
Abstract
Background:
Reusable elastomeric half-mask respirators (EHMR) are an alternative to address shortages of disposable respirators. While respirator discomfort has been noted as a barrier to adherence to wearing an N95 filtering facepiece respirator (FFR) among health care personnel (HCP), few have examined EHMR comfort while providing patient care, which was the purpose of this study.
Method:
Among a cohort of 183 HCP, we prospectively examined how HCP rated EHMR tolerability using the Respirator Comfort, Wearing Experience, and Function Instrument (R-COMFI) questionnaire at Study Week 2 and Week 10. At the completion of the study (Week-12), HCP compared EHMR comfort with their prior N95 FFR use. Overall R-COMFI scores and three subscales (comfort, wear experience, and function) were examined as well as individual item scores.
Findings:
The HCP reported an improved overall R-COMFI score (lower score more favorable, 30.0 vs. 28.7/47, respectively) from Week 2 to Week 10. Many individual item scores improved or remained low over this period, except difficulty communicating with patients and coworkers. The overall R-COMFI scores for the EHMR were more favorable than for the N95 FFR (33.7 vs. 37.4, respectively), with a large proportion of workers indicating their perception that EHMR fit better, provided better protection, and they preferred to wear it in pandemic conditions compared with the N95 FFR.
Conclusion/Application to Practice:
Findings suggest that the EHMR is a feasible respiratory protection device with respect to tolerance. EHMRs can be considered as a possible alternative to the N95 FFR in the health care setting. Future work is needed in the EHMR design to improve communication.
Keywords
Background
Respiratory protection safeguards health care personnel (HCP) from exposure to infectious aerosol transmissible pathogens and is a critical component of infection control strategies in health care settings (Occupational Safety and Health Administration, 2011). The primary respiratory protection used in medical settings is the NIOSH Approved® N95® filtering facepiece respirator (N95 FFR; Wizner et al., 2016); however, hospitals faced significant challenges during the COVID-19 pandemic caused by the SARS-CoV-2 virus with shortages (Ahmed et al., 2020; Auerbach et al., 2021), leaving HCP vulnerable to exposure to infectious pathogens. In recent years, the elastomeric half-mask respirator (EHMR) has been proposed as one alternative to the N95 FFR (Baracco et al., 2015; Centers for Disease Control and Prevention, 2020; de Perio et al., 2020). EHMRs are half-face, tight-fitting respirators that are made of synthetic or rubber material and are equipped with replaceable filters or cartridges, and they have the same assigned protection factor (APF) as the N95 FFR (Centers for Disease Control and Prevention, 2020). One advantage over the N95 FFR is that the EHMR can be repeatedly disinfected, cleaned and reused. To date, literature in this area remains sparse, with very few studies having examined EHMR use in health care (Ciconte & Danyluk, 2013; Hines et al., 2019a, 2019b). Prior studies suggest that discomfort was a barrier to HCP’s adherence to wearing the N95 FFR (Locatelli et al., 2014), with limited findings about how the EHMR has been rated (Hines et al., 2019b; Radonovich et al., 2009). The purpose of this study was to examine HCP’s level of comfort while wearing the EHMR when providing patient care and to compare comfort ratings between the EHMR and N95 FFR.
Methods
We conducted a 12-week prospective cohort study at two Level-1 trauma centers in Georgia (GA) and Texas (TX) from September through December 2021. Workers were fit-tested and trained to wear an EHMR, which they were asked to wear over a 12-week time period in lieu of their assigned N95 FFR. More specifically, they were trained to wear their EHMR when respiratory protection was warranted (e.g., patients with known aerosol transmissible diseases). Every 2 weeks, workers were asked to complete a survey about their perceived comfort and function with the respirator. Study details about EHMR wear time, respirator disinfection, use, and storage are reported elsewhere (Lane et al., 2024).
Elastomeric Respirator
The elastomeric respirator that was included in this study was the NIOSH Approved Honeywell RU8500 (Honeywell International Inc., Charlotte, NC) which participants were asked to use during routine patient care (e.g., feeding, bathing, suctioning, and intubation). This model was chosen due to four characteristics (Figure 1): (a) the exhalation valve diversion cover that kept air from being exhaled into a patient’s breathing zone; (b) filter covers that prevented potential liquid splashes from reaching the filter material; (c) the silicone body, as silicone is known to be easy to clean and disinfect; and (d) the speech diaphragm to facilitate clearer communication from the wearer. Because little was known about the EHMRs exhaled air during the start of the COVID-19 pandemic, the study hospitals required workers to place a surgical mask over the exhalation valve to ensure that patients were not inadvertently exposed to COVID-19 if a worker was infected (National Institute for Occupational Safety and Health [NIOSH], 2022). For purposes of feasibility, we chose to use smaller, pediatric masks, which workers were trained on how to place.
