
Abstract
In hospitals, health care workers (HCWs) are exposed to a wide range of respiratory hazards, which requires using respiratory protective equipment and implementing Respiratory Protection Programs (RPPs). The aim of this cross-sectional study was to investigate RPP implementation in 36 teaching hospitals located in the Fars province of Iran. A researcher-developed checklist, including nine components of the RPP standard, was completed by industrial hygienists in the study hospitals. The Fuzzy Analytical Hierarchy Process (FAHP) was used to determine the weight coefficient of RPP components. Finally, a Respiratory Protection Program Index (RPPI) was developed to calculate hospital compliance with RPP. The results showed that RPP were not fully implemented in the studied hospitals, and the highest and lowest RPPI scores were related to training and fit testing, respectively. To promote the implementation of RPP, significant efforts are required for all components, especially fit testing and worker evaluation.
Keywords
Health care settings are high-risk environments where employees are exposed to a wide range of respiratory hazards including bacteria, viruses, fungi, infectious aerosols, and chemical agents (Braun, Tschurtz, Hafiz, & Williams, 2014; Bunyan, Ritchie, Jenkins, & Coia, 2013; Lenhart, Seitz, Trout, & Bollinger, 2004; U.S. Department of Labor, 2015; U.S. Department of Labor, Occupational Safety & Health Administration, 2014). Transfer of these hazards to health care workers (HCWs) occurs via patients, contaminated equipment, and the hospital environment (Amoran, 2013; Delclos et al., 2007; Jahdhami, 2013; Luksamijarulkul, Khumsri, Vatthanasomboon, & Aiumlaor, 2009; Luksamijarulkul, Kiennukul, & Vatthanasomboon, 2014). In recent years, the incidence and prevalence of infectious diseases (e.g., severe acute respiratory syndrome [SARS] and influenza) have increased international concern about the health of HCWs (Lowe & Wilder-Smith, 2005).
In health care settings, respirators may be required to protect employees from exposure to aerosol transmissible diseases (ATD; MacIntyre et al., 2011; Siegel, Rhinehart, Jackson, Chiarello, & the Healthcare Infection Control Practices Advisory Committee, 2007) and other respiratory hazards (e.g., aerosol medications, surgical smoke, and high-level disinfectants; The Joint Commission, 2014). Different types of respirators provide varying degrees of protection and each has specific features, advantages, and disadvantages (Lenhart et al., 2004). Respirators can play an essential role in protecting HCWs from respiratory hazards, especially in situations where other control strategies (i.e., engineering and administrative) are inappropriate or impractical (Hines, Rees, & Pavelchak, 2014).
Occupational Safety and Health Administration (OSHA) standard (29 CFR 1910.134) requires that Respiratory Protection Programs (RPP) be implemented in workplaces where respirators are required to protect the health of employees; RPPs consist of nine components, including evaluation of respiratory hazards; selection of respiratory protective equipment (RPE); medical evaluation; fit testing; training; use of RPE; inspection, cleaning, and maintenance of RPE; program evaluation; and recordkeeping (OSHA, 2015). A limited number of international studies have been conducted regarding implementation of RPP in hospitals. The results of these studies, mainly conducted in the United States, showed that some elements of RPP (e.g., medical evaluation, fit testing, training, and recordkeeping) were not fully implemented according to OSHA standard (Beckman et al., 2013; Peterson, Novak, Stradtman, Wilson, & Couzens, 2015). However, no studies have investigated RPPs in Iranian hospitals. Thus, this study evaluated the implementation of RPPs in hospitals located in the Fars province of Iran.
Methods
This cross-sectional study was conducted on hospitals located in Shiraz, Fars, one of the largest provinces of Iran. Industrial hygienists employed by the hospitals were invited to participate in a 1-day educational workshop that provided information about the elements of RPP and how to complete the audit checklist. From all 61 invited hospitals, 36 hospitals participated in the workshop and completed the checklist. The audit checklist was constructed based on the OSHA RPP standard (29 CFR 1910.134.c); the checklist included evaluation of respiratory hazards (5 items), selection of RPE (11 items), medical evaluation (3 items), fit testing (5 items), maintenance of RPE (6 items), use of respirators (12 items), training (6 items), recordkeeping (3 items), and RPP evaluation (2 items).
