
Abstract
Obstructive sleep apnea (OSA) is a chronic condition characterized by occlusion of the upper airway during sleep resulting in daytime sleepiness. Drivers with OSA are at a two- to sevenfold increase in risk of motor vehicle crashes (MVCs). Approximately, 13% to 28% of commercial motor vehicle drivers (CMVDs) are thought to have OSA. Obstructive sleep apnea is a significant issue in the transportation industry. Currently, The Federal Motor Carrier Safety Association (FMCSA) does not mandate OSA screening. Federal regulations only specify that CMVDs be free of “respiratory dysfunction” that would impair driving. Untreated OSA is a public safety concern. The purpose of this article is to use Bardach’s eightfold policy analysis approach to examine policy options related to OSA screening in the trucking industry.
Keywords
Obstructive sleep apnea (OSA), safety, and mandatory OSA screening in the trucking industry have garnered much discussion. After several years of contentious debate among regulatory, advocacy, and key stakeholders, in October 2013, President Obama signed into law a bill requiring that any federal standards and federally mandated screening, testing, and treatment of OSA among commercial truck drivers (CMVDs) be set forth through formal rulemaking, rather than a guidance process (Public Law 113-45, 2013). The regulatory process, through formal rulemaking, began on March 10, 2016, with the Federal Motor Carrier Safety Administration (FMCSA) and Federal Railroad Administration (FRA) issuing an Advanced Notice of Proposed Rulemaking regarding moderate and severe OSA among individuals in safety-sensitive positions in highway and railroad transportation (Darling & Feinberg, 2016; Minor & Lauby, 2016). In an unexpected turn of events, the FMCSA and FRA announced that the OSA proposed rule was rescinded as of August 2017 (FMCSA, 2017a). Although the FMCSA is not seeking to establish federal regulations regarding OSA screening and treatment, OSA remains a significant safety issue in the trucking sector. The purpose of this article is to use Bardach’s (2012) eightfold policy analysis to analyze mandatory OSA screening policy options in the trucking industry.
Bardach’s Eightfold Policy Analysis Path
Bardach’s (2012) eightfold path to policy analysis (Figure 1) is a straightforward, concrete method of analyzing public policy. The process includes eight steps that guide the analysis from delineating the problem to sharing the policy narrative. The critical first step is to define the problem. Identifying the problem supports the need for conducting the analysis and provides direction for gathering supporting data. After defining the problem, the next step is assembling evidence related to the problem. Three main purposes guide data collection: (a) assessing the extent and nature of the problem, (b) assessing the current policy climate, and (c) examining policies from other locales similar to the problem under study.
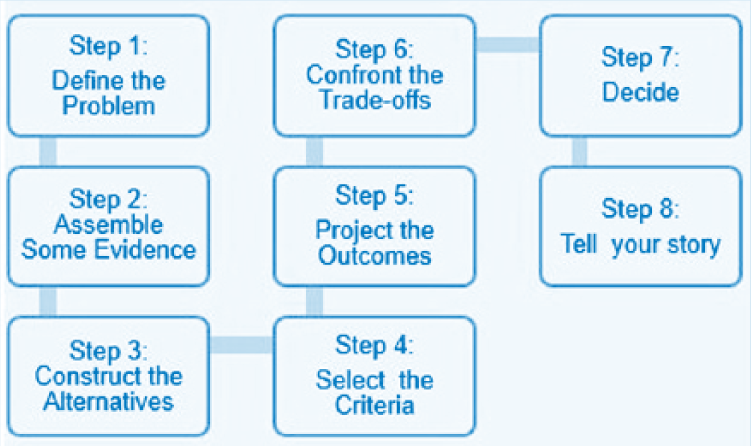
Bardach’s eightfold path to policy analysis.
The next step is to identify or construct alternative strategies, policy options, or interventions. Work within this step begins with a broad approach and then concentrates on two to three main alternatives. The fourth step is primarily focused on evaluation. Through this step, values and philosophy are applied to judgments about projected outcomes. The most important evaluation measure examines whether the proposed outcomes will adequately solve the problem.
Often identified as the hardest step in the process, Step 5 involves projecting realistic future outcomes. After projected outcomes are identified, the sixth step is to consider strengths and limitations. In some cases, one outcome is obviously best, but generally this is not the case and trade-offs between outcomes must be explicated. In Step 7, after all evidence, alternatives, evaluation measures, outcomes, and trade-offs have been appraised, the best approach for addressing the problem must be chosen. The eighth and final step is sharing the analysis with interested audiences and stakeholders. The analysis should be presented so that both lay and professional audiences can understand the implications. This policy analysis is presented using the organizing framework of the Bardach eightfold path.
