
Abstract
Shoulder pain is a common complaint in the workplace. A shoulder condition may arise from acute trauma or non-traumatic work-related activities. Shoulder pain falls into three categories: acute, chronic, and referred pain. The occupational health nurse can document detailed health histories and focused complaint-driven physical examinations. Nurses’ expert assessments can guide injured workers to necessary treatment, case management, and return to full employment.
Keywords
Every year, thousands of workers in the United States are hurt on the job. Shoulder conditions are one of the most common causes of pain and disability among adults, with a lifetime prevalence rate of 7% to 10% (Yousik Roh, Karandikar, Dutton, & Chen, 2015). Shoulder conditions may arise from acute trauma or, in some circumstances, from non-traumatic industrial activities (Walker-Bone & Cooper, 2005). Occupational factors related to shoulder pain in the workplace vary based on physical exposures related to the type of work, overall working conditions, repetitive activities, ergonomic resources, and past health history (Kennedy et al., 2010). Occupational health nurses can assist injured workers to recover and “stay at work.” Factors associated with shoulder conditions include trauma, overuse, inflammation, age-related tissue degeneration, and smoking (Tashjian, 2012). To establish a work-related cause of the condition, a careful occupational history and mechanism of injury needs to be established. Occupational health nurses can play critical roles in the health maintenance and recovery of injured workers. They are supportive and usually familiar with workplace exposures.
Injury-promoting job tasks can include
Carrying or lifting heavy loads on or above the shoulders, or carrying with the hands
Pushing and pulling heavy loads
Working with arms above the shoulder for more than 15-minute intervals
Repetitive arm and wrist movements combined with force for long periods
Overhead reaching
Due to the unique practice setting of occupational health nurses, workers’ compensation insurance regulations, and the needs of individual companies, shoulder injuries are managed differently. Yet, occupational health nurses support injured workers as they recover their health and full productivity. Once an injured worker is referred to an outside health care provider, it is important to continue communicating with both the treating provider and injured worker. The nurse must be familiar with workers’ compensation statutes in the state in which the occupational health nurse practices. Each state has different regulations for shoulder injuries to be accepted as an occupational injury or disease (United States Department of Labor, 2016).
This article addresses the key elements in shoulder assessment for occupational health nurses providing additional tools as resources for monitoring, treatment, and case management.
Anatomy of the Shoulder
In assessing shoulders in the occupational health setting, a basic understanding of shoulder anatomy is needed. The shoulder joint is the most complex joint in the human body. This complex network of anatomic structures provides exceptional mobility, enhanced by a girdle of three bones, the clavicle, scapula, and proximal humerus (Galatz, 2010). Four articular surfaces (joints), steno clavicular, acromioclavicular (AC), glenohumeral, and scapulothoracic, are found within the girdle of the shoulder itself. The glenohumeral joint, or shoulder joint, is the principal articular surface. A common term used in describing shoulder injuries is a rotator cuff injury. The rotator cuff is comprised of four muscles, supraspinatus, infraspinatus, subscapularis, and teres minor, and a cuff around the head of the humerus to which all four muscles attach. Three additional muscles, the teres major, latissimus dorsi, and pectoralis major provide additional support to the glenohumeral joint (shoulder joint). The neural networks of the brachial plexus form proximal to the glenohumeral joint and innervate this complex joint (Figure 1; Galatz, 2010).