RPPI
To create an index and calculate the compliance percentage of each RPP element, each item was scored as 1 (no compliance), 2 (partial compliance), or 3 scores (full compliance). Items that were not applicable to a particular condition were marked not applicable (NA). For example, if fit test was not performed in the hospitals, other subitems of the fit test were marked as NA. The content validity of the checklist was confirmed by three experts in occupational safety and health (two PhD holders and an MSc in occupational health with at least 5 years’ work experience).
Calculation of the RPP indices was conducted by the first author. The degree of compliance was computed for each element of the RPP as follows:

where RPPI i is the Respiratory Protection Program Index for each element, Xi is the score of each item, and n is the number of items in each element of the RPE.
The overall Respiratory Protection Program Index (RPPI T ) was created to calculate the percentage of provided RPE in the study hospitals:

where RPPI i is the degree of compliance for each RPP element and Wi is the Fuzzy Analytical Hierarchy Process (FAHP) weight coefficient for each RPP element. The RPPI was graded using the following scale: very poor (<25%); good (25% to <50%), moderate (50% to <75%), and poor (75% to 100%). These categories were applied to judge provided RPE in the study hospitals. All the calculations used Excel software.
Calculating the FAHP Weight Coefficient
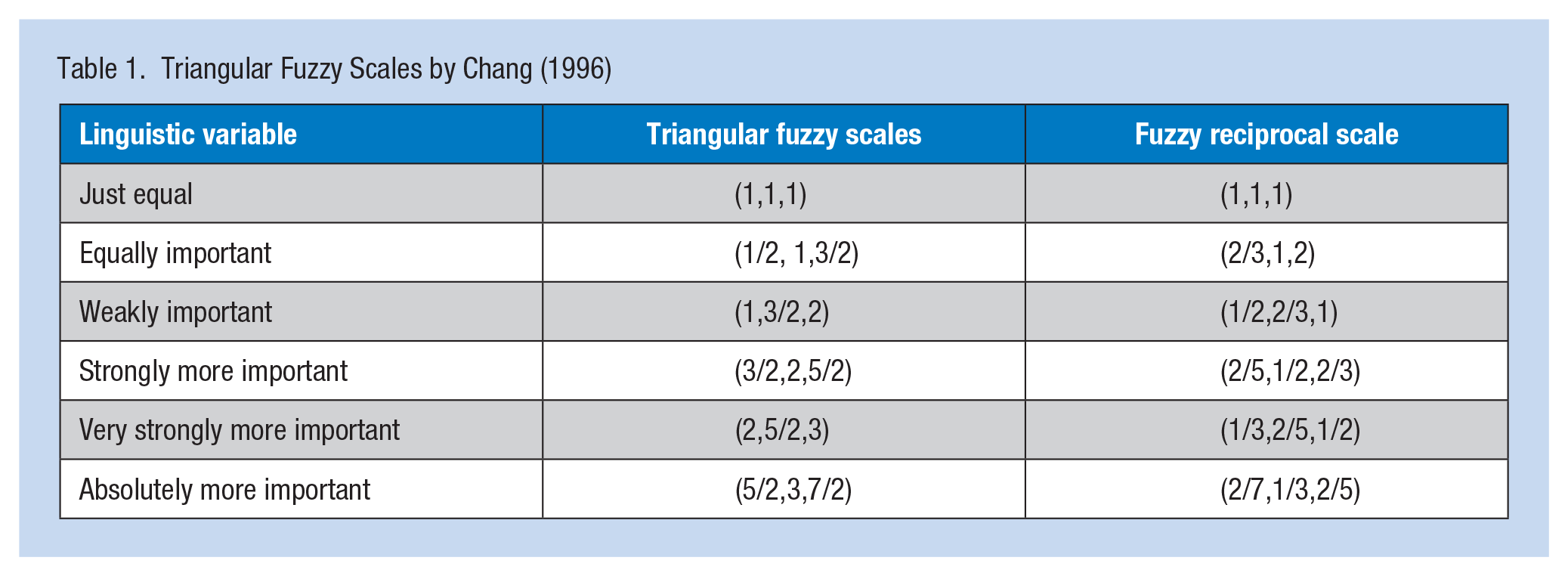
