
Abstract
Increased prevalence of obesity may be due to an increase of being sedentary at work. Increasing non-exercise activity thermogenesis (NEAT) using walking workstations may increase total physical activity and promote a leaner physical body composition (or phenotype). The purpose of this study was to test whether walking slowly during work was sufficient to promote a leaner phenotype by increasing physical activity in sedentary desk workers without inducing compensation or a decrease in activity or energy expenditure during the nonworking hours. We conducted a prospective cohort study using a within-subjects crossover design. The design involved two phases each lasting 2 weeks: a treadmill exercise phase in which subjects used a walking workstation for 2.5 hours a day 5 days/week and a control phase in which subjects maintained their normal work activity. Twenty-five sedentary adults working at the Minneapolis VA Health Care System. We measured body weight, body composition, food intake, 24-hour physical activity, and self-reported physical activity with the International Physical Activity Questionnaire (IPAQ). Treadmill exercise caused a leaner phenotype (lean mass gain and fat mass loss) and significantly increased their 24-hour physical activity. Walking workstation use had favorable effects on physical well-being and mental focus and did not adversely affect productivity. Light treadmill exercise during work can increase physical activity and result in a leaner body composition. This is a potentially useful intervention to increase NEAT in the modern sedentary work environment.
Keywords
Introduction
Obesity is a global epidemic as its prevalence has increased across all ages, races, and socioeconomic groups (Wang, McPherson, Marsh, Gortmaker, & Brown, 2011). Employment-related physical activity has declined over recent decades, correlating with increased body weight among U.S. adults (Church et al., 2011). Energy expenditure associated with sedentary behaviors, such as sitting during work or commuting, is very low at 1.0 to 1.5 METs (metabolic equivalents, a measure of physical activity; Ainsworth et al., 2000). Thus interventions to reduce sedentary time at work may be useful in the battle against obesity.
Traditional “exercise” prescriptions do not always successfully increase overall energy expenditure (Colley, Hills, King, & Byrne, 2010). This may be due to individual variability in appetite and total energy expenditure responses to exercise which in some individuals may result in increased food intake or decreased energy expenditure. This phenomenon has been referred to as “compensation” (King et al., 2012; Pomerleau, Imbeault, Parker, & Doucet, 2004; Whybrow et al., 2008). Some researchers have proposed that this “compensation” occurs by reducing one specific component of total energy expenditure, the non-exercise activity thermogenesis (NEAT; Levine, Eberhardt, & Jensen, 1999). Non-exercise activity thermogenesis encompasses all activities of daily living other than exercise, including sitting, standing, walking, and fidgeting, and has been suggested to explain the variability among individuals’ susceptibility to weight gain (Donahoo, Levine, & Melanson, 2004; Elbelt et al., 2010; Levine, 2007; Levine et al., 1999; Levine et al., 2005; Levine, Schleusner, & Jensen, 2000; Ravussin, 2005). Thus, “compensatory” reduction in NEAT may explain how exercise interventions sometimes fail to promote weight loss, particularly where subjects have been reported to be less active during subsequent hours of the day, negating any increases in total energy expenditure (Colley et al., 2010; Rosenkilde et al., 2012; Thivel, Aucouturier, Metz, Morio, & Duché, 2014; Whybrow et al., 2008).
The walking workstation consists of a setup that allows for walking slowly on a treadmill while working at a raised desk and has been proposed as an intervention to increase NEAT (Levine & Miller, 2007; Thompson, Foster, Eide, & Levine, 2008). The walking workstation is feasible in the work environment (Thompson et al., 2008) and does not have adverse effects on typing (Funk et al., 2012; Straker, Levine, & Campbell, 2009), speech quality (Cox et al., 2011), or cognitive function (Ohlinger, Horn, Berg, & Cox, 2011). Estimates of NEAT requirements for weight loss based on controlled experiments of short duration, deduced that walking workstation use for 2.5 hours per day would achieve a weight loss goal of 20 to 30 kg/year in obese individuals (Levine & Miller, 2007). Prospective studies evaluated the effects of a long-term intervention using walking workstations and found favorable effects on total daily physical activity, anthropometric measures, body composition, lipid, and metabolic variables (John et al., 2011; Koepp et al., 2013; Schuna et al., 2014), but limitations of both studies are that participants were not directed to the duration of use and total energy expenditure was not assessed. Understanding whether the use of walking workstations causes a sustained increase in NEAT is important in predicting weight loss or obesity prevention outcomes and determining the usefulness of recommending a “NEAT approach” to obesity prevention in the modern work environment. This study was designed to test whether the addition of low-intensity activity in the form of walking during work for 2 weeks could promote a leaner phenotype without compensatory reductions in physical activity. The hypothesis was that the intervention would result in increased physical activity and a leaner phenotype.
