
Abstract
Background: The demand for home-based health care support providers (HB providers) is growing as the locus of care shifts to private homes. However, industry representative data of these workers are limited. Methods: Washington Behavioral Risk Factor Surveillance System (WA BRFSS) data from 2011 to 2016 were analyzed to compare HB providers (n = 385) with health care support occupations not based in the home, non-HB providers (n = 229), and all other occupations (n = 32,011). Findings: More HB providers were overweight (4.2%, 95% confidence interval [CI] = [3.3%, 5.2%]) than non-HB providers and all other occupations. Significantly more HB providers had arthritis (33.2%, 95% CI = [27.0%, 39.4%]) and diabetes (9.4%, 95% CI = [5.7%, 13.2%]) than non-HB providers. Nearly twice as many HB providers currently smoked (31.3%, 95% CI = [24.2%, 38.4%]) than non-HB providers. Significantly more HB providers reported serious mental illness (6.8%, 95% CI = [2.8%, 10.7%]) than all other occupations (2.2%). Conclusion/Application to Practice: It is imperative to maintain good health in this home-based health care population as these workers are aging and their professional time becomes limited.
Keywords
Introduction
The health care system in the United States is undergoing many dramatic changes including the delivery of health care. The locus of care is shifting from clinical settings, such as hospitals and nursing homes, to communities and private homes, resulting in rapid growth for the demand of home-based care and those who provide that care. In 2016, 3.5 million elderly people (average age of 76 years) received Medicaid home health benefits (Centers for Medicare & Medicaid Services, 2016). The population 85 years of age and older is projected to triple between 2015 and 2050, an age group that will be in most need of assistance with activities of daily living (ADL) such as bathing and toileting (Houser, Fox-Grage, & Ujvari, 2018).
The shift to community-based and home-based care is driving a demand for different types of home-based care providers. In addition to nurses, therapists, and social workers, there are increasing demands for those who provide supportive services. These home-based health care support providers (HB providers) include home health aides, home care aides, and personal care aides. Nationally, the overall employment of home health aides and personal care aides is projected to grow 41% from 2016 to 2026, much faster than the average for all occupations (Bureau of Labor Statistics, U.S. Department of Labor, 2017). In Washington State, the projected growth for home health aides between 2014 and 2024 is estimated at 28%, and the projected growth for personal care aides during this same period is 22% (Projections Central: State Occupational Projections, 2017). The Washington State Employment Security Department estimates that between 2015 and 2016 more than 33,000 home health and personal care aides were employed (Washington State Employment Security Department, Workforce Information and Technology Services, 2017).
As a health care group, until recently, HB providers have not received the same attention as those working in clinical settings. Care practices, health care devices, and workplace policies and programs intended to improve the health and safety of both care providers and care recipients in the clinical setting have been extensively developed and studied. However, the efficacy of these same care practices, health care devices, and workplace policies and programs in the home setting is not clear (National Research Council, 2010). It is important to recognize that home-based health care workers and their work environment are distinct and not an extension of the clinical setting. Home-based health care support providers may have capabilities and limitations that differ from those providing clinical health care support services (non-HB providers), and as such, the needs of HB providers to reduce the risk of injury and illness will differ (National Research Council, 2010). Factors affecting the delivery of care by HB providers may also differ from those factors affecting non-HB providers (National Research Council, 2010). As the need for HB providers continues to increase, it is imperative to gain a comprehensive understanding of the factors that influence their health and well-being, their ability to remain in the profession and deliver care, and the capacity to attract new workers. Care practices, health care devices, and workplace policies and programs unique to the home setting will be essential (Beer, McBride, Mitzner & Rogers, 2014).
The shift of locus of care in health care has created numerous challenges that present risk factors for musculoskeletal disorders (MSDs) and other injuries that are unique to home-based health care (Department of Health and Human Services, 2010b). For example, unlike health care support workers in the clinical setting, home-based health support providers must work in an environment that is rarely designed for the delivery of health care. Care providers in the home most often work alone and cannot rely on assistance from coworkers (Markkanen et al., 2007). For home-based care providers, the workplace is a private residence, meaning they have little or no control over their surroundings (McBride, Beer, Mitzner, & Rogers, 2011). Home-based health care support providers have been found to have high rates of musculoskeletal symptoms (Faucett, Kang & Newcomer, 2013; Myers, Jensen, Nestor & Rattiner, 1993; Torgén, Nygård, & Kilbom, 1995), MSDs from overexertion (Ono, Lagerström, Hagberg, Lindén, & Malker, 1995), back injuries (Myers et al., 1993), and back pain (Quinn et al., 2016).
Among Danish home helpers, Hannerz and Tüchsen (2002) found significantly higher standardized hospitalization ratios for several injuries and diseases, including ischemic heart disease, asthma, emphysema, arthrosis of the hip and knee, and injuries in the lower extremities. In Washington State between 1998 and 2007, home-based care providers had a workers’ compensation claims rate of 1,375 claims/10,000 workers, while the rate for all industries was 862 claims/10,000 workers (Howard & Adams, 2010). The most common body region injured is the back (Lee & Jang, 2016; Quinn et al., 2016; Schoenfisch, Lipscomb, & Phillips, 2017). Meyer and Muntaner (1999) found home health workers had 2.5 times more lost workdays due to injury than nursing home workers. The more common mechanisms of injury include bodily reaction, overexertion, and falls from the same level (Howard & Adams, 2010; Schoenfisch et al., 2017). In another study (Merryweather et al., 2018), home health aides were more likely to have suffered a slip, trip, or fall in the past year compared with therapists and office workers.