The FAHP technique uses approximate and uncertainty information for decision-making (Kahraman, Cebeci, & Ruan, 2004; Lee, Chen, & Chang, 2008).In this study, weight coefficients for the RPP components were calculated using FAHP, adjusting the RPP components for a pair wise comparison. Fifteen occupational safety and health experts used the FAHP questionnaire to compare each RPP element pair by degree of importance based on linguistic expressions (Table 1; Chang, 1996).Verbal phrases were converted to triangular fuzzy numbers. To determine the reliability of the FAHP questionnaire, the consistency ratio was calculated using Equations 3 and 4 where CI, λmax, RI, and n represent a consistency index, largest special value for paired comparisons matrix, a random index, and the number of compared cases, respectively. A consistency ratio less than 0.1 was considered acceptable (Saaty, 1990).

Triangular Fuzzy Scales by Chang (1996)
Chang’s Extent FAHP
Several analytical hierarchy process methods have been presented based on triangular fuzzy numbers (Erensal, Oncan, & Demircan, 2006). Triangular fuzzy numbers are a type of fuzzy numbers whose membership function is defined by three real numbers (l, m, u) mathematically (Cox, 1995):
After completing the FAHP, the weight of each RPP component was calculated using Chang’s extent analytic hierarchy process (Chang, 1996): Calculating the value of fuzzy synthetic extent according to the ith object,
where gi (i = 1,2,3,…,n) and
Calculating the degree of possibility of M2 = (l2,m2,u2) ≥ M1 = (l1,m1,u1),

where x and y are values in the membership function of each criterion. This statement can be written as follows:
Calculating the degree of possibility of being greater,
Calculating the weight vector,

Calculating the normalized weight,

Results