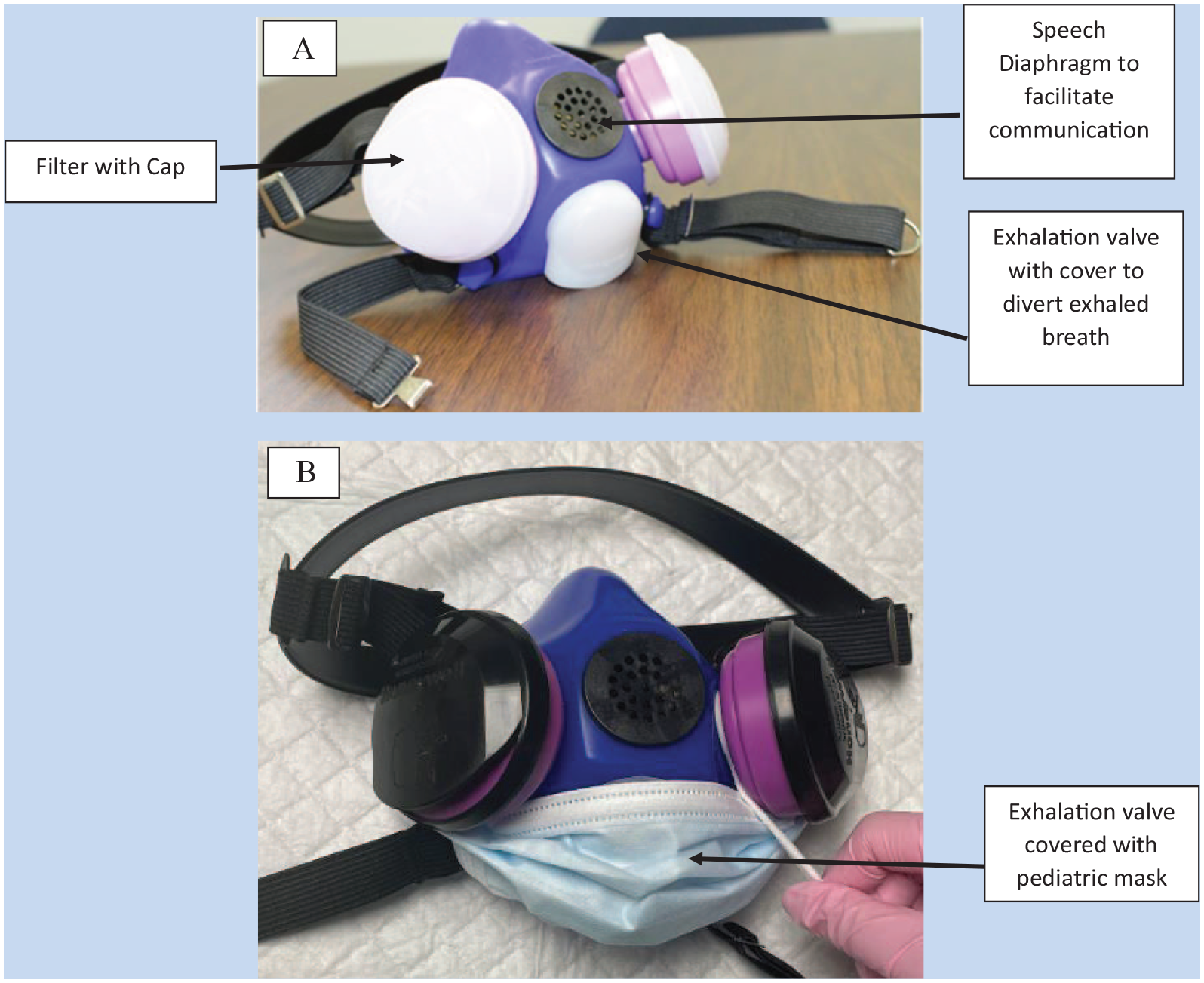
NIOSH Approved Honeywell™ RU8500 Series Elastomeric Half-Mask Respirator (EHMR) (A) Without Pediatric Mask; and (B) With Pediatric Mask Covering the Exhalation Valve
Subjects
Workers were eligible to participate if they were: (a) at least 18 years of age, (b) their jobs involved direct patient care or in-person counseling, (c) had been fit-tested to wear a N95 FFR in the prior two years, and (d) answered “yes” when asked if they regularly wore a respirator or mask to care for patients in the prior year. Workers who reported having anosmia or ageusia during recruitment were excluded from the study given the assumption that they would not be able to detect Bitrex™ (Dräger US, Houston, TX), the qualitative fit testing solution which was used to fit test workers prior to respirator use. They were also excluded if they had facial hair (e.g., beard or mustache) or a facial injury or adornment that would interfere with the seal of the respirator. At the TX hospital, recruitment was targeted to HCP who worked on inpatient units that were more likely to have patients with aerosol transmissible diseases such as COVID-19 or tuberculosis (e.g., emergency department and intensive care unit). The GA hospital restricted its recruitment to nurses and certified nursing assistants that provide care on one general medical ward and one intensive care unit. Workers were incentivized up to US$450 for their participation in the seven study surveys. This study received human subjects’ approval from the Institutional Review Board at The University of Texas-Health Science Center in Houston, Baylor College of Medicine, and Emory University.
Recruitment
Recruitment at the TX hospital was conducted virtually due to hospital-based COVID-19 restrictions that prevented study staff from entering the hospital. Study investigators presented an online study overview presentation to eight inpatient unit leaders who were then asked to email study invitations and flyers to their frontline workers. The invitations included a link to a REDCap (Harris et al., 2019) study site page in which workers had access to an online video about the study, an inclusion criteria questionnaire, and an online consent form. Workers who met the eligibility criteria and completed the consent form were then asked to sign up for a 60-minute time slot for fit testing and training. During the fit testing and training session, they watched a 10-minute video about EHMR use, what to expect over the course of the study, and the request to complete biweekly surveys. They were then fit-tested using qualitative methods and received face-to-face training on how to disinfect the EHMR and how to place the pediatric mask over the exhalation valve.
At the GA site, HCP employed on a general medical ward and an intensive care unit were invited to participate including nurses, certified nursing assistants, and patient care assistants. HCP received information about the study at daily unit huddles and through email. Charge nurses were recruited as “super users” and received additional training so that they could be the on-unit experts on the use of the EHMRs. Super users reminded participants to wear the EHMR and were available to answer questions and let the study team know if more supplies were needed. Upon enrollment, HCP filled out a screening survey and consent form online and then scheduled themselves to attend a fit testing session through the study hospital’s employee health unit. During fit testing appointments, Emory’s study team conducted a small training session with participants on the parts of the respirator, the placement of a pediatric mask over the exhalation valve, and the surveys they would be asked to complete as part of the study. Super users were trained to conduct an in-service training for the participants on their unit which included protocols for disinfection and storage. Participants were also sent a link to a video describing the different aspects of EHMR use.
