
Abstract
Mindfulness training, which teaches individuals to bring awareness and acceptance to the present moment, has been effective in improving the well-being of health care workers. Limited research examines the adoption of mindfulness practices using health behavior theories. The current study sought to conceptualize hospital health care workers’ experiences in adopting mindfulness practices using the Health Belief Model (HBM), a theoretical framework used by health promotion practitioners to design and implement health behavior change interventions. Hospital health care workers in Colorado participated in an 8-week Mindfulness-Based Stress Reduction (MBSR) course. Participants (n = 19) answered open-ended questions about their experiences adopting mindfulness practices. A theory-driven thematic analysis approach was used to analyze data with key constructs of the HBM acting as the framework for the analysis. Results showed that HBM constructs, including internal cues to action, perceived benefits and barriers, and self-efficacy, helped portray the participants’ experiences and challenges in adopting and adhering to the mindfulness practices taught in the MBSR course.
Keywords
Introduction
Occupational health and safety among health care workers is a critical public health issue. The National Institute for Occupational Safety and Health (NIOSH; 2009) identifies the health care sector as a high-risk industry due to numerous job hazards including high levels of job stress, workplace violence, musculoskeletal disorders, and exposures to needle sticks and other sharp instruments. Many health care workers also experience high levels of mental and emotional distress that can lead to burnout, depression, substance abuse, and suicide (Wallace, Lemaire, & Ghali, 2009) and affect patient care and safety (Charney & Schirmer, 2007; Wallace et al., 2009; Yassi & Hancock, 2005). Mindfulness training has been increasingly used with success to decrease stress and promote health and well-being among health care workers (Burton, Burgess, Dean, Koutsopoulou, Hugh-Jones, 2017; Cohen-Katz, Wiley, Capuano, Baker, & Shapiro, 2004; Duchemin, Steinberg, Marks, Vanover, & Klatt, 2015; Fortney, Luchterhand, Zakletskaia, Zgierska, & Rakel, 2013; Geary & Rosenthal, 2011; Goodman & Schorling, 2012; Irving, Dobkin, & Park, 2009; Lamothe, Rondeau, Malboeuf-Hurtubise, Duval, & Sultan, 2016; Shapiro, Astin, Bishop, & Cordova, 2005).
Mindfulness Interventions Among Health Care Workers
Mindfulness training teaches participants skills and practices that increase their ability to attain nonjudgmental awareness in the present moment (Kabat-Zinn, 1990). Mindfulness training has been used as a workplace wellness promotion intervention strategy that improves attention, which in turn positively impacts cognition, emotion, behavior, and physiology with positive implications for workplace outcomes, including performance, relationship quality, and worker safety and well-being (Burton et al., 2017; Good et al., 2015).
Research on mindfulness training among health care workers suggests that mindfulness training leads to significant reductions in mental health outcomes including perceived stress, anxiety, depression, and burnout (Burton et al., 2017; Fortney et al., 2013; Irving et al., 2009; Warnecke, Ogden, Bentley, & Nelson, 2017). Mindfulness-based stress reduction (MBSR) programs, considered the gold standard of secular mindfulness training programs, have successfully improved physical and mental health outcomes among health care workers (Burton et al., 2017; Cohen-Katz et al., 2004; Geary & Rosenthal, 2011; Goodman & Schorling, 2012; Irving et al., 2009; Lamothe et al., 2016; Shapiro et al., 2005).
The MBSR program was created at the University of Massachusetts School of Medicine. It was initially used to treat chronic pain patients and since then has been used to train a variety of populations, including health care providers, to adopt mindfulness practices (Kabat-Zinn, 1990, 2003). MBSR training typically consists of weekly group sessions and one full-day silent retreat session over the course of 8 weeks.
Several limitations exist, however, within the literature examining the impact of MBSR programs on health care provider occupational health and safety. As reviews of mindfulness studies among health care professionals and within the workplace argue, extant research fails to identify contextual factors that are critical for understanding how and why mindfulness interventions work, as well as how results may differ by population and setting (Burton et al., 2017; Good et al., 2015; Irving et al., 2009). Similarly, the studies on the effect of mindfulness training programs on health care worker stress and well-being have not used established theoretical frameworks to design the programs and they pay limited attention to the mechanisms of change behind the programs’ effectiveness (Burton et al., 2017). Using a theoretical model can help target specific improvements in health behavior change intervention design (Glanz, Rimer, & Viswanath, 2008) and help health promotion practitioners tailor mindfulness training to fit the needs of health care providers.
