
Abstract
Evidence has consistently shown that low/limited health literacy (HL) is associated with negative health consequences and higher costs for individuals and society. To generate internal data for employee training and health/wellness programming, an HL assessment of 120 university employees was conducted using the Newest Vital Sign (NVS), a valid and reliable clinical screening tool that asks individuals to interpret a nutrition label. Sociodemographic data were collected and time to administer the NVS tool was also measured. Even in this employed, well-educated sample (mean years of formal education was 16.6 years), 17% had scores indicating limited or possibly limited HL. Findings have implications for occupational training and health providers and programs. Even a well-educated workforce benefits from addressing HL challenges or situational issues with universal strategies. This project supports initiatives to assist employees better navigate, understand, and use health information and services to improve their health.
Keywords
Health literacy (HL) is defined as “the capacity to obtain, communicate, process, and understand health information and services in order to make appropriate health decisions” (Affordable Care Act, 2010, p. 1252). Occupational HL specifically refers to how well workers obtain, communicate, process, and understand occupational health and safety information and services, and then use that information to make decisions about their health (Wong, 2012). Importantly, HL is a strong predictor of individual and population health, stronger than age, income, race, ethnicity, education, or employment status (Berkman, Sheridan, Donahue, Halpern, & Crotty, 2011). Studies show that individuals with lower HL have poorer health outcomes, higher rates of hospitalization, higher health care costs, and are less likely to access preventive health services compared with individuals with adequate HL (Berkman et al., 2011; Mancuso, 2009). In addition, the National Occupational Research Agenda (NORA) has identified workers with low HL as a population at risk of more injuries, illnesses, and fatalities in the workplace (Parks, Chikotas, & Olszewski, 2012). The collective financial cost of low HL in the United States alone is between US$106 billion and US$236 billion annually (National Institutes of Health, 2014). Unfortunately, studies over the past 20 years have consistently shown that health information is often presented in ways that many individuals cannot understand or use (Berkman et al., 2011). For example, a worker with low HL may struggle interpreting drug labels, especially if the instructions are not clearly written. “Twice a day” or “two times daily” is not as clear as “take one pill at 7 a.m. and another pill at 6 p.m. every day.” As such, medications may be consumed incorrectly, increasing the risk of life-threatening complications.
Many national and global HL experts recommend approaching all individuals as though they are at risk of misunderstanding health information. This approach is termed “health literacy universal precautions” (Brega et al., 2015). Studies have shown that health professionals generally overestimate clients’ HL levels (Dickens, Lambert, Cromwell, & Piano, 2013; Kelly & Haidet, 2007) as well as their own knowledge of HL (Mackert, Ball, & Lopez, 2011). For instance, Dickens et al. (2013) reported that when nurses estimated clients’ HL based on their “gut feeling” or clients’ answer to a single question (“What was the highest grade level you have completed?”), 68% of the sample were determined to have adequate HL level; when using validated HL tools, only 28% were determined to actually have adequate HL. Moreover, anyone, even someone who is usually knowledgeable about their health and who has proficient HL under normal conditions, can have “situational” HL challenges (Koh, Brach, Harris, & Parchman, 2013). Communicating health information using clear, simple language is appreciated by individuals with low or even adequate HL (Meppelink, Smit, Buurman, & van Weert, 2015; Otal et al., 2012; Table 1). The Agency for Healthcare Research and Quality (AHRQ) has developed specific interventions addressing HL and distributed through the AHRQ Health Literacy Precautions Toolkit. This resource was originally released in 2010, revised in 2015, and is now available for download free of charge (Brega et al., 2015; DeWalt et al., 2010).