Data Collection
Participants were asked to complete pre- and post-surveys (baseline and Week 12) and five biweekly surveys during Weeks 2 through 10 of the study. For purposes of examining the level of comfort with wearing the EHMR, participants were asked to complete the validated Respirator Comfort, Wearing Experience, and Function Instrument (R-COMFI; LaVela et al., 2017).
For these analyses, we examined their responses to this survey pertaining to EHMR tolerability at study Weeks 2 and 10, in which workers were asked to rank their tolerability in the prior 2 weeks of EHMR use. In addition, at Week 12 workers were asked to compare the EHMR comfort over the entire study period with their comfort of prior N95 FFR use before the onset of the study.
The R-COMFI questionnaire includes 21 questions that measure respirator tolerability including subscales of discomfort (10 items), general wearing experience (6 items), and function (5 items). For respirator discomfort, workers were asked to rate on a three-point Likert-type scare (0 = none of the time, 1 = some of the time, 2 = all of the time) about physical discomfort such facial irritation, itching, and pinching as well as experiences with nausea and headache while wearing the respirator (score range 0 to 20; higher score indicates greater discomfort). For general wearing experience, the same three-point Likert-type scale was used to rate workers’ experiences with physical factors such as dizziness, claustrophobia, shortness of breath, and dry/itchy eyes (score range 0 to 12, higher score indicates more difficult wear experience). The function scale measured workers’ ability to verbally communicate, their hearing and vision, as well as general interference with patient care duties while wearing the respirator, on a four-point Likert-type scale (0 = strongly disagree, 1 = disagree, 2 = agree, and 3 = strongly agree, score range 0 to 15, higher score indicated greater interference). We added four additional questions to the survey in which workers were asked to rate their difficulty with getting straps over their hair, frustration with wearing, and whether patients or coworkers reacted negatively to the respirator.
At the 12-week post-study period, participants were asked their level of agreement on a four-point Likert-type scale about their experiences with wearing the EHMR versus the N95 FFR, including questions as to which respirator they felt provided a better fit, better respiratory protection, and their preference of which respirator they would prefer to wear in current and future pandemic and non-pandemic conditions.
Open-ended questions were asked in each of the biweekly surveys, where participants were asked to indicate any new or continuous challenges with wearing the EHMR in the previous 2 weeks as well as issues that had improved. In the post-survey, participants were also asked to describe what they liked least and most about the EHMR.
Demographic details were also collected including age category, race, Hispanic/Latino ethnicity (yes/no), self-described sex, job title, work department, and types of prior respirator use.
Data Analysis
Descriptive statistics were employed to describe the occupational characteristics of study participants and their history of respirator use. For purposes of comparing changes in the R-COMFI measures across time periods, we restricted our analyses to individuals who completed both Weeks 2 and 10 surveys. For examination of individual survey items, categories were collapsed to compare some/all of the time (some/all) versus none of the time (none) for the Discomfort and General Wear items, and strongly agree/agree versus strongly disagree/disagree for the Function items. To examine an overall R-COMFI score, the three subscales were summed, including Discomfort (score range: 0-20) and General Wear (score range: 0-12), and Function (score range: 0-15; LaVela et al., 2017; Radonovich et al., 2019). The total sum of the R-COMFI score could range from 0 to 47, with a lower score equaling better respirator tolerability. All participants were included in the analysis at Week 12 where we compared R-COMFI measures between the EHMR and the N95 FFR. Differences between categorical measures were examined using the Mantel-Haenszel chi-square test, while differences in R-COMFI scores were measured using the paired t test. Open-ended data regarding respirator comfort and use were categorized into similar themes by two study investigators and reviewed by a third to ensure the accuracy of coding. We sought to describe themes that were more commonly experienced. SAS 9.4 was used to conduct all quantitative data analysis.
Findings
Among the 208 workers recruited from both locations, 183 (88.0%) completed the study through Week 12, and of those, 139 (74.0%) completed both the Week 2 and Week 10 surveys. Participants were more likely to be aged 18 to 35 years (62.3%) and identify as female (74.3%; Table 1). A large proportion indicated their race as White (59.0%), Black (20.8%), or Asian (14.8%), while the majority were non-Hispanic ethnicity (84.7%). More than half (52.5%) reported having a bachelor’s degree or higher (27.3%). Workgroups were predominantly nurses (51.9%), occupational/physical/speech therapists or assistants (16.9%), physicians/nurse practitioners or assistants (9.8%), or respiratory therapists (9.8%). A large proportion of workers were employed in intensive care units (ICU; 56.8%) or floated between hospital units (21.8%) followed by working in the emergency department (9.3%) or in general medicine units (8.2%).
