
Abstract
Background. To maximize often limited resources for health promotion interventions, it is critical to identify and consult with the target population to inform program design and implementation. Objective. To highlight the value of scoping (identifying any barriers or limitations within a target population group) in the initial social marketing phase of targeting physical activity interventions for positive mental health. Method. Semistructured focus groups were undertaken in 2 segmented population groups: Study 1—adults (aged between 20 and 50 years) from a deprived community; Study 2—older adults (50+ years of age) attending physical activity groups. Discussions centered on health, mental health, physical activity, and methods of promotion. Results. Five focus groups were conducted, 2 in study 1 (n = 17; age 38.1 ± 10.8 years) and 3 in study 2 (n = 25; age 68.1 ± 5.6 years). Themes and perspectives were consistent within each case study, but differed between them, indicating that basic segmentation during recruitment (by age, area of residence, and physical activity participation) had identified 2 distinct audience segments. Differences between groups in perceived benefits of physical activity, preferred intervention type, and appropriate terminology provided valuable insight to inform physical activity promotion. Conclusion. Focus groups offer a simple and feasible means of scoping to begin to identify and understand population segments for targeting of health promotion efforts.
Social marketing is an approach that is increasingly used to promote positive behavior change of individuals and groups. 1 A set of social marketing national benchmark criteria 2 and a process model 3 have been developed to guide social marketing in the United Kingdom. The model includes a number of sequential phases: scope—develop—implement—evaluate— follow up. The initial “Scope” phase is designed to identify potential targeted audiences and explore any barriers and limitations to achievement, to identify any critical insights that will inform the “Development” phase, and identify key drivers of behavior among the target audience(s).
Health promotion continues to shift away from individual-orientated approaches, often operating at the community or neighborhood level.
This article reports the findings of the scoping phase for 2 case studies that aimed to gain insight into key messages for “selling” the benefits of physical activity, with an emphasis on understanding the mental health benefits. Physical activity interventions have often focused on physical benefits (eg, weight loss, cardiovascular risk factors).4,5 It is, therefore, important to understand how participants in these population groups perceive mental health and its relationship to physical activity so that different promotion methods and messages can be considered.
Health promotion continues to shift away from individual-orientated approaches, often operating at the community or neighborhood level.6,7 One advantage is the greater potential public health impact through reaching a larger number of people.7-9 The ability to tailor interventions is, however, reduced. Those implemented on a one size fits all basis are less likely to reach priority groups (ie, those with the greatest health need),10,11 which are often targeted by health promotion12,13 but tend to be difficult to engage in such programmes. 14 Therefore, further segmentation within these groups would be useful to enable more focused intervention 10 and maximize the often limited resources for health promotion programs.
Market or Audience Segmentation involves segmenting the potential target population into subgroups of those who share needs, wants, lifestyles, behavior, and values that make them likely to think alike and respond to health interventions similarly. 15 This helps, first, to identify the groups that can realistically be reached with the available resource and, second, to determine the best way of reaching the particular group(s). 10 In the United Kingdom, this concept has been embraced by the Department of Health and Sport England. They used quantitative data from the UK-wide Active People Survey 16 to create 19 population segments characterized by their sociodemographics and sport and active recreation preferences/behavior. 17 Attempting to apply character traits broadly across national samples is somewhat limited; as this article highlights, community-level interventions demand a degree of local knowledge.
Social marketing, which is increasingly popular in health promotion,1,15 relies on market (or audience) segmentation. 15 It is essentially a consumer-orientated approach that explores people’s wants and needs, 18 and in contrast to the one size fits all approach of program implementation, social marketing is “front loaded.” In-depth research is carried out prior to establishing any intervention to better understand and segment target groups. This “scoping” is seen as an essential precursor to the development of any behavior change intervention.
To be successful, health promotion programs often need to operate at a relatively local level and use the knowledge, needs, and wants of local people to drive program design and implementation. 19 Consistent with the social marketing approach, it is important to understand how population groups think, their motivation and priorities, and how they behave, to first segment the audience and then to understand how to target and design health promotion interventions. 20
By giving participants freedom to discuss their experiences, preferences, and opinions, qualitative data from focus groups can provide rich insight that is not obtainable through quantitative, closed questionnaire approaches.20,21 This can be invaluable in gaining local knowledge required for successful segmentation and targeting, despite the common problems of engaging with the so-called hard to reach groups.