Step 1: Define the Problem
Obstructive sleep apnea is a condition characterized by collapse of upper airway soft tissues and obstruction, resulting in episodes of apnea and hypopnea during sleep (Sanchez-de-la-Torre, Campos-Rodriguez, & Barbe, 2013). These episodes are associated with frequent arousals and subsequent fragmented, nonrestorative sleep (Stone, Taylor, McCrae, Kalsekar, & Lichstein, 2008). Drivers with OSA frequently experience residual sleepiness that may be related to such factors as hypoxia (Feng, Wu, Zhang, & Chen, 2012), primary sleep insufficiency (Al Lawati, Patel, & Ayas, 2009), inadequate treatment (Mulgrew et al., 2010), comorbid conditions, such as depression (Wheaton, Perry, Chapman, & Croft, 2012), and periodic leg movement and restless leg syndrome (Roux, 2013). Along with residual sleepiness, negative effects on cognition have been noted in individuals with OSA and respond to some extent to continuous positive airway pressure (CPAP) treatment. Among the noteworthy cognitive effects associated with OSA are attention, vigilance, and visual-spatial declines (Ferini-Strambi, Marelli, Galbiati, & Castronovo, 2013), all of which may affect driving safety. The condition often goes undetected because many signs and symptoms are evident only during sleep (Sanchez-de-la-Torre et al., 2013), and daytime symptoms such as sleepiness and cognitive performance declines may not be readily recognized or may be associated with other conditions or circumstances. Drivers with OSA are at increased risk of motor vehicle crashes (MVCs; Mulgrew et al., 2008; Shiomi et al., 2002). A systematic review and meta-analysis of OSA-related MVC risk in commercial drivers indicated that commercial drivers with OSA had a two-fold higher MVC rate per mile than commercial drivers without OSA diagnoses (Tregear, Reston, Schoelles, & Phillips, 2009). Obstructive sleep apnea prevalence among CMVDs is estimated to range from 13% to 28% (Berger et al., 2012; Gurubhagavatula, Maislin, Nkwuo, & Pack, 2004; Talmage, Hudson, Hegmann, & Thiese, 2008). OSA has been cited as a significant issue among commercial motor vehicle drivers (CMVDs; Kales & Straubel, 2014).
Step 2: Assemble Evidence
Concern regarding CMV crashes and public safety raises the issue of whether OSA screening among CMVDs should be mandatory. Motor vehicle crashes involving CMVDs are costly in terms of human capital, property loss, and litigation. In 2015, 116,000 individuals were injured in crashes involving large trucks (gross vehicle weight rating greater than 10,000 pounds) in the United States (National Highway Traffic Safety Administration [NHTSA], 2017). This statistic represented a 4% increase from 2014 crash reports. Of the 116,000 injured, 73% were occupants of other vehicles, 24% were occupants of the large trucks, and 4% were nonoccupants. In the same year, 4,067 individuals were killed in large truck crashes; 74% of those killed were occupants of other vehicles, 16% were occupants of the large trucks, and 10% were nonoccupants (NHTSA, 2017). Although these numbers represent the human toll, the economic costs are also staggering. For 2015 alone, large truck and bus crashes that resulted in property-damage-only cost an estimated US$28 billion (based on 2015 dollars) and fatalities and injuries caused due to large truck crashes cost an estimated US$90 billion combined (FMCSA, 2017b).
Although these statistics are startling, they do not necessarily link OSA to crash risk. Findings of a systematic review of MVC risk among individuals diagnosed with OSA indicated that studies that included noncommercial drivers found a positive correlation between MVC and OSA (Ellen et al., 2006). For studies involving CMVDs, the association between MVC and OSA was weaker than the association noted among noncommercial drivers (Ellen et al., 2006). The University of Pennsylvania Sleep Apnea Study found no statistical evidence that supported the belief that OSA significantly increased the risk of crashes by CMVDs (Steinberg, 2002). However, a recent study by Burks et al. (2016) found a link between OSA treatment nonadherence and increased crash risk among CMV drivers; truck drivers who were nonadherent to OSA treatment had a fivefold increased risk of preventable MVCs.