Demographic Characteristics of Health Care Personnel (n = 183)
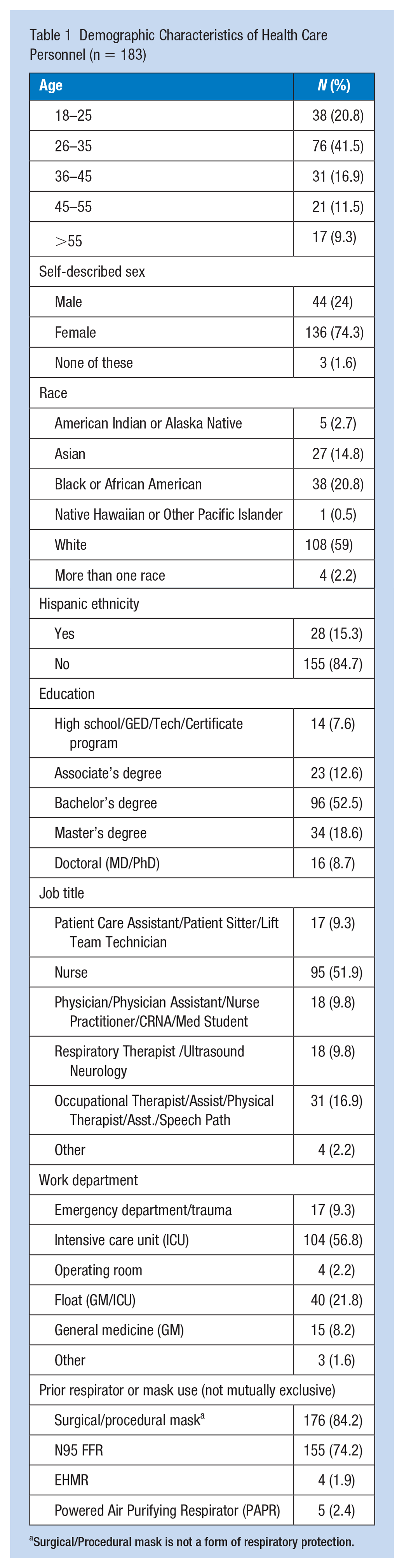
Surgical/Procedural mask is not a form of respiratory protection.
EHMR Wear Week 2 Versus Week 10
Among participants who indicated wearing their EHMR in the prior 2 weeks at study Week 2 and Week 10, the overall R-COMFI score slightly improved from 30.0 to 28.7 (p < .01; Table 2).
Continuous and Categorical Ratings of R-COMFI Among Health Care Personnel at Weeks 2 and 10 of Elastomeric (EHMR) Use (n = 139) a
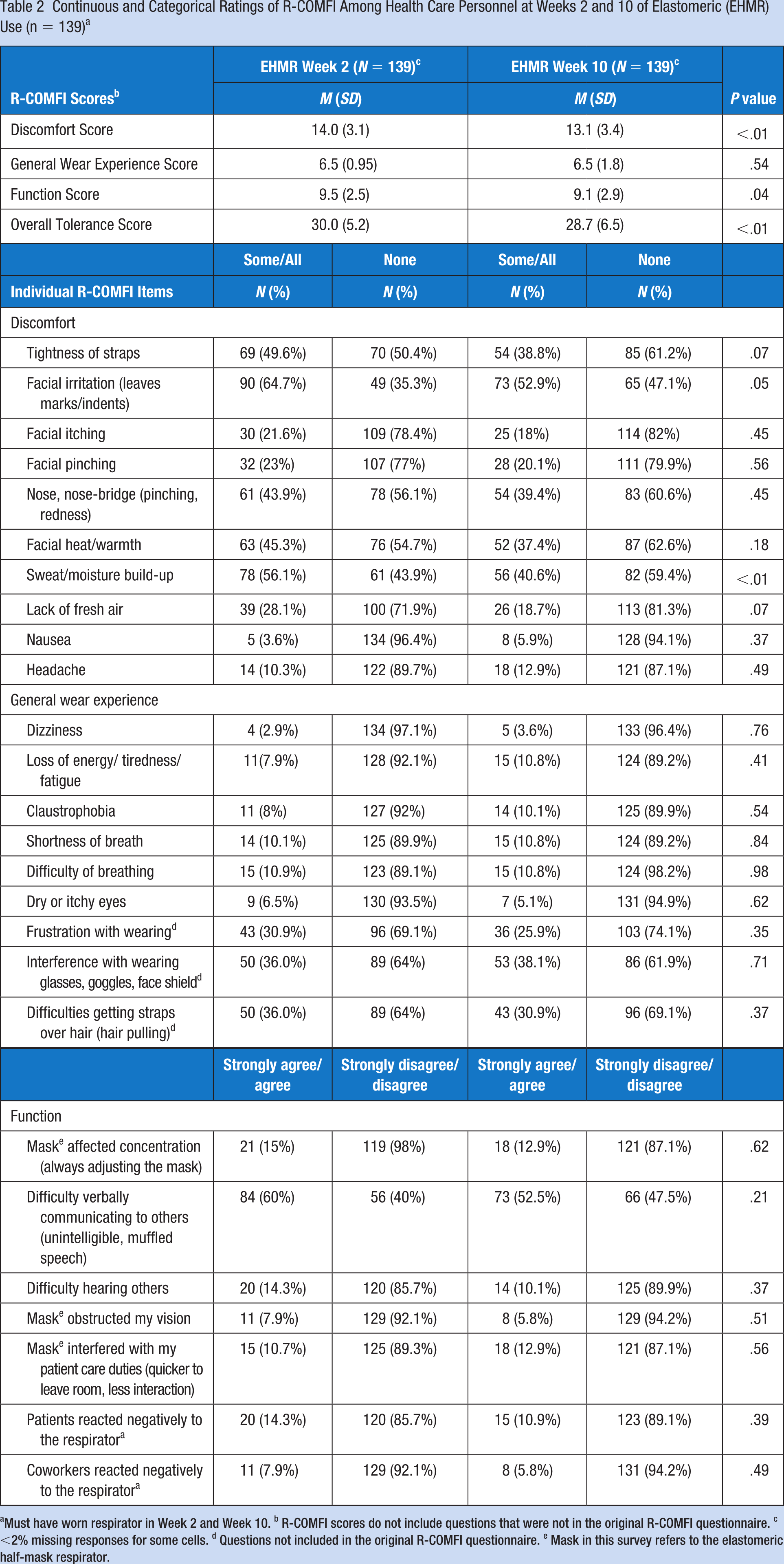
Must have worn respirator in Week 2 and Week 10. b R-COMFI scores do not include questions that were not in the original R-COMFI questionnaire. c <2% missing responses for some cells. d Questions not included in the original R-COMFI questionnaire. e Mask in this survey refers to the elastomeric half-mask respirator.