To highlight the value of simple scoping through focus groups, we present findings from case studies of 2 population groups 22 that tend to have low levels of physical activity 23 and are often identified as priority groups for health and physical activity promotion12,24: middle-aged adults (age 38.1 ± 10.8 years) living in deprived communities and older people (age 68.1 ± 5.6 years). The aims of this scoping exercise were to (a) identify population segments that could feasibly be targeted for physical activity intervention, (b) increase understanding within these segmented populations that could be used to target physical activity campaigns, and (c) explore how physical activity could be promoted for its mental health benefits.
Methods
Participants
Study 1 involved adult residents of a deprived community in Staffordshire, United Kingdom, aged 20 to 50 years. Basic segmentation involved delimiting inclusion based on home postcode (and, therefore, area deprivation 25 ) and approximate age group aimed to avoid likely generational differences in experience and relevant issues in younger/older people, while ensuring that local issues could be discussed. Focus groups were segmented by gender. Study 2 involved older adults who attended physical activity groups within Staffordshire. Again this targeted recruitment was used to engender group homogeneity, but in terms of life stage and participation status.
Recruitment
Potential participants in study 1 were approached using a combination of door-to-door and random street stops, with a basic screening questionnaire to identify those eligible (aged 20-50 years and resident within defined postcode areas). Study 2 participants were initially approached by a physical activity group facilitator. Written consent was obtained for all participants, and the study was approved by the Staffordshire University ethics committee.
Focus Groups
Scoping involved focus groups, which provide a good forum for generating discussion 21 and a useful means of audience segmentation. 10 Semistructured discussions were facilitated by an experienced moderator using guide questions that covered a number of topics: understanding of relevant terms (health, mental health, and physical activity), their importance to participants, ideas for physical activity interventions, and appropriate messages and advertisement approaches. Discussions were recorded with contemporaneous notes taken by the moderator. Participants were also asked to complete a questionnaire providing basic demographic information and approximate physical activity levels using a single-item question. 26 Sample characteristics and key findings from each case study are presented with quotations to illustrate salient themes (Table 1).
Summary of Themes From Focus Group Discussion
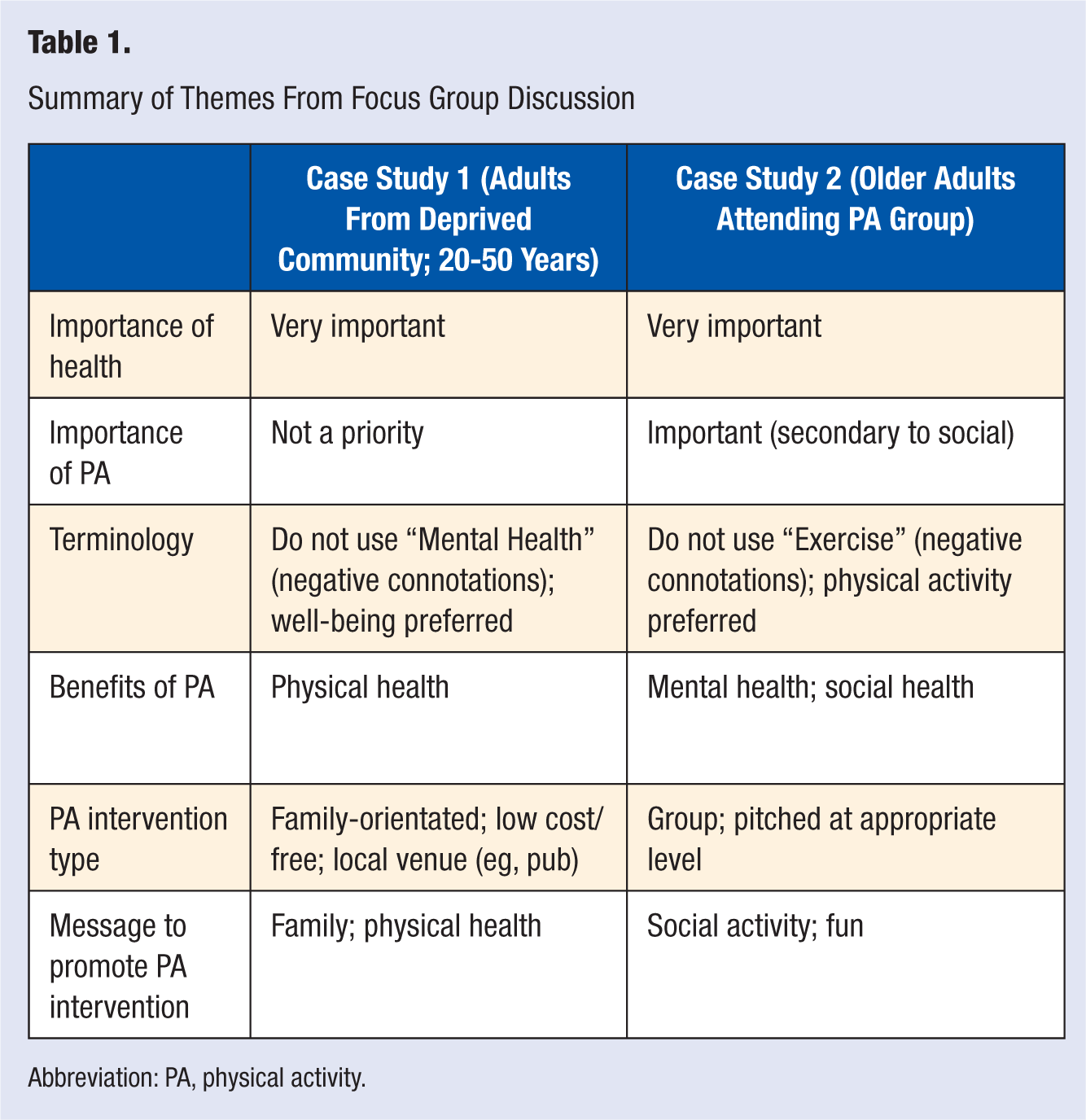
Abbreviation: PA, physical activity.
Qualitative data were transcribed verbatim and analyzed using thematic analysis. 27 Analysis was conducted using the 6 stages recommended 28 : becoming familiar with the data through extensive reading, generating preliminary codes, identifying themes, reviewing themes, naming themes, and finally writing the report. Two independent researchers coded the raw data and identified initial themes. These themes were then reviewed and agreed by both researchers.