Materials and Methods
Study Subjects and Design
This prospective cohort study was conducted at the Minneapolis Veterans Affairs Health Care System (MVAHCS) in Minneapolis, Minnesota, USA. Participants were adult (>18 years of age) MVAHCS employees who had a sedentary job, defined by the Social Security Administration and Code of Federal Regulations as “work that involves lifting no more than 10 pounds at a time, and which mainly involves sitting” (20 CFR 404.1567 Physical exertion requirements). Exclusion criteria included current smoking; current alcohol use of more than two drinks per day; intake of a weight-altering medication or undergoing weight reduction surgery; pregnancy, lactation, or having given birth in the past year; chest pain or shortness of breath during exercise or after walking one block; physical disability that would prevent walking; and serious neurological or chronic illnesses including cancer, diabetes, stroke, heart disease, lung disease, kidney failure, liver failure, or any severe physical or psychiatric illness preventing the subject from fully participating in the protocol. Recruitment flyers were posted for 2 weeks in the MVAHCS employee daily briefing email. In total, 148 subjects were recruited and 25 finished the study and were included in the data analysis (Figure 1). The study protocol was reviewed and approved by the MVAHCS Institutional Review Board. Written informed consent was obtained from each subject prior to enrollment.
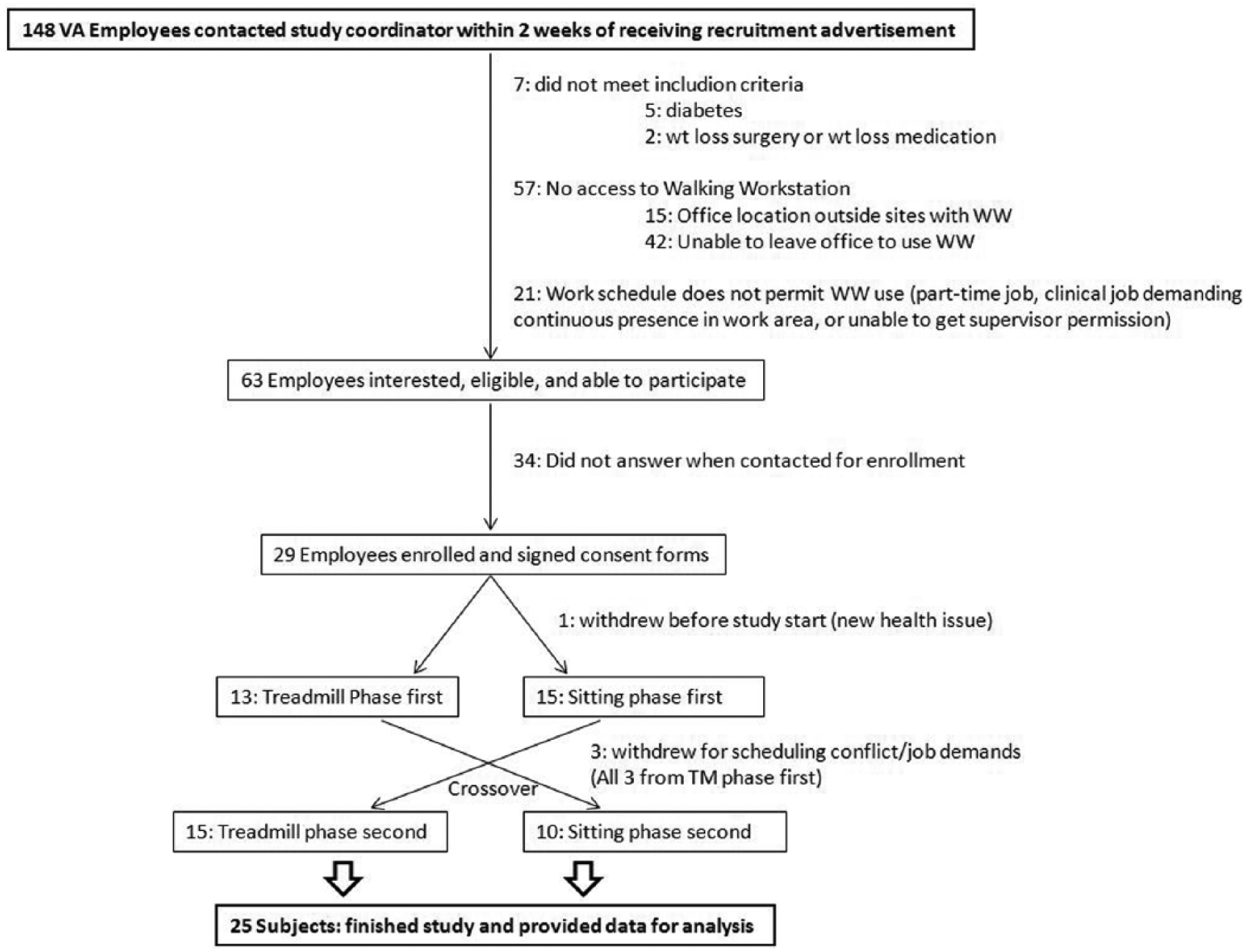
Study flow of participants.
