
Abstract
Despite improvements in the treatment of stroke, many individuals still face cognitive, emotional, and physical impairments. Stroke is a leading cause of serious long-term disability and subsequent failure to return to work (RTW). The purpose of this literature review was to synthesize and discuss the literature relevant to factors affecting RTW for stroke survivors, summarize the identified gaps, and discuss steps occupational health nurses can take to facilitate RTW among stroke survivors. A literature search was conducted using the keywords: “stroke,” “cerebrovascular disease,” “return to work,” and “employment.” After excluding articles based on inclusion/exclusion criteria, 19 quantitative research articles were reviewed. Consistent themes found in the literature affecting RTW following stroke included physical, social, and cognitive factors. One of the most consistent predictors of RTW found was stroke severity. Individuals who experienced a mild to moderate stroke, those of Caucasian ethnicity, and higher socioeconomic levels were more likely to RTW. Findings suggest the importance of future studies to examine factors among African American stroke survivors that predict RTW and the role of occupational health nurses.
Keywords
According to Benjamin et al. (2017), about 92.1 million American adults are living with some form of cardiovascular disease or the after effects of stroke. Each year, almost 800,000 people experience a new or recurrent stroke (Benjamin et al., 2017). African Americans below 65 years of age are 2 to 5 times more likely than Caucasians to experience strokes and have strokes at younger ages (Kissela et al., 2012). African American males, as compared with other racial/ethnic groups, have higher rates of hypertension (45%), obesity (37%), and diabetes (14%), which are the most common conditions that increase the risk of stroke (Benjamin et al., 2017).
Despite improvements in the treatment of stroke, many individuals still face cognitive, emotional, and physical impairments. Moreover, disabilities resulting from stroke may have considerable negative consequences for quality of life and self-esteem in individuals, including the loss of productivity and resulting economic burden (Arwert et al., 2017). In the United States, stroke is a leading cause of serious long-term disability (Benjamin et al., 2017) and subsequent failure to return to work (RTW), with RTW rates varying from 11% to 85% (Arwert et al., 2017). Failure to RTW following stroke has been associated with negative health outcomes such as cardiac disease, depression, isolation, poor coping skills, and higher mortality rates (Harris, 2014). The physical, psychological, social, financial, and economic costs associated with loss of productivity for patients post-stroke are reported to be billions of dollars each year (Harris, 2014). African Americans are disproportionately affected by stroke; however, factors affecting RTW for this population have not been studied extensively.
The purpose of this study was to synthesize and discuss the relevant to factors affecting RTW for stroke survivors, summarize the identified gaps, and discuss the importance of RTW following stroke to occupational health nursing. There is a dearth of evidence that focuses on African American stroke survivors’ RTW; therefore, this literature review focused on stroke survivors across all populations.
Method
For this study, we used the World Health Organization (1988) definition of stroke as “a clinical syndrome consisting of rapidly developing clinical signs of focal disturbance of cerebral function lasting more than 24 hours or leading to death with no apparent cause other than a vascular origin” (p. 108). RTW was defined as employment status, which was either self-reported or assessed through questionnaires regarding employment. RTW included returning to previous job, returning to similar or modified job, or starting a new job, and included both part-time and full-time work. No restrictions were placed on geographic location. Studies focusing on traumatic brain injury, case studies, and reviews were excluded.
An electronic literature search was conducted using the databases PubMed, Cumulative Index of Nursing and Allied Health Literature (CINAHL), and Scopus. Search terms were separated into two groups: stroke and employment. Stroke terms included “stroke” and “cerebrovascular disease.” Employment terms included “return to work” and “employment.” Terms were searched in the title, abstract, and keywords of articles. The search was limited to articles published between 2009 and 2018, written in English, and available in full-text. Inclusion criteria included articles with the following focus: (a) working-age adults with a clinical diagnosis of stroke, (b) RTW evaluated as an outcome, (c) quantitative study design, and (d) published within the past 10 years.
Findings
The database search yielded 2,586 articles. After excluding duplicate citations, 521 articles were screened according to inclusion/exclusion criteria. A total of 349 articles were excluded after title/abstract screen. Seventy articles were excluded after full-text screen, and 50 articles were excluded during data extraction. Nineteen quantitative research articles were reviewed, as illustrated in Figure 1. Articles included in the review are listed in Table 1, which highlights the main domains that were examined in the manuscript with respect to RTW and stroke including physical, social, and cognitive factors.