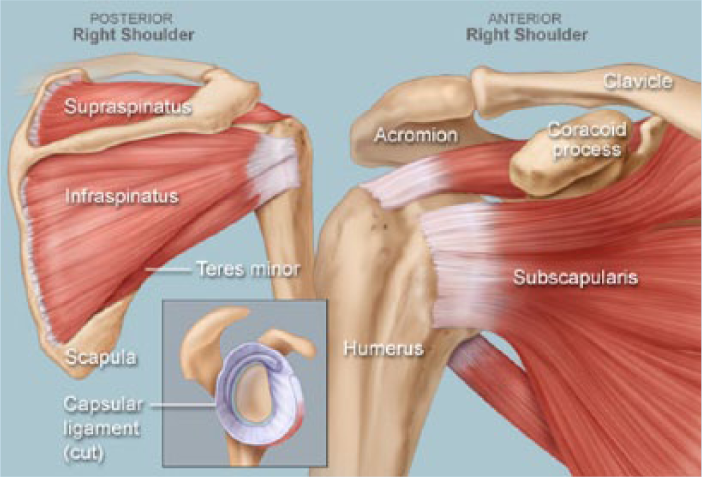
Anatomy of the shoulder.
During the occupational health nurse’s assessment, it is important to differentiate between acute, chronic, and referred shoulder pain. Based on whether the pain is acute, chronic, or referred, the nurse will recommend monitoring, referral for treatment, or longer term case management according to the specific setting or protocol.
Acute Shoulder Pain
Acute shoulder pain is defined as pain lasting less than 2 weeks. Overuse, an overstretched arm, or blunt trauma are common causes of acute pain; so considering workplace injuries and understanding the mechanism of injury is essential (e.g., falls directly on the shoulder, or falls onto an outstretched arm). Fractures and dislocations usually present as acute pain. Fractures of the clavicle, proximal humerus, or scapula and undifferentiated strain or sprain of the shoulder present as acute shoulder pain; the majority of dislocations produce acute pain in the anterior glenohumeral joint.
Chronic Shoulder Pain
Chronic shoulder pain lasting longer than 4 weeks without resolution often presents as an injury to the rotator cuff, occurring most commonly in middle age or older workers. With the aging workforce, occupational health nurses will see rotator cuff injuries as a common cause of shoulder pain. Rotator cuff injuries result from repetitive work tasks, poor muscular conditioning, poor posture, difficult ergonomic positions, and failure of the subacromial bursa to protect the supporting tendons (Tashjian, 2012). Rotator cuff injuries are often referred to as impingement syndrome, defined as compression of the rotator cuff tendons and the subacromial bursa between the greater tubercle of the humeral head and the lateral edge of the acromion process. Long-term rotator cuff injuries can present as adhesive capsulitis (frozen shoulder), which is a stiffened glenohumeral joint that has lost range of motion (ROM). Any shoulder pain that causes an injured worker to protect the shoulder can lead to decreased mobility and ultimately adhesive capsulitis (Kennedy et al., 2010)
Referred Shoulder Pain
Employees’ descriptions of pain can assist occupational health nurses to decide whether pain is shoulder based or referred from the neck, which is common in workplace injuries. Referred pain from the neck usually develops in or near the shoulder blade or on the side of the neck. The pain is described as sharp, stabbing, burning, or tingling. This referred pain may radiate down past the elbow and even into the hand. In contrast, pain that is shoulder based develops in the shoulder itself or on the outside of the upper arm. Often described as dull, aching pain, shoulder pain is elicited with overhead or behind the back reaching or when lifting. Shoulder pain persists at night and improves when resting the arm (Yousik Roh et al., 2015).
Although less common, many health-related conditions can present as referred shoulder pain including myocardial ischemia, distension from the hepatic capsule to gallbladder and liver disease, perforated or ruptured ectopic pregnancies, splenic laceration, and intrathoracic tumors. In the occupational setting, the focus should be on workplace injuries leading to referred shoulder pain. Workplace injuries involving the cervical spine, thoracic outlet syndrome, or brachial plexus trauma can present as referred shoulder pain. Shoulder pain usually worsens with activity or movement of the arm or shoulder. With referred pain, the pain is poorly localized or vaguely described and not produced with movement of the shoulder or arm (Yousik Roh et al., 2015).
