
Abstract
The workplace is an invaluable venue for health protection and promotion interventions, particularly for truck drivers due to their overreliance on their work environments, a plethora of work-related stressors, and their morbidity rates. Extant efforts of trucking companies to address driver health through worksite health and wellness programs have been inadequate, producing unsustainable results. The Driver Health and Wellness Program Survey was designed for and disseminated to 46 trucking companies to assess the current state of health and wellness programs in the trucking industry, including program participation rates and longevity, program evaluation procedures, and program activities and resources. Findings indicate that programmatic efforts in trucking companies continue to fall short, and health and wellness programs are insufficient to improve health outcomes in a sustainably positive direction. A new integrated, systems-based paradigm is proposed as a conceptual and methodological framework with the potential to meaningfully advance interventions in blue-collar work settings.
Keywords
The workplace is an invaluable population health promotion setting, both because of the amount of time workers spend at work and because of the influence the workplace has on human health (HealthyPeople.gov, 2013; Linnan et al., 2008). Hence, occupational health professionals have the potential to deliver comprehensive, multilevel health promotion programs to large segments of the adult population (Leka & Kortum, 2008). Health promotion initiatives can take any number of forms across different types of worksites, across and within multiple levels of influence (Sorensen & Barbeau, 2012). The powerful influence of contexts in which workplace health and safety interventions are administered must be considered (Sorensen & Barbeau, 2012).
The trucking work environment is detrimental to the health and safety of its employees (Bureau of Labor Statistics, 2010). Truck drivers operate in an occupational context with interconnected and far-reaching stressors, including physical and psychological workload and fatigue, the pressures of tight schedules and just-in-time deliveries, exposure to physical and chemical hazards, irregular shift work leading to chronic sleep deprivation, scarcity of workplace resources to promote health, sedentary work conditions, low job-control and satisfaction, extended social isolation, and work–life conflicts (Apostolopoulos, 2012; Apostolopoulos et al., 2012).
Truck driver health outcomes include high rates of obesity, cardiometabolic disease, and musculoskeletal, mental health, and sleep disorders (Apostolopoulos, Sonmez, Shattell, & Belzer, 2011; Apostolopoulos et al., 2013; Caban et al., 2005; Hadler, Keyserling, & Press, 2008; Howard et al., 2004; Krueger, Brewster, et al., 2007; Parks, Durand, Tsismenakis, Vela-Bueno, & Kales, 2009; Saltzman & Belzer, 2007; Shattell, Apostolopoulos, Collins, Sonmez, & Fehrenbacher, 2012; Wood, Hegmann, Murtaugh, & Thiese, 2007). Excess morbidity rates often medically disqualify drivers from employment (Krueger, Belzer, et al., 2007). The combination of truckers’ excess morbidity rates and elevated exposure risks (e.g., miles driven) are associated with fatality rates 11 times higher than that of the general workforce, accounting for 13% of all fatal occupational injuries (NIOSH, 2007; Bureau of Labor Statistics, 2010). Life expectancy for these employees is 16 years less than that of the general male population (Ferro, 2011).
Such morbidity and mortality rates have far-reaching repercussions for a wide array of stakeholders. Increased driver turnover, health care and insurance costs, workers’ compensation claims, lost time injuries, and lower productivity generate a substantial financial burden for employers (Apostolopoulos et al., 2012; Krueger, Brewster, et al., 2007). Annual health care costs have reached US$1,944 for obese drivers compared with US$1,131 for normal-weight drivers (Martin, Church, Bonnell, Ben-Joseph, & Borgstadt, 2009). Annual costs of absenteeism and health care expenditures for drivers with body mass indexes (BMI) of 40 or higher are US$2,027 compared with US$175 for drivers with BMIs of 25 to 29.9 (Osland, Clinch, Ramsay, & Wells, 2011). Beyond financial costs, the human costs of impaired trucker health are borne by both the drivers themselves and the motoring public. Drivers with BMIs of 35 or higher have a 43% to 55% increase in accident risk for all types of crashes of any severity (Anderson et al., 2012).
Limited research has identified inadequate programmatic efforts to address truck driver health at the workplace. Driver health and wellness programs have been shown to be individually based and reactive (Apostolopoulos, 2012; Krueger, Brewster, et al., 2007). These programs frequently are underfunded, limited in scope, and operated in “silos” within trucking companies (Apostolopoulos, 2012; Krueger, Brewster, et al., 2007). Substantial variation exists among driver health and wellness programs currently provided. Annual program budgets may range anywhere from US$150 to US$500,000, and program longevity ranges from newly initiated to 18 years (Krueger, Brewster, et al., 2007). Some companies offer small, simple programs; others provide comprehensive programs that are integrated into overall corporate culture (Krueger, Brewster, et al., 2007; Respiratory Care & Sleep Medicine, 2009).
Companies have generally found health and wellness programs to be effective investments (Krueger, Brewster, et al., 2007). Large companies such as Schneider National, JB Hunt, and Trucks, Inc. have all reported cost savings from their efforts (Krueger, Brewster, et al., 2007). Con-way Freight operates a comprehensive driver health and wellness program and has reported an 80% reduction in workplace injuries, 32% reduction in workdays lost due to injury, a mean weight loss of 11.1 pounds, and a reduction in blood pressure to below hypertensive status for 1,810 participating employees (Osland et al., 2011). Efforts to improve driver health have also been initiated by stakeholders outside of the trucking companies. For example, Travel Centers of America/Petro and Pilot/Flying J offer nutrition education and physical activity for drivers (Ellin, 2011).
The dismal state of driver health, and thus the relevance of and need for workplace interventions, suggest a need for an organizational assessment of current driver health and wellness programs. Grounded in a synergy of job strain, ecological, and system-science theoretical frameworks (Homer & Hirsch, 2006; Karasek, 2008; Stokols, 1996), the aims of this article are to (a) determine the support for and integration of these programs within companies, (b) assess program proliferation and longevity, (c) identify key program components and resources, (d) gather company perceptions regarding program elements, (e) examine program evaluation processes, and (f) extend a new integrative, systems-based worksite health promotion paradigm.
Method
Forty-six trucking companies that provide health and wellness programs to their drivers served as the sample for this study. This number was reduced from a total of 51 companies because five responses were not from trucking companies. Companies were solicited for participation through two avenues: First, the study was announced through daily emails to American Trucking Association (ATA) member companies. This email was distributed to the entire ATA national membership list, which includes private carriers, for-hire carriers, shippers, and other allied companies. Second, companies with publicized health and wellness programs were contacted and invited to participate through direct email. Respondents were health and wellness program managers, often within the safety or human resources departments of responding companies, and upper management, including presidents and vice presidents.