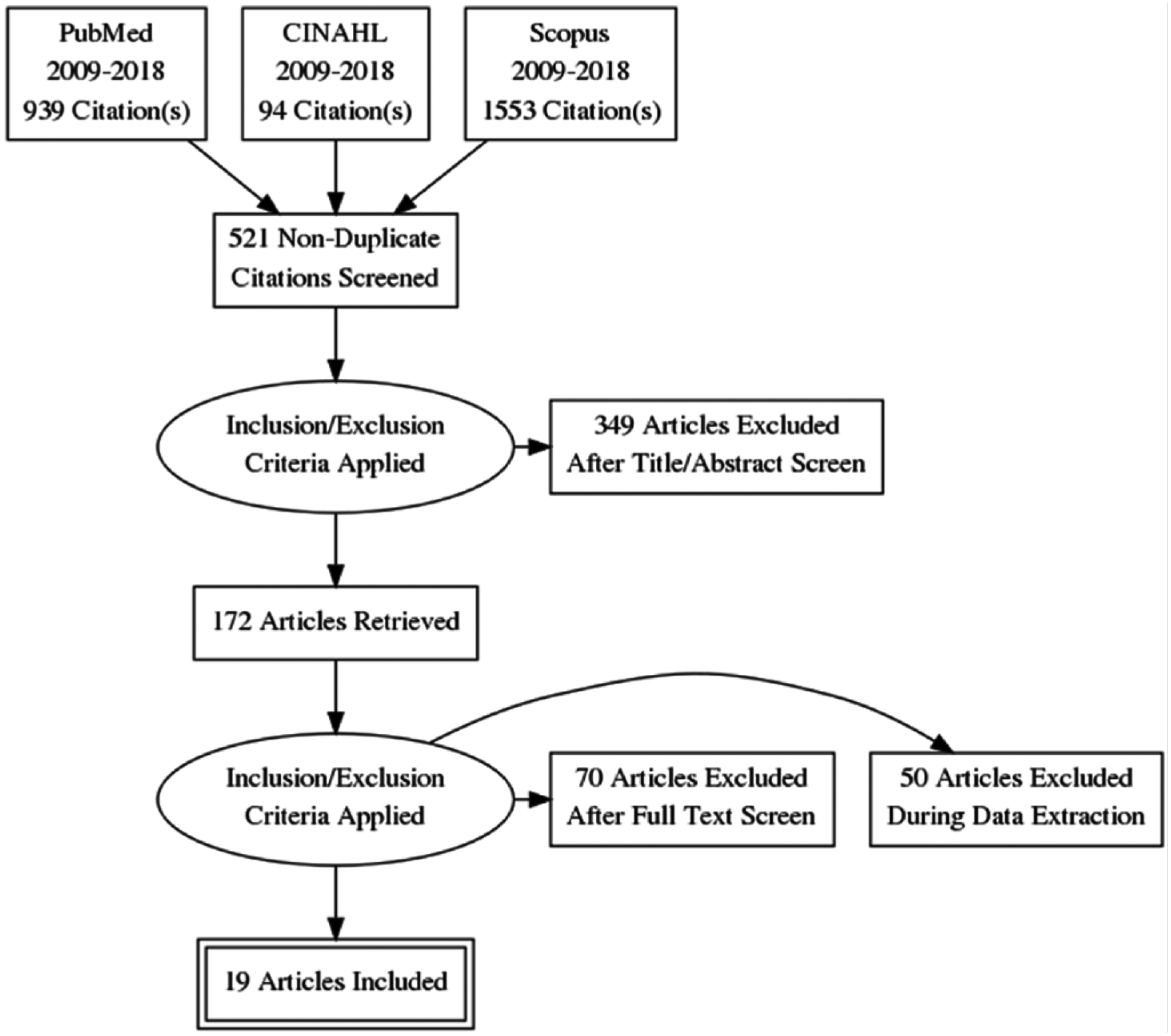
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) diagram.
