allow for having a fixed salary.
Participants indicated exposure to health hazards at work, such as falls from heights, patient handling and lifting, manual handling of loads, and psychosocial strain. A female participant said, I worked 25 months without a contract and was exposed too many risks because I took care of a woman over 150 kg. I lifted her daily from the bed and it was terrible for my back. They demanded a lot of me and that was also a constant stress. (I27 female, 42 years)
Another said, “Some Alzheimer’s patients have hit me, there is that risk of being attacked. I have also been infected with the flu” (I6 male, 49 years). Participants verbalized that they have not had been received training: “They never train you, they have never done it with anyone I know” (I91 female, 49 years); “I was never trained in safety or occupational risk prevention” (I11 male, 44 years); “The company was never interested in offering me training” (I14 male, 28 years). Nevertheless, they pointed out that the identification of labor risks has been possible, thanks to the OHS training received: “After the course, I knew what a work accident was and that if we suffered one, we could take a day off . . . but then, we had to continue working” (I14 male, 28 years).
Immigrants associated these risks with their working conditions, lack of personal protective equipment (PPE), poor training, and incomplete information: “I have worked under stress, for many extra hours without receiving additional payment, with lack of good treatment of the employers towards their workers, and several physical risks due to lack of adequate PPE and unmanaged machine handling” (I22 male, 37 years); “When caring for elderly people, I shower them without gloves and doing all the tasks without rest” (I4 female, 45 years).
The riskiest devices used on the job that were reported by participants were the crane or wheelchair (for user mobilization), the automotive, and agricultural vehicles. A female worker said, I talked to the son of the woman I was caring for, because I always had to get the woman in a wheelchair down the stairs. That was very difficult for me and dangerous for her. Finally, I got the family to install a ramp. (I19 female, 41 years)
Chemical products were also mentioned, such as those used for cleaning or handling medication for dependent persons: “I was exposed to chemical liquids while cleaning without a mask, gloves and safety clothing” (I78 male, 49 years).
Occupational Health
Overall, participants perceived their health status worsening due to exposure to occupational risk factors. Several health problems were identified: “My health is worse and I feel very tired, since I have to bend over constantly to clean and my feet and back hurt” (I12 female, 34 years). Back pain (i.e., joint and muscle) is considered the most common problem related to their working conditions, followed by stress, anxiety, and respiratory symptoms: “My asthma is worse. The doctor said that it had been caused by the store where I worked, since there was a lot of dust there” (I4 male, 51 years). However, the few job opportunities and the irregular job contracts affect the mental health of immigrants, causing sleep and mental health disorders.
Occupational medical evaluations were reported as not being frequently performed, although they considered it necessary: “I never did a health assessment during 8 years while working there. In my opinion, inspectors should go to all companies and investigate it” (I4 male, 51 years). Only five immigrants reported having been subjected to this type of health procedure. General blood and urine analysis were the most cited (I2 female, 43 years; I13 female, 44 years), followed by vision and hearing tests and weight and height measurements (I43 female, 32 years). Occupational vaccinations were also not very common and usually limited to tetanus and flu vaccines, whereas Hepatitis A and B vaccinations in the health care workers were not provided (e.g., informal caregivers).
The most common work accidents were falls at the same or different levels, cuts and wounds, and those related to musculoskeletal disorders: “I only suffered some burns or cuts, but without seriousness. I also had difficulty breathing once, when washing and ironing, since the chemical affected my lungs when inhaled” (I79 male, 30 years). However, most respondents stated that they had not suffered work accidents or had not reported them because they were minor. According to the immigrants, workplace incidents are often poorly documented because they do not consider it an accident and because of fear related to their immigrant status (Hernandez Quevedo & Jimenez Rubio, 2009; Porthe et al., 2010; Sole & Rodriguez, 2010). This is why researchers observed that absenteeism caused by leave due to accidents was almost nonexistent and immigrants justified it by the concerns of losing their job, as mentioned by a participant: “I was 6 days off work [due to leave], I didn’t want to spend more time because I was afraid of losing my job and finally, I was fired” (I53 female, 50 years).
Furthermore, participants felt the duty to continue working under any circumstance to avoid being expelled from the country and to support their family: “I fell and had a bruise on my foot and inflammation for 20 days but I did not go to any doctor. I had to keep working, my children need it” (I70 female, 48 years). Another worker indicated, I lost total strength in my body, I couldn’t stand up and I had a lot of pain in the calves . . . I was working as a caregiver when this happened, and I kept working every day until the person died. I think if I don’t work the police can expel me from the country. (I14 female, 43 years)
Discussion
This study explored the occupational health and the working conditions of immigrants living in Spain. We found that most immigrants were from Latin America, were unemployed or had part-time jobs, worked in low-skill jobs, were not hired under an employment contract, and were exposed to several occupational risk factors.