Participants completed the 33 questions of the Driver Health and Wellness Program Survey, which addressed key health and wellness issues as reported in the worksite health promotion literature. Many questions were duplicated or modified from an established survey used by the Federal Motor Carrier Safety Administration (Krueger, Brewster, et al., 2007). Additional questions were developed following a comprehensive review of health and wellness program literature, including programs offered outside the transportation industry (Brewster & Littler, 2010; Kahn, 2010; Krueger, 2012; ). Topic areas included general company information, general health and wellness program information, driver characteristics, program characteristics, organizational characteristics, program activities, program resources, and program evaluation. Companies were asked to rate driver characteristics, program characteristics, organizational support for programs, barriers to success of programs, and reasons for initiating and maintaining a program. Program activities, resources, and evaluation questions asked companies to select items that applied to their health and wellness program using a checklist format.
Collected data were cleaned by eliminating responses from companies reporting an absence of health and wellness programs, incomplete responses, and responses that were not from trucking companies (i.e., health and wellness program partner organizations). Data were analyzed using the Statistical Package for the Social Sciences (SPSS), computing frequencies, and descriptive statistics. Finally, because the researchers only obtained information about organizations and programs, the Institutional Review Board (IRB) office determined that no human participants were involved and thus the study was deemed exempt from human participants’ approval.
Results
Trucking Company Demographics
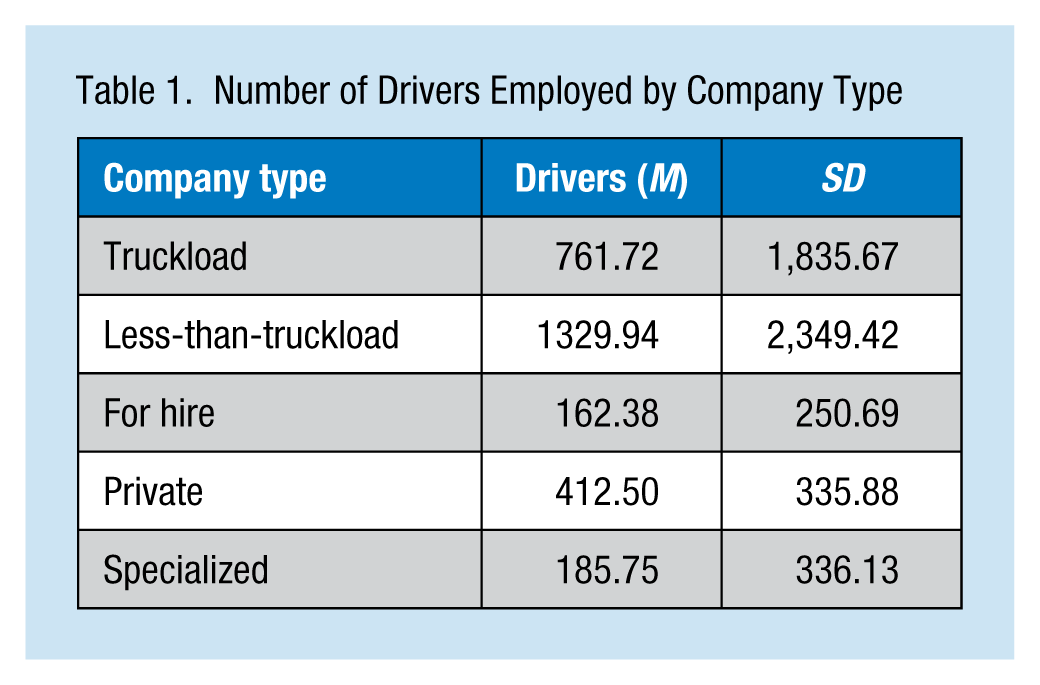
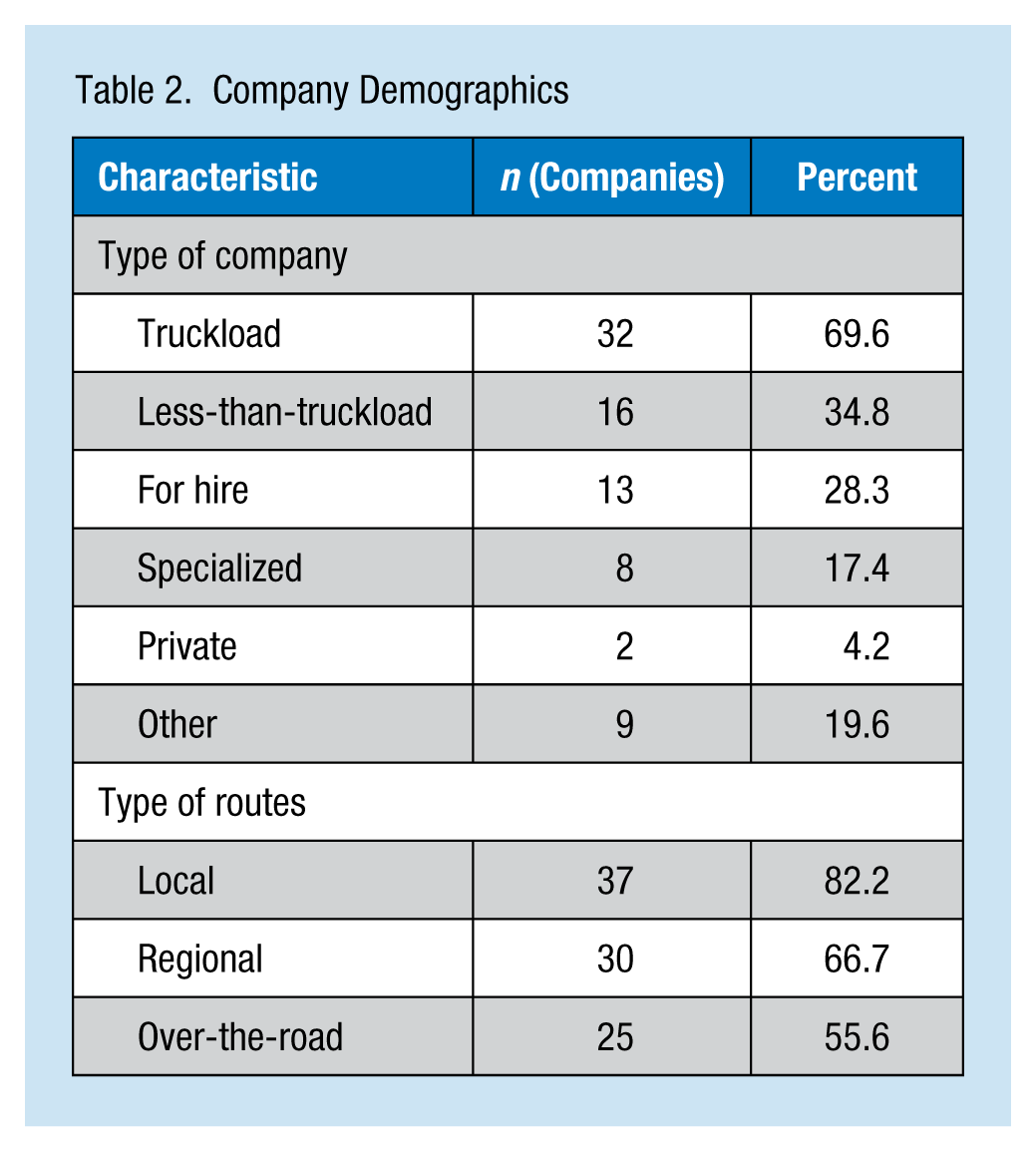
Most companies were truckload, less-than-truckload and for hire, with balanced route types. Several of the companies included in the study had multiple types of operations (e.g., truckload and less-than-truckload). The mean number of drivers employed by study companies was 809.65 (SD = 1897.27), with the number of drivers employed ranging from 2 to 7,426. The number of drivers employed by company type was as follows: truckload, 761.72 (SD = 1835.67); less-than-truckload, 1329.94 (SD = 2349.42); for hire, 162.38 (SD = 250.69); private, 412.50 (SD = 335.88); and specialized, 185.75 (SD = 336.13; Tables 1 and 2). The majority of drivers were male (99.2%, SD = 15.96) and not unionized (95.57%, SD = 18.02).