The research protocol consisted of a crossover design with two phases: a treadmill exercise and a control phase. During the treadmill exercise, subjects walked on a treadmill at a slow pace (maximum 2 mph) while performing the usual work duties for 2.5 hours a day, 5 days/week. The control phase consisted of performing usual activities while sitting at a desk. Each phase lasted 2 weeks. Three walking workstations (FitWork® Walkstation; ©2010 Steelcase Inc., Grand Rapids, MI) were available on-site at the MVAHCS for use: one purchased by the study group, and two donated by the Employee Health Promotion Disease Prevention Program (Occupational Health Safety and Prevention Strategic Health Group) of the MVAHCS. Treadmill dimensions were 78 × 67 inches, and the work surface dimension was 78 × 29 inches. Subjects were allowed to set their own comfortable height and speed as long as they were actively walking during the entire 2.5 hours. Subjects were asked to maintain a log of the actual treadmill usage time and speed, and this log was used to determine which subjects achieved the recommended treadmill usage duration. Subjects were asked not to make any changes in diet and exercise routine between the two phases of the trial.
Variables and Measurements
At the beginning and end of each phase, subjects’ height and weight were measured by Stadiometer and body composition by air displacement plethysmography (BOD POD® Gold Standard; Life Measurement, Inc., Concord, CA, USA; McCrory, Gomez, Bernauer, & Molé, 1995). Physical activity was monitored by the Actical® activity monitor at the ankle (Philips Respironics, Bend, OR, USA) for the entire duration of the study, using 1-minute intervals to record physical activity (Heil, 2006). Weekly International Physical Activity Questionnaires (IPAQ®, Short Version; Mäder, Martin, Schutz, & Marti, 2006) were completed by each subject. At the end of the study, subjects completed an exit questionnaire evaluating their overall experience.
Statistical Analyses
Our purpose was to test the effectiveness of the intervention, and thus, a per-protocol analysis was performed in which only the subjects who completed the prescribed regimen (≥1,500 minutes of treadmill usage per 2-week period, as evidenced by treadmill usage logs that they completed) were included in the analysis (n = 19). Changes in body weight, fat mass, and lean mass (kg) were analyzed using a linear mixed model. Effects of treatment (i.e., treadmill usage) on actual total physical activity (as measured by daily step counts using Actical® accelerometer) were tested with a paired t test for data obtained from all subjects who achieved the recommended treadmill usage. Effects of treatment on food intake were analyzed with an analysis of covariance (ANCOVA) using number of weekend days in the measurement period as a covariate.
Results
Of the 29 subjects who enrolled in the study, four subjects withdrew, and 25 completed the entire study (Figure 1). We present the data for 19 subjects who achieved at least the prescribed 1,500 minutes of treadmill usage during the total 2-week period for a per-protocol analysis. Table 1 shows baseline characteristics of the 25 subjects who completed the study and the 19 subjects who complied with the prescribed intervention. Their job descriptions encompassed administrative, management, research, or clinical coordinator roles, all of which required mostly computer and telephone work. Medical conditions reported by the subjects were hypothyroidism (n = 4), hypercholesterolemia (n = 3), migraines (n = 1), pacemaker (n = 1), allergic rhinitis (n = 1), inflammatory arthritis (n = 1), and Factor V Leiden (n = 1). There were no differences in baseline characteristics between all subjects (N = 25) and those who achieved the prescribed treadmill usage (n = 19) that predicted completion of the treatment.