The first remarkable finding of this study was the fact that most immigrants were from Latin American countries, although the African continent is closer to Spain. This may be justified by the fact that the Spanish language is the most common spoken language in Latin American countries. In our study, among all Latin American countries, the highest number of immigrants interviewed was from Nicaragua (25.8%), which may reflect the political crisis faced by this Central American country and has resulted in the emigration of 10.56% of its population in the last decade (53.74% are females). These findings make Spain the third country of destination for these immigrants and the first one in the European continent (Eurostat Statistics Explained, 2019).
It is also noteworthy that although 50% of immigrants had a higher education degree (Agudelo-Suárez et al., 2009), most of them occupy less qualified jobs (i.e., agriculture, domestic, and construction sectors). These jobs are very different from the jobs they were assigned in their country of origin (Rinken, 2005), and although immigrant education is appreciated by their employers, this does not seem to provide the expected job opportunity (Cuban, 2018).
In fact, immigrants’ job opportunities in Spain are usually accompanied by factors that may impact their quality of life and working conditions such as working in irregular and illegal situations, occupying jobs in small businesses where supervision and protection of occupational risks are limited (Mucci et al., 2019), have been living in the host country for a short time (Ronda-Pérez et al., 2019), and extensive working days and temporary or part-time jobs (Simkhada et al., 2018). The rates of unemployment, the lack of access to health services, the lack of social support, ethno-cultural and language differences, ignorance of labor rights and security measures, and family economic dependence (Ronda-Pérez et al., 2014; van Tubergen, 2011; Yanar et al., 2018) are some of the factors that motivate these immigrants to accept these jobs and poor labor conditions.
These problems mentioned above become even more important over time, when the immigrant population, previously healthy, started to increase the morbidity and mortality rates as compared with the native population (Mehmood et al., 2018; Pocock et al., 2016; Ronda-Pérez et al., 2014). Concerning OHS, the rates of trauma in construction sector, respiratory and dermatological diseases in the agricultural sector, or those derived from lack of hygiene and exposure to high temperatures in the eating establishments are frequent (Mucci et al., 2019). The long working hours seem to intensify these risks (Ronda-Pérez et al., 2014), increasing disease vulnerability (Ahonen et al., 2007; Moyce & Schenker, 2018). Besides, mental health is also affected by occupational exposures and poor conditions. Previous studies described cases of burnout, depression, and personality changes in immigrant population related to their working conditions (Bener, 2017; Dodd et al., 2017; Simkhada et al., 2018). Other studies also reported these differences due to a lower knowledge of labor rights by the immigrant population (Yanar et al., 2018), inexperience in the labor sector (Pocock et al., 2016), a greater workload, and the lack of health and safety training (Gálvez Herrer et al., 2011).
The caregiving job is commonly associated with extensive working days and performing tasks that exceed job requirements. This is mostly experienced by females, who receive lower salaries in comparison with other occupational groups (Dodd et al., 2017) and are more subjected to abuse (Simkhada et al., 2018) and injuries derived from occupational incidents (Ronda-Pérez et al., 2014). An example is the higher prevalence of gynecological problems in females working in the domestic service due to the manipulation of toxic cleaning products (Moyce & Schenker, 2018).
In this delicate labor context, health surveillance is considered a great resource to identify diseases related to these poor working conditions. However, periodic occupational health assessments are seldom performed and this is closely related to the situation of irregularity, economic problems, and difficulties in accessing health services (Badanta et al., 2020; Bener, 2017; Moyce & Schenker, 2018; Sterud et al., 2018). Likewise, few occupational incidents are reported and employees usually have low rates of absenteeism due to fear of being fired from work or suffering a decrease in salary (Mehmood et al., 2018). All these underreporting incidents may hinder a better analysis on how working conditions may affect the health of immigrant populations. However, it is necessary to deepen these aspects because adverse working conditions motivate the search for another job with better conditions, but do not discourage them from stopping work and return to the country of origin (Dodd et al., 2017). These findings should be taken into account by the government and public health managers to provide a better assistance to these immigrants in Europe.
This study has some limitations that should be considered. First, a convenience sample was used and generalizability to the immigrant community in Andalusia or Spain should be taken with caution. Nevertheless, our results are consistent with the official data and other studies (Agudelo-Suárez et al., 2009; Arici et al., 2019; Cayuela et al., 2018; García et al., 2009). Second, this study examined the working conditions and their relationship with health in an immigrant population, which received OHS training. Thus, it is expected that this specific sample was better able to identify poor job conditions and occupational safety and health risks than the general immigrant population, limiting the generalizability of our findings. Third, participants were recruited from NGOs, implying a selection bias. Finally, a large proportion of immigrants were unemployed, and because the objective of the present study was to learn about working conditions, the study population may have different experiences than those employed.