Results
Study 1: Deprived Adult Population
Two focus groups, segmented by gender, were conducted with sedentary adults (10 females and 7 males) with an average age of 38.1 ± 10.8 years (range = 21.1-53.7 years). From participant postcodes, 85% of the participants lived in areas that fall within the bottom 10% for national rankings of the Index of Multiple Deprivation (IMD 2007), and the remainder lived in areas within the bottom 40%. 25 Consistent with deprivation, self-reported physical activity levels in men were low, with 88% (n = 7) reporting activity levels below recommended levels (ie, 30 minutes moderate–vigorous intensity activity on ≥5 days/week). 29 Although half of the female participants claimed to be active at recommended levels (n = 5), focus group discussions indicated that this was likely to be an overestimation. Only 2 out of the 10 women were in paid employment and all had children (1 woman with grandchildren), whereas 2 out of the 7 men reported being unemployed and 5 were parents.
From the discussion it was evident that participants’ lives centered on their local area, where they not only lived but also shopped and socialized and where their children attended school. The presence of crime, antisocial behavior, and tensions among different factions/individuals within the community were accepted as a part of normal everyday life: “A typical estate.” Yet the sense of a close knit community was also apparent among participants who saw it was a “family estate,” albeit one thought to lack local leisure services for parents and children.
Despite a range of ages within the focus groups, this commonality, which seemed to originate from residing in the same estate, led to consensus on most issues around mental health and physical activity within each focus group.
A number of key themes relating to mental health and physical activity emerged from focus group discussions. Health was important to all participants, particularly the health of children and family. The family was a fundamental aspect of participants’ lives and was regularly referred to as the primary concern: “Your kids are more important than yourself.” It was suggested that any physical activity intervention should emphasize general health benefits for children and families and should “something for the family to do.”
When questioned on the meaning of the term mental health, only negative connotations were identified. Both men and women made immediate links with “depression,” “mental illness,” “loonies on drink and drugs,” and “nutters.” Participants were eventually able to relate to positive mental health, but this required use of different terminology that centered on “well-being.” It was clear that using the term mental health in relation to potential physical activity benefits would be a deterrent to male and female participants. Different words and terms with more positive associations were preferred and considered more acceptable and easier for people to relate to their meaning, for example, mentally well, positive thinking.
