
Abstract
An employee is labeled “accident-prone,” and sustained an acute lumbar injury at work. Upon physical examination, a diagnosis of multiple sclerosis was suspected. She was referred to a public health clinic for further evaluation. This is a review article of multiple sclerosis and workplace interventions.
Keywords
TG, a 37-year-old female hotel housekeeper, was referred to an occupational health clinic by the hotel’s Human Resources manager for a fall that resulted in a low back injury. TG had been working as a hotel housekeeper for the past 3 years. The manager reported that TG, who had worked for the hotel for 3 years, is “a hard worker and a very kind lady but is accident-prone.” Furthermore, the manager stated that TG is always losing her balance and is uncoordinated.
TG explained to the occupational health nurse that she was attempting to pick up a box at the time of the accident. As she leaned forward to pick up the box, TG fell forward and rolled on her right side, sustaining a contusion on her right lower back. The fall was witnessed and reported to human resources. TG insisted that she was fine and did not want to go to the occupational health clinic for evaluation.
Upon examination, TG had a contusion with spasming on the right sacroiliac joint; she had full range of motion of the lumbar spine. Upon sensory examination, patchy areas of numbness, not following a specific dermatome, were noted. Motor examination of the lower extremities was 4/5 strength bilaterally. Upon examination of the patellar and Achilles reflexes, 5+/5+ were assessed bilaterally with bilateral sustained clonus.
These abnormal findings warranted further investigation. Reflexes of the upper extremities, triceps/biceps, and brachial radius were 5+/5+ bilaterally. Pronator drift revealed bilateral fine tremors. TG was unable to do rapid alternating hand movement, fell during tandem walking, and had a positive Romberg. Finally, TG was unable to perform finger to nose coordination and had bilateral nystagmus.
TG was born in the Soviet Union and had arrived in the United States 4 years earlier. She had a 20-pack year smoking history, but quit 2 years earlier due to the cost of cigarettes. She denied any other health concerns or surgeries. She stated that during the past 2 years, she had noticed more difficulty completing certain tasks (e.g., walking up a flight of stairs, carrying boxes, or focusing on an object because she was “seeing double”).
TG did not have health insurance so was referred to the local public health clinic. The social worker referred TG to the local hospital so she could be enrolled in Medicaid. Magnetic resonance imaging (MRI), with and without contrast, revealed multiple plaques in the cerebral cortex and cerebellum; the final diagnosis was multiple sclerosis (MS).
Multiple Sclerosis
Multiple sclerosis is a demyelinating disorder that affects the central nervous system (CNS). Fauci et al. (2015) described a triad of inflammation, demyelination, and formation of scarring or gliosis in the CNS. Multiple sclerosis can be a progressive disease or one of relapsing-remittance. Clinical manifestations include a sudden onset or slow development. Workers may exhibit a loss of strength in the upper or lower extremities. Upper motor signs and symptoms can include spasticity, hyperflexia, and gait disturbances (i.e., ataxia). Cranial nerve involvement includes diminished visual acuity or loss of central field vision. Workers may also complain of eye pain and blurring. Diplopia may be present due to lateral rectus muscle paralysis. Facial nerve weakness with a loss of taste may also be present.
Sensory symptoms include nonspecific pain or parenthesis anywhere on the body. Bowel or bladder dysfunction (e.g., episodes of constipation or urinary incontinence) may also be reported. Other general symptoms include vertigo, fatigue, and depression. Ancillary symptoms such as Lhermitte’s symptom (i.e., electrical shocks that radiate down either leg) have also been assessed (Fauci et al., 2015). Workers may also exhibit trigeminal neuralgia, hemifacial spasms, or glossopharyngeal involvement.
Four clinical types of MS have been identified. Relapsing/remitting MS is a common form characterized by brief, intense exacerbations that may occur over weeks to months. Ambulation is impaired and may not improve; however, in between exacerbations, workers may be neurologically stable. Secondary progressive MS is characterized by steady deterioration but no acute attacks. Primary progressive MS presents with a steady functional decline without abrupt attacks. Finally, progressive/relapsing MS is characterized by steady deterioration with acute exacerbations.