Most of the hospitals were general (83.3%), government (58.3%), and large in size (58.2%). No significant relationships were found between the RPPI and general characteristics of the hospitals, such as type, ownership, or size (p > .05; Table 2). The consistency index was calculated to be less than 0.1 for the central number (m) and geometric mean of the high and low (g) matrixes (0.037 and 0.014, respectively).Therefore, the experts’ opinions had the required convergence and the final pairwise comparison matrixes were compatible. A sample of calculations to determine the FAHP weight coefficient for the components of RPE selection has been presented below:
Fuzzy values:
FAHP weights:
General Characteristics of the Studied Hospitals and Their Relationship With the Respiratory Protection Program Index
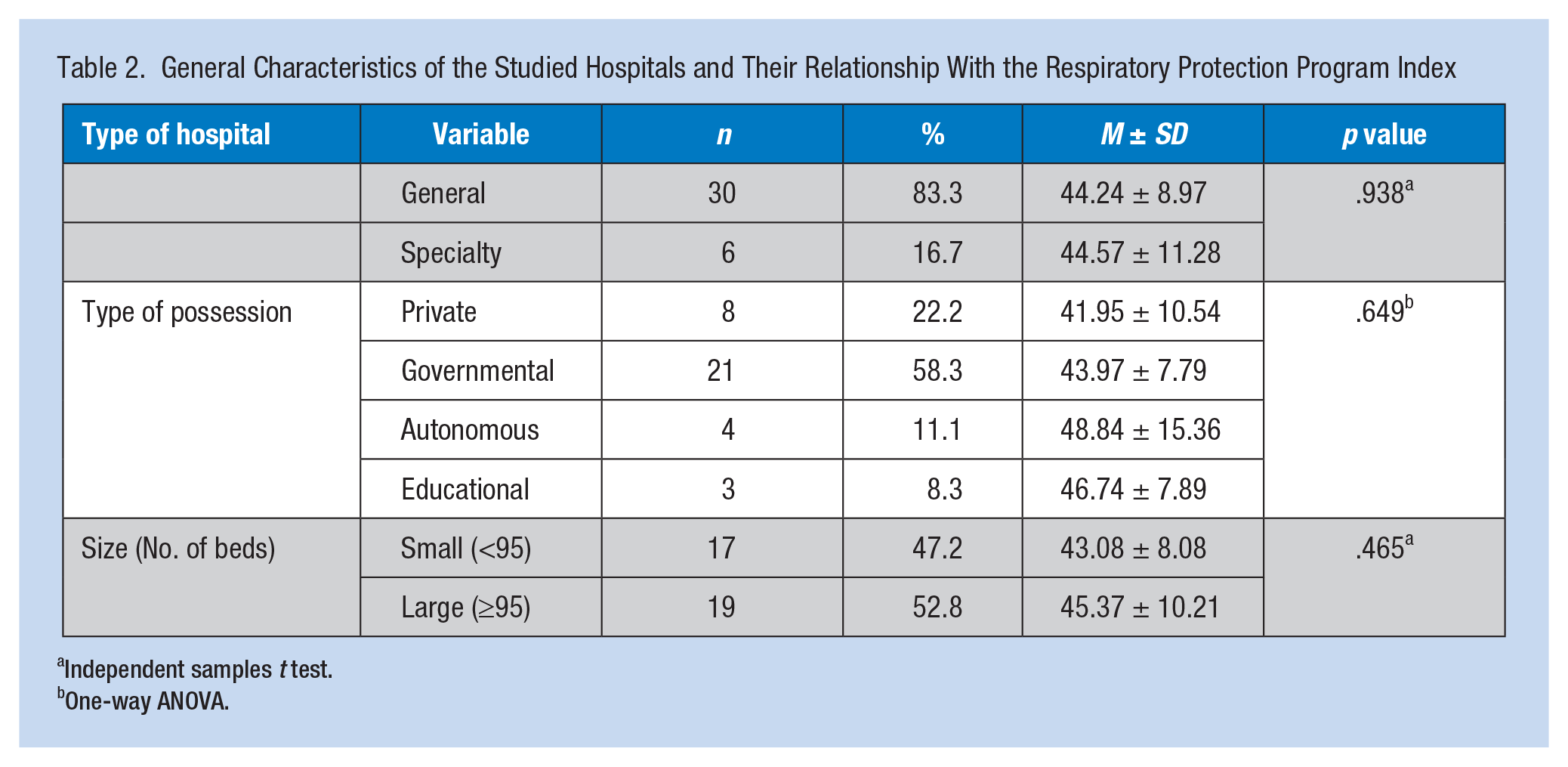
Independent samples t test.
One-way ANOVA.
The weight of each RPP component and their rank is shown in Table 3. Accordingly, the highest and lowest FAHP weight coefficients were related to the evaluation of respiratory hazards and recordkeeping, respectively. The mean and standard deviation of the RPPI and the distribution of RPPI scores in various dimensions are presented in Table 4. As the table depicts, the highest and lowest RPPI scores were related to training (67.27 ± 21.44%) and fit testing (6.66 ± 0%), respectively. The mean value of RPPI among the studied hospitals was 44.29 ± 9.21%, which was classified as poor. The degree of RPP implementation was also poor in most of the hospitals (77.8%). Only 22.2% of hospitals were classified as medium in terms of RPP implementation. Detailed RPPI results for all checklist components are in the Appendix.
FAHP Weight Coefficients of RPP Dimensions
Note. FAHP = Fuzzy Analytical Hierarchy Process; RPP = Respiratory Protection Programs; RPE = respiratory protective equipment.