When examining the mean R-COMFI subscales, the discomfort score slightly improved from Week 2 to Week 10 (mean score: 14.0 vs. 13.1, p < .01). For the individual categorical discomfort scale items, all but two items improved in Week 10 relative to Week 2, with two that were significantly improved including facial irritation (64.7% vs. 52.9%; p = .05) and sweat/moisture build-up (56.1% vs. 40.6%; p < .01), and two that were borderline significant, including tightness of straps (49.6% vs. 38.8%; p = .07), and lack of fresh air (28.1% vs. 18.7%; p = .07). The other discomfort measures were not significantly different across time periods, with approximately 40% to 50% that indicated all/some of the time for nose pinching and facial heat/warmth. A much smaller percentage reported facial itching, pinching, nausea, and headache. The improved comfort scores over the 10-week period (Week 2 vs. 10) were reflected in participants’ comments, such as one worker who referred to the EHMR as a “mask” when they stated, “I surprisingly liked the mask a lot more as I got more comfortable with it. I will probably continue to use it . . .,” while another indicated “[The] comfort has gotten better—feels like [the] mask has molded to my facial features and sits perfectly, fitting got better.”
For the total general wear experience mean score, no difference was observed between Weeks 2 and 10 (mean score: 6.5 vs. 6.5, p = .54). When examining the individual categorical general wear items, approximately one-third of participants reported general frustration with wearing the EHMR (30.9% vs. 25.9%, p = .35), noting that the EHMR interfered with wearing glasses/face shield/goggles (36.0% vs. 38.1%, p = .71) as well as experiencing difficulty getting straps over their hair, which was not significantly different across time periods (36.0% vs. 30.9%, p = .37). When participants were asked what they liked/disliked about the EHMR, one participant indicated “I didn’t like my hair getting stuck in the straps” while others indicated “It was hard to keep my glasses in place on bridge of my nose,” and “It took time to get used to wearing bifocals with the mask (i.e., EHMR). When I was able to adjust my glasses with the straps there were very few problems.” Only a small proportion of participants (<10%) reported dizziness, loss of energy/fatigue, shortness of breath, or dry/itchy eyes in either time period.
Differences in the EHMR mean function score between Weeks 2 and 10 were modestly improved (mean score: 9.5 vs 9.1, p = .04). The individual categorical function items revealed that more than half of the participants during Week 2 (60.0%) had difficulty communicating to others despite this EHMR having a speech diaphragm, which persisted through to Week 10 (52.5%; p = .21). When participants were asked to indicate what they did not like about the EHMR, there was consensus that communicating with patients was difficult, with one worker indicating, “My main dislike was that it was difficult for patients and peers to hear me with the respirator on,” and another indicating “. . .I felt like I was always yelling.” When participants were asked how they would improve the design of the respirator, some indicated that the respirator needed an “improved voice box” or a “microphone.” Participants rated the other function items more favorably with only a small proportion indicating difficulty hearing others (Week 2,14.3% vs. Week 10, 10.1%, p = .37), visual obstruction due to mask (7.9% vs. 5.8%, p = .51), adversely affecting concentration (15.0% vs.12.9%, p = .62), and interference with patient care (10.7% vs. 12.9%, p = .56). A small proportion indicated that patients reacted negatively to the EHMR (14.3% vs. 10.9%, p = .39), and fewer (7.9% vs. 5.8%, p = .49) indicated that participants reacted negatively, with some stating, “It does freak out some older, confused patients” and “People react to it as if it’s a bit sci-fi.”
EHMR Versus N95 FFR