History
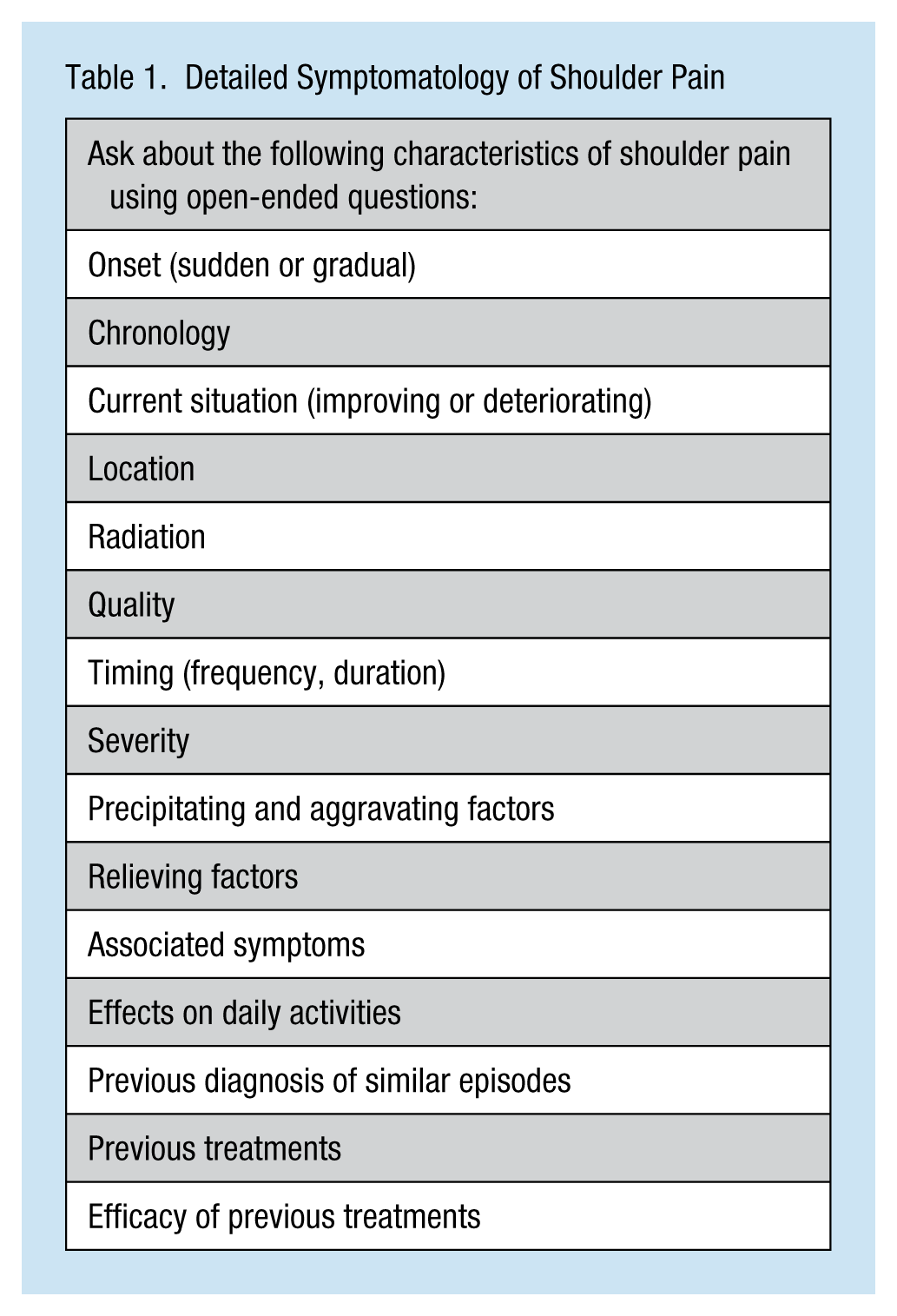
Documenting a thorough history of the complaint is key to assessing shoulder pain. The history is divided into three parts. First is the two-part history of the complaint, detailed symptomology of the complaint (Table 1), and directed questions related to the workplace (see sidebar). History of the shoulder injury and pain should include a review of systems and symptoms. For the musculoskeletal system, inquire about the neck and elbow. Ask questions about pain and ROM. Other systems to include are neurologic, respiratory, and cardiac as well as other general constitutional symptoms. Focus on non-musculoskeletal concerns if a suspicion of referred shoulder pain exists (Table 2).
