
Abstract
According to the Bureau of Labor Statistics, more than 18 million health care workers in the United States are currently employed in the health care field and at risk of infectious respiratory exposure. With the emergence of global infectious diseases such as Ebola and Severe Acute Respiratory Syndrome (SARS), there is a need for increased and more clinically competent use of respiratory protection among healthcare workers. In an effort to improve knowledge about the practice of respiratory protection against respiratory infectious agents, a NIOSH-funded project that included an educational program, observations of HCWs, and focus groups was conducted. This study aimed to develop, implement, and evaluate respiratory protection educational program for HCWs and hospital management. This study identified respiratory protection practice issues among HCWs and strategies for integration of respiratory protection standards and procedures into practice. Findings from these efforts were used to develop respiratory protection competencies. Any worker who has the potential for respiratory exposure to infectious agents should be protected and should be able to demonstrate these specific competencies to achieve a standard level of respiratory protection.
With the emergence of global infectious diseases such as Ebola, severe acute respiratory syndrome (SARS), Influenza A H1N1, and other highly infectious diseases, the need for increased and more clinically competent use of respiratory protection is essential (Baka et al., 2007). According to the Bureau of Labor Statistics (2018), more than 18 million health care workers (HCWs) in the United States (US) were employed in the health care field and at risk of infectious respiratory exposure (National Institute for Occupational Safety and Health [NIOSH], 2014) with approximately 35% employed in hospitals, 23% in nursing/long-term care facilities and residential care facilities, and 17% in physicians’ offices. This can include those who provide direct patient care or support the delivery of health care through dietary, clerical, engineering, security, maintenance, and housekeeping services.
As reported by the Occupational Safety and Health Administration (OSHA), the Centers for Disease Control and Prevention (CDC), and NIOSH (2015), HCWs, in the course of their work caring for patients, may potentially be exposed to aerosol transmissible disease (ATD) pathogens, which are particles or droplets suspended in air that can cause disease (Figure 1). These ATD pathogens require airborne precautions outlined by the CDC’s Healthcare Infection Control Practices Advisory Committee (HICPAC), which includes the use of a respirator (e.g., N95 filtering face piece respirator). In addition, airborne precautions should be implemented when aerosol-generating procedures are being conducted on patients infected with other forms of pathogens that are not considered ATDs (e.g., seasonal influenza). These infectious microorganisms can also become aerosolized during procedures such as bronchoscopies, electrocautery surgery, open suctioning, intubation, and possibly when infected patients are coughing (Banach et al., 2017; Noti et al., 2012; OSHA CDC, & NIOSH, 2015). For example, although droplet precautions (CDC, 2017, 2018) are recommended by the CDC for seasonal influenza, HCWs performing aerosol-generating procedures on patients with seasonal influenza should wear respiratory protection equivalent to a fitted N95 filtering face piece respirator (CDC, 2018). Aerosol studies show that infectious particles are released from patients’ respiratory tracts in a wide array of sizes and the size of a droplet or particle decreases as water evaporates with smaller particles staying airborne longer. How long a specific pathogen particle can remain viable is uncertain, especially with novel pathogens (Banach et al., 2017; OSHA, CDC, & NIOSH, 2015). Without knowing the contributions of each of the possible route(s) of transmission, all routes must be considered probable and consequential (Institute of Medicine [IOM], 2008).
CDC and HICPAC diseases/pathogens requiring airborne precautions.a
The risk of ATD pathogen exposure (Figure 1) to HCWs is not a new concern and among the many considerations for the health and well-being of HCWs are questions about what types of personal protective equipment (PPE) are needed to fully protect these frontline workers (Liverman, Harris, Rogers, & Shine, 2009). On the continuum of safety and infection prevention efforts in health care facilities, OSHA recommends following a hierarchy of controls, which includes hazard elimination, engineering controls, administrative and work practice controls, and use of PPE such as respirators (Liverman et al., 2009). Although engineering and administrative strategies are the preferred prevention and control approaches for reducing HCW infection risk, these methods are not always possible. Respiratory protection devices and other forms of PPE are considered the last, but not the least important, line of defense. PPE must be employed to offer protection (Wizner, Stradtman, Novak, & Shaffer, 2016).
PPE (e.g., respirators, gloves, gowns, eye protection, and other equipment) works by acting as a barrier to hazardous agents. However, HCWs face challenges in wearing PPE that include difficulties in verbal communication and interactions with patients and family members, maintaining tactile sensitivity through gloves, and physiological burdens such as difficulty in breathing while wearing a respirator (Hines, Mueller, Oliver, Gucer, & McDiarmid, 2017; IOM, 2008; Radonovich, Cheng, Shenal, Hodgson, & Bender, 2009).