Regular exercise and physical activity were positively associated with mental health, such as feeling better, feeling less stressed, and “a sense of achievement.” Participants referred to exercise as a way of “perking you up” and “getting you out of the house,” which was seen by some females as a place where they would eat and smoke more. Male participants spoke of going out for a walk or a run as a means of relief from their busy lives or “time out from the kids.”
A small number of participants were regularly active and most were not as active as they would have liked to be. All recognized both physical and mental health benefits of exercise/physical activities, but main motivators identified in relation to being more active were physical (not mental) health benefits, such as weight loss and general health improvement. Barriers to physical activity tended to be practical, centering on time, cost, and motivation: “I am lazy!” The time and financial constraints of work and/or family life seemed to dictate which physical activities would be appropriate for this population group:
By the time I finish my day and I get back, and then I’ve got to do the kids’ tea and put them to bed, I don’t have really much time, and by the time you have done that you are too knackered and you want to go to bed.
Only activities that were flexible and free or subsidized appealed, particularly to those with large families: “It is frustrating. You want to do things, but you just don’t have the time.”
In turn, when asked to consider the types of physical activity that could be incorporated into participants’ lives and how they would like to see it marketed, there was concordance that family-orientated activities would be most appropriate: “You should be able to do stuff with your children, because children get bored sitting at home all the time . . . and it is nice to do things with your children as well as do things by yourself.” Creating an activity suitable for children was desirable, separate from adults: “If the kids could do their bit and adults do something else” or “Something for the family to do.”
Consistent with cited barriers to physical activity, affordability and flexible timing were seen as key characteristics of potential interventions. Times would need to cater for both school and working hours. Although participants did not specify a maximum acceptable cost, the frequently mentioned question of “How much is it going to cost?” suggested that this would have a considerable impact on uptake and participation. Minimal cost, without joining or annual membership fees, and the possibility of free provision for children were thought to be imperative. There was, however, recognition that this would be somewhat dependent on the type of activity.
Locality was also thought important, with a strong preference for community-based physical activities and events. The community center was favored by female participants, but not by males who described it as “run down” and “not adequate.” The men felt that the pub was a more central community meeting point and had more space, therefore allowing for more possibilities.
Suggested methods for advertising of interventions included using the local press and radio, distribution of leaflets through local shops and schools, and word-of-mouth recommendation. The importance of local knowledge was highlighted through the general consensus that the local fish and chip shop was one of the best places to advertise and that the local pub was the best venue from which any physical activities should run. Neither may have been considered as sites for health promotion without this local insight.
In terms of marketing messages, participants believed that people ignored shocking stories and images related to health issues (eg, those used in national smoking cessation or drinking driving campaigns) given exposure to health problems and health damaging behaviors through the television and media: “When you see these pictures of like a heart or stuff like that of people who are smoking, it still doesn’t encourage you to stop smoking. They just don’t pay attention to it.” Rather, messages conveying the benefits of physical activity for mental health (eg, “self-confidence, feeling sexier, feeling proud of myself”) were thought more inspirational, as long as they were not “patronizing” or dictatorial (eg, stop smoking, eat healthily).
One aim of this scoping project was to ascertain the relative merits of promoting physical activity for its mental health benefits within a suitable local population segment. Physical rather than the mental health benefits were the main motivators for participants to undertake physical activity. Therefore, messages to attract adults from this community should be positive, focus on the physical rather than the mental benefits, and, most important, promote them as an opportunity for family/child-orientated activities.
Finally, key barriers related to perceptions of the prohibitive cost of other opportunities for active family pursuits, such as visiting the swimming pool, led participants to express the need for any physical activity intervention to be local and affordable, with partial or complete subsidy (eg, from local authority), particularly for children.
It was clear from both discussions that this was a close knit community. Despite evidence of problems in the area around antisocial behavior, crime, and reported tensions between groups or individuals, a sense of community and that everybody knew each other was articulated. Moreover, the commonality in themes and perceptions clearly related to participants’ circumstances. Factors such as residence on the same estate, prevalence of unemployment, and having to support families on low/modest income (and/or benefits) meant that the day-to-day issues faced by participants were similar. This indicated that the group assembled using basic geographic and demographic segmentation did represent a segment that would be similar in their motivations, deterrents, and behavioral responses to physical activity or health promotion efforts. In relation to physical activity programs aiming to improve mental health, regardless of the aim, the focus and associated messages for this population segment should be on family as a priority, physical health second, with due consideration to cost and locality.