Detailed Symptomatology of Shoulder Pain
Review of Systems and Symptoms
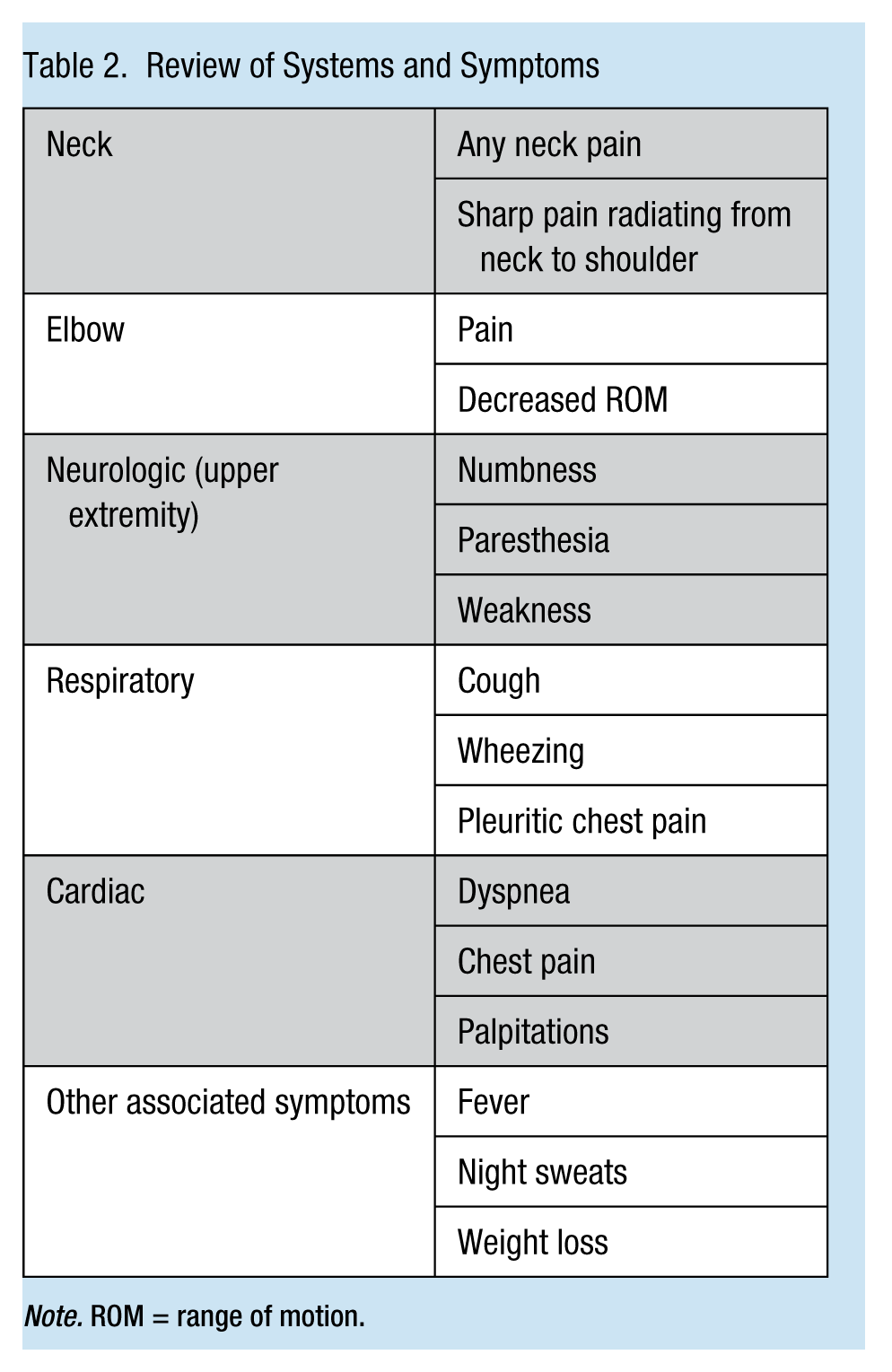
Note. ROM = range of motion.