Number of Drivers Employed by Company Type
Company Demographics
Overview of Health and Wellness Programs
Of the 46 participating trucking companies, 60.9% had a health and wellness program for drivers, and 64.3% of the programs were developed in-house. When companies were asked from where they obtained their programs if they were not developed in-house, answers included an agent, a broker, a local hospital, the Teamsters, and a third-party vendor. Approximately 57% of companies with health and wellness programs reported that they teamed with other organizations for their health and wellness program. Programs had been in place for an average of 5.82 years (SD = 10.45). Most companies indicated that participation rates increased substantially (14.3%), increased modestly (33.3%), or remained about the same (42.9%) since their program began. None of the companies indicated that participation rates had declined since their health and wellness programs began.
Rationale and Management of Programs
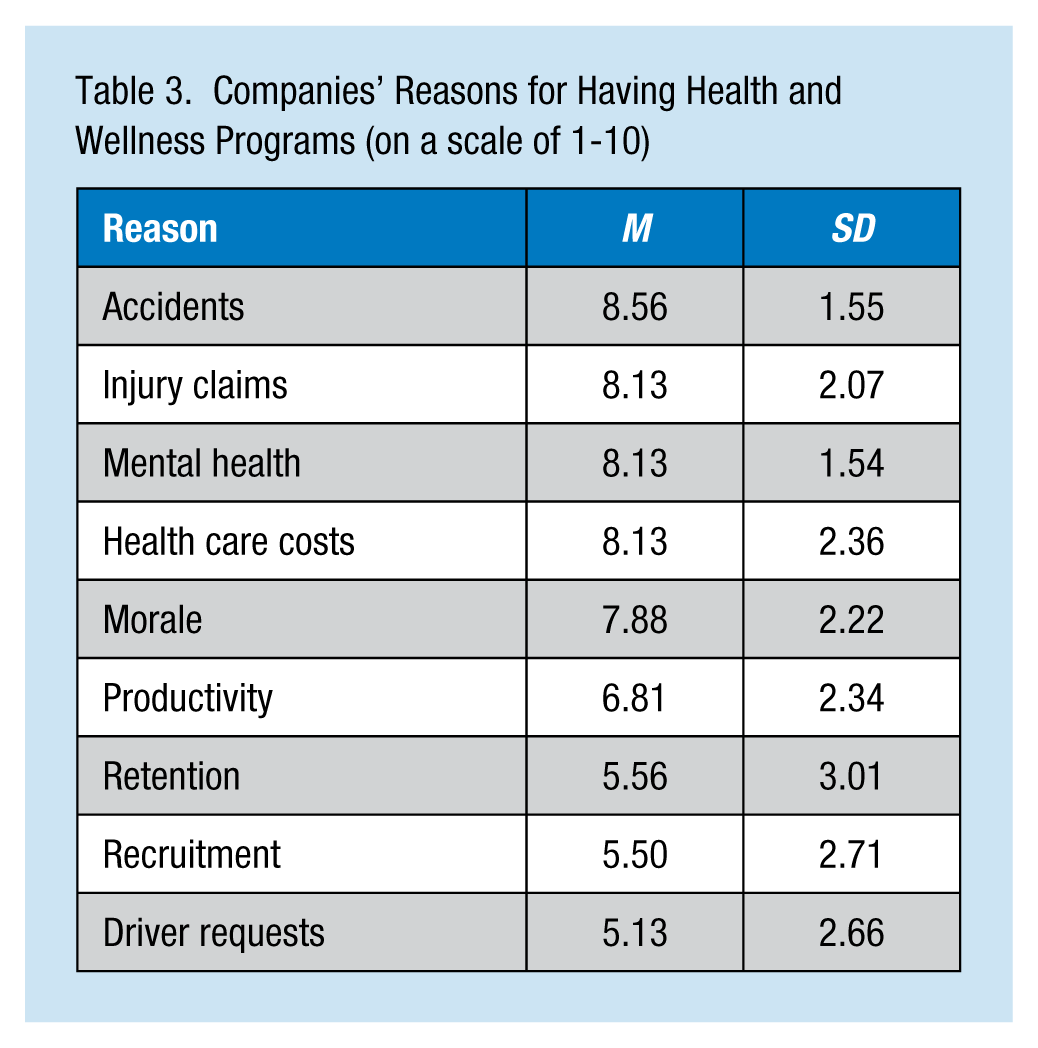
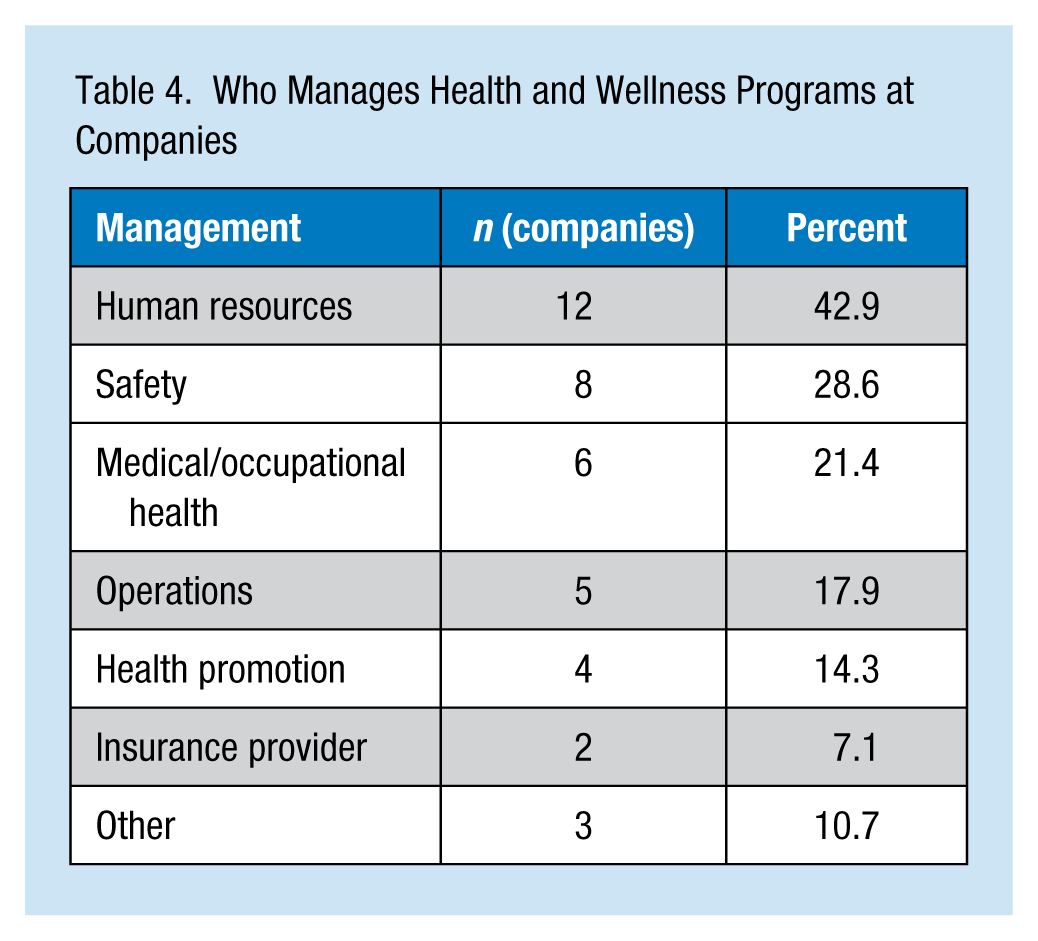
Companies were asked to rate reasons for having a health and wellness program. The highest rated reasons were accident prevention (M = 8.56, SD = 1.55), followed by reducing injury claims (M = 8.13, SD = 2.07), mental health issues (M = 8.13, SD = 1.54), and health care costs (M = 8.13, SD = 2.36; Table 3). Programs were most commonly managed by human resources departments, followed by departments of safety, medical/occupational health, operations and health promotion, as well as insurance providers (Table 4). Other departments that managed these programs were benefits and medical/wellness departments as well as fitness coaches. Program resources were most commonly allocated to behavior change efforts (M = 30.27%, SD = 24.28), followed by awareness (M = 28%, SD = 16.37), education (M = 26.61%, SD = 15.71), and changing the environment (M = 15.11%, SD = 9.22).