Results of the Respiratory Protection Program Index in the Studied Hospitals (n = 36)
Note. RPP = Respiratory Protection Programs; RPE = respiratory protective equipment; RPPI = Respiratory Protection Programs Index.
Discussion
This study assessed the extent to which RPP was implemented in hospitals located in Fars province, Iran. The mean value of RPPI was 44.29 ± 9.21% in the studied hospitals. Therefore, RPP was not fully implemented in any of the hospitals, and most of them (75%) were classified as poor. This is similar to the findings of Sietsema, Conroy, and Brosseau (2015), which showed that the mean score of RPP was 46% and 44% in Minnesota and Illinois hospitals, respectively.
In most of the studied Iranian hospitals, no individuals were responsible for the full implementation of their RPPs. Some parts of the program (e.g., selection of RPE) had been assigned to the Infection Control Committee, but the committees had not received sufficient training to competently oversee the program. Furthermore, insufficient budgets were allocated for providing fit testing and suitable respirators for identified respiratory hazards.
The RPP dimensions were ranked in order of importance as follows: evaluation of respiratory hazards, training, fit testing, program evaluation, use of respirators, selection of RPE, medical evaluation, maintenance of RPE, and recordkeeping. Based on the FAHP analysis, the highest and lowest RPP importance weights were related to evaluation of respiratory hazards (0.0145) and recordkeeping (0.071), respectively. However, the highest and lowest compliance scores of the RPPI were related to training (67.27 ± 21.44%) and fit testing (6.66 ± 0%), respectively. Evaluation of respiratory hazards (chemical or biological agents) is necessary to ascertain the need for and appropriate type of RPE. Although this dimension had the highest FAHP importance weight among all RPP dimension, only 2% of the study hospitals were good in terms of evaluating respiratory hazards. This finding was lower than the values reported in the study by Brosseau, Conroy, Sietsema, Cline, and Durski (2015; Minnesota (47%) and Illinois (23%) hospitals) and the Peterson et al. (2015) study conducted in 98 hospitals located in six U.S. states (89.4%).
In the present study, the highest compliance score for RPE elements was related to training, which was the second priority established by the FAHP. This finding was comparable to U.S. studies (Brosseau et al., 2015; Peterson et al., 2015; Siegel et al., 2007). In this study, hospitals were weak in fit testing, donning and doffing respirators, and annual retraining programs following changes in workplace conditions. Respirator fit testing was ranked as the third priority among the RPP elements; however, fit testing was not implemented in any of the study hospitals. Only one model and size (medium) of respirator was provided for all employees. In contrast, fit testing was reported in 60% to 83% of U.S. hospitals including hospitals in Minnesota (Brosseau et al., 2015), California (Beckman et al., 2013), and New York (Siegel et al., 2007).
After fit testing, medical evaluation had the lowest compliance score for RPE elements. According to OSHA RPP standard (29 CFR 1910.134), the respirators can make breathing more difficult and not everyone is able to wear a respirator due to health conditions including heart conditions, lung disease, and psychological conditions like claustrophobia. Therefore, before using or fit testing a respirator, users must be medically evaluated to ensure their ability to wear respirators. However, medical evaluations for respirator users were not conducted in any of the studied hospitals.
Study Limitations
The most significant limitation of this study regarded data collection. All data were self-reported by occupational safety and health experts employed by the study hospitals. These data could have been affected by a social desirability bias.
Conclusion
Effective protection of HCWs from respiratory hazards requires the full implementation of RPP in hospitals. This program must include evaluation of respiratory hazards, appropriate selection and maintenance of respirators, medical evaluation, fit testing, employee training, recordkeeping, and program evaluation. However, the least implemented RPP components were fit testing and medical evaluation.