Baseline Characteristics of Participants of the NEAT Study
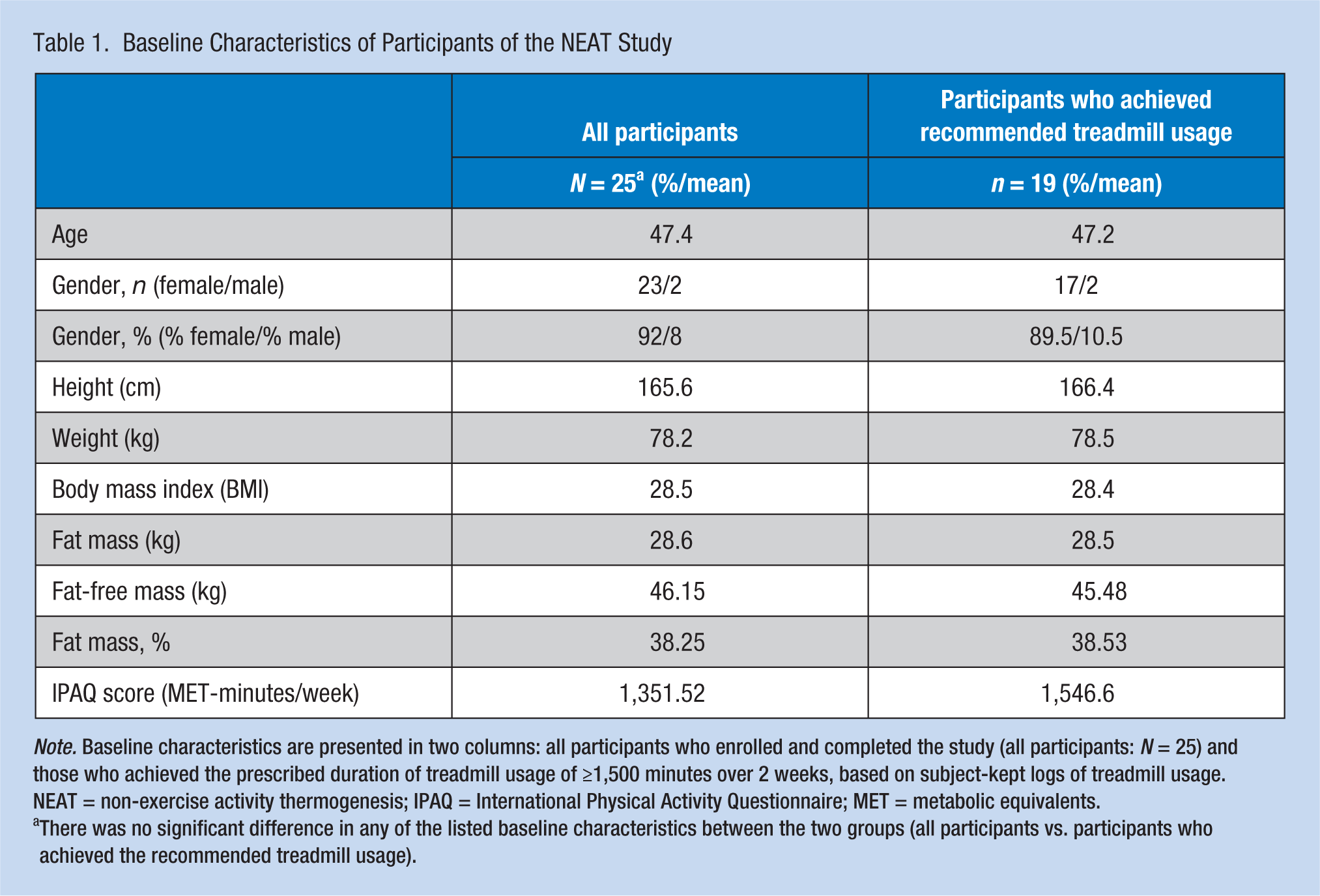
Note. Baseline characteristics are presented in two columns: all participants who enrolled and completed the study (all participants: N = 25) and those who achieved the prescribed duration of treadmill usage of ≥1,500 minutes over 2 weeks, based on subject-kept logs of treadmill usage. NEAT = non-exercise activity thermogenesis; IPAQ = International Physical Activity Questionnaire; MET = metabolic equivalents.
There was no significant difference in any of the listed baseline characteristics between the two groups (all participants vs. participants who achieved the recommended treadmill usage).
Figure 2 shows the effects of treadmill exercise on body weight (BW), fat mass (FM), and lean mass (LM) (Figure 2). Treadmill exercise use resulted in a nonsignificant trend toward body weight loss after the treadmill phase and body weight gain after the control phase (Figure 2a, p > .05). There was a significant loss of fat mass (Figure 2b, p = .04) and a significant increase in lean mass (Figure 2c, p = .012) compared with control treatment. Treadmill exercise increased overall physical activity measured by step counts using the Actical® system (p < .01) (Figure 3).
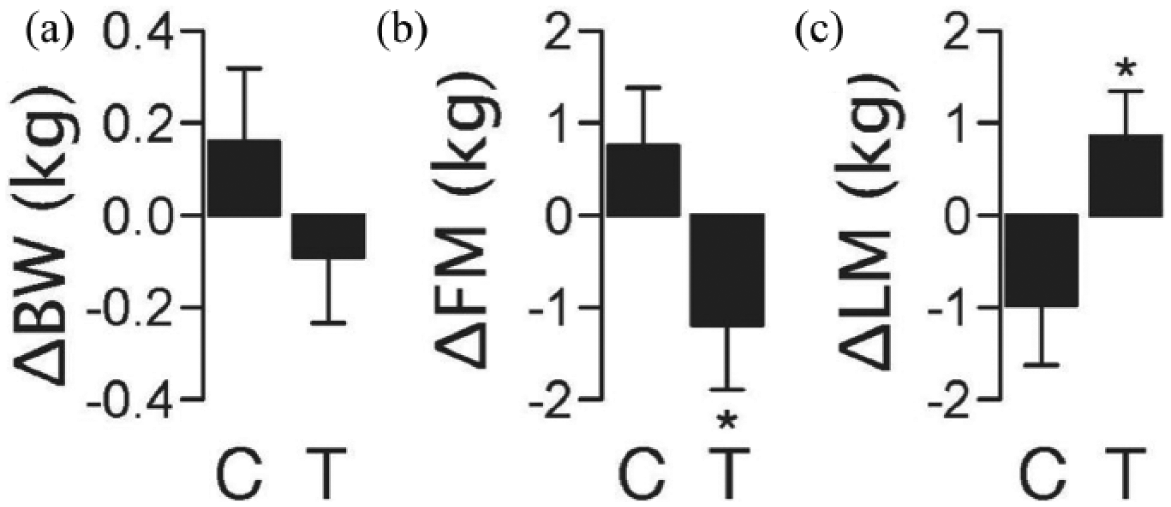
Effect of treadmill exercise on body weight and composition: (a) ΔBW: change in body weight in kilograms; (b) ΔFM: change in fat mass c in kilograms; (c) ΔLM: change in lean mass in kilograms.