Companies’ Reasons for Having Health and Wellness Programs (on a scale of 1-10)
Who Manages Health and Wellness Programs at Companies
Program Components and Resources
Companies were asked to indicate the activities and resources that were included in their programs. The most common activities were weight management (30.4%), nutrition education (28.3%), and smoking cessation (28.3%). The most common resources provided through programs were wellness brochures and poster displays (26.1%), healthy food at company facilities (21.7%), and nutrition education and information (21.7%). An average of 6.18 activities and 3.96 resources were included in these programs, with significant variation between the programs.
Company Support and Integration
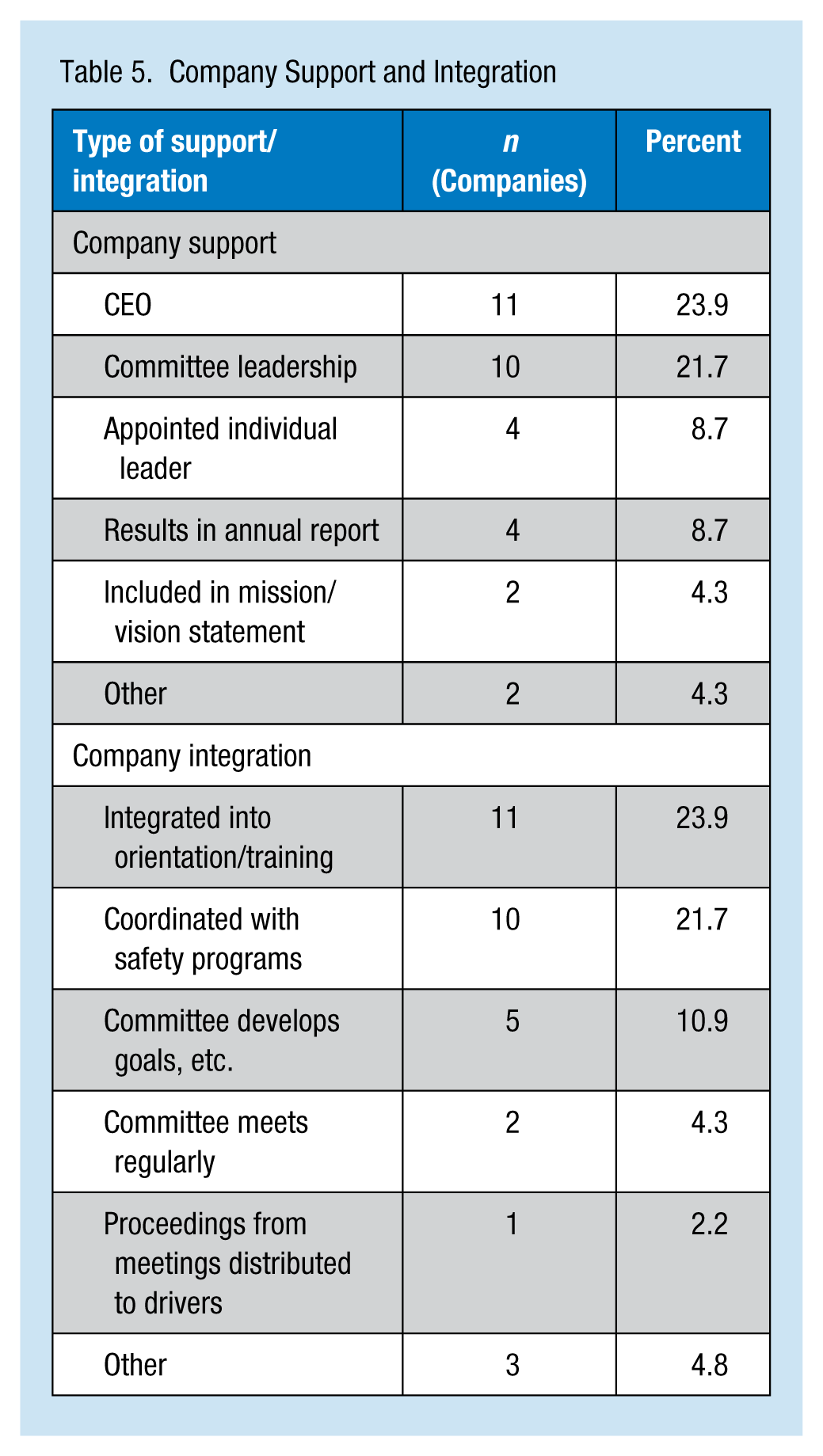
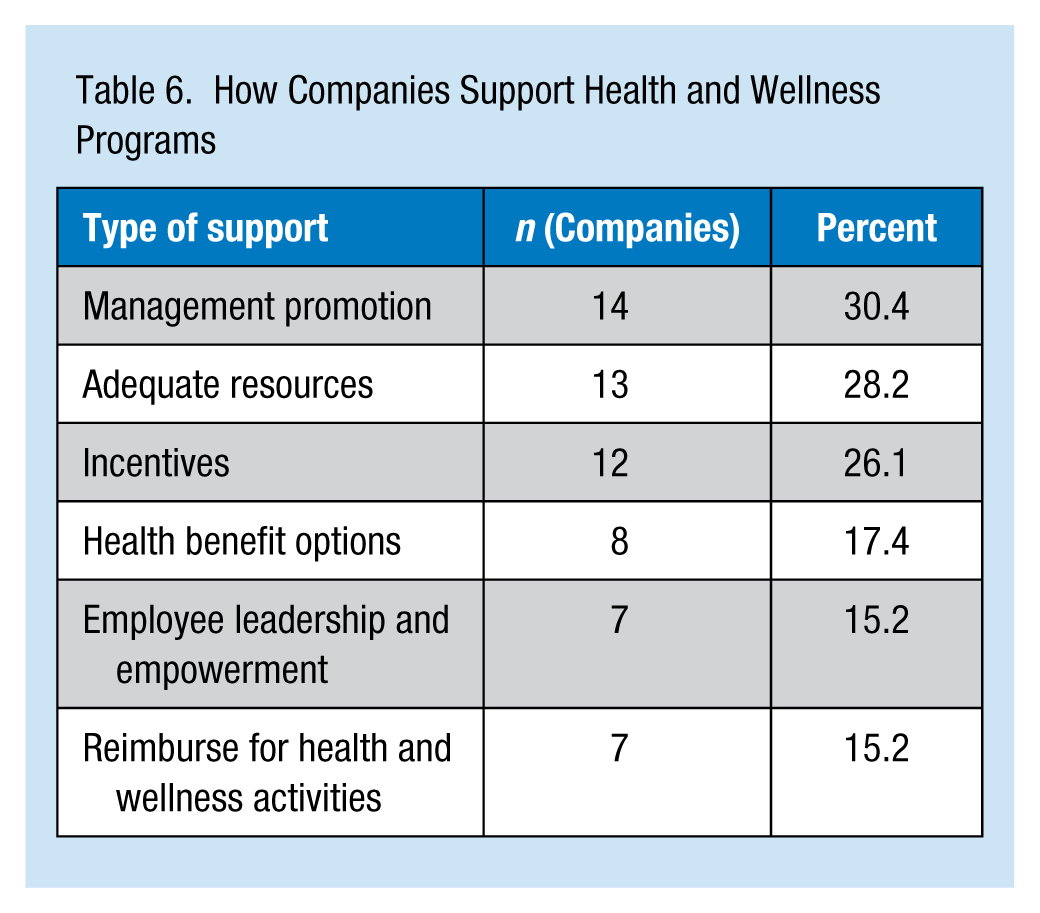
Support for these programs within companies was most commonly from the CEO (23.9%), followed by leadership committees (21.7%; Table 5). The most common way that programs were integrated into companies was through orientation and training (23.9%), followed by coordination with safety programs (21.7%; Table 5). When asked to indicate the ways in which companies provide support for health and wellness programs, management promotion of programs (30.4%) and provision of adequate resources (28.2%) were the most common (Table 6).
Company Support and Integration
How Companies Support Health and Wellness Programs
Program Evaluation
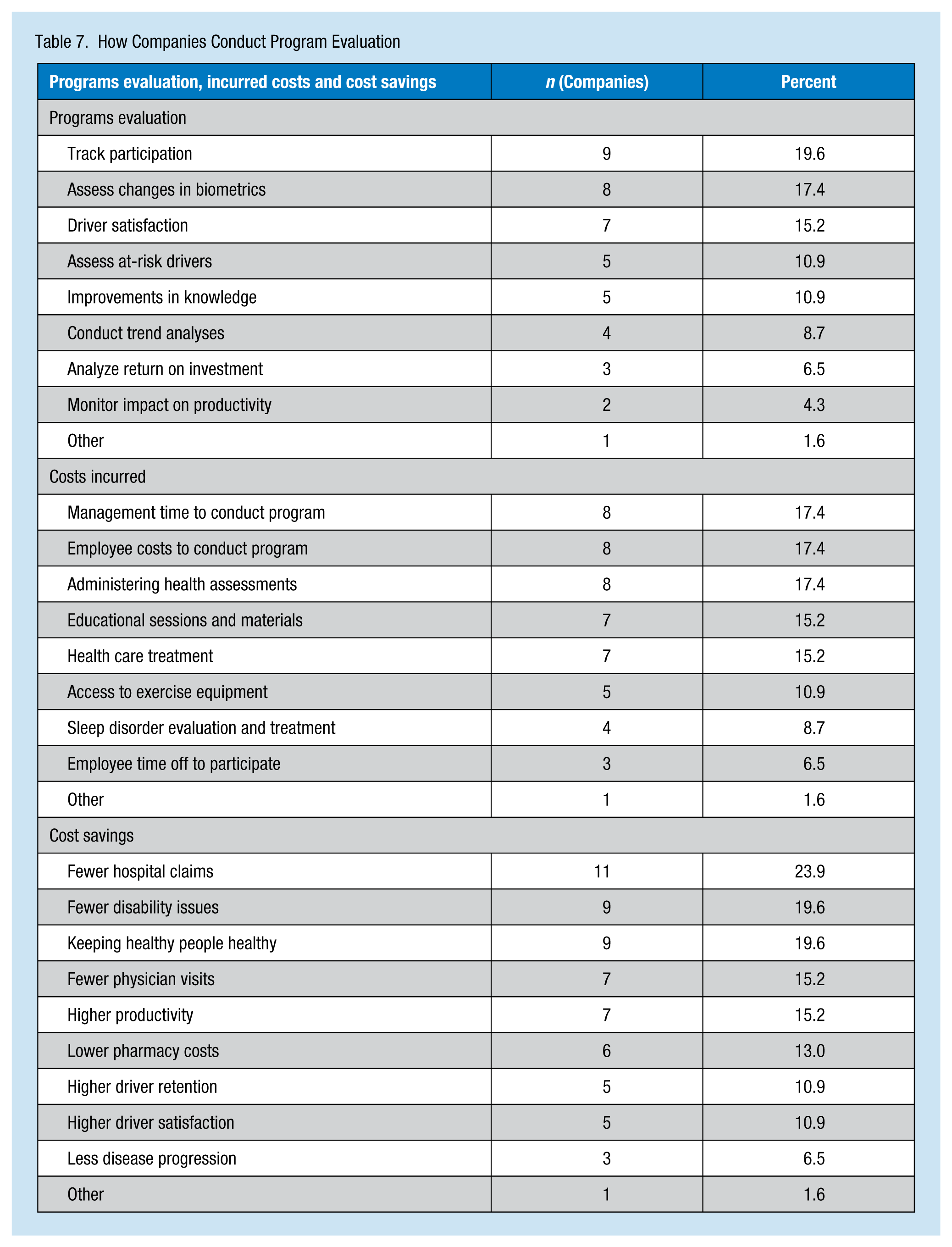
Programs were most commonly evaluated by tracking participation (19.6%), assessing changes in biometrics (17.4%), and surveying driver satisfaction (15.2%). In evaluating the costs of administering these programs, the most common costs considered were management time for conducting the program (17.4%), employee costs associated with conducting the program (17.4%), and