Precedence in linking OSA to a crash involving a CMVD was set in a notable case in which the Celadon trucking company settled with the family of John Lindsay for US$3.25 million after what was determined to be a likely OSA-related crash (Platenburg, 2011). Lindsay was killed when a 40 ton truck rear-ended Lindsay’s car while stopped in traffic. In an industry first, Celadon acknowledged that the crash was most likely related to the truck driver’s untreated sleep apnea (Platenburg, 2011).
Currently, FMCSA, the regulatory agency for the trucking industry, does not mandate OSA screening for CMVDs. Current regulations are broad and specify only that CMVDs cannot be medically certified to drive if they have a “respiratory dysfunction” that would interfere with their ability to drive safely (Subpart E—Physical Qualifications and Examinations, 1970). Over the years, various health-related experts, professional health-related organizations, and an expert panel have made recommendations regarding OSA screening for transportation industry workers; the FMCSA has not implemented any of the recommendations as federal regulations (Czeisler, 2011).
Untreated OSA has been associated with multiple health problems such as cognitive deficits (Engleman & Douglas, 2004), hypertension (Calhoun, 2010; Konecny, Kara, & Somers, 2014), cardiovascular disease (Sanchez-de-la-Torre et al., 2013), diabetes (Kendzerska, Gershon, Hawker, Tomlinson, & Leung, 2014), and decreased quality of life (Isidoro et al., 2015). Treatment of OSA with CPAP for as few as 2 to 7 days is associated with improved performance on a driving simulator (Tregear, Reston, Schoelles, & Phillips, 2010). Cognitive improvement post-CPAP therapy has been found to be inconsistent, and more research in this area is recommended (Aloia, Arnedt, Davis, Riggs, & Byrd, 2004; Kylstra, Aaronson, Hofman, & Schmand, 2013). Furthermore, mandatory OSA policies have garnered support both from inside and outside the trucking industry. Schneider National Inc., a major U.S. trucking company, implemented a fleetwide OSA screening and treatment program for their drivers (Garber, 2008). Professional organizations such as the Joint Task Force of the American College of Chest Physicians, American College of Occupational and Environmental Medicine, and the National Sleep Foundation (Hartenbaum et al., 2006) and the FMCSA Medical Expert Panel have recommended mandatory OSA screening and treatment for CMVDs (Ancoli-Israel, Czeisler, George, Guilleminault, & Pack, 2008).
Step 3: Construct Alternatives
Several policy options to address the problem of undiagnosed OSA among CMVDs were identified. One bold option would be to mandate trucking companies to implement sleep programs for all employees and contractors who drive for their companies. Sleep apnea programs generally include screening, diagnosis, education, treatment, and monitoring (Benefit Design Group, n.d.; SleepSafe Drivers, n.d.). Schneider National serves as an exemplar of a trucking company’s commitment to the safety of their drivers and the public (Mabry, Baker, Hickman, & Hanowski, 2012). In 2007, Schneider won the National Sleep Foundation Healthy Sleep Community Award for their sleep apnea program (Lazar, 2007). Through their program, the company has reported savings of US$538 to US$780 in health care costs per driver each month, a 30% reduction in crash frequency and a 65% increase in retention among drivers treated for OSA (Garber, 2008). J. B. Hunt explored the utility of a sleep program. The company participated in a clinical trial focusing on treatment of sleep apnea in their fleet of CMVDs, with positive results for both the company and drivers (Heavy Duty Trucking, 2009; Mabry et al., 2012). The company later contracted with SleepSafe Drivers, a national provider of sleep apnea management programs, to deliver OSA testing and treatment to the JB Hunt driving fleet (Heavy Duty Trucking, 2011). This option may be possible for large companies; however, small independent trucking companies would not likely have the human or financial resources to implement mandatory sleep management programs for their employees.
A second policy option would involve revisions to the current medical examination report form to include areas specific to OSA recognition, which could increase identification of CMVDs at risk for OSA and hold them accountable. Two task forces consisting of experts in sleep, respiratory, and occupational medicine (Epstein et al., 2009; Hartenbaum et al., 2006) have recommended that measurement of body mass index (BMI) and neck circumference be included in assessments of individuals at risk for OSA because BMI greater than or equal to 30, and neck circumference greater than or equal to 17 for males and greater than or equal to 16 for females may suggest OSA. The current medical examination report form does not include any questions or measurements that are specific indicators of OSA risk (FMCSA, 2015). Questions addressing BMI, neck circumference, and history of OSA could be easily added to the form. Currently, height and weight are collected during medical examinations, but BMI and neck measurements are not usually documented. If neck measurements and BMI were readily available, these measures could be used in conjunction with OSA history to identify drivers at risk for OSA. The examiner could then recommend further testing or provide conditional certification.