Recent qualitative research on mindfulness training among health care workers has begun to examine the process of change among participants and the challenges health care workers face during mindfulness training (Irving et al., 2014; Mensah & Anderson, 2015; Morgan, Simpson, & Smith, 2015). Some of the barriers reported in the qualitative studies included logistical issues such as limited time due to demanding work schedules and responsibilities outside of work and psychological challenges to prioritizing self-care as their professional training and work focused on caring for others (Morgan et al., 2015). Key facilitators to increasing health care worker engagement in mind–body programs included presenting the evidence that supports the efficacy of the programs and gaining financial assistance and support from organizational leaders (Mensah & Anderson, 2015). However, these findings have not previously been placed within the context of established theories of health behavior.
Health Belief Model (HBM)
The Health Belief Model (Becker, 1974), developed to understand why certain people did not participate in health prevention practices, has been used to help explain and predict the adoption of a variety of preventive and treatment health behaviors (Glanz et al., 2008). According to the HBM, see Figure 1, individuals will be prompted to consider adopting a protective health behavior when they perceive a threat of a preventable health condition. The level of the perceived threat of the health condition varies by beliefs about the severity of its consequences and individuals’ susceptibility to the condition. The likelihood of adopting the preventive health behavior increases when the perceived benefits of adopting the health behavior outweigh the barriers to adopting it and when the individuals believe that they have high self-efficacy, believing they can successfully adopt the health behavior. Individual characteristics, such as age, sex, or education, may modify these perceptions that influence behavior change.
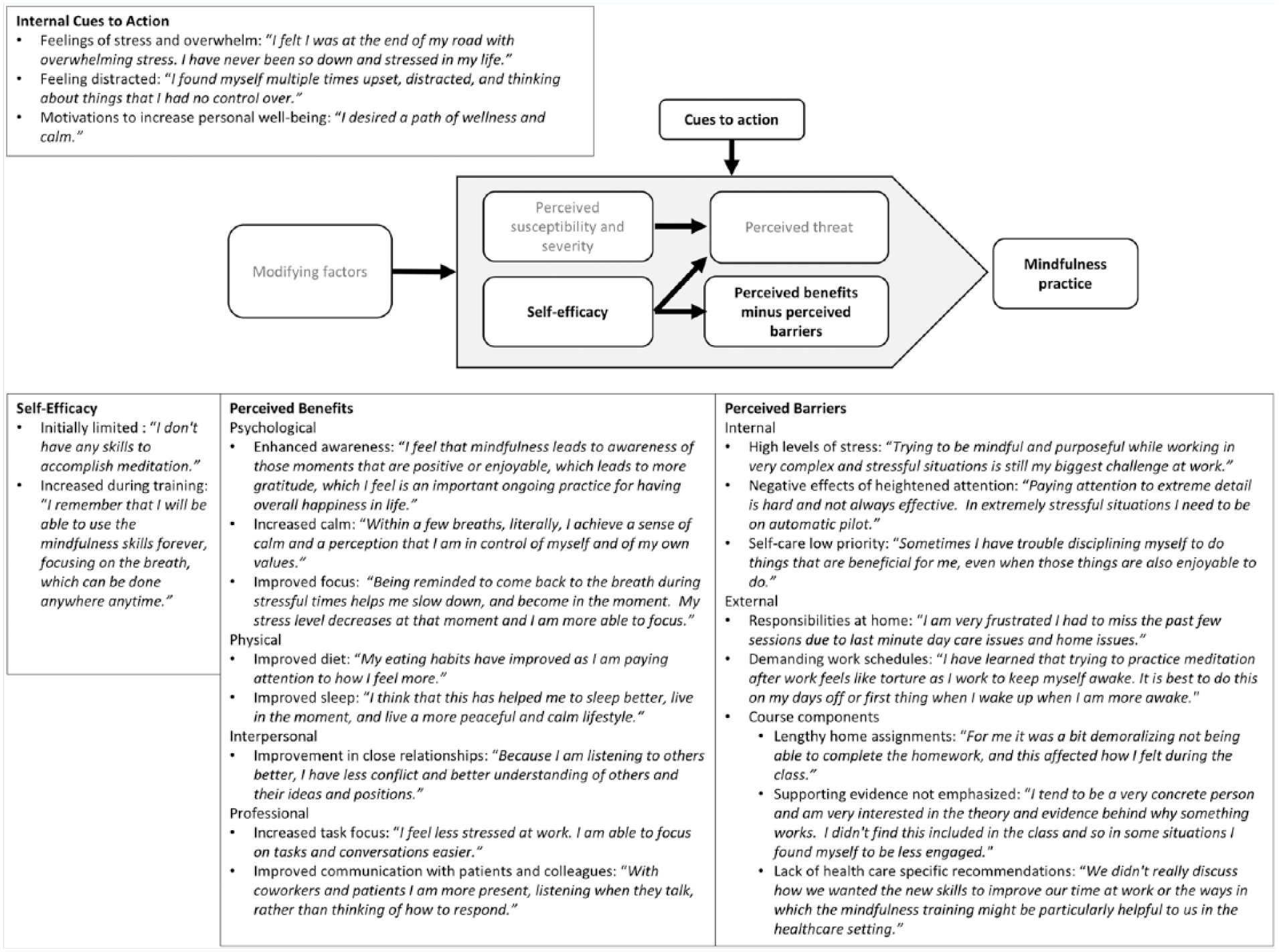
Themes and subthemes of relevant Health Belief Model constructions with illustrative quotes from study participants.
Evidence regarding the predictive validity of the HBM is mixed (Linke, Robinson, & Pekmezi, 2013). However, research shows that the model is valuable for explaining the adoption of preventive health behaviors and designing interventions that target specific health behaviors (Harrison, Mullen, & Green, 1992; Janz & Becker, 1984; Linke et al., 2013). As such, the HBM may offer a useful theoretical framework for understanding the factors that increase health care workers’ likelihood of adopting mindfulness practice as a preventive health behavior, which in turn can help health promotion practitioners tailor and design interventions to promote mindfulness practices among health care workers.