Key Concepts Addressing Potential HL Challenges
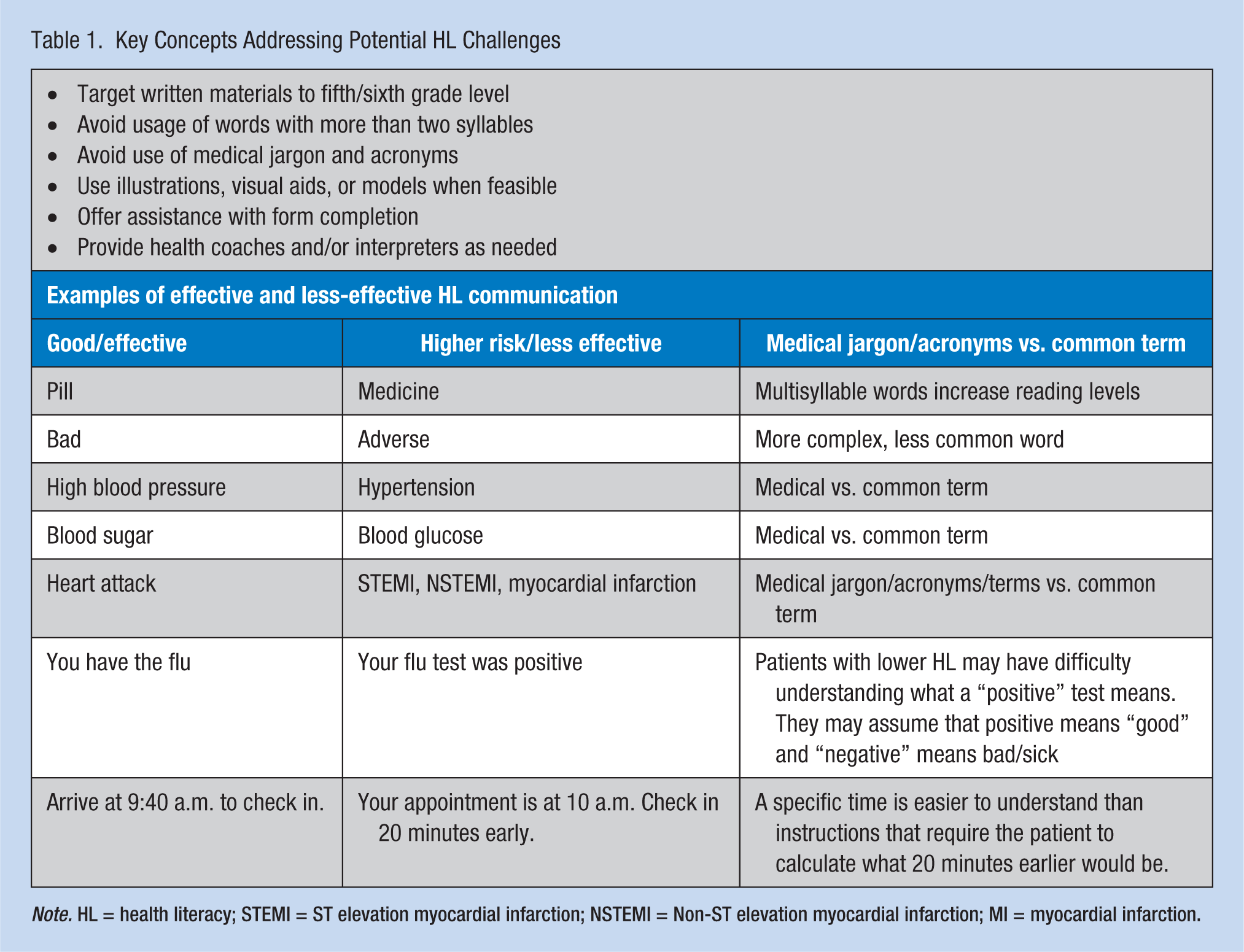
Note. HL = health literacy; STEMI = ST elevation myocardial infarction; NSTEMI = Non-ST elevation myocardial infarction; MI = myocardial infarction.
Studies show that health outcomes can be improved, and some diseases prevented, by reducing HL demands on workers receiving basic health information (Koh et al., 2013). Thus, occupational health and safety policy experts advocate building health literate workplaces (Wong, 2012) and recommend that organizations implement system-wide HL universal precaution strategies (Batterham, Hawkins, Collins, Buchbinder, & Osborne, 2016; Koh et al., 2013; U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion, 2010). When system-wide HL universal precaution strategies are in place, all personnel work together to create a welcoming, shame-free environment. They approach all workers as though they may be at risk of not understanding health information, and clearly communicate health information verbally and in written form to all workers. Furthermore, all health care, human resource, and health education forms; training programs; and policies are designed with simple and culturally appropriate language, and interpreters and/or health coaches are available to assist in health communication and workplace training activities. Health literacy experts believe that such initiatives may also reduce health disparities (Koh et al., 2013; The National Academies of Sciences, Engineering, and Medicine, 2015). However, despite the evidence that improving HL is key to improving health outcomes for individuals and populations, wide-spread adoption of universal HL precautions by organizations has been slow (Batterham et al., 2016; Koh et al., 2012; Koh, Baur, Brach, Harris, & Rowden, 2013; The National Academies of Sciences, Engineering, and Medicine, 2015).
The purpose of this HL assessment of employees of a large Midwest university was to generate internal data as a platform for organizational HL discussions. The project was also designed to inform initiatives for employee training and health plan and wellness programs.
Method
This project used an observational, cross-sectional design to evaluate HL in a convenience sample of 120 new and existing employees who visited a university employee outpatient clinic for routine care. Institutional review board exempt approval was granted for the project. All adult university employees who presented to the clinic for postoffer employment screening, health surveillance activities, or routine care were eligible to participate in the project. Employees less than 18 years of age and those presenting to the clinic for treatment of an acute injury or illness were excluded. Participation was voluntary and verbal consent was obtained. Participant self-reported data on gender, age, occupation (job title), employee status (new or existing employee), years of formal education, and native language were gathered via interview and deidentified data were recorded. Based on the reported job title, participants’ occupations were categorized as “medical” or “nonmedical.” Education was categorized by the years of formal education reported by each participant with “12 years” considered high school graduation or the equivalent. Reported native language was categorized as “English” or “non-English.”