When examining the overall and subscale R-COMFI scores at the end of the study period (Week 12) between the EHMR and N95 FFR, the overall score was more favorable for the EHMR (33.7) versus the N95 FFR (37.4, p < .01; Table 3). Similarly, two of the three subscales of discomfort (p < .01) and general wear experience (p = .03) were more favorable for the EHMR, while function was more favorable for the N95 FFR (p < .01).
Comparison of R-COMFI of Elastomeric Versus N95 Filtering Facepiece Respirators Among Health Care Personnel at Two U.S. Hospitals (n = 183)
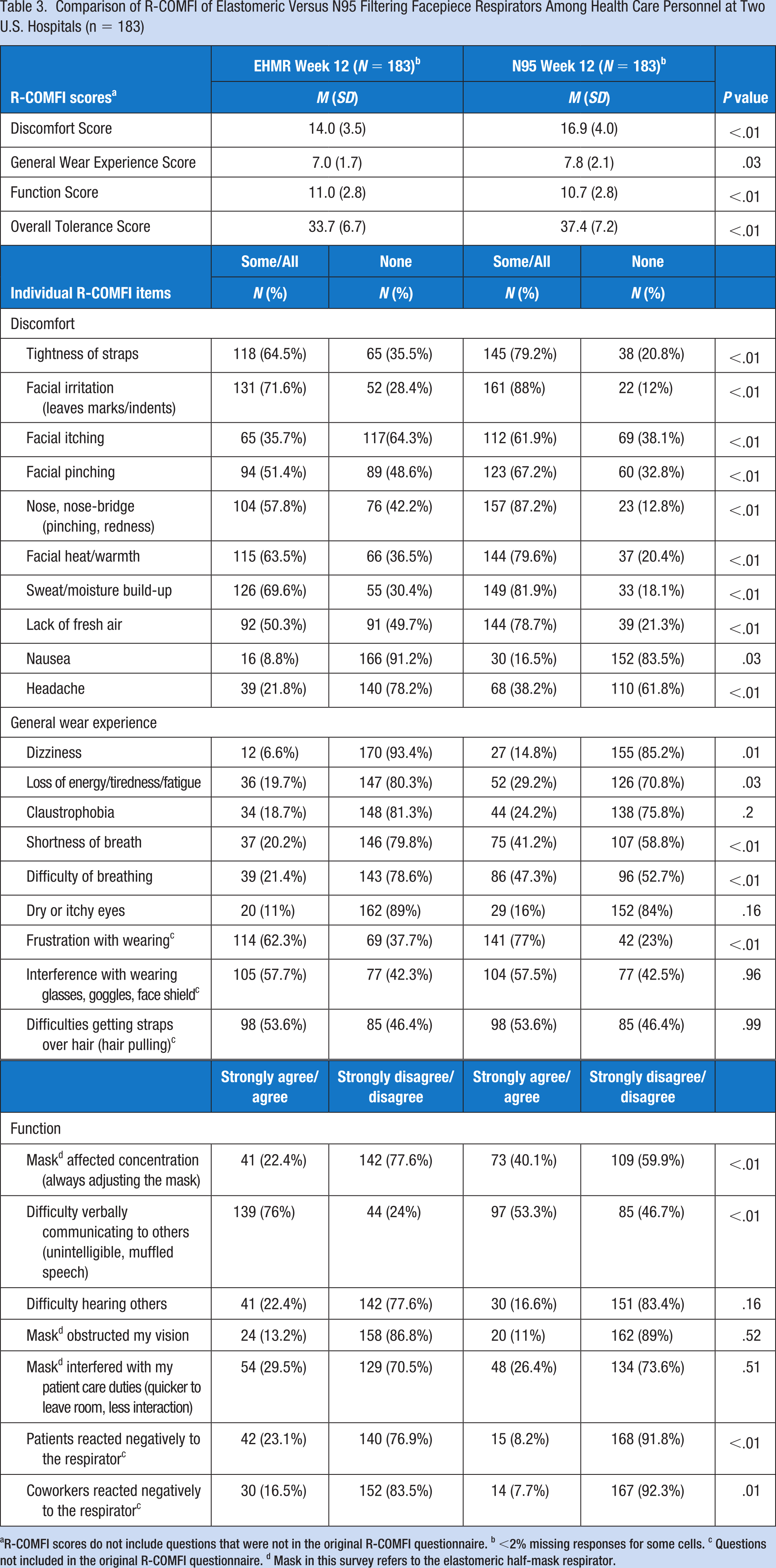
R-COMFI scores do not include questions that were not in the original R-COMFI questionnaire. b <2% missing responses for some cells. c Questions not included in the original R-COMFI questionnaire. d Mask in this survey refers to the elastomeric half-mask respirator.
When comparing individual comfort items across the R-COMFI subscales, most were rated more favorably for the EHMR relative to the N95 FFR. Among the discomfort items, all were rated more favorably for the EHMR, including facial itching (EHMR: 35.7% vs. N95 FFR: 61.9%; p < .01), lack of fresh air (50.3% vs. 78.7%, p < .01), nausea (8.8% vs. 16.5%, p = .03) and headache (21.8% vs. 38.2%, p < .01).
Similar patterns were observed for the general wear items, including shortness of breath (EHMR 20.2% vs. N95 FFR: 41.2%; p < .01), difficulty breathing (21.4% vs. 47.3%; p < .01), and dizziness (6.6% vs. 14.8%; p < .01). Although more than half (62.3%) of participants indicated frustration with wearing the EHMR, even more (77.0%, p < .01) rated the N95 FFR as frustrating to wear. When participants were asked what they liked about the EHMR, many indicated that they favored it over the N95 FFR, with one stating, “I like that there is a good, secure fit to my face and it’s easy to test the positive/negative pressure to ensure a good fit. The material also felt better against my face, compared to the N95 FFR.” Another participant indicated, “[It] made me feel extra secure during my patient interactions. I felt the fit was more customized to my face compared with the N95s FFRs provided by my department.”
For the EHMR function measures, only one item was rated more favorably for the EHMR versus the N95 FFR, which included the respirator affecting the worker’s concentration while working (EHMR 22.4% vs. N95 FFR 40.1%; p < .01). The EHMR was rated as being more difficult than the N95 FFR for verbally communicating (76.0% vs. 53.3%; p < .01). Workers also indicated that they perceived more negative reactions from patients (23.1% vs. 8.2%, p < .01) and coworkers (16.5% vs. 7.7%, p < .01) with the EHMR relative to the N95 FFR. No significant differences between the two devices were observed for difficulty hearing others, obstructed vision, or interference with patient care.
In the post-study period, compared to the N95 FFR, the majority of participants (88%) indicated that they felt the EHMR fit better, felt it provided greater protection from viruses and bacteria (88%), and they preferred to wear it while caring for COVID-19 patients (74.9%; Table 4). These findings were reiterated in the open-ended questions where participants were asked what they liked about the EHMR, with many indicating that they felt more protected relative to the N95 FFR. For example, one worker indicated that “It had a great seal and I felt better protected related to mask [facepiece] leaks with N95 FFR,” while others indicated that it “felt safe and more comfortable than a N95 FFR,” it has a “better seal than [the] N95 FFR,” and “I can breathe easier.” With regard to wearing the EHMR during non-pandemic conditions, the majority of participants (69.9%) indicated that they felt comfortable doing so; however, half (53.6%) indicated that in nonpandemic conditions they would prefer to wear the N95 FFR over the EHMR. Some participants commented on their preference for N95 FFR in non-pandemic conditions, with one participant who indicated “for extended wear the elastomeric is much more comfortable, the N95 FFR is more convenient for intermittent use as it doesn’t require disinfection and drying time.”