HCWs have long relied heavily on surgical masks to provide protection against ATDs; yet, the N95 respirator (not the mask) is the recommended form of protection against these pathogens (Bach, 2017). Masks are loose-fitting and do not provide a tight seal around the face. They have also proved to vary widely in filtration capability ranging from a 4% to 90% penetration of aerosol particles (CDC, 2018; Oberg & Brosseau, 2008). This is why the mask is not considered respiratory protection as they do not provide reliable, adequate protection (Brown, Rogers, Buckheit, & Curran, 2017; OSHA, CDC, & NIOSH, 2015).
Respirators, by contrast, at a minimum cover the nose and mouth and are designed to purify the wearer’s air either by filtering it as the worker inhales or by providing an independent air supply (Shine, Rogers, & Goldfrank, 2009). The N95 filtering face piece respirator filters out 95% of aerosol particles and should be fitted to the wearer to achieve efficacy (Colton & Townsend, 2013). The respirator when worn by the HCW is to protect the wearer by decreasing the concentration of infectious particles in the air inhaled by the wearer from sneezing, coughing, and so on and from particles generated from medical procedures such as bronchoscopies (Brown, Rogers, Buckheit, & Curran, 2017; OSHA, CDC, & NIOSH, 2015).
Responsibilities are incumbent on the HCW to adhere to proper hand and respiratory hygiene practices and appropriate PPE. Unfortunately, evidence for compliance by HCWs indicates that these measures are significantly underused, as are most types of PPE (IOM, 2008). For example, Daugherty et al. (2009) reported on a study in two Baltimore hospitals where 40% of HCWs reported noncompliance with wearing PPE when exposed to influenza and 53% of HCWs observed nonadherence to PPE use by coworkers. These are findings supported by other studies with similar results (Bien, Gillespie, Betcher, Thrasher, & Mingerink, 2016; NIOSH, 2015). Many factors, such as lack of time, lack of ready access to equipment, concerns about interference with patient care, and problems with comfort have been identified as contributing to noncompliance.
In 2011, a NIOSH-supported respiratory protection project was completed in 21 North Carolina acute care hospital facilities involving more than 400 HCWs (Rogers, Buckheit, & Alfano-Sobsey, 2011). This project was designed to evaluate knowledge about, and observe the use of, respiratory protection among HCWs. Although many positive findings were reported, several deficiencies were noted in practice and policy between HCWs, unit managers, and hospital managers. For example, 95% of unit and hospital managers indicated there was a written respiratory protection; whereas, nearly 25% of HCWs were unaware of a policy. In addition, 45% of HCWs, 62% of unit managers, and 38% of hospital managers believed a surgical mask was sufficient when performing an aerosol-generated procedure on patients with influenza. Furthermore, in observing 69 HCWs, one third incorrectly positioned the respirator straps, donned and doffed, and disposed of the respirator, and only about 25% performed seal checks. These findings are consistent with those reported by other investigators previously described and supports the findings that knowledge about when, how, and what types of respiratory protection are needed by HCWs remains a serious concern (Peterson, Novak, Stradtman, Wilson, & Couzens, 2015).
Program Description
In an effort to improve knowledge and practice about respiratory protection against respiratory infectious agents, a NIOSH-funded project that included an educational program, observations of HCWs, and focus groups was conducted at the University of North Carolina (UNC) among hospital personnel in a sample of North Carolina hospitals (Rogers, Buckheit, Ostendorf, & Alfano-Sobsey, 2013). The project goals were to (a) develop, implement, and evaluate an educational program for HCWs and management to include core elements for respiratory protection; (b) identify respiratory protection practice issues among HCWs and strategies for integration of respiratory protection standards and procedures into practice; and (c) develop respiratory protection competencies.
Procedures
Hospital Selection
Of the 21 North Carolina hospitals that participated in the 2011 respiratory protection project (Rogers et al., 2011), 10 were randomly selected to participate in this project based on hospital size (small vs. large) and location (rural/suburban vs. urban). A letter of invitation was sent to each hospital employee health director which described the project purpose and goals, and that participation would include attendance at a 1-day educational program on respiratory protection, identification of volunteers as “practice champions” at each hospital, and an opportunity to participate in focus groups held at each hospital facility. Six hospitals agreed to participate.