Health literacy data were collected using the Newest Vital Sign (NVS) tool, which is available from the Pfizer Pharmaceutical Company at no cost to health care providers and public health officials (Figures 1 and 2). The NVS is a six-question bilingual screening tool that identifies patient risk of low or limited HL based on interpreting an ice cream nutrition label. The test can be administered in approximately 3 minutes in a clinical setting. The English version of the NVS tool was used in this project and measured understanding and use of words (prose literacy), numbers (numeracy), and forms (document literacy; Pfizer, 2016). The NVS instrument has been compared with the more commonly used, lengthier, and more well-established HL assessment tool, Test of Functional Health Literacy in Adults (TOLFHLA). The TOLFHLA assesses an individual’s ability to read and comprehend text and perform health-related computations. The NVS correlates reasonably well with the longer established TOLFHLA tool. Internal consistency of the NVS has been established using Cronbach’s alpha (α = .76), criterion validity (r = .59) with area under the receiver operating curve of 0.88 for the English version (Mancuso, 2009). In a recent systematic review, the NVS was identified as the best current tool choice for measuring HL in clinical settings (Duell, Wright, Renzaho, & Bhattacharya, 2015). Total time to administer and complete the NVS tool was measured in the current study by using the stopwatch function on an iPhone 4. Time was recorded in minutes, seconds, and hundredths of seconds, but converted to minutes for data management purposes. Scores of each participant’s NVS tool were tallied and all data loaded into a secured Microsoft Access Database. Sociodemographic and NVS-related data were converted from the Microsoft Access Database into a Microsoft Excel spreadsheet and analyzed using IBM SPSS version 21.
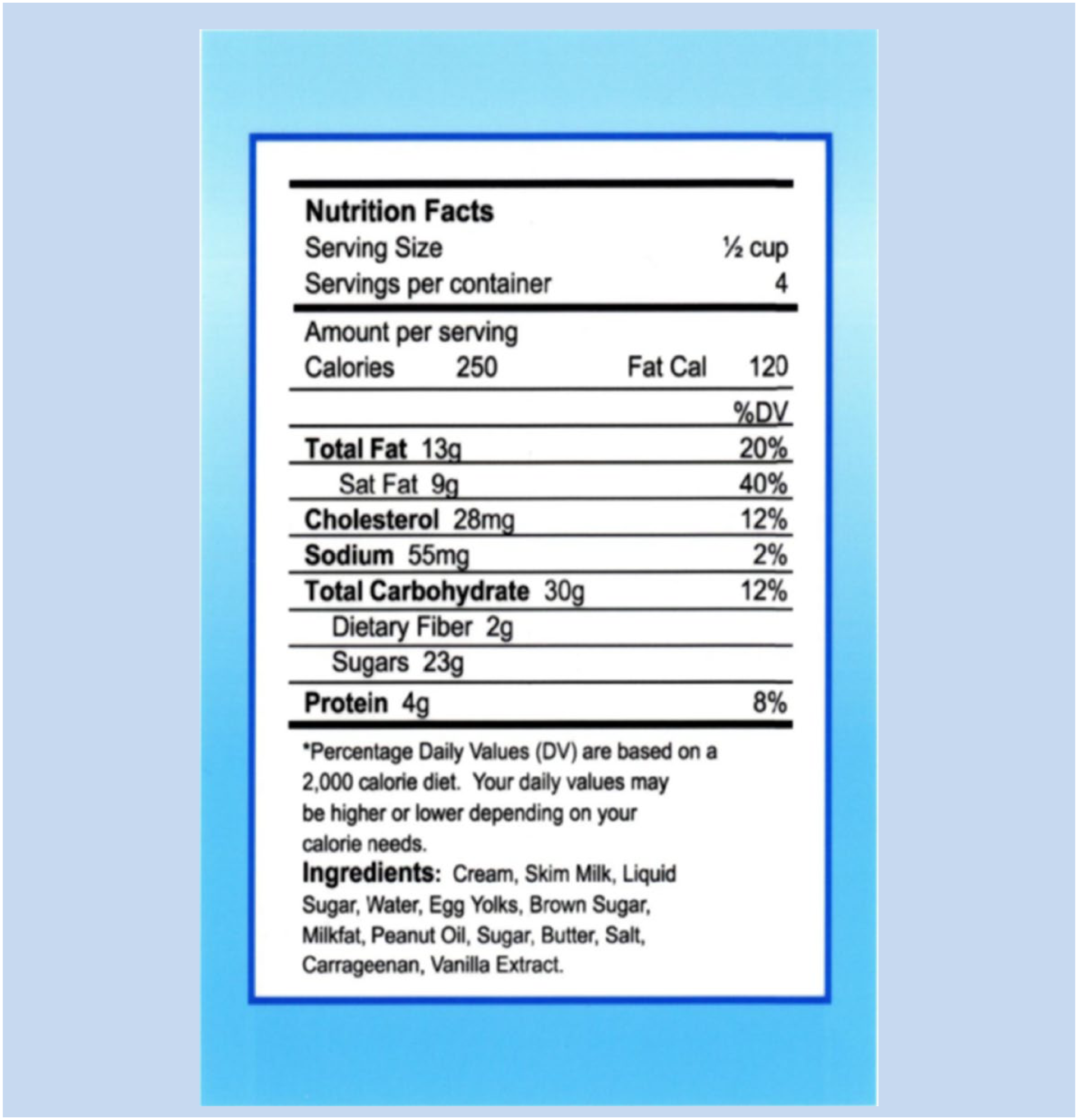
Newest Vital Sign nutrition label.