administering health assessments (17.4%). The most common cost savings used to evaluate driver health and wellness programs were fewer hospital claims (23.9%), fewer disability issues (19.6%), and keeping healthy people healthy (19.6%). Information on evaluation of company health and wellness programs is displayed in Table 7.
How Companies Conduct Program Evaluation
Program Characteristics and Barriers
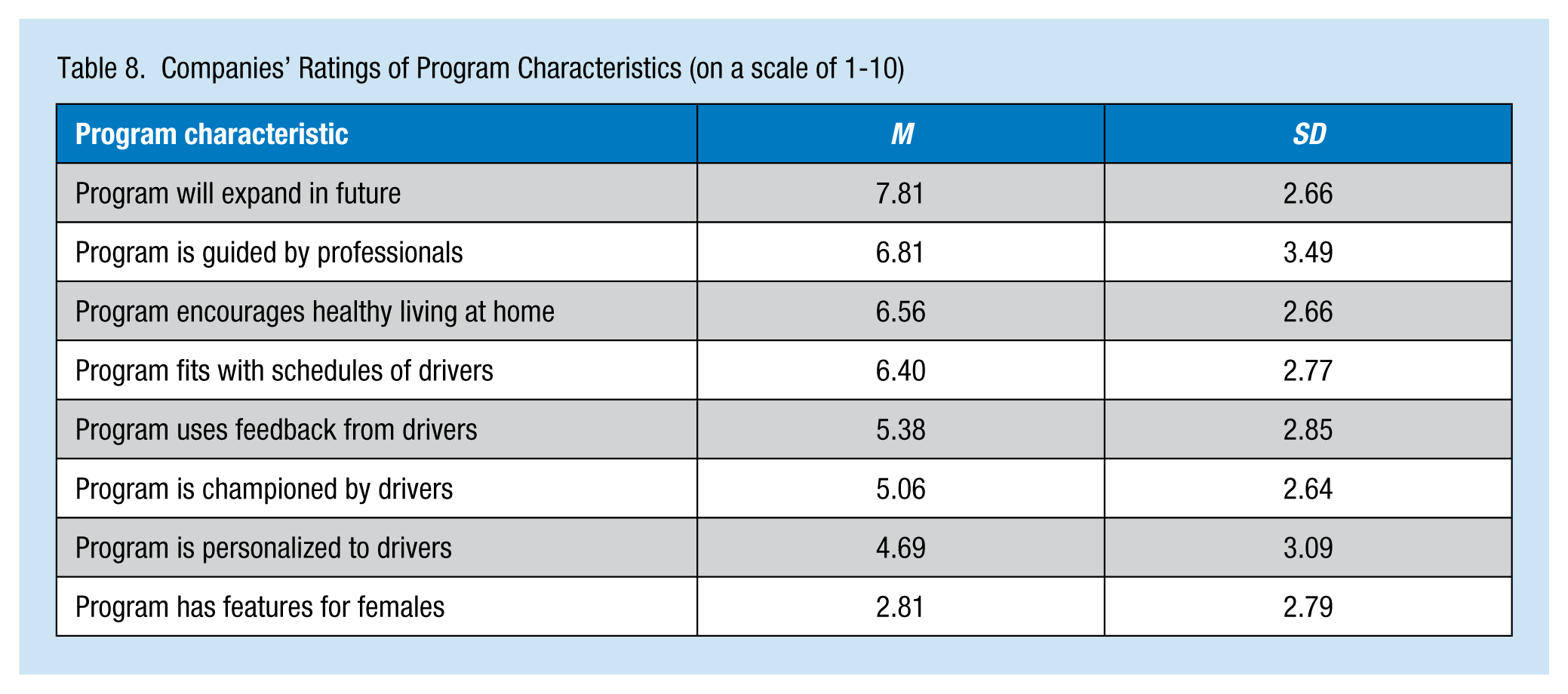
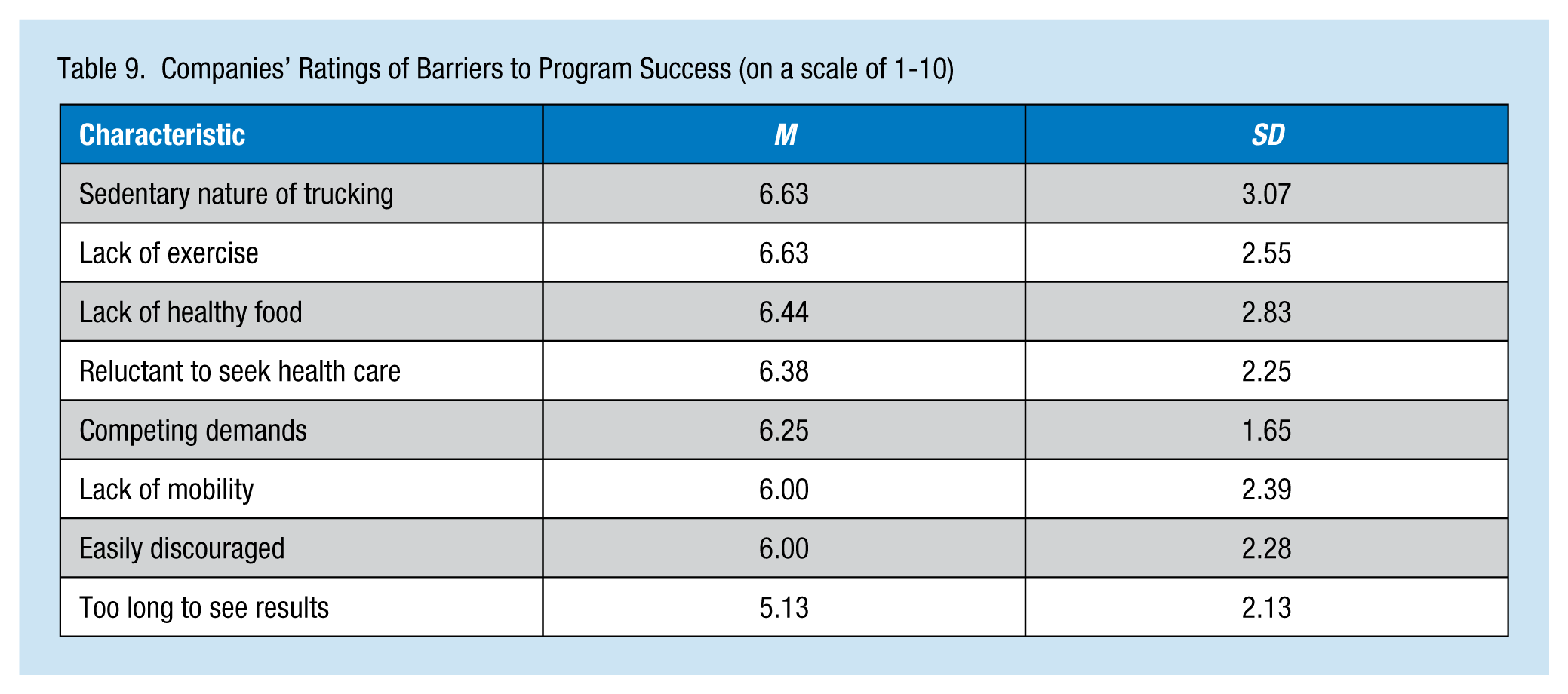
Companies rated anticipated expansion of the program in the future most highly (M = 7.81, SD = 2.66), followed by being guided by professionals (M = 6.81, SD = 3.49; Table 8). The lowest rated characteristic was program features specifically for female drivers (M = 2.81, SD = 2.79). Companies were also asked to rate barriers to program success (Table 9). The highest rated barrier was the sedentary nature of trucking (M = 6.63, SD = 3.07), followed by access to physical activity amenities (M = 6.63, SD = 2.55) and healthy food (M = 6.44, SD = 2.83) while on the road. The lowest rated barrier was driver turnover (M = 4.20, SD = 3.47).
Companies’ Ratings of Program Characteristics (on a scale of 1-10)
Companies’ Ratings of Barriers to Program Success (on a scale of 1-10)
Discussion
Prevalence of Programs
Proliferation of comprehensive worksite health promotion programs, those which include health education, supportive physical and social environments, links to related programs, program integration, and worksite screenings (Linnan et al., 2008), is considered a significant national population health objective. Healthy People 2010 called for at least 75% of worksites to offer comprehensive health promotion programs by the year 2010; however, a national survey of worksite health promotion programs revealed that only 6.9% of responding worksites offered such programs (Linnan et al., 2008; Sorensen & Barbeau, 