As noted, FMCSA regulations do not require OSA screening during fitness-for-duty examinations of CMVDs. A third policy option would be to mandate OSA screening in all medical certification examinations and require ongoing compliance with treatment regimens as a condition of medical certification with required annual recertification. The goal of the mandate would be to identify drivers with undiagnosed or untreated OSA and require treatment. Theoretically, with comprehensive screening, more drivers would be referred for formal diagnosis and begin treatment if diagnosed with OSA. This option alone could decrease daytime sleepiness and fatigue among drivers, and thereby increase safety on U.S. roadways (Lazar, 2007). In a study examining the impact of CPAP treatment on health plan and disability costs, treatment of OSA was associated with lower health care and disability costs (Hoffman, Wingenbach, Kagey, Schaneman, & Kasper, 2010). Estimates suggest that mandatory OSA screening would cost the trucking industry US$1 billion and more than US$100 million to the private bus industry (U.S. House of Representatives, Office of Congressman Larry Bucshon, 2011). Given such costs, cost–benefit analyses should be conducted to determine the benefits of such mandates. Cost–benefit analyses are most useful for analyzing policies to determine whether their benefit to society exceeds their costs (Cellini & Kee, 2010).
Per public law, the third policy option, mandatory OSA screening, and treatment among CMVDs would have to be pursued through the formal rulemaking process (Public Law 113-45, 2013). On March 10, 2016, the FMCSA and FRA initiated the formal rulemaking process by publishing an Advance Notice of Proposed Rulemaking and sought public comment on a proposed rule regarding the impact of OSA screening, evaluation, and treatment of safety-sensitive personnel (Darling & Feinberg, 2016; Minor & Lauby, 2016). A federal OSA rule would have specified treatment protocols and conditions that would require a diagnostic laboratory sleep study. Under the current system, medical examiners use their judgment and training to determine who is referred for diagnostic sleep studies. In a surprising development, FMCSA and FRA announced on August 4, 2017, that the Advanced Notice of Proposed Rulemaking regarding OSA among rail workers and CMVDs was withdrawn (FMCSA, 2017a). The agencies believe that currently established safety programs and the FRA’s regulations that address fatigue are appropriate methods to manage OSA (FMCSA, 2017a). Although this policy option was begun in 2016 and subsequently abandoned, it remains a potential path to implementing mandatory OSA screening in the trucking industry should the effort be revisited.
Maintaining the status quo is always a possibility and constitutes a fourth policy option. Recently, FMCSA’s status quo sustained a significant change which was the establishment of the National Registry of Certified Medical Examiners (NRCME; Hartenbaum, 2012). The NRCME regulation stipulates that health care providers who conduct medical certification examinations for CMVDs must be trained about specific physical qualifications that affect drivers’ ability to safely drive vehicles (Subpart D—National Registry of Certified Medical Examiners, 2012). As of May 2014, all certified medical examiners must have completed the required training and be listed on the registry; drivers must schedule medical examinations with certified examiners who are listed on the registry (Subpart D—National Registry of Certified Medical Examiners, 2012). According to the FMCSA, establishment of the NRCME is part of the organization’s commitment to prevent crashes, injuries, and fatalities associated with commercial motor vehicles (NRCME Plus, n.d.). Training of certified medical examiners is standardized and, therefore, ensures examiners identify and properly address disqualifying conditions. The addition of the NRCME is a significant step in taking a more structured approach to addressing OSA in the transportation industry.
Step 4: Select the Criteria
Criteria commonly used in the Bardach (2012) approach to policy analysis include such labels as efficiency, freedom, equity, fairness, justice, and legality. Given the potential impact of OSA screening and treatment regulations, efficiency is of utmost importance. Policy outcomes that can be achieved in the most efficient manner for all stakeholders are the goal. Outcomes such as increased public safety, decreased liability, and improved health status are quasi-tangible results that may take months or years to realize, yet, given time, these results will prove to be efficient outcomes. However, some stakeholders may incur initial costs that will be recouped through future savings and indirect benefits (e.g., longer, more productive work lives, and decreased liability; Hoffman et al., 2010; Nguyen, 2006).