The history is not complete unless it includes past health history. In an occupational health setting, ask about previous shoulder injuries and treatments, any shoulder-based diagnostic testing, hospitalizations, surgeries, and pain management. In terms of overall health history, review the injured worker’s medications, including herbals and supplements, and medication allergies.
Directed questions related to the workplace setting:
What is your dominant hand?
What are your job duties/work activities?
How long have you been at this particular job?
Any personal safety concerns in your job duties?
Was there an injury you can recall?
Describe the injury in detail
Specifically, what activities were being done at the time of the injury?
Lifting overhead, pulling, throwing, or no apparent cause for injury or re-injury?
Ever had a previous injury to this affected site?
Does the pain occur during activity but not restrict performance?
Does the pain occur during activity but restrict performance?
What other work settings have you worked in?
Have you always been a laborer?
What hobbies do you engage in?
Do you work at a second job?
What do you do for recreation?
Physical Examination
As occupational health nurses, having a private space to examine injured workers is essential. While measuring vital signs, assess general appearance, that is, color, apparent state of health, appearance of comfort or distress, nutritional status, hydration, and hygiene. The shoulder examination should include four components: inspect, palpate, assess ROM, and perform special tests.
Inspection involves observing how workers move and carry their shoulders. The nurse should inspect the front and back of the shoulder and the height of the shoulders and scapulae, comparing the injured shoulder with the non-injured shoulder. The examination, in addition, should assess swelling, bruising from recent trauma, and scars that could indicate old trauma. Assessing for deformity of the clavicle and glenohumeral joint is also essential. Asymmetry of the shoulder can occur with any number of injuries.
Palpation involves touching the necessary structures of the shoulder. With both shoulders exposed, palpate the AC joint, sternoclavicular joint, cervical spine, biceps tendon, anterior glenohumeral joint, coracoid process, acromion, and scapula for atrophy and swelling. In assessing for tenderness and pain, the AC joint, bicep tendon, and the greater tuberosity of the humerus (supraspinatus) should be included.
Assessment of active and passive ROM (i.e., internal rotation, external rotation, and abduction) should be included in a focused shoulder examination. Again, the injured shoulder should be compared with the uninjured shoulder (Figure 2).
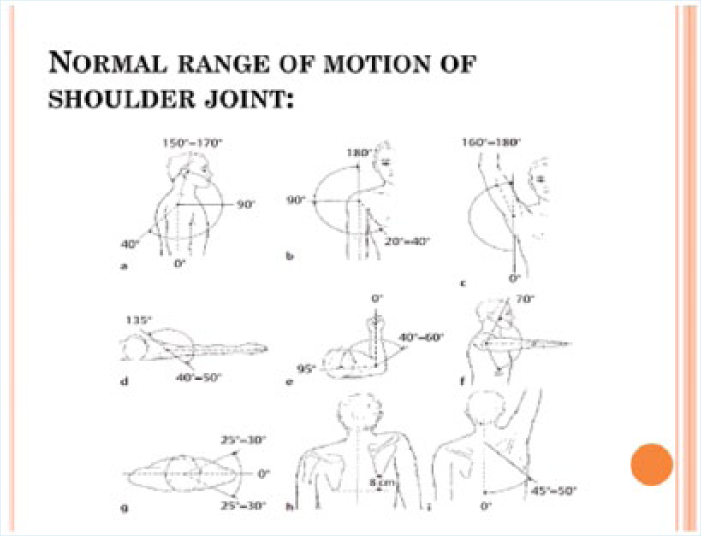
Range of motion of shoulder joint.