2012). As an occupational sector, it appears that the trucking industry currently falls far short of reaching this objective. This study was designed to gather information on existing health and wellness programs within companies; therefore, it is likely that the prevalence of these programs across the trucking industry as a whole is lower than the 60.9% indicated in this survey. Also, described programs were far from comprehensive, with substantial variation across characteristics such as program activities, resources, and integration.
Worksites with fewer employees are less likely, and perhaps less able, to offer health promotion and prevention programs (Linnan et al., 2008). Linnan et al. (2008) found that small employers in each industry were less likely to offer nearly all types of programs and services; sites with more than 750 employees offered more programs. This finding appears to be the case in the present study as well, as all four of the companies with more than 750 employees reported active health and wellness programs. Linnan et al. (2008) also found that 30% of worksites reported programs that had been in existence for at least 6 years. In this study, among the companies with health and wellness programs, 10.5% reported that their programs had been in existence at least 6 years; however, several respondents did not indicate how long their programs had been in place.
Characteristics of Programs
Best practices for workplace health promotion programs suggest several shortcomings in the programs described in this study. Krueger, Brewster, et al. (2007) conducted an extensive review of such programs in the trucking industry and identified 14 fundamental elements. Despite successful participation rates, the programs described in this study lacked most of these fundamental elements. Inconsistent and generally low levels of leadership and support from leadership, limited program