Summary of Literature Regarding Return to Work and Stroke (n = 19 Studies)
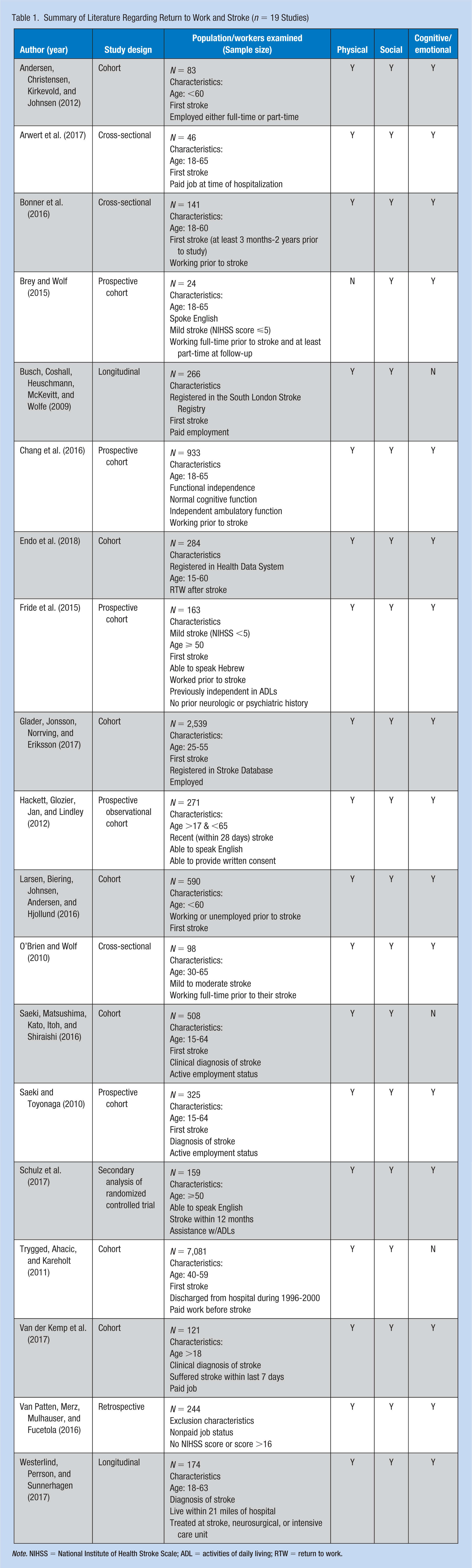
Note. NIHSS = National Institute of Health Stroke Scale; ADL = activities of daily living; RTW = return to work.
Studies included in the review collected data regarding demographics, stroke severity, disability, occupation, educational level, and presence of mood disorders (anxiety and depression). Individuals who experienced a mild to moderate stroke, of Caucasian ethnicity, and higher socioeconomic levels were more likely to RTW. The range of RTW varied from 28% to 88% across these studies.
Physical Factors
One of the most consistent predictors of RTW found was stroke severity (Saeki, Matsushima, Kato, Itoh, & Shiraishi, 2016; Van Patten, Merz, Mulhauser, & Fucetola, 2016; Westerlind, Perrson, & Sunnerhagen, 2017). The National Institute of Health Stroke Scale (NIHSS) was used across studies to measure stroke severity during time of hospitalization and time of discharge. Individuals who experienced a mild to moderate stroke were more likely to RTW, compared with those with severe disabilities (Larsen, Biering, Johnsen, Andersen, & Hjollund, 2016). Individuals 65 years of age and younger were more likely to RTW (Bonner et al., 2016; Chang et al., 2016; Glader, Jonsson, Norrving, & Eriksson, 2017; Saeki & Toyonaga, 2010). However, age has not been found to be a significant predictor of RTW in different age groups below the age of 65 years (Arwert et al., 2017; Larsen et al., 2016; Westerlind et al., 2017). Neither type of stroke (hemorrhagic, ischemic) nor location of lesion has been consistently predictive of RTW (Saeki & Toyonaga, 2010; Van Patten et al., 2016). Hemorrhagic stroke occurs when a blood vessel in the brain ruptures. Ischemic stroke occurs when a blood vessel in the brain is obstructed by a clot. Increased RTW rates have been associated with shorter hospitalization and mild stroke (Chang et al., 2016; Trygged, Ahacic, & Kareholt, 2011). For example, individuals who were hospitalized an average of 10 days or less were more likely to RTW. Functional disability was an important determinant in an individual’s RTW (Bonner et al., 2016). Lower scores on the Modified Rankin Scale (mRS), indicating no to slight disability, were positively associated with an individual’s ability to RTW. In contrast, dependence on others for activities of daily living (ADLs) was negatively associated with RTW (Fride et al., 2015; Glader et al., 2017; Hackett, Glozier, Jan, & Lindley, 2012; Larsen et al., 2016). Saeki and Toyonaga (2010) found that individuals who independently performed ADLs (e.g., dressing, toileting, and mobility) were 3 times more likely to RTW earlier compared with those who were dependent on others for ADLs.