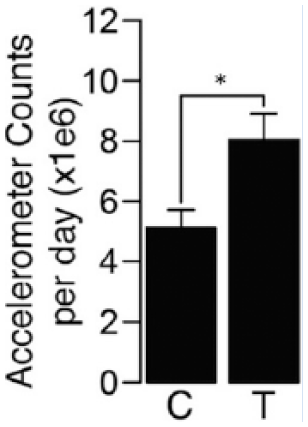
Effect of treadmill exercise on total physical activity.
Figure 4 shows the effects of the intervention on food intake patterns. There was a trend toward higher caloric intake during the treadmill exercise phase (Figure 4a, p = .11). Treadmill treatment significantly increased carbohydrate intake compared with the control period (Figure 4c, p < .05). A significant effect was not seen with protein or fat intake (Figure 4b and 4d).
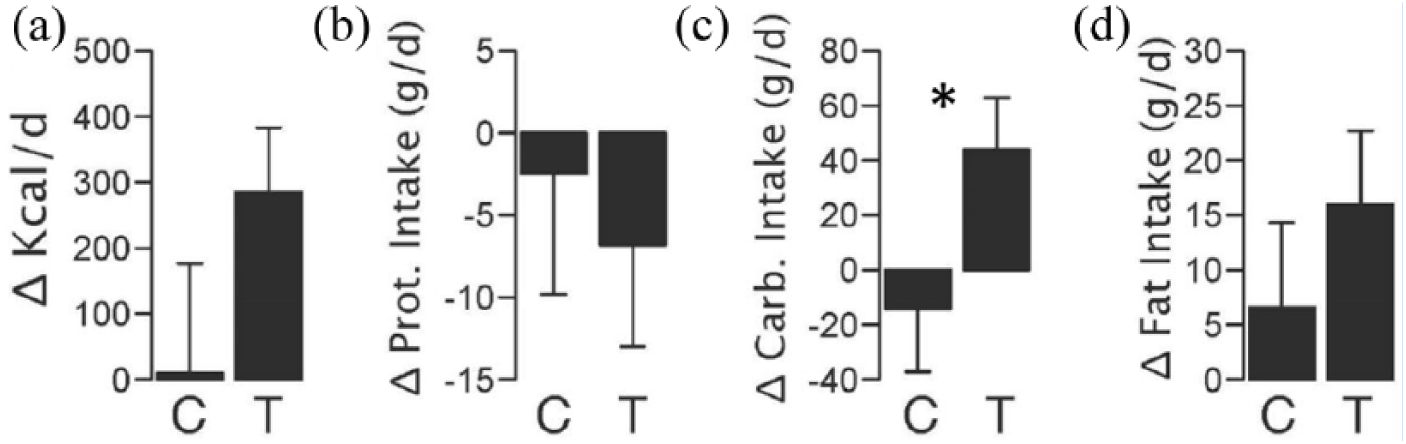
Effect of treadmill exercise on food intake: (a) Δkcal/d: change in total daily calorie intake, measured in kilocalories per day; (b) ΔProt intake: change in daily protein intake, measured in grams per day; (c) ΔCarb intake: change in daily carbohydrate intake, measured in grams per day; (d) ΔFat intake: change in daily fat intake, measured in grams per day.
Table 2 shows the assessment of the intervention by the subjects after completion of the study. Ninety-five percent of the subjects agreed that they would use the walking workstation in their work environment if available. Eighty-one percent of the participants described an improvement in their energy and mood after using the walking workstation. Some of the drawbacks were the initial need for adjustment to the new workspace and being away from one’s own desk/phone in cases where they had to share the workstation.
Subject Assessment of Walking Workstation Use.