Purpose
The present study aimed to use the HBM to understand what changes might be needed to improve mindfulness training to increase the adoption and adherence to mindfulness practices among health care workers.
Method
Participants and Procedures
Participants included health care workers from direct patient care units in two hospitals in Colorado. In 2014, participants were recruited as part of a larger study that used a randomized waitlist controlled trial to examine the effects of mindfulness training on health care worker safety (findings on safety outcomes are published separately, see Valley & Stallones, 2017). Using a computer-generated list of random numbers, participants were randomly assigned to participate in the first 8-week MBSR course or the waitlist control group. The waitlist control group started the 8-week MBSR course after the first group completed the course. Both courses were taught by the same experienced physician instructor in 2014 adhering to the MBSR standards of practice (Santorelli, 2014). The course included eight 2.5-hour weekly sessions and one silent 7-hour group retreat. Core components of the course included informal (e.g., awareness of pleasant and unpleasant sensations) and formal (e.g., hatha yoga, body scans, sitting and walking meditations) mindfulness meditation focusing on bodily sensations, didactic presentations on topics such as the physiology of stress, group discussions about the skills learned in the class and their impact on participants’ attitudes and awareness of experiences. The participants attended the course at a local yoga and fitness organization outside of work hours. At the silent retreat, participants met as a group to practice formal mindfulness meditation and personal reflection in silence. The participants were asked to complete home assignments that included relevant readings and time practicing the skills learned in the course.
Qualitative data were collected from participants using open-ended questions in weekly logs, a posttraining survey, and a 6-month follow-up survey. Open-ended questions in the weekly logs and study surveys asked participants to describe (a) their experiences in the MBSR course, (b) factors that helped or prevented them from using the mindfulness practices taught in the course, (c) changes in their life and role as a health care worker stemming from mindfulness practices, and (d) intentions to continue to use the mindfulness practices taught in the course. The 6-month follow-up survey asked participants whether they had continued to use the mindfulness practices they learned in the course.