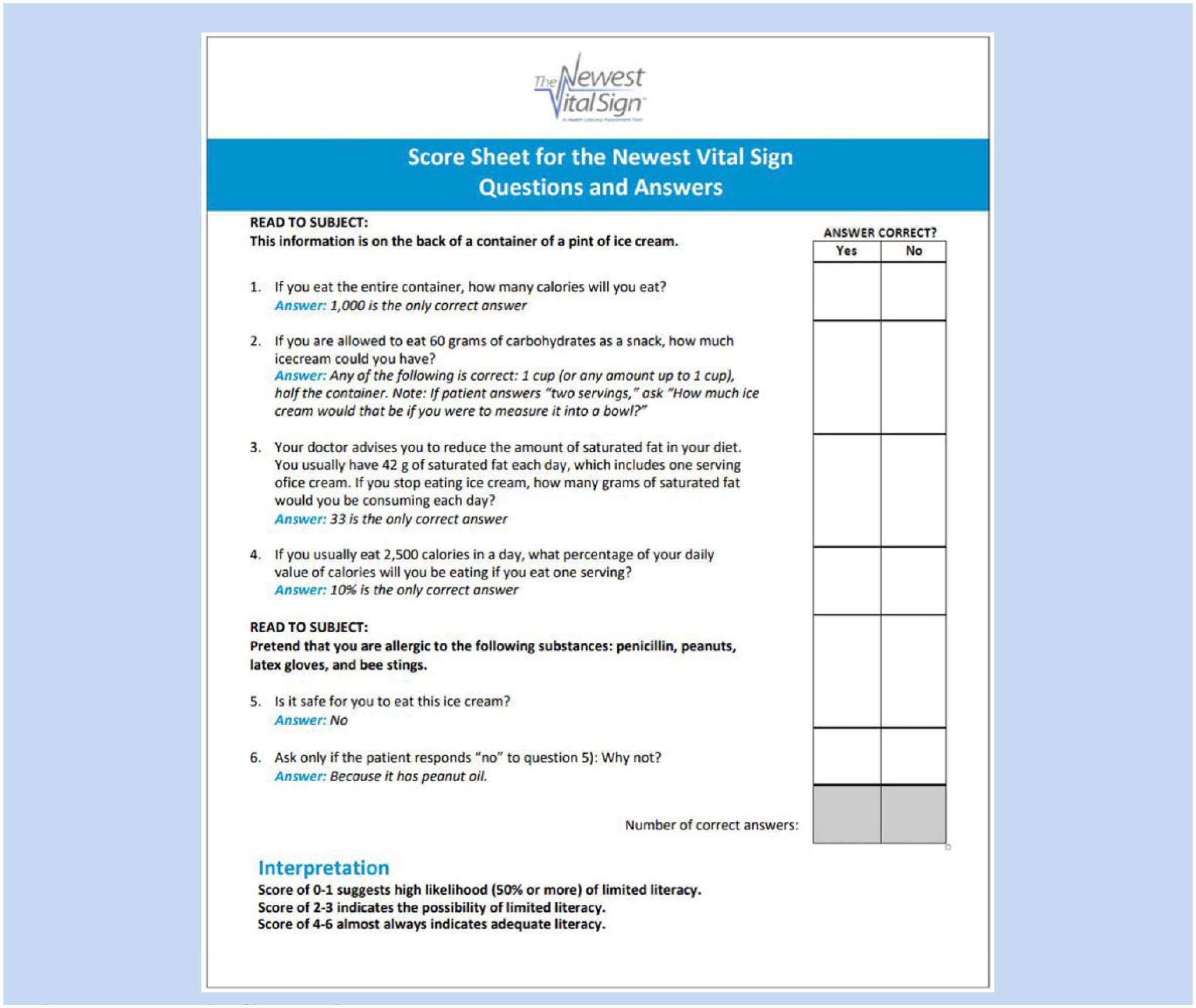
Newest Vital Sign questions and answers score sheet.
Descriptive statistics were generated for analysis. Categorical variables such as employment status, gender, job type, and native language were analyzed using cross tabulations. Bivariate relationships between the continuous variables of age of participants, years of formal education, NVS score, and time to complete the NVS were analyzed using Pearson product–moment correlations. Bivariate relationships of on-average group differences of the categorical variables on NVS score and time on task were evaluated using t tests.