Study 2: Older Adults
Three focus groups were conducted with 25 older adults attending physical activity groups in Staffordshire (17 females, 8 males). The mean sample age was 68.1 ± 5.6 years (range = 58.0-78.0 years). Postcode data revealed that participants resided in more affluent areas (compared with study 1); 22% lived in areas within bottom 40% for national rankings but almost half (44%) were from the top 20% least deprived areas. Despite being members of active ageing groups, more than three quarters of the participants reported being active below recommended levels (78%), a likely reflection of the age-related decline in physical activity.
Participants in these focus groups were generally familiar with one another, creating a relaxed atmosphere for the discussions in which many were keen to talk about physical activity. All participants were retired, although some reported involvement in voluntary work. Many participants, particularly women, had been widowed. Participants often traveled from nearby villages/towns to attend their groups and were more geographically disparate compared with those in study 1. As a segmented group, they appeared cohesive, with similar issues arising from each focus group.
A number of key themes emerged from discussions around mental health and physical activity that differed from study 1. The term health was discussed to understand what it meant to participants. They were keen to express the importance of health “without health you have nothing,” often emphasizing its signifigance in relation to aging: “You need to keep yourself healthy as you age so you don’t feel so old . . . through your diet, exercise, don’t smoke, don’t drink.” Health was considered essential for maintaining independence in later life, a major concern to most participants who cited examples of those who had poor health. When asked about “mental health,” some were initially drawn to discussing mental health problems such as dementia, depression, and loss of cognitive function or as a “freedom from anxiety or grief.” Participants were also concerned (particularly in the case of dementia) that it could affect people they described as “fit and healthy.” Generally, participants saw mental health as “mind agility, keeping the grey cells going” or as “feeling comfortable in your own skin, even as it wrinkles.”
All participants were able to identify both physical and mental health benefits of physical activity. In contrast to study 1, when asked about the general benefits of being physically active, participants focused on psychological (“being in a [physical activity group] gets you out of your depressions”) and social (“we meet people we didn’t know, it creates a community”) factors. Indeed, the mental health benefits were often associated with the social aspect the group: “the social interaction here helps keep me going,” “we have a laugh,” “you feel good and relaxed after and feel better because you’ve made the effort to come.” Physical benefits, such as being “more mobile,” were discussed, but given less credence.
A small number of participants raised concerns about the risks of physical activity and identified them as potential barriers to the inactive: “I have known some very fit people that have died recently. That doesn’t fit in with all the theory of doing lots of exercise.” Most acknowledged that if you “make sure you are within your own limits then you are not in danger.” A number of other barriers identified were practical, but most related to undertaking activities alone or the motivation to participate: “It’s a big step if you’re used to being on your own, it’s a big step to go and meet people” and “You just wouldn’t go on your own.” Attending a group alone was seen as the biggest potential barrier, but one that could be addressed through support: “People need the right encouragement; it can make a big difference.”
In keeping with this theme, the importance of the group was emphasized in relation to activity type: “You can walk alone, but it’s not nearly as much fun as in a group.” Having a group-based activity appeared as critical for this population group as a means of generating the social dimension and associated mental well-being benefits. For some people, meeting others also provided encouragement for sustained attendance: “If you weren’t meeting people at a certain time and place, then you just wouldn’t go.” In addition to tailoring activities to the age group, participants advocated careful consideration regarding the choice of individual leading the group: “I wouldn’t want a 20 year old man leading it.” For already active individuals, it was felt that an older person would be most appropriate: “They wouldn’t notice our lumps and bumps jiggling round as much as others might.”
Again, terminology appeared important, but in relation to “physical activity” rather than “mental health” (as in study 1). Participants discriminated between “physical activity,” which was seen as “everyday things” such as “gardening, walking, and housework,” and “exercise,” which participants associated with “a gym with all the machines, I’d hate that” or “a class like aerobics.” Given these negative connotations, some felt that using the term exercise would deter older adults who would associate it with younger, fitter people: “Young dolly birds who are lovely and trim seeing me being the size I am and not being able to do the exercises properly.” Although not the case with all participants, this distinction emerged as an important consideration for this population group, even those who are active: “People wouldn’t like it if it was pushed as exercise.”