Social Factors
Socioeconomic factors also play a role in RTW. Numerous studies have found increased rates of RTW for individuals who are Caucasian and have higher levels of education and income (Bonner et al., 2016; Busch, Coshall, Heuschmann, McKevitt, & Wolfe, 2009; Glader et al., 2017; Saeki & Toyonaga, 2010; Schulz et al., 2017; Trygged et al., 2011; Van Patten et al., 2016). Busch et al. (2009) found that African Americans were less likely to RTW after a first stroke, but it was unclear what caused these differences—whether it was the inability to work, individual preferences, or barriers to RTW. Gender was also found to be associated with RTW, such that female stroke survivors had lower rates of RTW than males (Busch et al., 2009; Saeki & Toyonaga, 2010; Trygged et al., 2011). Although, specific occupation has not been found to be predictive of RTW, studies have shown that blue-collar workers compared with skilled workers have decreased rates of RTW (Bonner et al., 2016; Brey & Wolf, 2015; Chang et al., 2016; Van Patten et al., 2016). The majority of studies did not identify specific occupations but classified workers as either skilled (professional) or unskilled (manual labor). Individuals who worked in manual labor occupations (e.g., laborers, craftsmen, machine operators, etc.) were less likely to RTW. It is noteworthy that skilled workers often have higher incomes and lower physical and psychomotor demands at work (Brey & Wolf, 2015). The majority of workers who did RTW returned to their previous job, but in a modified capacity (Chang et al., 2016; O’Brien & Wolf, 2010).
Cognitive/Emotional Factors
The effect of comorbidities pre- and post-stroke on RTW have not been extensively studied; however, psychiatric disorders such as depression and anxiety are emerging as predictive factors for RTW (Arwert et al., 2017; Glader et al., 2017; Van der Kemp et al., 2017). Higher rates of depression were found in non RTW groups (Arwert et al., 2017). Although it is unclear whether being diagnosed with depression and/or anxiety directly affects an individual’s ability to RTW post-stroke or whether failure to RTW causes depressive symptoms. The authors hypothesized that an individual’s mental health may be negatively influenced by unemployment (Arwert et al., 2017). High scores for depression on the Hospital Anxiety and Depression Scale (HADS) have been found in individuals who did not RTW (Arwert et al., 2017). Post-stroke depression (PSD) was associated with lower RTW rates at longer periods post-stroke (Arwert et al., 2017; Van der Kemp et al., 2017). Endo et al. (2018) found 21% of stroke survivors had recurrent sickness absences due to mental disorders. Cognitive functioning was significantly associated with RTW 1-year post-stroke (Fride et al., 2015; Van der Kemp et al., 2017). Individuals with cognitive impairments were less likely to RTW compared with those without cognitive impairments (Fride et al., 2015; Westerlind et al., 2017). Individuals who do RTW often complain of various cognitive deficits, such as trouble keeping organized, difficulty concentrating, and fatigue (O’Brien & Wolf, 2010). The prevalence of post-stroke fatigue was estimated to be 40% to 74% and has been found to be a barrier to RTW (Andersen, Christensen, Kirkevold, & Johnsen, 2012; Bonner et al., 2016).