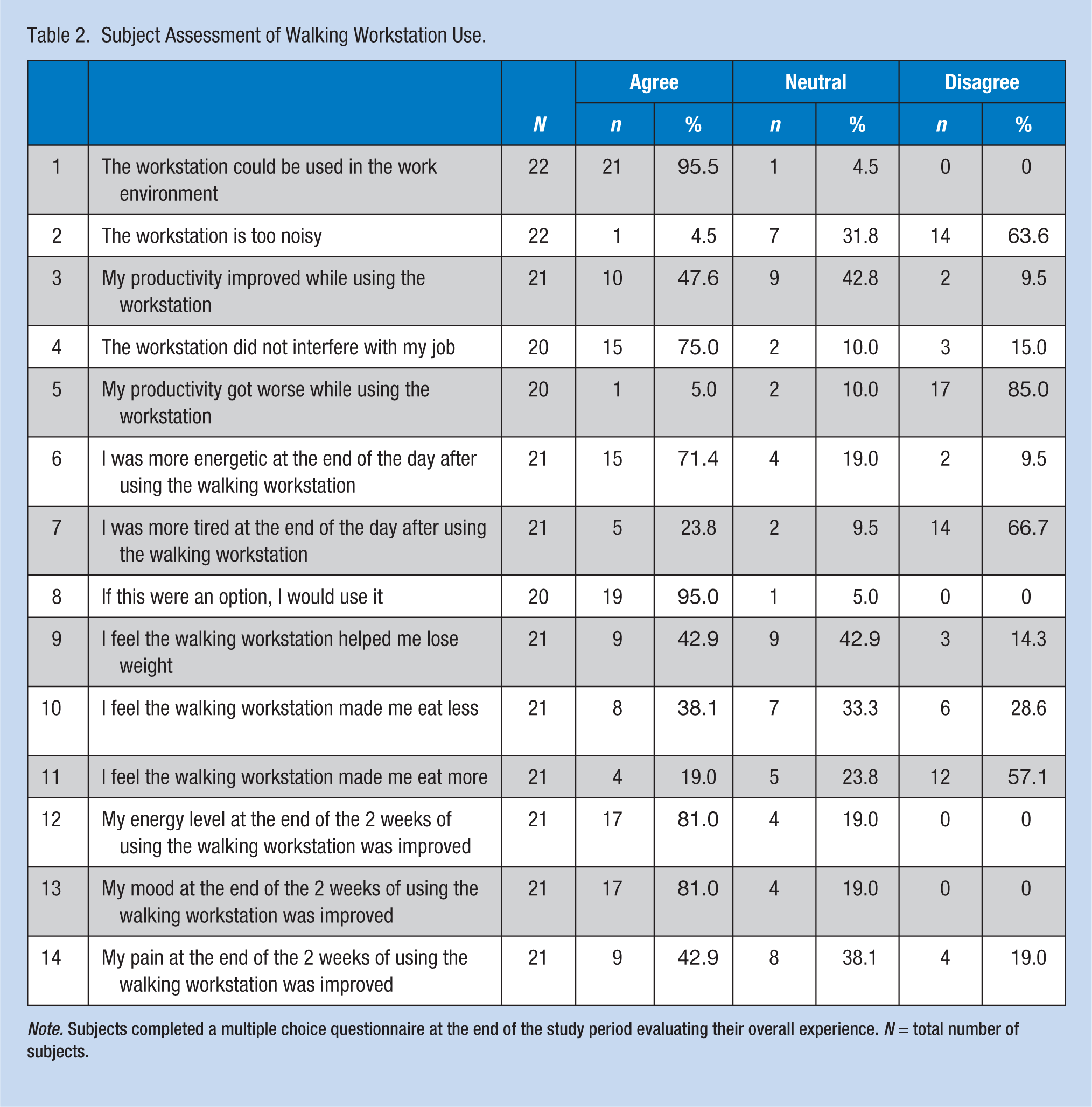
Note. Subjects completed a multiple choice questionnaire at the end of the study period evaluating their overall experience. N = total number of subjects.
Discussion
This study shows that in sedentary workers, low-intensity activity in the form of walking for 2.5 hours per day during work for 2 weeks increased overall physical activity and a trend toward a leaner body composition, despite increased carbohydrate intake. The within-subjects crossover design of this study allowed for comparisons between the intervention and control phases.
The study findings have clinical as well as societal/public health implications. The obesity epidemic has been attributed, in part, to the sedentary nature of work. Over the past 50 years, there has been a progressive decrease in the percentage of individuals employed in occupations that require moderate intensity physical activity, resulting in a decrease of more than 100 calories in daily occupation-related energy expenditure, accounting for a significant portion of the increase in mean body weight for U.S. women and men (Church et al., 2011). Work days are associated with more sitting and less walking/standing time than leisure days outside of work (McCrady & Levine, 2009). Both self-reported and objectively measured sedentary time are risk factors for mortality, independent of moderate to vigorous physical activity (Koster et al., 2012; Matthews et al., 2012). Moreover, having a higher number of breaks in sedentary time is beneficially associated with metabolic parameters such as waist circumference, body mass index, triglycerides, and 2-hour plasma glucose (Owen, Healy, Matthews, & Dunstan, 2010). Thus, reducing sedentary time at work may promote improved employee health. The findings from this study suggest that the walking workstation has the potential for reducing sedentariness at work.