Participants received the MBSR course free of charge and received US$25 gift cards as a token of appreciation for completing study questionnaires. The University of Colorado Health Poudre Valley Hospital and Colorado State University Institutional Review Boards reviewed and approved the study.
Data Analysis
Demographic characteristics of participants were summarized using descriptive statistics. Adherence was described using proportions of the participants who reported that they completed home assignments each week, attendance at the nine sessions, and self-reported continued practice of the skills learned in the course 6 months after the course.
Thematic analysis
The present study used a theory-driven thematic analysis approach to analyze the qualitative data with the key constructs of the HBM, see Figure 1, used as the framework for the analysis. The key constructs of HBM (Becker, 1974) include a person’s beliefs about (a) the likelihood of getting a health condition (perceived susceptibility), (b) the seriousness of the condition (perceived severity), (c) the benefits of the health behavior (perceived benefits), (d) the barriers to enacting the health behavior or the negative consequences of the behavior (perceived barriers), (e) internal or external factors that prompt behavior change (cues to action), and (f) one’s ability to successfully enact the health behavior (self-efficacy).
The qualitative analysis was conducted by two researchers using NVivo Version 11.3.2 (QSR International, 2015) to code the data. Analysis occurred in six steps, following the guide provided by Braun and Clarke (2006). First, the coders became familiar with the data by compiling the participants’ open-ended responses to the weekly logs and surveys. The coders read the responses several times and made preliminary notes about possible relations to the constructs of the HBM. Second, the research team generated initial codes throughout the data. Third, the codes were reviewed for potential themes under each of the constructs of the HBM. Fourth, the research team reviewed the themes to ensure that the codes fit within the themes and that the themes fit within the structure of the HBM. Fifth, the themes were named, defined, and refined. Finally, the primary author related the themes and codes back to the study aims during the process of manuscript preparation.
Results
Participants
Of the initial 19 participants, 17 completed weekly logs and the postsurvey (10 from the first group and seven from the second group), and 16 completed the 6-month follow-up survey. Of the 17 participants who completed the weekly logs and postsurvey, most (88%) were female and nurses (registered nurses [RNs] or nurse practitioner [NPs]). Two of the participants (12%) were paramedics. The participants ages ranged from 24 to 60 years (median = 46 years). Less than one third (29%) of participants had previous experience practicing mindfulness meditation, and of those with meditation experience, only two participants had practiced mindfulness meditation in the month prior to beginning the MBSR course.
Adherence and Sustained Use of Mindfulness Skills
Of the 17 participants who completed the postsurvey, five (29%) attended all nine sessions, six (35%) attended eight of the nine sessions, four (24%) attended seven of the nine sessions, one (6%) completed five of the nine sessions, and one (6%) attended only four of the nine sessions. Although all of the participants reported doing a portion of the home assignments each week, none of the participants reported that they completed all of the home assignments during the course. Of the 16 participants who completed the 6-month follow-up survey, 14 (88%) reported that they still used some of the skills they learned in the course.
Findings Based on the HBM
The themes derived under the HBM constructs are listed in Figure 1, which includes illustrative quotes from participants for each theme and subtheme. No themes emerged from the data related to perceived susceptibility, perceived severity, or perceived threat. Although many of the participants described their levels of stress and feelings of being overwhelmed, these descriptions did not directly relate to their beliefs about the likelihood of having stress (perceived susceptibility) or the severity of the consequences of stress (perceived severity). Instead, participant responses describing their stress levels seemed more relevant to cues to action themes.
Cues to action
Only internal cues to action and no external cues to action emerged from the data. The participants described internal factors that prompted their decision to adopt mindfulness practices related to stress, distraction, and motivations to increase personal well-being.
Perceived benefits
Participant responses related to perceived benefits of using mindfulness practices learned in the MBSR course fell under four themes: (a) psychological benefits, (b) physical benefits, (c) interpersonal benefits, and (d) professional benefits. The psychological benefits participants experienced from the MBSR course and the mindfulness practices included enhanced awareness, increased calm, and an improved ability to focus. Participants described how adopting mindfulness practices led them to pay more attention to themselves and their surroundings. Many participants described how their heightened awareness led to a cascade of positive effects. The psychological and interpersonal benefits participants described transferred into their professional roles as health care workers where they experienced increased task focus and improved interactions with colleagues and patients.