Educational Program
For each hospital, hospital contacts were asked to send up to eight participants to attend a 1-day respiratory protection education program at UNC. The purpose of the program was to provide information on respiratory protection for HCWs including infectious agent transmission routes, hand hygiene, hazard assessment, respirator selection and care, medical evaluation and monitoring, fit-testing and training, respirator donning/doffing and seal checks with return demonstration, appropriate strategies for effective respiratory protection implementation in practice, and program evaluation. Materials developed for the program were derived from a review of the relevant literature, examination of North Carolina influenza data, the NIOSH Hospital Respiratory Protection Program Toolkit (OSHA, CDC, & NIOSH, 2015), OSHA Respiratory Protection Standard (OSHA Respiratory Protection Standard 29 CFR 1910.134), and the Institute of Medicine Letter Report: Occupational Health Nurses and Respiratory Protection: Improving Education and Training (Clever, Rogers, Schultz, & Liverman, 2011).
Hospital contacts were asked to invite a diverse group of hospital employees to attend the meeting that included nurses, respiratory therapists, certified nursing assistants, industrial hygienists, safety and occupational health professionals, infection preventionists, and others identified with respiratory protection practice, and who represented an array of hospital areas such as the emergency department (ED), intensive care units, pediatric units, medical-surgical units, occupational health, and other units that typically require the use respiratory protection.
To assess knowledge pre and post the educational program, a pre-/posttest (same questions) was developed and pilot tested that included nine questions about respiratory protection with multiple choice responses. Participants completed the pretest prior to the start of the educational program and the post-test at the completion.
Practice Champions
Letters sent to hospital contacts included information on the recruitment and potential identification of volunteers to act as “practice champions” who would need to know about the hospital’s respiratory protection program (RPP). Volunteering practice champions were asked to have basic knowledge about respiratory protection including ATDs, transmission routes, approaches needed to minimize exposure; when a respirator should be used and differences between facemasks and respirators; and donning/doffing, seal check, and fit-test procedures. All potential practice champions attended the educational program, received practice champion guidelines for participation, and participated in a group discussion on the role of the practice champion immediately post the education program. Twelve practice champions from the six project hospitals received the educational program training and volunteered to participate as practice champions at their respective hospitals. Two practice champions each were from four hospitals, three from one hospital, and one from the sixth hospital.
The assignment for the practice champions was to make “spot” observations and contacts with HCWs who used respiratory protection, and to encourage good practice, answer questions about respiratory protection, which could be by an individual or discussed in a group, identify situations needed for work practice improvement or correction, and make referrals such as for a re-fit-test. All contacts made were documented as observations then recorded on a template checklist/log that included the date/location of incident (e.g., patient room); brief description of incident, observation, or guidance request (e.g., improper donning/doffing) and resolution action/intervention; referral needed to whom/why (e.g., re-fit-test); and follow-up provided.
Over the course of about 8 weeks, the practice champions documented observations of individual HCWs who used respiratory protection. If no respiratory precautions were in use, the practice champion approached a random worker and asked questions about, or observed a demonstration of, that worker’s use of respiratory protection including respirator donning and doffing. Observations were made in the following areas: ED, security, medical intensive care unit (MICU), medical progressive care unit (MPCU), various nursing units, surgery/trauma ICU, pediatric ICU (PICU), neurosurgical ICU, bone marrow transplant unit (BMTU), intermediate surgical care unit (ISCU), main operating room suite, postanesthesia care unit (PACU), burn center, ICU/PCU, registration staff in ED, medical units, employee health (EH), and cafeteria.
Practice champions also provided guidance or education about respiratory protection to groups of workers. Some of the practice champions counted a group as one observation instead of the actual number of individuals who were involved in the observation/discussion. As an example, a departmental meeting of 15 employees might have been identified as one encounter instead of 15 encounters. Other practice champions counted each of the individuals in the group. For this reason, more employees than the documented observations were likely assisted by the practice champions in the project.
Focus Groups
After completion of the educational program, focus groups were held in each hospital with each lasting 1 to 1.5 hours. Group members were introduced, ground rules discussed, and each session had the same five discussion areas about knowledge of the institution’s RPP, training in respiratory protection, care of respirators, recommendations for improvements, and competencies for respirator protection.
Results
Pretest/Posttest Summary Analysis
The educational program content provided a varied approach to presenting facts, scenarios, demonstrations, and discussions covering respiratory protection, especially on the use of N95 respirators. Educational program effectiveness was determined using a pre- and posttest administered to 25 of the 26 participants at the end of the 1-day program. The comparative results of each question scored are shown in the Table 1.