Special tests or maneuvers can assess the instability of the shoulder joint and whether a rotator cuff injury has occurred. The occupational health nurse should be prepared to use a small number of special tests to assess injured workers’ shoulders. The authors have chosen to describe four commonly used tests (Figure 3).
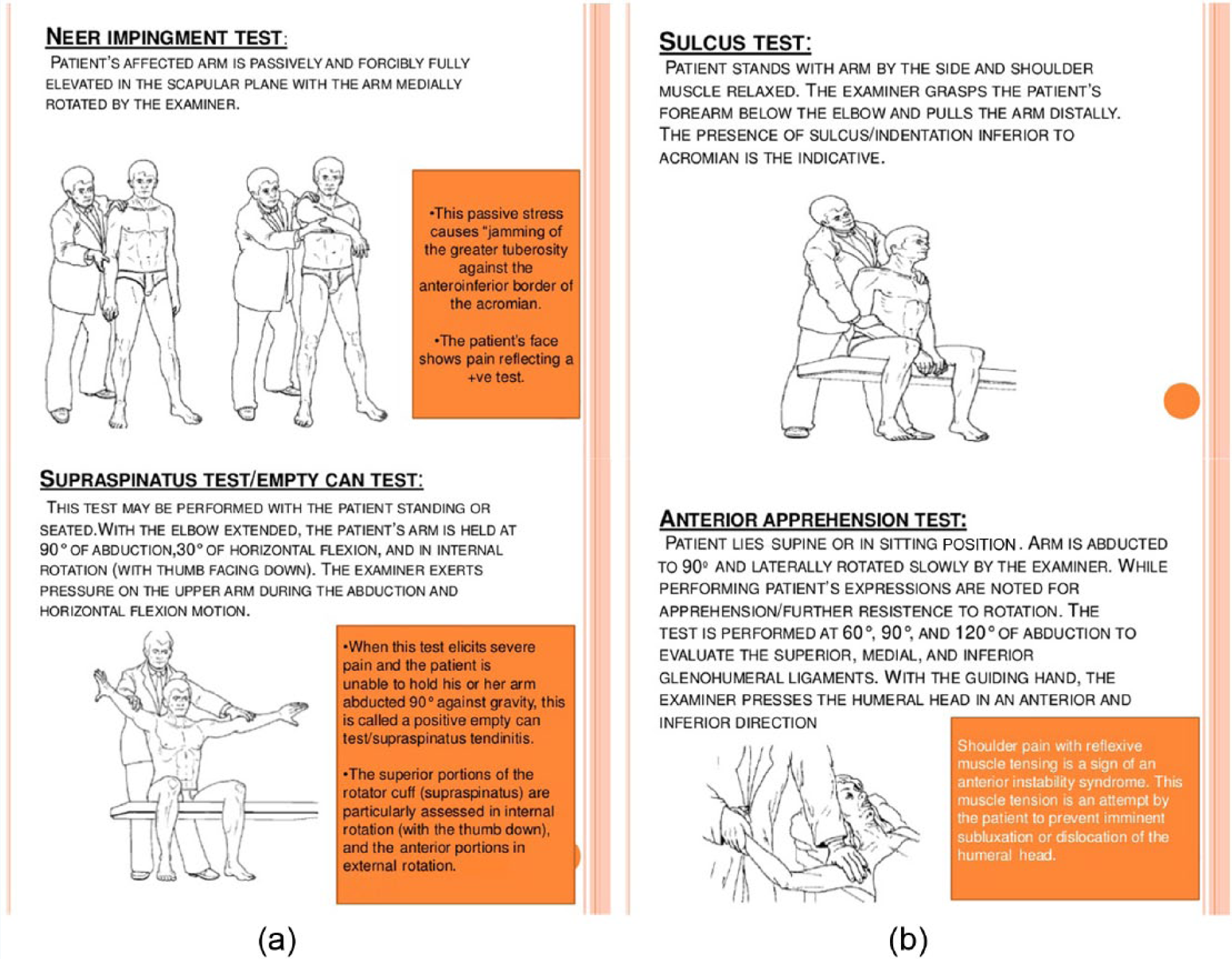
Special test in shoulder pain assessment: (a) Tests for rotator cuff impingement and (b) tests for instability.