Results
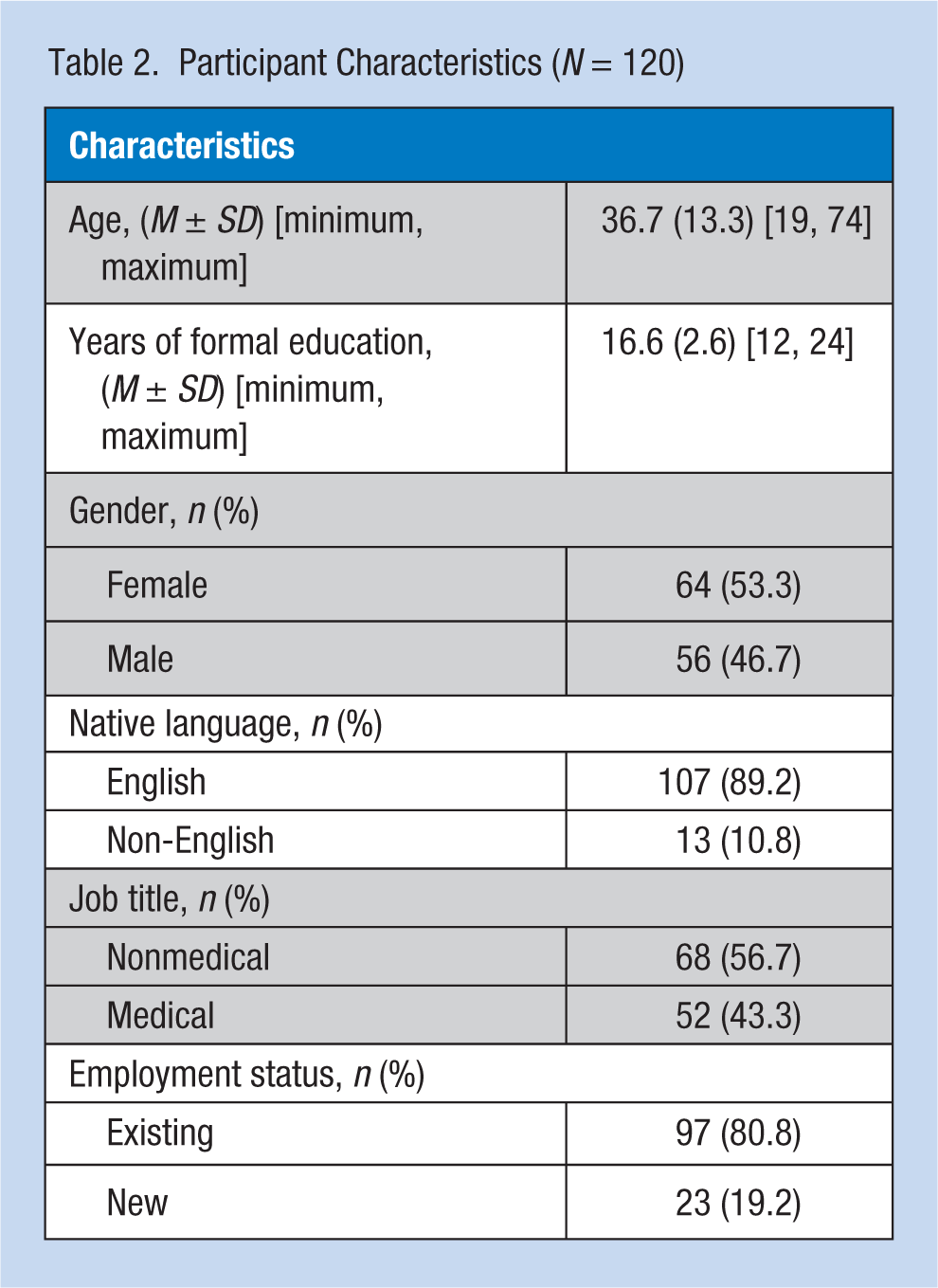
One hundred twenty employees volunteered to participate in this HL assessment project. No volunteers were excluded. One employee did not complete the NVS tool due to blindness. The average age of the group was 36.7 years (Table 2). All participants reported completing at least a high school diploma or the equivalent. The average number of years of formal education for the group was 16.6 years. The majority of the sample were female (53.3%), reported English as their native language (89.2%), were in nonmedical jobs (56.7%), and were existing employees (80.8%).
Participant Characteristics (N = 120)
The mean NVS score for the group was 4.76 (SD = 1.32, score range = 0-6). Newest Vital Sign scores were also aggregated into three groups: scores of 0 or 1 indicated limited HL (2.5%), scores of 2 or 3 indicated possibly limited HL (14.2%), and scores of 4, 5, or 6 indicated adequate HL (83.3%). The mean time to complete the NVS tool was just below 2 minutes (see Table 3).