Discussion
Studies predicting RTW in stroke survivors have used populations from multiple countries, varying follow-up periods, and inconsistent definitions of both “stroke” and “return to work” (Van Patten et al., 2016). This has made comparisons across studies difficult. RTW has been measured as both the process of returning an injured worker to work and the measurable final outcome of disability. Despite changes in stroke treatment, such as the use of tissue plasminogen activator (TPA) and rehabilitation, RTW rates have not improved. In a cohort study in Japan, the RTW rate was higher prior to medical innovations, with rates being 58% for the initial cohort in years 1986 to 1990 and 55% for the second cohort in years 2006 to 2007 (Saeki et al., 2016). Although patients who are younger and have mild strokes (limited to no functional disabilities) have higher rates of RTW, they are relatively understudied. Despite the prevalence of stroke in African Americans, there was a lack of participation from this population in reviewed studies. Bonner et al. (2016) found that participation in rehabilitation is not associated with successful RTW. Economics also plays an important role in RTW. Individuals with a lower, compared with higher, socioeconomic status are more likely to experience a stroke and have poorer outcomes, even when severity of stroke is similar (Brey & Wolf, 2015; Trygged et al., 2011). Future studies are needed to identify reasons for these RTW disparities. Some individuals are able to RTW but may still face absences from work due to a recurrent stroke or mental disorder, such as PSD (Endo et al., 2018). Difficulties comparing diverse stroke populations, national strategies in rehabilitation, employment of disabled persons, and income supplements could contribute to variations in the proportion of patients who RTW after stroke (Chang et al., 2016; Glader et al., 2017). Few studies identified occupation or hours worked per week prior to stroke to allow for conclusions regarding employment post-stroke (Arwert et al., 2017; O’Brien & Wolf, 2010; Trygged et al., 2011).
Limitations
This review has several limitations. First, there was a small number of studies reviewed. Of these studies, a majority were done outside of the United States that affects generalizability. There was also a lack of consistency in approaches to measuring RTW. The definition of RTW was inconsistent across studies as was the follow-up time period. Differences in sickness, disability, and retirement benefits in other countries most likely influenced RTW across studies.
Implications for Occupational Health Nursing Practice
Based on findings, some considerations emerged to improve practice, research, and education for occupational health nursing. Monitoring the course of an employees’ stroke hospitalization history can help predict potential complications and suggest the deployment of RTW support services. Under ideal circumstances, initiating employee preventive programs that minimize the incidence of stroke such as hypertension monitoring efforts may be beneficial. Occupational health nurses should be prepared to assist those individuals who do RTW. Advocating for individuals to have the resources necessary to perform their job within their capacity is important, which may include having the ability to take frequent rest breaks due to fatigue, use of adaptive devices for physical impairments, and support for depression and anxiety. Under the Americans With Disabilities Act (ADA), employers are required to provide reasonable accommodations to assist an employee in performing their job requirements (U.S. Equal Employment Opportunity Commission [EEOC], 2017). Accommodations can be deemed unreasonable if they are costly, disruptive to others, or too much for an employer to do reasonably (EEOC, 2017). Educational resources should be provided to occupational health and rehabilitation nurses to assist in identifying the factors affecting stroke survivors to promote successful RTW. Implications for research include increasing African American participation, conducting studies in the United States and consistency in the definition of RTW, as well as consistent follow-up time periods.
Conclusion
Employees are valuable members of the work environment, thus keeping them healthy and productive makes both human and financial sense. The ability to RTW following a stroke results in increased quality of life for stroke survivors (Chang et al., 2016; Saeki & Toyonaga, 2010). Even though African Americans are disproportionately affected by stroke and at younger ages, there are few studies exploring RTW rates in this population. Association between ethnicity and stroke outcomes, including RTW, is relatively unexplored (Glader et al., 2017). Future studies are needed to examine factors among African American stroke survivors that predict RTW in an effort to increase rates among this population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by the Deep South Center for Occupational Health and Safety (NIOSH-T42OH008436).
Author Biographies
Kristin D. Ashley, MSN, RN, CNE, is an instructor in the School of Nursing & Allied Health at Tuskegee University in Tuskegee, Alabama. She is currently pursuing a PhD in nursing with a research focus on return to work among African American male stroke survivors.
Loretta T. Lee, PhD, CRNP, FNP-BC, is an assistant professor at the University of Alabama at Birmingham and family nurse practitioner. Her primary goal is to advance scientific knowledge regarding cardiometabolic risk factors for older adults, with a particular emphasis on ensuring that culturally and ethnically appropriate intervention strategies are used to eliminate racial health disparities.
Karen Heaton’s, PhD, COHN-S, FNP-BC, FAAN, FAAOHN, program of research is primarily focused on the effects of sleep deprivation and obstructive sleep apnea on cognition and injury risk in workers. For example, she has been involved in projects that explored the impact of distraction and health issues on driving and driving performance among aging truck drivers, and self-assessment of driving performance compared with real-time simulated driving performance among truck drivers.