Health Care Personnel’s Perceptions of the EHMR After Three Months of Use (N = 183)
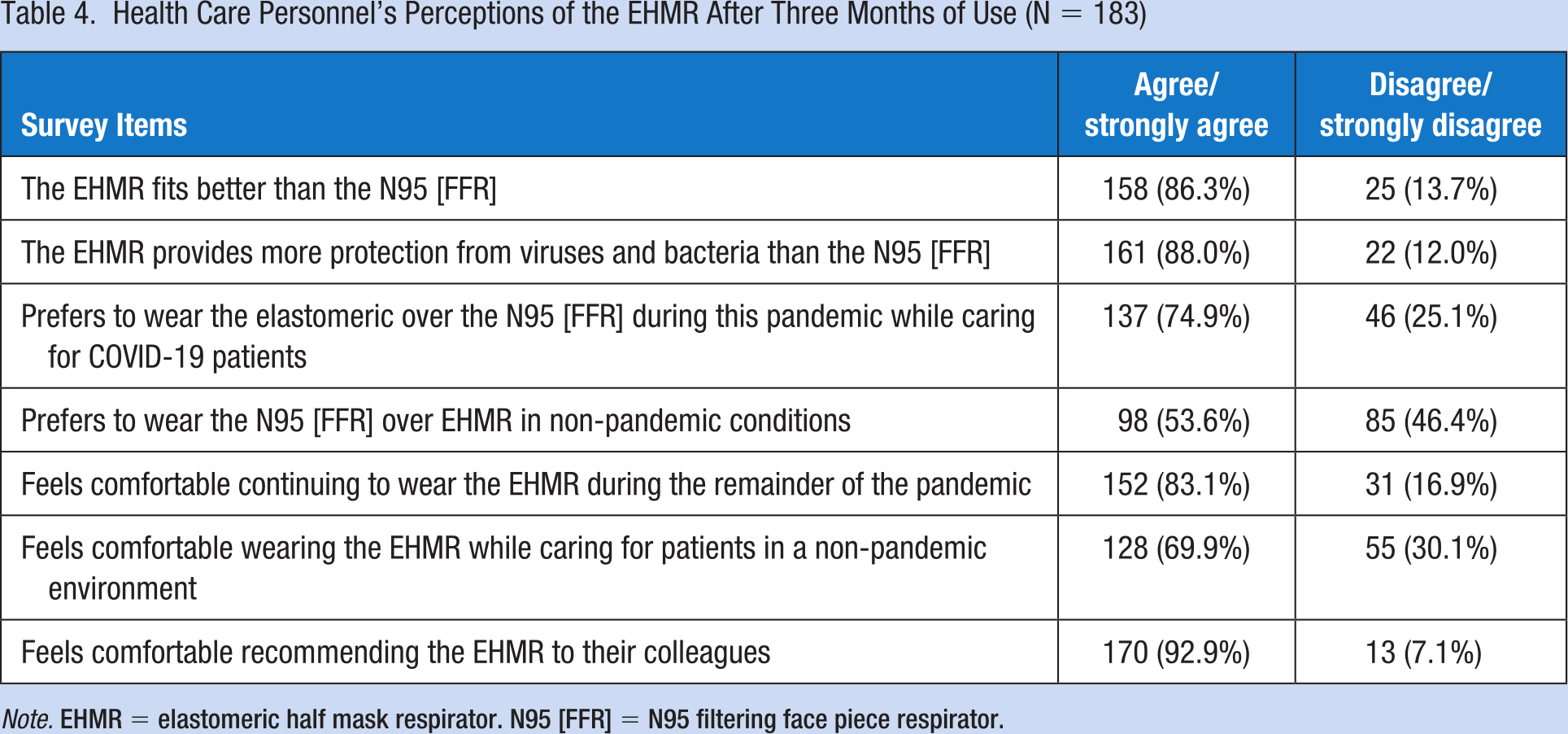
Note. EHMR = elastomeric half mask respirator. N95 [FFR] = N95 filtering face piece respirator.
When participants were asked why they chose to participate in this study, as well as aspects of the EHMR they liked, many indicated that they liked that the EHMR could be reused, with participants stating, “It minimizes waste,” “I feel like I am creating less waste by using the [EHMR],” and “I do like that you do not have to throw it away and it is essentially sustainable.” Because of respirator shortages, participants also liked that they were assigned their own respirator, with one worker indicating, “It was only mine, I was responsible for cleaning and caring for it, and I didn’t worry that it was worn by others then disinfected.” Others indicated, “I feel secure knowing I have an alternative mask [i.e., respirator] especially with supply shortage we’ve seen in the past” and “I liked having a personal respirator and not being reliant upon department provision of N95 FFR.”
Discussion
This study examined HCP’s perceived levels of physical comfort and function with wearing the EHMR while conducting routine patient care. Overall, the EHMR received respectable R-COMFI scores among participants who wore the respirator consistently over a 10-week period, including improved scores for several of the comfort items between the two time periods. These findings are promising, especially given that we also observed significantly better comfort ratings for the EHMR relative to the N95 FFR. To date, only one study has examined differences in comfort between these two devices, in which the N95 FFR was rated more favorably among HCPs who only wore the N95 FFR compared with HCPs who only wore the EHMR (Hines et al., 2017, 2019b). In this study, participants were asked a single question about how much they liked their respirator with respect to comfort and they rated the N95 FFR slightly higher (3.42) than the EHMR (3.28) on a five-point scale.
Although participants rated many of the R-COMFI items more favorably over time, and more favorably compared with the N95 FFR, there were some poorly rated items that persisted including issues with communication, facial irritation, facial pinching, nose pinching, heat/warmth, and interference with wearing glasses. Difficulty communicating while wearing the EHMR was not an unexpected finding as it has been reported in prior studies (Ciconte & Danyluk, 2013; Hines et al., 2019b), and this is recognized as an issue that needs to be addressed when designing future EHMRs specifically for use in health care settings (Radonovich et al., 2010). Prior multidisciplinary efforts to improve the design of the EHMR have proven successful, including efforts put forth by Project B.R.E.A.T.H.E., which is a partnership between federal agencies (e.g., NIOSH’s NPPTL), academic researchers and respirator manufacturers (U.S. Department of Veterans Affairs et al., 2009). It is essential to engage respirator manufacturers to improve the long-standing communication limitations with the EHMR.