Applying Research to Practice
Health care workers (HCWs) are exposed to a wide range of respiratory hazards. Effective protection of HCWs from these hazards requires the full implementation of respiratory protection programs (RPP) in the hospitals. Compliance studies of RPP in hospitals using the Respiratory Protection Program Index (RPPI) and tools such as Fuzzy Analytical Hierarchy Process (FAHP) can be adapted to discover gaps and elements which require significant promotion in hospitals and health care centers.
Footnotes
Appendix
The Results of the Completed Checklist for Evaluating Respiratory Protection Programs in the Studied Hospitals
| Program element, items | Y |
N |
P |
NA |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | |
| Evaluation of respiratory hazards | ||||
| 1. Respiratory hazards in the hospital (including chemical and infectious agents) are identified for determining the need for respiratory protective equipment (RPE). | 7 (19.4) | 4 (11.1) | 25 (69.4) | 0 (0) |
| 2. Respiratory hazards are evaluated periodically or after any change in workplace conditions. | 3 (8.3) | 21 (58.3) | 12 (33.3) | 0 (0) |
| 3. Physicians, students, volunteers, or others who are not hospital employees and are reasonably anticipated to be exposed to aerosol transmissible disease (ATD) pathogens are considered in risk evaluation. | 11 (30.6) | 19 (52.8) | 6 (16.7) | 0 (0) |
| 4. Airborne concentrations of chemicals are measured to determine the level of respiratory protection needed to reduce exposures to acceptable levels. | 3 (8.3) | 29 (80.6) | 4 (11.1) | 0 (0) |
| 5. First receiver of victims exposed to unknown radiological, biological, or chemical agents is considered in risk evaluation | 5 (13.9) | 25 (69.4) | 6 (16.7) | 0 (0) |
| Selection of respiratory protective equipment | ||||
| 1. For performing activities, such as bronchoscopy, in which infectious particles are produced in the form of aerosol, at least N95 respirators are selected. | 19 (52.8) | 13 (36.1) | 4 (11.1) | 0 (0) |
| 2. For contact with patients with diseases, such as seasonal flu, severe acute respiratory syndrome (SARS) and tuberculosis, N95 respirators are selected. | 23 (63.9) | 10 (27.8) | 3 (8.3) | 0 (0) |
| 3. Surgical N95 respirators are selected for operating or sterile rooms. | 1 (2.8) | 35 (97.2) | 0 (0) | 0 (0) |
| 4. For the first receivers who might be exposed to unknown substances, such as chemical, biological, radiological, and nuclear substances, powered air-purifying respirators (PAPR) with a full face piece, hood, or helmet and combination of HEPA filter and chemical cartridge with APF 1000 are selected. | 0 (0) | 36 (100) | 0 (0) | 0 (0) |
| 5. For coping with respiratory hazards, including gases and vapors that may come from procedures using hazardous drugs (including some cancer chemotherapy, hormones, and bioengineered drugs) and chemicals (e.g., anesthetic waste gases or equipment sterilization), the respirators with cartridges are used. | 10 (27.8) | 26 (72.2) | 0 (0) | 0 (0) |
| 6. The results of respiratory hazards evaluation and workplace conditions are considered for RPE selection. | 4 (11.1) | 11 (30.6) | 21 (58.3) | 0 (0) |
| 7. Physical and chemical nature of contaminants is considered in RPE selection. | 8 (22.2) | 26 (72.2) | 2 (5.6) | 0 (0) |
| 8. NIOSH-certificated respirators are used in compliance with the conditions of their certification. | 16 (44.4) | 13 (36.1) | 7 (19.4) | 0 (0) |
| 9. User comments are considered in RPE selection (or when selecting several respirators with different models and sizes available to users). | 11 (30.6) | 16 (44.4) | 9 (25) | 0 (0) |