Perceived barriers
Participants described numerous barriers to their successful adoption of mindfulness practices during the MBSR course and after they completed it. Internal barriers included difficulties with enhanced attention, high levels of stress, and a lack of prioritization of self-care. Although participants largely agreed that their enhanced attention due to mindfulness practice had positive effects, several participants also described how heightened attention sometimes felt like a barrier to their continued mindfulness practice as well as to their daily functioning. These participants said that they did not always want to have deliberate and focused attention. Another major internal barrier was their struggle to prioritize self-care. Participants often framed their discussion of this barrier in terms of their lack of discipline or need for greater diligence.
The prioritization and use of time for self-care practices was a major internal barrier that related to two of the external barriers that the participants faced—responsibilities at home and demanding work schedules. Given the demanding schedules that many of the participants had at the hospital and at home, participants found the scheduling and timing of the course challenging.
Other external barriers included certain course components, such as the home assignments and the content of the group discussion. Overall, participants agreed that they liked learning most of the formal mindful meditation practices (e.g., mindful walking, sitting meditation, hatha yoga) taught in the course. However, the lengthy home assignments acted as barriers to their successful adoption of mindfulness practices, and conflicted with their demanding work schedules. Although the home assignments varied each week, most assignments asked the participants to practice formal mindfulness meditation approximately 1 hour per day in addition to reading materials and making notes on their experiences throughout the week.
Additional barriers described by the participants included (a) the lack of group discussion on how to apply mindfulness skills in the health care setting and (b) the lack of emphasis on scientific evidence supporting the efficacy of mindfulness training. Although the course instructor provided articles reviewing the research on mindfulness during the first session of the MBSR course, the evidence was not discussed in detail with the participants. Participants stated that thoroughly presenting supporting evidence is especially important among health care workers given their foundation in evidence-based medical training and health care practices.
Self-efficacy
The theme of self-efficacy arose from the data collected in the weekly logs. The participants’ self-efficacy seemed to increase as the MBSR course progressed. Early in the course, several participants described how they felt that they did not have the ability to effectively adopt mindfulness practices. Later in the course, participants described how they felt more confident in using the different formal mindfulness meditation practices taught in the MBSR course. They described how they had learned that mindfulness tools are continually accessible, which increased their self-efficacy.
Discussion
The current study sought to conceptualize hospital health care workers’ experiences in adopting mindfulness practices using the HBM, a theoretical framework used by health promotion practitioners to design and implement health behavior change interventions. Themes related to the perceived severity, perceived susceptibility, and perceived threat constructs of the HBM did not emerge from the data. This may be due to health care workers’ use of denial and avoidance as coping strategies as well as their tendency to remain silent about personal health issues that have been well documented (Arnetz, 2001; Baldisseri, 2007; Firth-Cozens, 2001; Wallace et al., 2009). It may also be that these constructs within the HBM do not apply to health practitioners who adopted mindfulness practices to promote general well-being rather than to prevent a specific health condition.
The thematic analysis showed that the other HBM constructs, including internal cues to action, perceived benefits and barriers, and self-efficacy, helped portray the participants’ experiences and challenges in adopting and adhering to the mindfulness practices taught in the MBSR course. The benefits of mindfulness practice that participants described are similar to the process of change laid out by Irving et al. (2014).
Consistent with previous research (Mensah & Anderson, 2015; Morgan et al., 2015), participants described major barriers to adopting mindfulness practices including competing demands of work schedules and home responsibilities. The participants felt that the MBSR course home assignments were not tailored to their schedules and were too time-intensive. Additional course-related barriers participants cited included limited presentation of the evidence behind the program and a lack of discussion about tactics aimed at incorporating mindfulness at work in health care settings.