Results of Health Literacy Screening
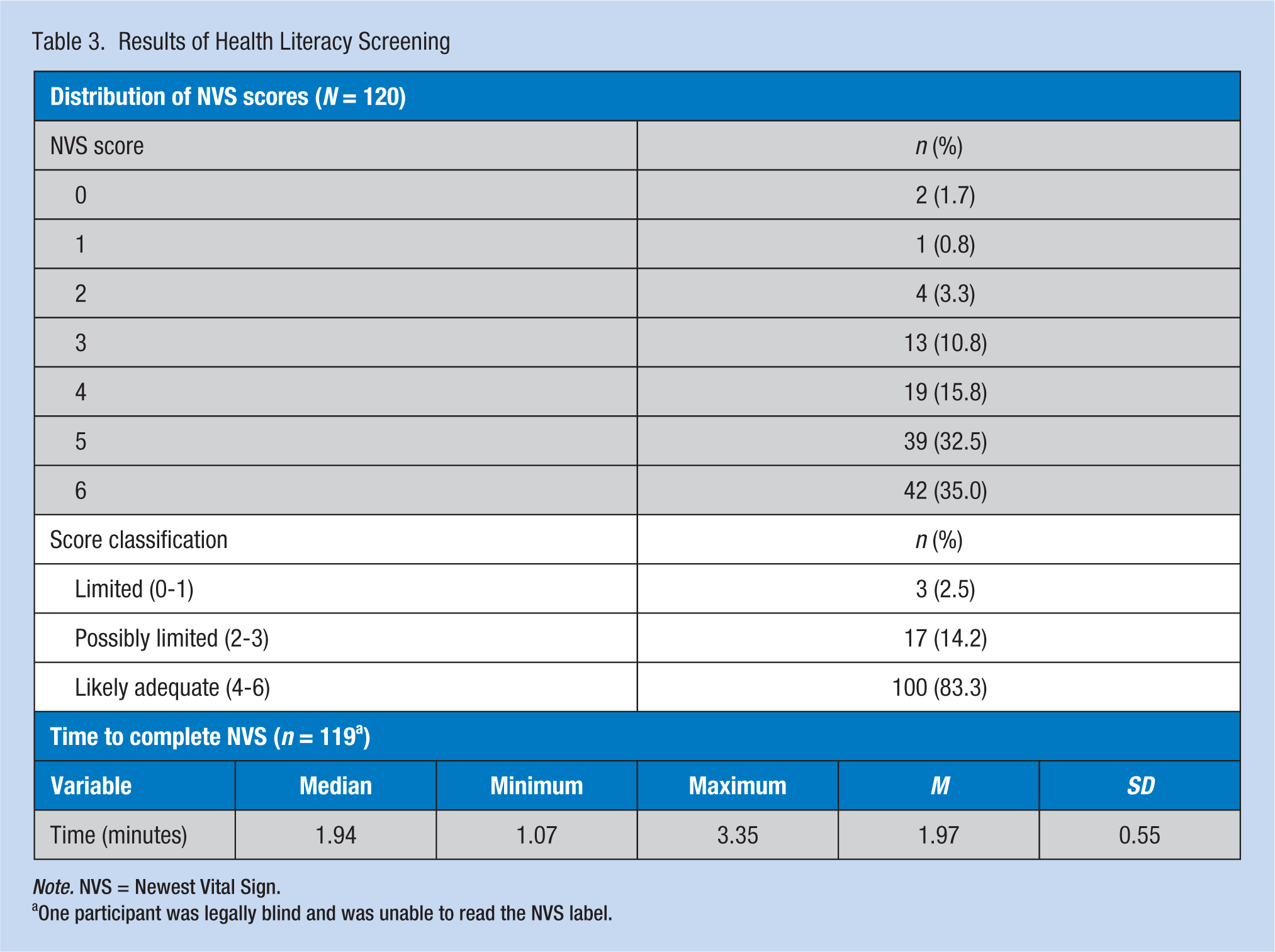
Note. NVS = Newest Vital Sign.
One participant was legally blind and was unable to read the NVS label.
Correlations
Longer time to complete the NVS (p < .001) and older age (p < .01) were correlated with lower NVS scores (Table 4). In addition, correlations between education and NVS did not achieve statistical significance. Non-English native language (p < .01) was also correlated with lower NVS scores (Table 5). Newest Vital Sign scores were lower for non-English native-speaking participants compared with native English-speaking participants (p < .01); non-English native-speaking participants took longer to complete the NVS compared with native English-speaking participants (p < .01). No significant differences emerged between medical and nonmedical job types relative to NVS scores or NVS completion times (data not shown).
Pearson’s Correlations Between NVS Score, Time, and Education (N = 120)
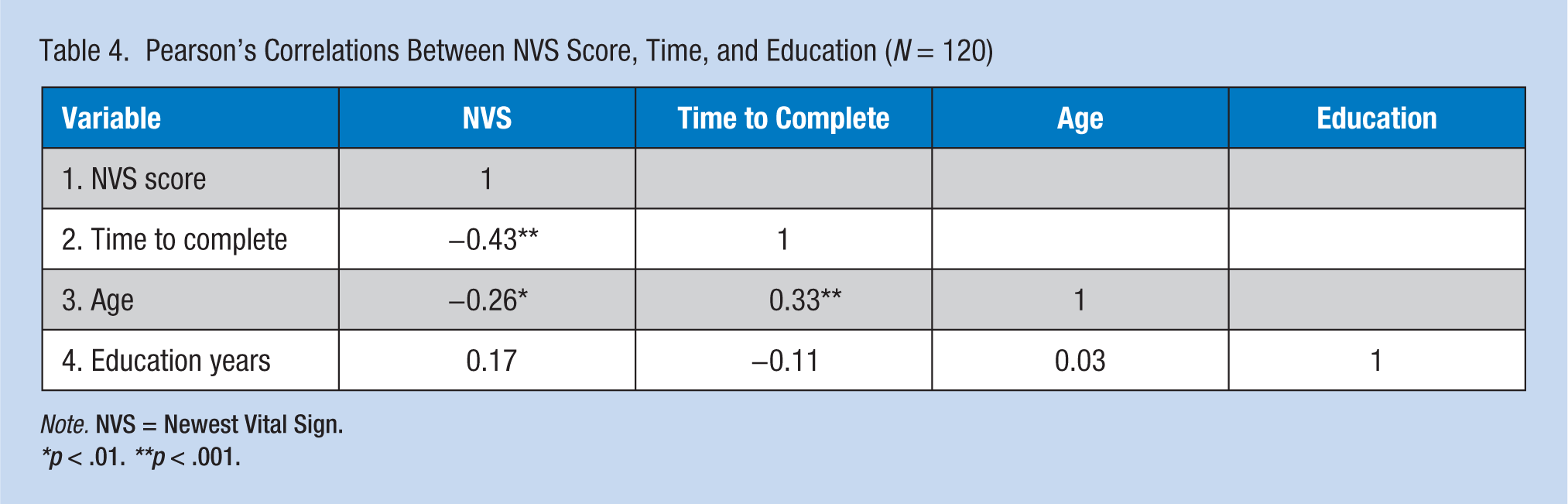
Note. NVS = Newest Vital Sign.