During a musculoskeletal exam, the nurse should examine the joint above and below the shoulder (i.e., the neck and elbow). For the neck, the nurse should palpate, assess ROM, and if concerned about referred pain to the shoulder, perform a Spurling’s test. This test, which is used to determine whether shoulder pain is referred from the neck, involves having workers turn their heads to the affected side while the examiner extends the head and applies downward pressure. If this movement induces symptoms, the Spurling’s test is positive. If no symptoms occur, the nurse should induce overpressure with hands on the head; if this induces symptoms, the Spurling’s test is also positive. For the elbow, the nurse should palpate for tenderness around the joint and assess for full active and passive ROM.
In summary, occupational health nurses are capable of documenting injured workers’ health history and completing a focused complaint-driven physical examination. Occupational health nurses’ expert assessment will guide injured workers to necessary treatment and be the foundation for case management activities and full employment.
Case Management and the Occupational Health Nurse’s Role
Case management has been described as a process to manage cost and treatment, thus returning injured workers to the workplace in a timely manner (Guzik, 2008). An effective workplace case management program should take into consideration the needs of injured workers and each company’s available resources to accommodate work restrictions (Guzik, 2008; Noel, 2010). Many times, shoulder rehabilitation after surgery can take several weeks and is considered high-cost. Therefore, modified duty programs can assist workers during the early transition back to work. These programs embrace health and safety in the workplace and decrease costs in time lost, health care expenses, and insurance premiums.
Occupational health nursing as defined in the 19th century has focused on prevention, education, and controlling and eliminating hazards (Guzik, 2013). However, trauma still occurs at the worksite and occupational health nurses should collaborate with other health care providers and communicate essential work status and job requirements to develop an appropriate plan that supports injured workers’ recovery. Often, injured workers worry about the future and losing their jobs (Guzik, 2013). Occupational health nurses can be sure injured workers feel needed and reassured that their jobs are secure. Occupational health nurses should continue communicating with primary care providers and physical therapists so that injured workers keep appointments and maintain rehabilitation regimes. All of these elements support workers’ positive self-images of being productive employees and reduce work-related stress.
Conclusion
Thousands of injured workers and employees face difficult challenges with shoulder injuries (Guzik, 2013). Therefore, a comprehensive approach from occupational health nurses, modified duty programs, primary care providers, and rehabilitation teams is critical to injured workers’ full recovery (Guzik, 2008). Occupational health nurses can work with all stakeholders to develop appropriate and realistic goals and facilitate communication. Occupational health nurses who can accurately assess shoulder injuries and refer workers for early treatment will have greater success returning injured workers to their jobs and preventing permanent disability.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Sarah A. Kooienga PhD, FNP ARNP is an Assistant Professor at the Fay W. Whitney School of Nursing University of Wyoming, Laramie WY. She has more than 25 years experience as a FNP and is interested in expanded RN roles.
Melody Rasmor, EdD, RN, ARNP-BC, COHN-S, is a FNP and a Certified Occupational Health NP Specialist with over thirty years of experience. She has worked as an occupational nurse consultant to a variety of U.S. companies. Currently, she is an assistant clinical faculty for Washington State University, Vancouver, WA.