Based on a pilot study quantifying energy expenditure during 20 minutes of walking workstation use, Levine et al. hypothesized that 2.5 hours of walking during a workday would overcome a NEAT deficit of about 2,000 kcal/week (Levine & Miller, 2007). It has been suggested that physical exercise may not result in increased total energy expenditure, due to a compensatory reduction in NEAT (Colley et al., 2010; Rosenkilde et al., 2012; Thivel et al., 2014; Whybrow et al., 2008). The data presented in this study are in agreement with Colley et al., who suggested that incidental and light physical activity (thus increasing NEAT) may promote increased total physical activity, without compensatory reductions during other times of the day (Colley et al., 2010). Obesity is associated with decreased activity thermogenesis (Elbelt et al., 2010), specifically a decrease in NEAT (Levine et al., 2005). Fidgeting-like movements at very low work intensities are associated with substantial increases in energy expenditure (Levine et al., 2000). In humans, fat mass gain due to overfeeding is inversely correlated with changes in NEAT (Levine et al., 1999). Non-exercise activity thermogenesis is the most variable component of daily energy expenditure, varying by as much as 2,000 kcal/day and ranging from ~15% to 50% or more of total daily energy expenditure (Donahoo et al., 2004; Levine, 2007). As the “energy gap” required to explain the increased prevalence of obesity is only 100 to 200 kcal/day, a sustained small decrease in energy balance (by either decreasing intake or increasing energy expenditure) might be sufficient to prevent obesity (Ravussin, 2005). The data presented in this study suggest that 2.5 hours a day of moderate physical activity (walking slowly) is sufficient to promote a leaner phenotype and does not cause a compensatory decrease in total physical activity.
Furthermore, evaluation by participants did not describe a negative effect of this intervention on productivity, matching previous studies suggesting perceived beneficial effects in mood (Thompson et al., 2008) and lack of negative effects on work performance (Cox et al., 2011; Funk et al., 2012; Ohlinger et al., 2011; Straker et al., 2009; Thompson et al., 2008). The findings also suggest the use of walking workstations can be effective against weight gain and obesity without affecting productivity. More recent studies on cognitive effects of walking while working have had conflicting results, with data showing a modest reduction in total learning and typing performance in one study (Larson, LeCheminant, Hill, et al., 2015), versus no negative impact on cognitive performance in another study (Larson, LeCheminant, Carbine, et al., 2015). Given that there is no consensus in the literature on the cognitive effects, it may be that the gain from increasing physical activity takes more of a priority (Larson, LeCheminant, Carbine, et al., 2015; Larson, LeCheminant, Hill, et al., 2015; MacEwen, MacDonald, & Burr, 2015).
The finding that only 2 weeks of treadmill workstation yielded positive changes in body composition is suggestive that prolonged use would promote sustained increases in NEAT and alterations in body composition. Our results add to and extend the work of prospective long-term studies on the effects of walking workstations during work. A 9-month clinical trial targeting 12 sedentary overweight or obese office workers showed the walking workstation increased total physical activity, decreased sedentary time, and reduced waist and hip circumference, low-density lipoprotein (LDL), and total cholesterol (John et al., 2011). A 1-year intervention with 36 sedentary office workers reported an overall increase in total physical activity, decrease in sedentary time, and an average weight loss of 1.4 kg from baseline to study end, with greater weight loss (2.3 kg) in obese subjects (Koepp et al., 2013). A randomized controlled trial showed a significant increase in daily steps in subjects who used the treadmill desk during work over a 3-month period (Schuna et al., 2014). Another randomized crossover trial showed an increase in physical activity among physicians in a 12-week intervention period (Thompson, Koepp, & Levine, 2014). In the aforementioned studies, there was no prescribed or specified duration of walking workstation use per day, and energy expenditure was not measured. In contrast, the current study employed a specified treatment (2.5 hours/day). This information should inform future studies aimed at establishing the minimal conditions for successful interventions.
Recent reviews on this topic have identified knowledge gaps and the potential for further research. This includes effects on cognitive function, and long-term clinical outcomes (Tudor-Locke, Schuna, Frensham, & Proenca, 2014). A systematic review of 23 studies published in 2015 on the effect of standing and treadmill desks in the workplace concluded that the evidence was limited, but favored treadmill desks over standing desks. Only four studies measured energy expenditure using indirect calorimetry measures, none using double-labeled water and three of which found an increase of an average of 100 kcal while walking. Anthropometric data showed favoring higher lean/fat mass or a trend to weight loss. Effects on physiologic measures, work performance, and cognitive outcomes were mixed and insufficient to draw any conclusions (MacEwen et al., 2015).