| 10. At least N95 respirators are used for entering the rooms of the patients with tuberculosis. | 17 (47.2) | 13 (36.1) | 6 (16.7) | 0 (0) |
| 11. For workers who are unable to use negative pressure respirators, PAPR is used. | 0 (0) | 36 (100) | 0 (0) | 0 (0) |
| Medical evaluation | ||||
| 1. Medical evaluation is conducted for the employees before fit testing and demonstrating the need for using respirators in the workplace. | 0 (0) | 36 (100) | 0 (0) | 0 (0) |
| 2. Medical evaluation is repeated after changes in the employees’ health status (asthma, breathing difficulty) or changes in job conditions. | 0 (0) | 0 (0) | 0 (0) | 36 (100) |
| 3. The following information is given to the physician before medical evaluation: type and weight of the respirator, duration and frequency of respirator use, physical work effort, and a copy of the written respiratory protection program (RPP). | 0 (0) | 0 (0) | 0 (0) | 36 (100) |
| Fit testing | ||||
| 1. Fit testing is provided for employees prior to initial use of tight-fitting face piece respirators. | 0 (0) | 36 (100) | 0 (0) | 0 (0) |
| 2. Fit testing is required at least annually. | 0 (0) | 0 (0) | 0 (0) | 36 (100) |
| 3. If employees fail fit testing of negative pressure respirators, PAPR respirators are used. | 0 (0) | 0 (0) | 0 (0) | 36 (100) |
| 4. The results of fit testing are given to the employees so they know the model and size of respirators they should use. | 0 (0) | 0 (0) | 0 (0) | 36 (100) |
| 5. Fit testing is repeated after any changes in employees’ physical conditions that could affect the respirator’s fit (such as facial scarring, cosmetic surgery, dental changes, or an obvious change in body weight) or changes in the type of respirator required. | 0 (0) | 0 (0) | 0 (0) | 36 (100) |
| Maintenance of respiratory protective equipment | ||||
| 1. RPE is inspected periodically and before each use. | 13 (36.1) | 15 (41.7) | 8 (22.2) | 0 (0) |
| 2. Personal respirators are always cleaned, disinfected, and kept sanitary. | 19 (52.8) | 6 (16.7) | 11 (30.6) | 0 (0) |
| 3. Common RPE for emergencies are cleaned and disinfected before and after each use. | 10 (27.8) | 15 (41.7) | 11 (30.6) | 0 (0) |
| 4. Respirators are stored properly and protected from contamination, dust, sunlight, extreme temperatures, extreme moisture, damaging chemicals, and deformation. | 20 (55.6) | 8 (22.2) | 8 (22.2) | 0 (0) |
| 5. Filter, cartridge, and canisters are labeled and color-coded with the NIOSH approval label; the label is not removed and remains legible. | 5 (13.9) | 3 (8.3) | 1 (2.8) | 27 (75) |
| 6. A change schedule has been developed for respirator cartridges. | 3 (8.3) | 5 (13.9) | 1 (2.8) | 27 (75) |
| Use of respirators | ||||
| 1. Individuals who have facial hair use PAPR for respiratory protection. | 0 (0) | 36 (100) | 0 (0) | 0 (0) |
| 2. Personnel replace their respirators when problems occur, such as difficulty breathing, leakage, or saturation of the filter with material. | 14 (38.9) | 14 (38.9) | 8 (22.2) | 0 (0) |
| 3. Respirators are applied after gowning and before goggles and gloves are applied. | 24 (66.7) | 5 (13.9) | 7 (19.4) | 0 (0) |
| 4. When respirators are worn, the top strap is placed at the top back of the head and the bottom strap is placed below the ears near the neck. | 26 (72.2) | 4 (11.1) | 6 (16.7) | 0 (0) |
| 5. When employees are at risk of pathogenic droplets from patients’ nose and mouth, respirators with minimum respiratory protection (surgical mask) are used. | 27 (75) | 5 (13.9) | 4 (11.1) | 0 (0) |
| 6. User seal is checked before each use of respirators. | 4 (11.1) | 27 (75) | 5 (13.9) | 0 (0) |