Summary Results of the Pre-and Posttest by Question
All pre- and posttest answers were correct for these questions.
Of the 25 participants tested, five (20%) scored 100% on both the pre- and posttests and an additional 10 (40%) raised their scores to 100% on the posttest, yielding 15 (60%) participants with perfect posttest scores. Although not achieving a score of 100%, two additional respondents scored higher on the posttest, bringing the total of higher scoring participants on the posttest to 12 (48%). Three respondents (12%) scored lower by one question in the posttest and all three incorrect answers were for a different question. Overall, 17 (68%) participants received either a higher or perfect score on the posttest.
Practice Champions’ Observations
There were 216 documented incident observations of individuals and worker groups that resulted in 253 actions or resolutions by the practice champions. These actions included guidance and training about respiratory protection for respirator users who were not in compliance with respiratory protection policies or procedures, and referrals were made to the occupational/employee health department for assistance or appropriate service.
Based on the type and severity of the recorded incident, a resolution was implemented, which was an action or intervention initiated by the practice champion intended to correct the issue observed such as proper storage of the respirator. Although this resolution may have been all the correction needed, some of the incidents observed required follow-up by the practice champions or referrals to other departments or individuals best-suited to ensure that the respirator wearer incorporated the recommended resolution(s).
Incident Location, Observation, and Description
As shown in Table 2, practice champions recorded 216 respiratory protection observations/incidents of nurses, doctors, nursing assistants, care/case managers, environmental health workers, and respiratory therapists in patient rooms on the units, and during staff meetings including improper respirator usage, fit-testing issues, and training and policy issues needing attention or discussion. There were 163 (75%) observations for improper use of respirators. Incorrect donning and doffing (n = 70, 43%) were the most frequently documented observations, followed by no seal check (n = 22, 14%), and improper strap placement (n = 20, 12%). Ten male workers with facial hair wore the N95, which is contraindicated.
Observations/Incidents for Respiratory Protection Made by Practice Champions
Note. PAPR = powered air purifying respirators.
Thirty fit-testing issues were documented as 14% of all observations reported. These included new employee initial fit-testing that had never been done, employees never completing annual fit-testing, and repeat fit-testing for problems wearing the assigned respirators and failed fit-test with two employees requiring powered air purifying respirators (PAPRs).
Issues related to training and policy review resulted from 23 observations (11%) including workers needing overall updated training on respiratory protection, fit-testing requirements, respirator cleaning, storage, and location requirements, the meaning of respiratory protection signage on patient doors, and failure to place the patient on required respiratory protection precautions. Two workers with high blood pressure were instructed to consult with their health care providers regarding their use of respiratory protection.
Resolution
As some observations required more than one action, 253 resolutions were implemented and documented and categorized as training/guidance, and standards and policies. Of the 253 resolutions implemented, training and guidance on the proper use of respirators were provided to 207 (82%) workers including seal checks, strap placement, nosepiece adjustment, improper donning/doffing, disposal/storage, and failure to use the respirator when required. Several workers were referred to infection control/prevention or employee health for additional guidance and discussion of respiratory protection and fit-test requirements. Additional respirator demonstration was given to 25 (10%) workers who used PAPRs and N95s.
Standards and policy discussion was provided to 46 (18%) workers about the OSHA Respiratory Protection Standard and hospital infection control policies including the policy restricting the use of N95 respirators to men with beards because facial hair impedes the seal and effectiveness of the respirator.
Follow-Up
Practice champions decided which respiratory protection incidents required follow-up because they were not immediately remedied or needed additional guidance, instruction, or referrals. Follow-up contact was scheduled with 124 HCWs (n = 76, 61%) of which the majority concerned re-education and training including respirator donning/doffing, strap placement, nosepiece adjustment, seal check, cleaning, storage and disposal, signage, respirator return demonstrations, ATD pathogen exposure, no facial hair with use of N95s, and methods to remember respirator type and size.
Referral/consultation for 26 HCWs to employee health, infection control, and management was made because of respiratory protection noncompliance concerns. In addition, fit-testing follow-up was needed for 22 (18%) HCWs because initial or scheduled repeat fit-tests was not done, repeat fit-tests were needed because of a weight change over 10 pounds, and also for clean-shaven men requesting N95 respirators instead of PAPRs (n = 6).