Epidemiology
Multiple sclerosis affects mostly women with an onset between 20 and 40 years of age (Fauci et al., 2015). According to the Journal of Managed Care, approximately 400,000 individuals have been diagnosed with MS and approximately 200 individuals are diagnosed annually in the United States (Tullman, 2013). Multiple sclerosis has both environmental and genetic etiologies (Tullman, 2013). It is speculated that adults with northern European backgrounds are at risk due to their lack of ultraviolet radiation exposure needed to generate adequate Vitamin D levels (Fauci et al., 2015).
Pathophysiology
Multiple sclerosis is characterized by infiltration of inflammatory mononuclear cells (i.e., T cells, microglia, and macrophages) in the CNS mostly white matter. B lymphocytes infiltrate the CNS and cause demyelination of the myelin sheath which is responsible for nerve conduction. The formation of plaques is the result of gliosis, a nonspecific reaction in the CNS that results in astrocytic scarring and loss of oligodendrocytes (Fauci et al., 2015). Ultimately, these plaques disrupt nerve conduction with axonal loss that results in motor neuropathy.
Plaques are randomly distributed in the CNS but have an affinity for the periventricular white matter, optic nerves, and spinal cord. Eventually, plaques form in the cerebral cortex, deep nuclei, and brainstem. Workers exhibit visual loss, paralysis, sensory deficits, and balance difficulties. Memory may eventually be impaired.
Diagnostics
Multiple sclerosis is diagnosed by at least two signs and two symptoms that reflect disease of the white matter (e.g., cerebellar dysfunction such as balance disturbances or visual changes that last for more than 24 hours at different times; Fauci et al., 2013). An MRI of the brain and spinal cord, with and without contrast, reveals lesions and demyelination. Evoked potentials may reveal sensory and motor deficits. Finally, a sample of cerebrospinal fluid shows increased levels of IgG and mononuclear cells (Table 1).
Differential Diagnosis of MS
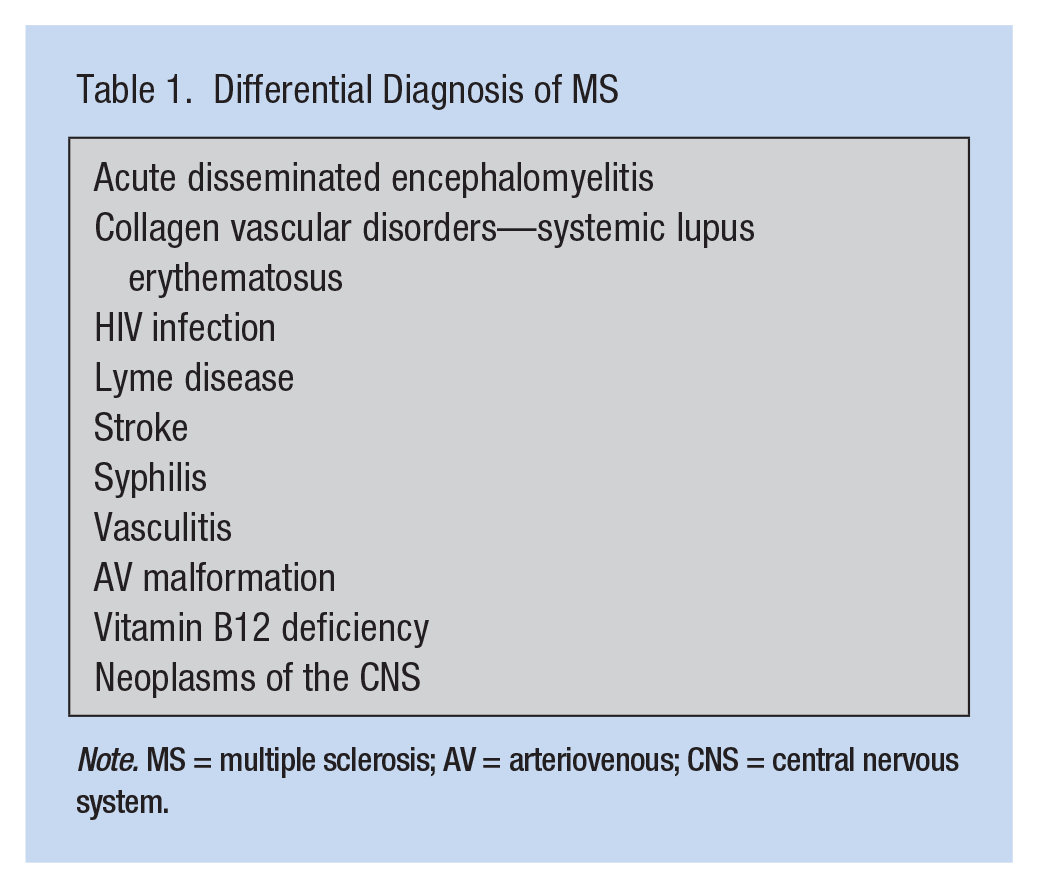
Note. MS = multiple sclerosis; AV = arteriovenous; CNS = central nervous system.