A revised medical examination report form may be the least efficient option given the time and effort required to convene expert panels and elicit recommendations from professional groups concerning form revisions; this approach may not be an efficient use of financial and human resources. Despite the lack of efficiency associated with medical examination form revision, this approach may be a most equitable way of applying OSA screening standards across all CMVDs who must have a medical examination at least before their driving careers commence and every 2 years afterward.
All policy alternatives are unlikely to be perceived as satisfactory and fair for all parties involved. For example, with the implementation of mandatory OSA screening, some CMVDs may be deemed unfit for service or given conditional driving certifications that require time off from work. These outcomes may not be deemed fair, particularly in light of the potential for referrals of drivers who ultimately are not diagnosed with OSA. Truck drivers may question the fairness of proposed OSA regulations that they perceive as potential actions that will cause them to lose their livelihoods (Nguyen, 2006). The fairness of mandating employer-sponsored sleep programs could also be questioned. Will such regulations create fair outcomes for small businesses that may not be able to absorb the costs of employer-sponsored sleep programs? Schneider National acknowledged that they are able to offer free OSA diagnosis and treatment to their drivers because of their size (Nguyen, 2006). Treatment of sleep apnea not only has the potential to increase safety on U.S. roads, but it also improves quality of life and decreases disability rates among drivers who are treated for OSA (Mabry et al., 2012; Nguyen, 2006). Fairness and justice may also be viewed through a utilitarian lens. That is, although more stringent screening, diagnosis, and treatment of OSA in commercial drivers may be inconvenient, perceived as unfair, or costly to the commercial drivers, the potential benefit to the much larger driving public outweighs these concerns. However, increased public safety may be diluted when only CMVDs, and not the general public, undergo mandatory screening for OSA.
Regardless of the policy alternative chosen, years may be required before a federal rule mandates OSA screening and treatment, if such regulations are proposed again. The Safe, Accountable, Flexible, Efficient Transportation Equity Act: A Legacy for Users (2005) mandated development and implementation of the NRCME. Nine years passed between the mandate and full enactment of the NRCME. The time required to change federal legislation, coupled with the potential economic burden that new OSA regulations could place on stakeholders, may impede implementation of stringent OSA rules (Dills, 2012).
All stakeholders must be given an opportunity to voice their opinions about and recommend proposed changes to policies so that outcomes reflect the interests of all affected parties. Due process is automatically built into the federal regulation revision mechanism. Any proposed changes to federal regulations include a required public comment period. This approach creates the potential for federal OSA screening, evaluation, and treatment outcomes to be crafted by all stakeholders.
Step 5: Project Outcomes
For the policy alternatives under review, stakeholders include CMVDs, the Department of Transportation, the FMCSA, trucking companies, the general public, the public safety community, medical examiners, sleep professionals, companies that produce sleep apnea treatment appliances, and advocacy groups. Desired outcomes of OSA policies include (a) more CMVDs treated for OSA; (b) improved quality of life for CMVDs; (c) decreased disability among CMVDs treated for OSA; (d) disqualification of medically unfit CMVDs; (e) decreased MVCs related to OSA; (f) increased safety of U.S. roads; (g) decreased loss of life, productivity, and property due to OSA-related crashes; and (h) less liability for CMVDs and trucking companies when drivers are involved in MVCs. Projected negative outcomes are also associated with policy alternatives. Implementation of federal OSA screening and treatment regulations would be challenging. Although a large number of CMVDs are estimated to have OSA, coordinating and financing the testing of drivers would be difficult (Czeisler, 2011; Papp, 2012). Referrals for OSA testing based on objective measures such as BMI would inevitably result in referrals of individuals who do not have OSA and failure to refer those who do have OSA but do not meet the BMI referral criterion (Czeisler, 2011). The average cost of a sleep study is US$1,800 to US$2,000 (Dills, 2012; Gold, 2012) and these figures do not include loss of wages due to overnight testing in a sleep lab, nor do they include treatment and maintenance costs. The costs of OSA testing can negatively impact CMVDs. Furthermore, some truck drivers, particularly if uninsured, may not be able to afford a positive airway pressure mask and machine which are often the recommended treatment for OSA (Stanton, 2012). According to the Agency for Healthcare Research and Quality consumer summary, the costs of CPAP machines (before insurance adjustments) ranged from US$300 to US$2,000 plus supplies (e.g., masks, tubing, and filters) which can cost US$300 to US$800 annually (John M. Eisenberg Center for Clinical Decisions and Communications Science, 2011). Such economic burdens create an environment in which truckers are reluctant to seek diagnosis or treatment for OSA (Smith & Phillips, 2011). The loss of commercial drivers related to policy implementation may add tremendous burden to an already short-staffed trucking workforce (Walsh, 2013). In light of these realities, consideration must be given to acceptable accommodations.