Focus Groups Results
For the six hospitals, 11 focus groups with 72 participants were conducted (two from five hospitals and one from one hospital). All levels of health care providers including registered nurses, physicians, EMT-P, industrial hygienists, respiratory therapists, phlebotomists, certified nursing assistants, public health epidemiologists, housekeeping staff, and maintenance workers participated in the focus groups. A variety of hospital departments was represented such as corporate health and safety, cardiopulmonary, infection prevention/control, ED, laboratory services, kids immune-suppressed specialty (KISS), medical intensive care, surgery and trauma, nephrology, radiology, angiography, critical paramedic transport (both helicopter and ambulance), pathology, outpatient clinic, and lung transplant services. Five questions were asked during each focus group meeting and a summary of discussions for each focus group question follows.
Can you describe your RPP?
Participants in the focus groups from all hospitals reported there was a written RPP policy online (intranet) and available to employees 24/7. The policy was also available on mobile computers as probability density function (PDF) files in transport trucks and aircraft, so Internet access was not needed. Policy review frequency was uncertain and whether or not employees actually reviewed policies was not tracked. All personnel with respiratory illness exposure to patients, including staff and health care providers, were in the RPP. One hospital even required RNs without respiratory illness exposure to be included in the RPP because he or she may be called to work with patients with respiratory infection in case of disaster situations.
Participants from each hospital described the RPP to include initial education with medical questionnaire and fit-testing as well as an annual centralized computer-based training and hands on fit-testing. Access to obtaining respirators was generally okay. One hospital participant mentioned that there were some barriers to getting PAPRs when needed because of too few PAPRs; however, they were able to “find” one eventually.
Fit-testing methods, both qualitative and quantitative, were described as variable among the hospitals due to Portacount (quantitative) availability, type of respirator (full face respirator vs. N95s), and the department conducting the testing (environmental services or employee health). Generally, questions about the RPP were directed to the employee health nurses, infection control nurses, or to the administrator of the RPP.
The strength of the RPP was that infectious agent exposure was reduced and employees were protected. Program weaknesses identified included difficulty in getting third-shift people tested; monitoring if an employee was out due to the Family Medical Leave Act or an injury, so he or she did not “fall through the cracks”; and being certain that steps in fit-testing were not omitted.
2. Can you describe how you get your training and education in the RPP?
All focus group participants indicated that respiratory protection computer-based training modules (intranet) were available to employees 24/7 with initial and annual training and fit-testing required. The annual computer-based training was stated as taking approximately 15 to 30 minutes with a passing posttest score after which a certificate of completion was generated. The actual fit-testing was completed in approximately 15 to 30 minutes. Ramifications for not completing scheduled annual fit-testing and training modules included work suspension, incomplete employee performance evaluation, and lack of pay raises.
3. How do you take care of your respirators?
Discussion about respirator care included three main areas: replacement and disposal of N95s (including Duckbills), cleaning of PAPRs and half-mask elastomerics (e.g., 3M6000s), and storage of respirators.
Replacement and disposal
All focus group participants agreed that the N95s (including Duckbills) were accessible either in patient’s anteroom, on a cart, or by calling materials handling/central supply. There was much uncertainty about reuse and replacement of the respirator and with varied comments within the same focus group. For example, in one focus group comments about respirator replacement included “the respirator should be replaced each time a patient’s room is entered” or “the N95 should only be replaced when soiled, splattered, or wet; otherwise it can be reused for 12 hours with the same patient.” In another focus group, a participant stated that one N95 was used per patient per day but another participant stated, “the policy states that when we are not in a pandemic situation, the N95 should be disposed of every time it is used.” Comments from a third focus group included that the N95 should be “replaced if bent, or after seven days if it is not used much, whether damaged or not.” If the N95 was to be reused, it could be stored in a Ziploc bag (name on it) and stored either on a shelf or in a cabinet in the anteroom.
In all focus groups, it was stated that N95s were disposed of in a trash container. Focus group participants from two hospitals cautioned that N95s should not be carried on the elbow by a strap because “the strap could stretch and the respirator would not fit properly and it might also come in contact with ‘germs’ as it swings on the person’s arm.”
Cleaning
Cleaning of the PAPRs and half-mask elastomerics (e.g., 3M6000s) was inconsistent within and across the hospitals and cleaning responsibility varied with the person who used the respirator, the technical staff, employee health, or environmental services. Participants in all focus groups mentioned that the PAPRs and elastomerics were disinfected by using Super Sani-wipes, CAVI (cardio-ankle vascular index), or bleach wipes. In only one focus group, participants were able to describe the cleaning process, which was specific and included cleaning the outside hood, inside the bouffant hat (or if a hood, thrown away at end of the shift), changing the felt strips, and plugging in the battery at the end of shift if the PAPR was kept on the unit.