*p < .01. **p < .001.
Language Differences of On-Average Group Differences in NVS Score and Time to Complete
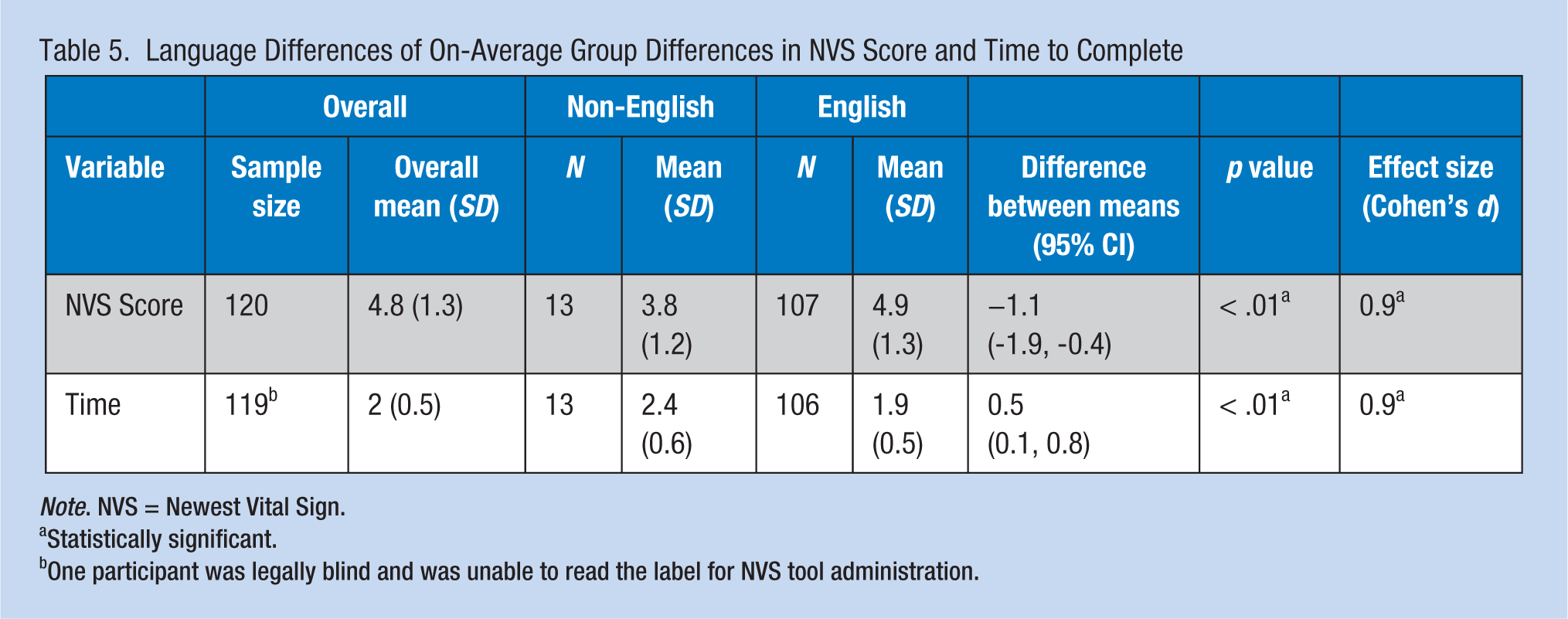
Note. NVS = Newest Vital Sign.
Statistically significant.
One participant was legally blind and was unable to read the label for NVS tool administration.
Discussion
The HL levels varied in this sample of 120 university employees who were generally well-educated. Although the majority of participants (83%) were classified by their NVS score as having “likely adequate” HL skills, 17% had scores that indicated “limited” or “possibly limited” HL. The findings suggest that HL levels cannot always be predicted by sociodemographic characteristics such as education. For example, some more highly educated (≥16 years of formal education) and native English-speaking participants had “limited” or “possibly limited” NVS scores. These findings are aligned with previous studies evaluating HL in diverse populations (Easton, Entwistle, & Williams, 2010). Although some populations are not generally considered at high risk of limited HL, individuals within those populations may struggle routinely or situationally with HL issues (Koh et al., 2013).