These findings suggest that health promotion practitioners who aim to reduce stress and promote well-being among health care workers can use constructs of the HBM to understand the most salient factors that encourage or discourage participants from adopting mindfulness practices. The HBM construct of perceived barriers to adoption in this study suggest that changes are needed to improve the effectiveness of mindfulness interventions among health care workers. Specifically, the trainings need to align the course timing and materials with health care workers’ demanding schedules and provide evidence substantiating mindfulness practices along with recommendations for mindfulness practices appropriate to health care workspaces.
This study has several important limitations. The sample included a small number of hospital health care workers from a single hospital system. The qualitative data were collected using open-ended questions in a series of surveys. Although participants provided examples of their experiences in their responses, the research team did not have an opportunity to ask participants for additional explanation or narrative examples or probe deeper into themes that emerged as researchers do when using other qualitative methods such as focus groups and in-person interviews.
The participants self-selected into the MBSR course as part of a larger study on mindfulness and health care safety. The study’s findings on participants’ experiences in adopting and adhering to mindfulness practices taught in the MBSR training were shaped by their motivations and willingness to participate in the study and may not generalize to other health care workers. The MBSR program, initially designed for chronic pain patients who received the training in a medical setting (Kabat-Zinn, 2003), was not tailored for health care workers in the current study for the sake of maintaining the fidelity of the evidence-based course for the larger study on health care safety. Recent work has started to examine the effectiveness of mindfulness training modified specifically for health care workers. Although these modified mindfulness programs have led to improvements in providers’ mental health (Burton et al., 2017; Fortney et al., 2013), their participants, like those in the current study, reported scheduling conflicts and difficulties with the time-intensiveness of the training. The modified mindfulness training programs were not designed using theoretical frameworks (Burton et al., 2017), and further support the need for using theoretical foundations that can improve interventions’ efficacy and feasibility among health care workers.
Implications for Practice
The study’s findings highlight the benefits of mindfulness practice among health care workers, which included enhanced awareness and improvements in social relationships and interactions with patients and colleagues. Results suggest that health promotion practitioners who aim to provide mindfulness training to health care workers may improve adoption and adherence to mindfulness practices by tailoring the course timing and materials to fit the health care workers’ demanding schedules. Didactic materials and group discussions should thoroughly explain the growing body of evidence that supports the use of mindfulness practices in health care and provide practical, health care–specific applications of mindfulness practices. Viewed within the context of the HBM, these qualitative findings may help practitioners design and tailor workplace mindfulness programs to fit the needs of health care workers.
As research continues to explore the impact that mindfulness training has on health care workers’ occupational health and safety and ultimately patient care, the field could be advanced by researchers expanding their use of health behavior models and theoretical frameworks in examining how and why mindfulness interventions work as well as how results may differ by population and setting. Future research can build off of the present study’s findings to help health promotion practitioners tailor mindfulness training to fit the needs and schedules of health care workers.
Applying Research to Practice
A growing body of research indicates that mindfulness training can improve health care workers’ well-being (Burton et al., 2017; Duchemin et al., 2015; Fortney et al., 2013; Lamothe et al., 2016), which has far-reaching consequences for the health and well-being of health care workers and the quality of care of their patients (Charney & Schirmer, 2007; Yassi & Hancock, 2005). Health promotion practitioners who aim to provide mindfulness training to health care workers should tailor the course timing and materials to fit the health care workers’ demanding schedules. Training materials should thoroughly explain the growing body of evidence that supports the use of mindfulness practices in health care and provide practical, health care–specific applications of mindfulness practices.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was partially funded by the Colorado Injury Control Research Foundation at Colorado State University and a small grant from National Institute for Occupational Safety and Health (NIOSH) through the Mountain & Plains Education and Research Center.
Author Biographies
Morgan Valley, MPH, PhD, an occupational healthy psychologist by training, is an evaluator at Vantage Evaluation. She previously worked with Lorann Stallones to research and evaluate community and workplace health and safety programs.
Lorann Stallones, MPH, PhD, an epidemiologist by training, is a professor in the Applied Social and Health Program of the Department of Psychology at Colorado State University and director of the Graduate Degree Program in Public Health of the Colorado School of Public Health at Colorado State University. She has extensive experience in research related to health promotion, disease prevention, and public health program evaluation in workplace health and safety.