Further studies should include immigrants not related to NGOs. The prevalence obtained in our study was limited to this specific group of immigrants and may not be the same while investigating the general population of immigrants. Nevertheless, our study has strengths that should be considered. Although the OHS of immigrants are very important, this topic is often overlooked in countries outside the United States. Likewise, the qualitative nature of the study helps to further understand the opinions of immigrants through their own perceptions, adding to the quantitative studies already published in this field.
Implications for Occupational Health Practice
Our results reveled that excessive working hours, poor occupational environment, and the lack of labor rights are potential problems that should be addressed in the immigrant population in Spain. Furthermore, there is also a lack of OHS training in these individuals. Occupational health professionals and managers should provide OHS training to immigrants as it can improve the identification of occupational risks and health problems they are exposed to, resulting in lower costs to the government and minimizing the overload of the health care system in the future.
This training should take into account the specific characteristics of the labor sector involved, but it should also consider the peculiarities, the vulnerability, and the cultural background of the immigrant population. Therefore, our findings support that the government should encourage the participation of immigrants in OHS training and, to achieve this goal, should make this information more available to the community using different media platforms.
Conclusion
Our results indicate that the immigrant population working in Andalusia, Spain, has low qualified jobs and precarious conditions, which is associated with the lack of stability and excessive working hours. The lack of training on OHS and lack of labor rights are related to a low identification of work risks that seem to have a negative impact on the health of immigrants. These findings highlight the importance of deepening the aspects related to the occupational health of immigrant workers.
Applying Research to Occupational Health Practice
Acute and long-term health problems can result from the exposure to certain occupational risk factors. Given that the job security is a global concern, it is necessary to understand the working conditions of immigrant Spanish workers to promote a safer and healthier work environment. The current study found that the immigrant population worked in low-skilled labor sectors with precarious temporary conditions, irregular work schedules, and excessive working hours. Although participants reported a lack of knowledge and the problems with labor rights, their training in OHS was related to a better identification of occupational risk factors, which could have a positive impact on the health of immigrants. These findings highlight the importance of deepening aspects related to the occupational health of immigrant workers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Rocío de Diego-Cordero (PhD) is Assistant Professor at the School of Nursing, Physiotherapy and Podiatry at University of Seville.Occupational Health Nursing. (Ministry of health, consumption and social welfare ,2005).Master in Occupational Risks Prevention (Expert in Ergonomics and Psychosociology, 2006).Degree of Anthropology (University of Seville, 2009). Member of Research Group CTS 969 “Innovation in HealthCare and Social Determinants of Health”.Member of International Commission on Occupational Health (ICOH).Member board of “Scientific Association Spanish Association of Specialists in Occupational Nursing”.
Manuel Romero-Saldaña, assistant professor, Department of Nursing, Phamacology and Physiotherapy, University of Cordoba. Registered Nurse since 1993. Master’s degrees in Safety and Occupational Health (2001), Master’s degrees in Research Methodology in Health Sciences (2012) and Dotoral degree in Biomedicine (2016). Specialty in Occupational health Nurse since 1998. Editor-in-Chief of European Journal of Occupational Health Nursing (FOHNEU) since 2020. Member of AET (Asociación Española de Enfermería del Trabajo) since 2001. Research group of Instituto Maimónides de Investigación Biomédica de Córdoba: “GA-16 “Estilos de vida, innovación y salud”. Ana Jigato-Calero, resident nurse of Community Health Nursing at the Health District of Cadiz, Spain. Registered Nurse since 2019.
Bárbara Badanta (PhD), professor in nursing at the University of Seville, Spain. Registered Nurse since 2008. Master’s degrees in Nursing research and Teaching, and a doctoral degree in Nursing. Member of Research group PAIDI-CTS 1050 “Atención compleja, cronicidad y resultados en salud”. Expert in Transcultural Nursing and Development Cooperation. Member of Board Directors of “Desarrollo Comunitario Internacional”. Member of “Centro de Estudio de las Migraciones y las Relaciones Interculturales” (CEMyRI).
Giancarlo Lucchetti MD, PhD, received his MD from the Santa Casa of São Paulo Medical School, Brazil and his PhD from the Federal University of São Paulo, Brazil. He currently works as an associate professor at the school of Medicine from the Federal University of Juiz de Fora (UFJF), Brazil. He works supervising PhD students in the Health and Public Health programs at UFJF. He is also a Grantee of Research Productivity Scholarship – Level 2 in the area of Medicine for the Brazilian National Council for Scientific and Technological Development (CNPq).
Juan Vega-Escaño, graduated in nursing from the University of Seville since 2001. He is currently developing his work as a nurse in the area of Health Surveillance since 2003 as a Specialist Nurse in Occupational Nursing. Official Master’s Degree in New Trends in Health Sciences and Master’s Degree in Occupational Risk Prevention from the University of Seville. He is currently a PhD candidate at the Nursing Department of the Faculty of Nursing, Physiotherapy and Podiatry of the University of Seville and have carried out a pre-doctoral research stay at the Escola Superior do Saúde at the University of the Algarve (Portugal).