In this project, lower NVS scores (indicating lower HL) were associated with non-English native speakers, older age, and longer time to complete the NVS assessment. These findings support the evidence from previous studies that vulnerable populations (e.g., older adults, minority cultures, those not fluent with English) are more likely to have HL challenges, lifestyle risk factors, and difficulty accessing and navigating the health care system (Adams et al., 2013; Koh et al., 2012; Levy & Janke, 2016). Conversely, strengthening HL in vulnerable populations improves individual and community resilience, decreases health inequities, and improves health and wellness practices (WHO Regional Office for Europe, 2013).
Similar to the claims by the NVS tool developer and prior studies, the NVS tool was administered and completed by participants in the current project in approximately 2 minutes (Heinrich, 2012; Pfizer, 2016; Weiss et al., 2005; Welch, Vangeest, & Caskey, 2011). If a quick baseline assessment of HL is needed, these findings indicate the NVS tool is feasible to use during a routine primary care or occupational health visit.
This project had some limitations. The sample size was relatively small. A convenience sample of 120 employees visiting a single clinic during a one-time 10-week timeframe limits the generalizability of the findings. In addition, enrollment into the project was voluntary, so the HL status of individuals who chose not to participate is unknown. Furthermore, only the English version of the NVS was used. Therefore, it is not known whether non-English native-language participants might have had higher scores if the tool had been in their native language.
Despite the limitations, however, this project had several strengths. The study generated new HL data about a cohort of workers in an organization that did not currently use HL universal precautions. Although the majority of participants were highly educated, employed, and interacted with the health system in a relatively low stress situation, the data indicated that some of these individuals still had low/limited HL. These findings are similar to previous larger studies and support the majority of HL expert recommendations that HL universal precautions should be used in all organizations.
Implications for Occupational Health Nursing Practice
Increasing cultural and linguistic diversity in the United States exists in health care settings and organizations nationwide (Arcury, Estrada, & Quandt, 2010; Batterham et al., 2016). Integrated system-wide approaches are needed to address the associated HL challenges when delivering health information (Brega et al., 2015; Coleman, Austin, Brach, & Wagner, 2009; Koh et al., 2013). In addition to using universal HL precautions, novel approaches are needed to improve access to care for individuals with HL challenges (Levy & Janke, 2016; U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion, 2016). Heath literacy advocacy is needed at all levels, from championing individuals in clinical settings to influencing organizational, local, regional, national, and international policies. It is critical that occupational health professionals and staff learn to efficiently recognize and address potential HL issues in the populations they serve.
To successfully improve health outcomes, individuals must be fully engaged in disease-prevention practices, health care decisions, and self-management activities, all of which require adequate levels of HL (Koh et al., 2013). Everyone, including employees of organizations, benefit when health information is presented using clear, simple communication techniques in a comfortable, welcoming environment. Human resource personnel, job-training educators, and supervisors use educationally, culturally, and linguistically appropriate materials during health and safety training (Arcury et al., 2010).
Successful strategies to address low HL include using (a) the teach-back method; (b) jargon-free, unhurried verbal communication; (c) simple illustrated written materials; (d) continuing phone calls or text-targeted messages; and (e) involving family and significant others (Cloonan, Wood, & Riley, 2013; Sheridan et al., 2011). In addition, some workers may require very detailed, personalized assistance (e.g., health coaches, interpreters and/or navigators, picture cards, individualized hands-on teaching by health professionals) to assist workers in overcoming barriers to understanding, navigating, and using the health system. Even individuals who read well, are comfortable using numbers and forms, and hold professional positions can face situational HL challenges when they or their loved ones are frightened, seriously ill, or injured; have temporary or permanent cognitive impairments; receive new diagnoses; have complex treatment regimens; are not familiar with language or terminology; or lack adequate insight into how their bodies work (French, 2015; Koh et al., 2013). Using individual-centered, focused communication is especially important when relaying health information to workers with limited HL (Speros, 2011). Occupational health nurses can assist individual employees reach their HL potential and lead organizational initiatives to address HL challenges.
Conclusion
The authors report that some individuals employed by a large Midwest university who had no obvious risk factors for low HL did, in fact, have NVS scores indicating low/limited HL. These findings suggest that organizations adopt the use of HL universal precautions and use evidence-based strategies to improve HL when needed. Everyone should be presented with health information in ways they can understand (Brega et al., 2015; DeWalt et al., 2010; Wong, 2012). Using system-wide HL universal precautions and assisting workers in navigating the health care system can improve health outcomes and reduce health care costs.
Footnotes
Acknowledgements
The authors would like to acknowledge Loraine Sinnott for her statistical assistance and Janine Overcash for assistance with editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This scholarly project was supported in part by a grant from Sigma Theta Tau, Epsilon Chapter.
Author Biographies
Joyce I. Karl is an assistant professor and adult nurse practitioner at The Ohio State University (OSU) College of Nursing. She currently teaches in the Master’s Nurse Practitioner and DNP Programs. Her scholarly interests include health literacy, active learning strategies, and use of an academic electronic health record in nursing and interprofessional education.
Jodi C. McDaniel is an associate professor at the OSU College of Nursing. Her research focuses on determining the effects of select polyunsaturated fatty acids (PUFAs) on the cellular and molecular mechanisms of chronic inflammation and the associated conditions in the aging population (e.g., chronic wounds, cognitive decline).