Storage
Storage of the respirators varied by hospital and within a hospital itself. N95s and Duckbill respirators were stored on shelves or cabinets in the patient’s anteroom or in the HCW’s locker. PAPRs and 3M6000s were stored in the patient’s anteroom on a shelf or in a cabinet outside of the area, in the storeroom in a plastic tote container or the original “bag” with the user’s name on it, in isolation towers with docking stations, or in central supply.
4. Do you have recommendations for improvement in your RPP?
Focus group participants from all six hospitals stated that because so many policies were introduced initially to new hires and some HCWs use RPP infrequently, a review of the RPP more frequently at least every 6 months after hire would reinforce important policy information.
Other recommendations included, but were not limited to, education of visitors about the enforcement of respiratory protection (suggested developing a handout for visitors); emphasis on seal checks; distribution of at least one PAPR to each floor, if in short supply; spot-checking by practice champions for respiratory protection compliance; movement from qualitative testing to quantitative testing; and vigilance about being proactive regarding signage that PPE is needed (make available in multiple languages). An important comment was that at some hospitals, fit-testers (for new employees) were exposed to saccharine and bitrex, which seem to have created an allergic-type response for staff exposed over time.
5. What knowledge and skills do you think are important for people to have who need to use respirators? In other words, what competencies should HCWs have to properly know about and use respiratory protection?
Focus group participants were specific about the importance of knowing health impact information about exposure to infectious agents such as acid-fast bacteria, postexposure meningitis, chickenpox, and shingles. It was emphasized that all steps of the fit-testing process should be explained so that the employee does not feel frightened or become claustrophobic.
In addition, participants commented about important knowledge, skills, and competencies for respiratory protection, which included the following:
Each employee must take personal responsibility to use respiratory protection properly; otherwise, other workers are placed at risk as respiratory protection can save lives.
Knowledge about biological agents and transmission methods must be reinforced.
Respirators are not interchangeable and fit-testing is done for a specific respirator model and size.
Basic knowledge of donning and doffing with both straps placed properly must be emphasized, or the respirator will not be effective.
Seal checks must be performed every time the respirator is donned and when the employee is moving about, laughing, smiling, and talking a lot or for any other reason when the seal may be broken.
Proper attention must be given to hand hygiene before and after doffing/taking off respirator.
Men with beards who wear N95s are not protected and noncompliant.
Proper care, storage, and maintenance of respirators is needed.
Questions about the RPP must be clarified with the appropriate resource (employee health nurse, infection control nurse, or administrator of RPP).
In all focus groups, participants stated having a practice champion on each unit for respiratory protection was extremely helpful and should be continued.
Competencies for Respiratory Protection
Any worker who has the potential for exposure to respiratory infectious agents should be protected and should have specific competencies to be able to achieve a standard level of protection. As a result of the analysis of focus group data collected and logged observations/incidents, nine competencies for respiratory protection were developed, which cut across all workers who need respiratory protection. These nine competencies were then sent to employee health directors/contacts from 18 of the 21 North Carolina hospitals, who participated in the initial North Carolina respiratory protection study (Rogers et al., 2011), who agreed to evaluate the competencies for respiratory protection importance on a 5-point Likert-type agreement scale (1 = low agreement and 5 = high agreement). The range for competency agreement was from 4.50 to 4.94 indicating high agreement with all nine competency statements. Editorial comments to improve competency statements were incorporated into the final competencies for respiratory protection for HCWs, which are listed in Table 3.
Health Care Worker Competencies in Respiratory Protection
Note. OSHA = Occupational Safety and Health Administration.
Discussion and Recommendations
Many participants were eager to learn more about and improve practice in respiratory protection. Participants rated the educational program very high with pretest/posttest results indicating good achievement of knowledge learned with nearly 70% of participants increasing scores or achieving 100% score on respiratory protection.
HCWs were enthused about becoming practice champions in their health care systems, and they were proved to be a critical resource in addressing practice, compliance, and respiratory protection knowledge. The overall theme of the findings from the practice champions’ activities revolved around the actual function and proper use of the N95 respirator. Employees wearing respirators needed improved or additional education on the actual use of the N95. All aspects of proper donning and doffing were major deficiencies including strap placement, nosepiece adjustment, and seal checks performed before entering the patient’s room, which were often neglected. Some workers had the wrong size N95 and some workers did not understand the difference between masks and respirators and wore surgical masks instead of the N95s. Several male HCWs with facial hair were found using N95s instead of PAPRs. In addition, several users had not been fit-tested initially or were out of date for annual fit-testing requirements. Clearly policy and educational guidance could provide enhanced knowledge about and compliance with respirator usage. As pointed out in OSHA, CDC, & NIOSH’s (2015) respiratory toolkit, it is important to have a written RPP that provides clear policy guidance regarding respirator use and detailed procedures including, for example, fit-testing, donning/doffing and respirator use, and facial hair.