| 7. Respirators are removed after other PPE. | 18 (50) | 10 (27.8) | 8 (22.2) | 0 (0) |
| 8. During respirator doffing, hands are not contaminated. | 17 (47.2) | 5 (13.9) | 14 (38.9) | 0 (0) |
| 9. Respirators are removed outside the patient’s room and after closing the door. | 21 (58.3) | 4 (11.1) | 11 (30.6) | 0 (0) |
| 10. After doffing respirators, hands are washed with alcohol-based disinfectants. | 17 (47.2) | 4 (11.1) | 15 (41.7) | 0 (0) |
| 11. Users of tight-fitting respirators must not have conditions, such as facial hair, that disturb respirator fitting and the action of the air valves. | 9 (25) | 12 (33.3) | 15 (41.7) | 0 (0) |
| 12. Eyeglasses, goggles, and other protective equipment should not interfere with respirator fit or action of the air valves. | 11 (30.6) | 16 (44.4) | 9 (25) | 0 (0) |
| Training | ||||
| 1. Individuals are trained about the limitations and applications of their respirators. | 14 (38.9) | 6 (16.7) | 16 (44.4) | 0 (0) |
| 2. Employees are trained about all the elements of RPP. | 15 (41.7) | 10 (27.8) | 11 (30.6) | 0 (0) |
| 3. Employees are trained about the user seal check (positive and negative pressure test) for tight-fitting respirators. | 7 (1 9.4) | 23 (63.9) | 6 (16.7) | 0 (0) |
| 4. Individuals are trained to correctly don and doff the respirators. | 14 (38.9) | 12 (33.3) | 10 (27.8) | 0 (0) |
| 5. Individuals are trained about the sequence of donning and doffing the PPE. | 17 (47.2) | 10 (27.8) | 9 (25) | 0 (0) |
| 6. Retraining is required annually and after change in work conditions. | 11 (30.6) | 12 (33.3) | 13 (36.1) | 0 (0) |
| Recordkeeping | ||||
| 1. Records of fit testing are kept in the hospital. | 0 (0) | 0 (0) | 0 (0) | 36 (100) |
| 2. Records of medical evaluation are kept in the hospital. | 0 (0) | 0 (0) | 0 (0) | 36 (100) |
| 3. Records of the evaluation of respiratory hazards are kept in the hospital. | 6 (16.7) | 21 (58.3) | 5 (13.9) | 4 (11.1) |
| Program evaluation | ||||
| 1. RPP is monitored periodically. | 4 (11.1) | 25 (69.4) | 7 (19.4) | 0 (0) |
| 2. Identified problems and deficiencies are included in the monitoring process. | 6 (16.7) | 21 (58.3) | 9 (25) | 0 (0) |
Note. Y = yes; N = no; P = partial; NA = not applicable; NIOSH = National Institute for Occupational Safety and Health; HEPA = high-efficiency particulate air; APF = Assigned Protection Factor; PPE = personal protective equipment.
Acknowledgements
The authors thank all the occupational safety and health specialists employed in Shiraz University of Medical Sciences hospitals for their assistance in conducting this project. They also thank Ms. A. Keivanshekouh at the Research Improvement Center of Shiraz University of Medical Sciences for editing the manuscript.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from Shiraz University of Medical Sciences, Shiraz, Iran (Grant 94-01-04-10307).
Author Biographies
Marzieh Honarbakhsh is MSc student of occupational health at Shiraz University of Medical sciences, Shiraz, Iran. She is completing her master’s thesis, focused on respiratory protection in hospitals and health centers.
Mehdi Jahangiri is associate professor in Occupational Health Department at Shiraz University of Medical Sciences, Shiraz, Iran. He conducts research focused on the safety and health of health care workers.
Haleh Ghaem is assistant professor in the Research Center for Health Sciences and Epidemiology Department at the School of Health, Shiraz University of Medical Sciences, Shiraz, Iran.
Payam Farhadi is a faculty member in the Department of Management, Zand Higher Education Institute Iran, Shiraz, Iran. He conducts research in the field of operations research.