evaluation, lack of input from professionals, and underwhelming numbers of partner organizations, deficient participant information, failure to address environmental factors, and limited accountability were found to be common characteristics of health and wellness programs described in this survey. Certain companies came close to meeting the best practices identified by Kruger et al. (2007); however, substantial variation existed among companies, likely perpetuated by the insulated “silo” corporate environments in which these programs exist.
Company Perceptions of Programs
It appears that companies with health and wellness programs consider them to be an important component of their organization, with strong feelings that their programs will expand in the future. Potential expansion implies perceived program value among respondents. Although program evaluation is limited among the study companies, respondents seemingly felt that they generate a satisfactory return-on-investment, to the point that they expect to invest more in these programs despite a dearth of data that address their efficacy and effectiveness.
Perhaps not surprisingly, reasons for implementing these programs center on reducing financial costs related to accident rates, injury claims, and health care costs. One unexpected finding is the fairly low assessment management reported regarding the role these programs play in retention and recruitment of employees, especially compared with the reasons listed above. The turnover rate in the trucking industry is extremely high, with the average tenure of a truckload driver 9 to 12 months (Williams, Garver, & Stephen Taylor, 2011). Despite the impact of turnover on operating costs, customer service, and safety, companies apparently do not believe health and wellness programs are significant factors in retaining current drivers or recruiting new drivers (Williams et al., 2011).