This project raised the opportunity for the practice champions to reeducate and raise awareness of many respirator users as to what was being done correctly and incorrectly, why it was important to have annual fit-testing and education, and how to monitor each other to ensure protection from contaminant exposure through respiratory protection and hygiene practices. There are numerous educational resources available from OSHA and NIOSH describing specific risks and respiratory protection procedures and practices (OSHA, CDC, & NIOSH, 2015). Many practice champions expanded their educational activities from the individual worker who was observed to entire departments/units and medical practice staff and personnel. Referrals were made on an as needed basis after the individual was reeducated on the use of respiratory protection and the review of policies and procedures, which helped to improve work practice, be respirator refit if needed, and to have a better understanding of the policies and their purpose.
From their participation in this project, several of the practice champions shared that there were changes made to the respiratory program at their respective hospitals. This included providing a more detailed education and discussion during fit-testing about proper use procedures, reminding staff when the annual fit-testing and education was due, providing a sticker on the back of the HCW’s name badge about the type and size of respirator approved to wear, conducting spot observations, and providing group education about respiratory protection and hygiene practices. All practice champions indicated this project and the resultant activities were an excellent exercise in raising awareness and providing input into organizational changes for better respiratory protection.
From the focus groups, several common themes emerged. All hospitals had a written RPP policy online (intranet) available to employees 24/7; however, there was generally a lack of policy review. Most hospitals did not have respirator access barriers. Fit-testing methods and procedures and program evaluation varied considerably within and across hospitals, compliance with fit-testing as well as care, maintenance, and storage of the respirator was inconsistent, and physician compliance with respiratory protection was minimal. Development of respiratory protection certification should be considered.
Summary of Recommendations for Respiratory Protection for Health Care Workers
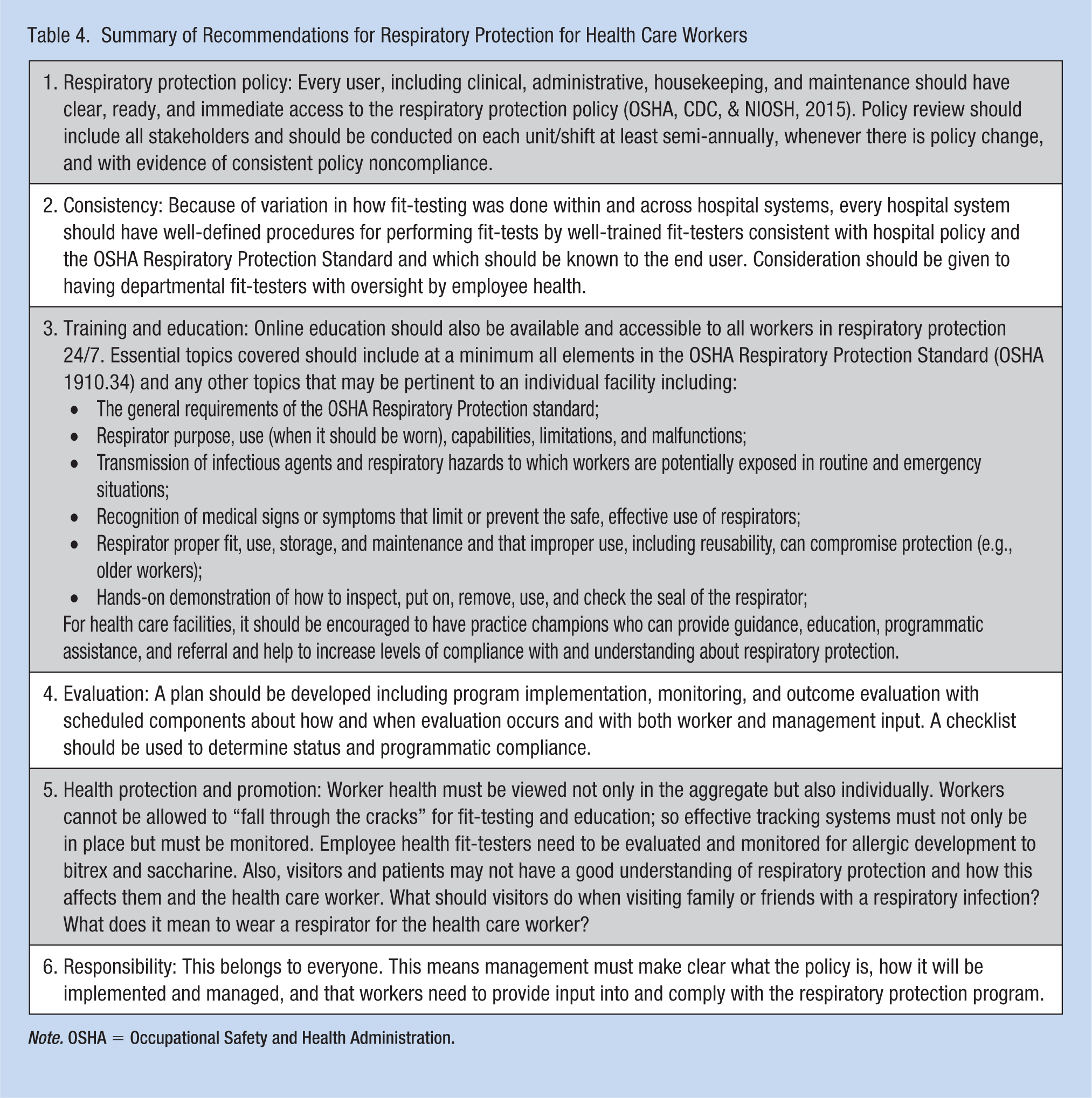
Note. OSHA = Occupational Safety and Health Administration.
Health care facilities need to foster and promote a strong culture of safety that includes a commitment to worker safety, adequate access to safety equipment, and extensive training efforts that utilize protocols requiring specific safety actions and detailing the consequences for noncompliance with PPE use. An organizational culture that supports worker health and safety has been shown to positively affect compliance with safety procedures (Burgel et al., 2014). Every effort should be made to ensure that HCWs wear appropriate PPE and these employees should feel uncomfortable when not wearing PPE during appropriate situations (Clever et al., 2011).