Whereas family-related benefits of physical activity participation were most important in study 1, social aspects were most important for older participants. When asked what sort of words or phrases should be used when promoting physical activity, participants suggested “emphasizing the social side of it.” It was felt that the group should be promoted as a social group: “It’s the social that’s better” and “The exercise is secondary.” There was also consensus that fun aspect was important: “When you’re retired everything you do has got to be fun” and “Tell them it’s good fun!”
Also in contrast to study 1, mental health benefits of physical activity were thought more important than physical benefits. Maintaining a good level of cognitive function was key and, for this population group, a good way to promote physical activity.
There was clear commonality among the participants. Despite attending physical activity groups in different locations, the similarity in age, motivation, and attitude toward physical activity meant that even basic targeting used for focus group recruitment resulted in a useful audience segment. From a public health perspective, older people who are already engaged in physical activity programs are unlikely to be the primary target for health promotion. Discussion with this group did, however, provide valuable insight into appropriate terminology to sell the benefits of physical activity for positive mental health.
Discussion
We used geographic and demographic segmentation to identify 2 distinct population groups: older adults (from more affluent areas) engaged in physical activity programs and young-to-middle-aged adults from a deprived community who did not participate in a physical activity program. Through focus group discussions, issues around health, mental health, physical activity, and related perspectives, priorities, motivations, and barriers were explored for each group. This gave valuable insight into whether they represented a tangible population segment that could reasonably be targeted for physical activity programs.
Findings from the case studies highlight the importance of initial scoping using basic segmentation and emphasized that insight can be gained through a simple scoping exercise. Focus groups not only identified that these represented distinct segments who tend to think and be motivated (or deterred) similarly (with respect to health and activity) but also identified that the nature of interventions and the messages used to promote physical activity to these groups differed markedly (Table 1).
Epidemiological data consistently demonstrate social trends in health, health behavior, and associated attitudes.23,30-33 For health promotion to successfully engage with people in their local community or neighborhood, however, scoping and consultation are necessary to understand target populations in that locality. The recent resurgence of interest in social marketing is evidence of growing recognition that both developing a greater understanding of the target population group and gaining local knowledge are critical to intervention success and effective marketing. 19
Involving the target population and using their local knowledge is important at all stages of a project, from consultation/scoping, to design, implementation, and evaluation. The findings presented highlight perspectives specific to the different groups that might not otherwise have been realized, especially in study 1. Scoping can, therefore, usefully inform program design. Moreover, if participants involved in such consultation could remain engaged in the design (and implementation) process, feelings of empowerment and ownership over the program could also promote sustainability. 7
The fairly modest resource necessary to undertake such scoping focus groups should make them a feasible inclusion in the design stage of any community health or physical activity promotion program. To ensure that the views of the target population can be ascertained, it is advisable to consider the allocation of adequate resource to the recruitment and, where appropriate, incentivized attendance at focus groups.
Finally, it is important to consider the order of events for the funding, design, and implementation of health promotion programs. Funding for public health interventions and related health research is often limited (relative to other areas of the health service and medical research). Therefore, calculating and justifying their cost is a challenging but important process, and funders understandably want to know where the money will be spent. There is a good argument, especially from a social marketing perspective, that consultation should drive design 34 ; that is, decision about the nature of an intervention should not precede adequate consultation and scoping. It is, therefore, important to make the case for adequately resourced consultation rather than implementing a predetermined intervention in a population for whom it might not be appropriate.
Conclusion
Scoping through focus groups offers a simple and feasible means of identifying and understanding target populations for health promotion. The need to maximize often limited resources mean that consultation with the target population is essential to understanding how resources are best used and make the most of existing local knowledge.
Footnotes
Acknowledgements
The authors would like to acknowledge the SMS marketing for their assistance in data collection, Dr Ray Lowry (University of Newcastle upon Tyne), Kate O’Hara (Program Specialist—Service Development, NHS West Midlands), Suzanne Gardener (Regional Physical Activity and Sport Coordinator, PAN WM), Age Concern, and all participants.