Limitations
The present study has two primary limitations. First, the companies in this sample may not be representative of all trucking companies. The method of distribution of the survey tool was through the ATA, so companies that were not members of this organization at the time of survey distribution were not included in the sample. Given the large number of trucking companies, as well as the diversity among these companies in terms of the number of drivers and company type, achieving a representative sample is complicated. Selection bias may have also occurred because companies with more interest in driver health and wellness may have been more likely to complete the survey. A second limitation is the lack of certainty in terms of response rate, as it was not possible to track precisely how many individual companies received a request to complete the survey. Without knowing the response rate for this survey, the ability to evaluate the representativeness of the sample is diminished.
Toward an “Integrative and Dynamic Healthy Commercial Driving” (IDHCD) Paradigm
Findings suggest that existing commercial driver health and wellness programs are usually based on the assumption that small, isolated inputs (i.e., information about healthful diet) can lead to corresponding proportional outputs (i.e., eating behavior modification; Apostolopoulos, Lemke, Perko, Sonmez, & Hege, 2015). Such assumptions underestimate the complexity of the root causes of driver health, as most occupational health issues are part of complex, dynamic systems; hence, these programs usually only produce underwhelming and unsustainable impacts on driver health (Apostolopoulos et al., 2015). It appears that a new worksite health promotion paradigm that takes these systemic, complex factors into account may be necessary to create meaningful change in driver health outcomes.
The researchers therefore propose a new paradigm that has the potential to substantively improve preventive interventions. The proposed preliminary IDHCD paradigm is based on three assumptions (Apostolopoulos et al., 2015): (a) the integration of primary, secondary, and tertiary prevention and intervention programs; (b) a holistic mental health framework that incorporates multiple, multilevel, complex, and interacting components, emphasizing upstream domains as root causal factors that influence truckers, the transportation sector, and the general population; and (c) the inclusion of key stakeholders across multiple levels of influence with an understanding that consensus among the stakeholders leads to more synergy and improved outcomes.
Critical in the IDHCD paradigm is identifying the feedback mechanisms among the multiple nonlinear causal domains (Apostolopoulos et al., 2015). Feedback mechanisms may be multilevel, diverse, evolving, or time-delayed (Apostolopoulos et al., 2015). These bidirectional interactions produce new, non-proportional properties, while maintaining the system and its environment (e.g., overall trucker health) in a state of constant co-change, which are not captured by traditional approaches (Apostolopoulos et al., 2015). In this context, the development of causal-loop-diagrams (CLDs), models of systems that are simplified representations of parts of reality (Homer & Hirsch, 2006), is a critical component of IDHCD. CLDs require identifying causal factors and their etiology, why they persist and, by connecting these factors in chains of cause-and-effect until feedback loops are formed, how they interact (Apostolopoulos et al., 2015). The development of CLDs is most effective when it occurs through a participatory process, one which involves diverse stakeholders and a conscientious effort to build consensus (Andersen, Richardson, & Vennix, 1997). Stakeholder involvement is also critical for pragmatic reasons, as they will be responsible for initiating interventions based on these models (Vennix, 1999). Because CLD development includes an array of factors and issues to consider, they offer a superior starting point for initiating interventions.
Following CLD development, their hypotheses and theories as well as data and expert input are used to translate the CLD into stock-and-flow diagrams and differential equations, which then become the basis for simulation models (Sweeney & Sterman, 2000). Simulation models provide a more accurate prediction of the effects of interventions in the dynamic and complex environments in which they are implemented, where pathways between intervention and outcomes may be delayed, indirect, or possibly affected by nonlinearities (Levy et al., 2011). Simulation testing provides an understanding of how health trajectories may change under different configurations of truck driver health and wellness programs (Apostolopoulos et al., 2015).
Conclusion
The workplace plays a vital role in population health. For truck drivers this is particularly true, given the unique milieu for these workers. Given the overreliance of truck drivers on their workplaces for access to healthy food, physical activity, and other relevant health protective and promotive resources, these workplaces represent a powerful leverage point for effective interventions to improve population health.
Similar to previous research regarding driver health and wellness programs (i.e., Krueger, Brewster, et al., 2007), the findings of this study suggest the trucking industry currently falls far short of supporting truck driver health and wellness. Judging by what is known about the challenges faced by drivers who attempt to live a healthy lifestyle while on the road as well as by best practices both for driver health and wellness programs and workplace wellness programs in general, the programs described in this study are inadequate to advance health outcomes in a sustainably positive direction. As obesity-related morbid conditions have reached pandemic levels in the general population of the United States, it seems that truckers will experience similar trends, with continued elevated chronic comorbidities. Comprehensive driver health and wellness programs are needed, and a new paradigm for guiding such efforts, the IDHCD paradigm, is recommended.
The IDHCD paradigm has the capability of capturing the complex factors that affect driver health. As a result, the framework can generate more effective and efficacious driver health and wellness programs by using a series of systems-science tools to identify effective leverage points. This paradigm provides a way to create pragmatic interventions that conceptually capture the complex, dynamic nature of sociostructural determinants that affect driver health. Application of this paradigm to driver health interventions could generate the type of comprehensive programs required to create significant, sustainable impacts on driver health. With the growing emphasis on driver health and increasing regulatory pressure that includes expanded health-related requirements to be certified to drive, substantial improvements in driver health have never been more important. Improving commercial driver health is essential for the long-term viability of the trucking industry, and comprehensive health and wellness efforts grounded in these new conceptual and methodological approaches hold the potential for efficacious health protection and promotion programs.
Applying Research to Practice
Commercial motor vehicle driver health and wellness programs are critical to improve health outcomes and productivity for an occupational segment with excessive health disparities. By addressing shortcomings of programs revealed in the current study, potential avenues for improving efficacy and sustainability may be identified. For health practitioners involved in such work, an important guiding principle appears to be the need to provide holistic and comprehensive interventions, following established best practices. It is suggested that health practitioners adopt the Integrative and Dynamic Healthy Commercial Driving Paradigm for the development and implementation of such programs, which is based in systems science and can guide holistic approaches due to its capability of capturing the full array of complex factors which impact commercial motor vehicle driver health and well-being.
Footnotes
Acknowledgements
The authors thank the American Trucking Associations (ATA) for their assistance and cooperation with this study.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Michael Lemke completed his PhD in community psychology from Wichita State University in 2013. He is currently a clinical assistant professor at Texas A&M University and is also a member of the Complexity in Health Research Group at Texas A&M University, which seeks to apply complexity science methodologies to delineate the direct and indirect effects of environments on health, uncover dynamic and interrelated health determinants, and ascertain high-leverage points for interventions to improve population health outcomes.
Yorghos Apostolopoulos is an associate professor at Texas A&M University. He also is the head of the Complexity in Health Research Group at Texas A&M University, which seeks to apply complexity science methodologies to delineate the direct and indirect effects of environments on health, uncover dynamic and interrelated health determinants, and ascertain high-leverage points for interventions to improve population health outcomes.