A point of interest is that in the current study, all patients had a body mass index (BMI) >25. It would be instructive to examine whether different intensities and durations of low-intensity exercise can induce body weight loss and whether there are differences dependent on intrinsic subject characteristics, such as BMI, gender, and age. Taken together, the main conclusions of these long-term studies fit with the current study’s results in that moderate exercise is sufficient to cause positive changes in body composition and weight. However, the present study highlights that even short-term interventions aimed at increasing low-intensity physical activity can have a positive effect on body composition.
The present study had several strengths, including that it consisted of an intervention phase and a control phase, subjects served as their own control in a crossover design, and there was a predetermined duration of exercise; whereas, the small sample size was a study weakness.
In summary, this study showed that in sedentary office workers, the addition of walking for 2.5 hours per day has a beneficial effect on body composition and increases overall activity without an overall compensatory decrease in activity. We acknowledge that one barrier is implementation of this strategy in the workplace. Cost of installing treadmill desks and redesigning the work environment may be prohibitive to some employers. As discussed in detail in a paper by Tudor-Locke et al., there are many logistical challenges (including financial and administrative) facing employers with the implementation of walking workstations. This makes it more imperative to gather solid evidence that can be used in health education, to promote the use of these interventions in the work environments to help circumvent the epidemic of chronic diseases and sedentariness (Tudor-Locke, Hendrick, et al., 2014). Future prospective long-term studies comparing this intervention with a control group are needed to test the benefits of walking during work, especially on clinical outcomes such as body weight, body composition, blood pressure, serum lipids, and insulin sensitivity (World Health Organization, 2000).
Implications for Occupational Health Nursing Practice
This study supports the role of physical activity at the workplace in promoting employee health and wellness. A report by the Centers for Disease Control and Prevention (CDC) in 2011 concluded that occupational physical activity makes a “modest contribution” toward meeting the physical activity guidelines set for U.S adults (CDC, 2011). Thus, adding more physical activity at work can be effective in promoting a leaner body composition, which is expected to reduce the risks of weight gain, diabetes, and other chronic diseases. Occupational health nurses can use the evidence provided in the current study to motivate their workers to seek opportunities at work to move and reduce their sedentary time. Some work sites offer designated areas with treadmill desks, such as the site where this study was conducted. These areas should be used more often, using awareness campaigns or incentives offered by occupational health programs. Finally, a large health care system piloted “exercise as a vital sign,” in multiple clinics and found that obtaining exercise information during outpatient visits was indeed associated with significant changes in exercise-related processes in clinical care, such as exercise counseling and related referrals, which resulted in positive clinical outcomes (e.g., weight, blood glucose; Grant, Schmittdiel, Neugebauer, Uratsu, & Sternfeld, 2014). These findings should encourage the use of exercise as a vital sign by occupational nurses in all workplaces.
Applying Research to Practice
Since occupational physical activity has a “modest contribution” towards meeting the physical activity guidelines set for U.S adults (Centers for Disease Control and Prevention [CDC], 2011), adding activity at work can be effective in promoting a leaner phenotype, reducing the risks of weight gain, diabetes, which are leading causes of death in the United States. Thus, occupational health nurses can use the evidence provided in the current study to motivate their patients to seek opportunities at work, such as treadmill desks, to move and reduce their sedentary time. Occupational health nurses can use exercise as a vital sign, which has been found in recent studies to lead to significant changes in exercise counseling and positive clinical outcomes (e.g., weight, blood glucose; Grant, Schmittdiel, Neugebauer, Uratsu, & Sternfeld, 2014).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Samar Malaeb is an endocrinologist at the University of Minnesota, Minneapolis, MN, with a clinical and research focus in nutrition, obesity, and weight management. She also received her master’s degree in Nutrition Science and Policy from Tufts University’s Friedman School of Nutrition, Boston, MA.
Claudio Esteban Perez-Leighton received his PhD from the University of Minnesota in 2012 after receiving a Fulbright Scholarship. At the University of Minnesota, he studied under Dr. Catherine Kotz and Dr. Charles Billington focusing on neuronal mechanisms mediating resistance to obesity. He currently works as an Assistant Professor at Pontificia Universidad Catolica de Chile, where his focus is neuronal regulation and environmental influences on feeding behavior.
Emily E. Noble received her PhD in Nutritional Biochemistry from the University of Minnesota in 2014. She is currently a postdoctoral researcher at the University of Southern California, Los Angeles, CA, where she studies the neurobiological controls of food intake and body weight regulation.
Charles Billington is the director of the division of Endocrinology and Metabolism at the Minneapolis VA Health Care System. He is Professor of Medicine at the University of Minnesota, and hold a faculty position at the Department of Food Science and Nutrition, University of Minnesota. He is a leading clinical and research expert in obesity medicine. Nutrition, University of Minnesota. He is a leading clinical and research expert in obesity medicine.