Interventions
Multiple sclerosis is a progressive disease without a cure. Acute attacks and relapsing episodes may be treated with glucocorticoids and plasma exchange (Burton, O’Connor, Hohol, & Beyene, 2012; Fauci et al., 2015). For relapses, interferon beta, Glatiramer acetate, and natalizumab may be used to inhibit the inflammatory response and the production of cytokines which may delay the progress of the disease; intravenous immunoglobulins may be used to reduce exacerbation of the disease (Fauci et al., 2015). Side effects of these medications (e.g., thinning of the skin, osteoporosis, and increased risk of infections) must be considered (Moghadam-Kia & Werth, 2010).
Other treatment options may include medications for ataxia and tremors (e.g., propranolol). Spasticity and spasms may be treated with diazepam or cyclobenzaprine and associated pain with anticonvulsants (e.g., gabapentin or pregabalin). Lifestyle changes should include a high fiber diet to prevent constipation and heat avoidance (Fauci et al., 2015). Memory impairment with depression symptoms should be managed by a specialist and may require cognitive training (Nourbakhsh, Julian, & Waubant, 2016). Occupational and physical therapy should be initiated. Dietary interventions (e.g., increasing polyunsaturated fatty acids and vitamin supplementation) remain inconclusive (Fainotti et al., 2012).
Implication for Occupational Health Nurses
Many occupational health nurses provide physical examinations to employees. They must recognize abnormal physical findings that warrant further investigation. Caution should be used when an employee is labeled “accident-prone.” A full history of “accidents,” or falls should determine underlying personal risk factors. If an employee is diagnosed with MS, the occupational health nurse should collaborate with the employee and other workplace professionals to maintain a safe workplace environment for the employee. Once employees are diagnosed with MS, they must be assessed to determine if they are “fit for duty” or if the employer can accommodate employees’ limitations. Intensive case management may also be warranted with appropriate consults (Gibson & Frank, 2002).
Physical therapy may be consulted for gait and balance training to prevent falls and, if appropriate, to recommend assistive devices. Home exercise programs can be implemented for strength and stretch training to improve muscle function and mobility. However, exercise therapy to improve fatigue is inconclusive (Rietberg, Brooks, Uitdehaag, & Kwakkel, 2004). Occupational therapy may be consulted for self-care activities such as dressing, grooming, and eating. An ergonomic consult to address fatigue and motor issues at the workplace may be warranted. For example, if the employee uses a computer, using voice recognition and large print may be required. Issues of dexterity should be addressed as well. Bowel and bladder training should be initiated if incontinence is an issue (Gibson & Frank, 2002).
Vocational rehabilitation may be considered when addressing physical, psychosocial, environmental and memory/attention impairments (Khan, Ng, & Turner-Stokes, 2009). Work is perceived to improve quality of life and may be therapeutic for an employee with a disability (Wadden & Foster, 2006). Other considerations may include heat adjustments in the workplace and mobility accommodations (Khan et al., 2009).
Conclusion
Unfortunately, TG was diagnosed with advanced MS. A fit for duty assessment deemed her unsafe to work as a housekeeper. Due to lack of education and skills, TG was unable to transfer to another position at the hotel, but she was able to apply for disability.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Ann Regina Lurati is a nursing lecturer at California State University Monterey Bay.