We tested the use of the EHMR during an ongoing pandemic, with a large proportion of participants who indicated that they perceived the EHMR to fit better and to provide better protection relative to the N95 FFR, which is similar to findings reported in other studies conducted during non-pandemic conditions (Ciconte & Danyluk, 2013; Hines et al., 2019b). Similar to Hines et al. (2019b), our study participants indicated that while the EHMR fit better and they perceived better protection, a large proportion also indicated that they would prefer to wear the N95 FFR in nonpandemic conditions (Hines et al., 2017, 2019b). Qualitative data from our study suggested that participants felt the N95 FFR was easier to use than the EHMR, especially when quick tasks needed to be conducted. Additional findings from our study (reported elsewhere; Lane et al., 2024) suggest that the process of doffing and disinfecting the respirator between patients was perceived as time-consuming, perhaps contributing to a preference for the disposable N95 FFR when shorter periods of respiratory protection are warranted.
There are several limitations to this study that should be considered. We compared EHMR use during the study period to workers’ N95 FFR use prior to the start of the study; however, we did not obtain detailed measures such as frequency of use. We used specific inclusion criteria to ensure that we included workers that had prior experience wearing the N95 FFR including those that had been previously fit-tested for the N95 FFR. Differences that we observed in EHMR vs. N95 FFR measures may have been influenced by differences in frequency of N95 FFR that we did not measure. Other limitations to consider, especially among occupational health professionals that are planning on implementing the EHMR into their health care setting. First, we only tested one model of EHMR which was the Honeywell RU8500 series. There are various EHMRs (makes and models) that should be pilot tested and considered prior to implementation. This includes newer models that do not have an exhalation valve or have adaptors to filter exhaled breath through valves, removing the need to place a mask or face shield over the valve. Such changes in model design could remove certain communication barriers but also exacerbate others such as breathing. This issue has not been examined. Given the stated dislikes for the EHMR by study participants, such as difficulty communicating and facial irritation, more studies need to be conducted for purposes of examining participants’ physical comfort while performing patient care tasks among a range EHMR makes and models. Future studies should also examine if and/or how duration of EHMR use over a work shift can be modified based on comfort, which our study did not examine. For purposes of examining if EHMR comfort changed over time, we restricted our longitudinal analysis to participants who reported using the EHMR at study Weeks 2 and 10; however, this most likely excluded participants that may have decreased their use because they found the respirator to be uncomfortable. This may explain why the 12-week R-COMFI findings for the EHMR were less favorable for the whole cohort compared to those in the restricted analysis. In addition, some participants may not have worn the N95 FFR since before the study period, which may have biased their rating to be more favorable for the EHMR relative to the N95 FFR.
Implications for Occupational Health Practice
There are numerous factors to consider when implementing the EHMR into the health care setting. This study focused on the individual workers’ comfort while wearing the EHMR, their ability to use the EHMR, disinfect and store it, as well as use it while performing specific patient care tasks (reported elsewhere; Lane et al., 2024). However, organizational factors must also be considered. For example, in a prior study, we observed that it was feasible to rapidly fit test and train HCPs to wear the EHMR in a hospital setting that had an established Occupational Safety and Health Administration (OSHA)-approved Respiratory Protection Program (OSHA, 2011; Pompeii et al., 2020). Furthermore, Hines and colleagues (2023) conducted a study examining an existing EHMR program where the hospital, rather than the worker, was responsible for EHMR disinfection and storage. While findings from these and other studies demonstrate that EHMR use in health care is feasible, more research is needed to support the implementation of an EHMR program at the work unit and organizational levels.
Applying Research to Occupational Health Practice
This prospective cohort study examined HCWs level of tolerance to wearing the EHMR during routine patient care, which we measured every 2 weeks, over 12 weeks, using the validated R-COMFI questionnaire. We also asked workers to compare their tolerance for the EHMR with their prior use of the N95 FFR. Overall, workers showed an improved tolerance for the EHMR between Week 2 and Week 10 of the study. Moreover, they rated the EHMR more favorably than their N95 FFR. These findings suggest that the EHMR may be a feasible respiratory protection device with respect to tolerance, which includes comfort, wear experience, and function. There are numerous factors that the occupational health nurse should consider when introducing the EHMR into the hospital setting, including the processes for fit testing and training workers, as well as training them on how it is used, disinfected, and stored. Our study only examined a single make and model of EHMR, while it would be beneficial to have various EHMR makes/models available to workers. There are numerous steps involved with introducing the EHMR into the hospital setting, and perhaps pilot testing the process prior to scaling the program hospital-wide would be advantageous.
Footnotes
Acknowledgements
The authors would like to recognize Kevin Strickland, Emily Haas, and Mihili Edirisooriya from the National Personal Protective Technology Laboratory for their thoughtful reviews of this document. We would also like to thank Dr. Lewis Radonovich for his earlier contributions to this work.
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention. Mention of any company or product does not constitute endorsement by the National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Centers for Disease Control and Prevention, National Institute of Occupational Safety and Health, cooperative agreement 75D30118C02645.
Human Subjects
This study received human subjects’ approval from the Institutional Review Board at The University of Texas-Health Science Center in Houston, Houston Texas; Baylor College of Medicine, Houston, Texas; and Emory University, Atlanta, Georgia.
Attribution Statement
N95 is a certification mark of the U.S. Department of Health and Human Services (HHS) registered in the United States and several international jurisdictions.