Conclusion
Respiratory protection for HCWs and exposed personnel is an essential component of policy, procedure, and practice. Through the use of a hierarchy of control strategy including implementation of engineering, administrative and work practice controls, and PPE, health care organizations have responsibility to ensure all staff are protected against infectious agents. HCWs and staff need to be fully informed of policies and procedures for respiratory protection, demonstrate respiratory protection competence, and fully implement these procedures into practice.
Applying Research to Practice
Health care workers are potentially at risk of exposure to respiratory infectious agents while providing care to patients and respiratory protection is critical. Effective use of respirators including proper fit-testing, size, and type, and wearing of the respirator including donning and doffing, user seal check, strap placement, and nosepiece fit is needed to ensure adequate respiratory protection. Monitoring for proper respirator use and compliance is essential. Practice champions were used in this project who observed and monitored health care workers while they used respirators. The practice champions provided guidance and referrals when needed to address issues such as education, proper use of the respirator, and cleaning and storage. In this study nine respiratory protection competencies were identified and validated for all health care workers with potential respiratory infectious agent exposure. Occupational health nurses should use these competencies to guide their implementation and maintenance of their respiratory protection program. These competencies are applicable in all high-risk exposure settings.
Footnotes
Acknowledgements
The authors thank the National Personal Protective Technology Laboratory, National Institute for Occupational Safety and Health for funding this project. They also thank Debra Novak, RN, PhD, National Institute for Occupational Safety and Health for scientific support for this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Bonnie Rogers is a professor at the University of North Carolina School of Public Health and the NC Occupational Safety and Health Education and Research Center and has been principal investigator for several NIOSH funded studies on respiratory protection for health care workers.
Kathleen Buckheit has been an occupational health nurse for 32 years in various settings and has worked on three NIOSH respiratory protection research projects. She has held the most recent positions of NC State Occupational Health Nurse Consultant and Director of Outreach and Continuing Education for the North Carolina Education and Research Center at the University of North Carolina, Chapel Hill, NC. She is a currently the Director of Education for the American Association of Occupational Health Nurses (AAOHN).
Judith Ostendorf is adjunct faculty in the Occupational Health Nursing Program at the University of North Carolina School of Public Health, Chapel Hill, NC. She has participated in several research projects on respiratory protection. She is a consultant for Practical Management Inc.