Step 6: Confront Tradeoffs
Mandating trucking companies offer sleep programs as part of their benefit packages is also unlikely to be a popular solution among stakeholders because of the costs associated with such programs. Thus, mandating company sleep programs is not a realistic option.
In 2000, the FMCSA medical examination form was revised for the first time since 1970, and use of the new form has been required since November 2001(Blumenthal et al., 2002). Thus, changing the medical examination form took approximately 30 years. In 2015, FMCSA implemented changes to the medical examination form that aligned the form with new certified medical examiner procedures and processes (Darling, 2015). Given the recently revised form, the likelihood of further revisions based on OSA-related biometric measures and family history is low, especially because none of the advisory committees made recommendations to revise the medical form. In addition, changes to the medical examination form that include documentation of OSA risk factors (e.g., BMI, neck circumference, and family history) could be interpreted as an indirect method of OSA screening. Any strategy that appears to circumvent the regulatory process will not be well received by CMVDs or motor carriers. Considering the possible costs of examination form revisions, the interests of public safety may be better served by pursuing other policy options.
More in-depth examinations of cost-effective screening and treatment options are needed before regulations that mandate OSA screening and treatment can be implemented. Given the high costs of screening, more affordable treatment options are needed before the industry will support comprehensive OSA screening and treatment (Dills, 2012). Moreover, implementation of mandatory OSA screening and treatment through formal rulemaking will require extensive research, cost–benefit analyses, and an open-comment period. Many CMVDs are fearful that OSA screening and treatment regulations will cause drivers to lose their jobs if they are diagnosed with OSA (Nguyen, 2006). Changing drivers’ attitudes and perceptions will take time.
Implementation of the NRCME is expected to bring some standardization to the fitness for duty medical certification process and reduce the number of CMV drivers who are medically unfit to drive (Lester, 2012). The NRCME went into full effect on May 21, 2014.
Regardless of which course of action is taken, the economic impact on motor carriers and CMVDs must be considered. Some truck drivers, both insured and uninsured, cannot afford testing and treatment options or lost work time due to testing and treatment (Stanton, 2012). In addition, treatment plans must incorporate strategies that address work environment challenges such as allowing idle time and fitting trucks to power CPAP masks safely (Stanton, 2012). The critical question is how the transportation industry balances the needs of drivers and the concerns of employers with public safety. In whatever manner the industry approaches OSA, the process that leads to reform will be lengthy; however, this process is a trade-off for embracing change that is acceptable to most stakeholders.
Steps 7 and 8: Decide and Tell Your Story
Bardach’s (2012) final steps are to decide upon a policy alternative and engage stakeholders to change current policy. Despite challenges to implementation and the time required to change attitudes, perceptions, and federal regulations, the best policy alternative for the transportation industry is pursuing mandatory OSA screening and treatment through the formal rulemaking process. This option is the fairest and most just policy for all stakeholders. To be fair to all parties, research on the efficacy of portable OSA testing and cost-effective treatment options must be conducted. Efforts must be made to increase driver awareness of OSA, their knowledge regarding the importance of treatment, and their belief that an OSA diagnosis does not inevitably result in loss of vocation. In addition, the FMCSA and motor carriers must earnestly support drivers by ensuring their livelihoods are not jeopardized by OSA diagnoses.
Regulations mandating screening and treatment have the potential to not only increase public safety, but also improve the health of CMVDs, extend their work years, and decrease cases of disability. Although the FMCSA has chosen not to pursue OSA screening and treatment through the formal rulemaking process, of the available policy alternatives, formal rulemaking is the approach most likely to produce results that support due process and are equitable for all stakeholders.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for doctoral studies: The National Institute for Occupational Safety and Health (NIOSH) Occupational Health Nursing fellowship (Kirkendoll) from the Deep South Center for Occupational Health and Safety (T42OH008436).
Author Biographies
Kenya D. Kirkendoll is a doctoral candidate at the University of Alabama at Birmingham School of Nursing. Her dissertation research focuses on CPAP use among long-haul truck drivers.
Karen Heaton is the director of Occupational Health Nursing in the Deep South Center for Occupational Health and Safety (T42OH008436) and the coordinator of the PhD Program at the University of Alabama at Birmingham School of Nursing.