Research to develop interventions and identify best practices within the home-based care industry is limited. Olson et al. (2015) used the National Institute for Occupational Safety and Health (NIOSH) Total Worker HealthTM (TWH) perspective (injury prevention plus health promotion) to develop and implement an intervention among home care workers in Oregon. Following monthly team meetings providing education and social support, participants reported a reduction in physical symptoms and improvements in well-being.
Representative data of the home-based care experience are also limited. The National Home Health Aides Survey (NHHAS), administered in 2007, was the first national probability survey of home health aides, collecting data from 3,416 interviews (Bercovitz et al., 2010). Although this survey gathered data on general injury types (mostly associated with patient handling), it did not inquire about diseases or chronic illnesses. In addition, questions of health behaviors were not included. No follow-up study has been conducted. The Long-Term Care Statistics Branch in the Division of Health Care Statistics at the National Center for Health Statistics (NCHS) uses the biennial National Study of Long-Term Care Providers to provide national and state statistical information about the supply, provision, and use of long-term care services. A 2011 report from the National Research Committee on the Role of Human Factors in Home Health Care (National Research Council, 2010) put forth several recommendations to address a range of issues that affect the safety, quality, and effectiveness of home health care. One of these recommendations was to capture comprehensive information on the elements relevant to health care in the home, including collection of data on the sociodemographic characteristics of those individuals providing health care in the home, the nature of caregiving they provide, and the attributes of the residential setting in which the care recipients live.
Occupational safety and health professionals should focus prevention efforts on this unique population of at-risk workers, especially as this industry grows. Foundational work to better understand the socioeconomic status, health status, and behaviors of home-based care workers will provide insight into the risks they face and potential impacts on patient care, and inform prevention efforts. Therefore, we analyzed the Washington Behavioral Risk Factor Surveillance System (WA BRFSS) to characterize HB providers, and compared this group with other health care support occupations not based in the home, and a second group of the general working population.
Method
The BRFSS is an annual telephone survey sponsored by the Centers for Disease Control and Prevention (CDC, 2018a) to collect information on health outcomes and behaviors in all 50 states, the District of Columbia, and three U.S. territories. The survey comprised standard core questions that must be asked by all states. Rotating questions are asked by all states every other year. In addition, states have the option of including additional questions. A multistage design and random-digit dialing are used to obtain representative samples of noninstitutionalized adults (i.e., adults aged ≥18 years in a private residence or college housing). Landline and cell phone numbers have been included in the sampling frame since 2011, with an increasing proportion of the annual sample from cell phone surveys each year in Washington State. Also in 2011, the survey weighting methodology changed, and therefore, data collected prior to 2011 cannot be combined nor compared with data collected after that year.
In Washington State, a health research company, on behalf of the Washington State Department of Health, conducts the survey. Interviews must be conducted according to BRFSS protocols, which include asking all of the standard core questions without modification. Trained coders assign industry and occupation codes to verbatim responses each year through automated and manual coding processes.
Workers were classified by occupation and industry using the 2000 Standard Occupational Classification (SOC) codes and the 2000 and 2002 Census Industrial Classification systems. Workers were then categorized into three different occupational groups. Home-based health care support providers included personal and home care aides (SOC: 39-9021) and home health aides (SOC: 31-1011), who indicated they worked for home health care services (Industry Codes: 817, 8170), individual and family services (Industry Codes: 837, 8370), or private households (Industry Codes: 929, 9290). Other health care support occupations not performed in-home (non-HB providers) included all health care support occupations included under SOC codes 31-1010, 31-2010, 3-2020, 31-9010, and 31-9090. Excluded from this occupational group were personal and home care aides and home health aides, who indicated they worked for any of the following: offices of physicians, dentists, chiropractors, or other health practitioners (Industry Codes: 797, 7970, 798, 7980, 799, 7990, 808, 8080); outpatient care centers (Industry Codes: 809, 8090); other health care services (Industry Codes: 818, 8180); hospitals (Industry Codes: 819, 8190); nursing care facilities (Industry Codes: 827, 8270); or residential care facilities, without nursing (Industry Codes: 829, 8290). Any other worker not defined in the above was included in the final group of “All Other Occupations.”
WA BRFSS data from 2011 to 2016 were extracted and combined for this study (n = 81,170). For this analysis, only those respondents who indicated that they were employed for wages (n = 32,028), self-employed (n = 6,429), or out of work for less than 1 year (n = 1,986) during this period were included. The annual response rates in Washington State during this time period ranged between 31% and 44% (CDC, 2011/2016b). The distribution of select demographic characteristics and indicators of general health status, access to health care, chronic health conditions, injuries and risk behaviors, and occupational health were compared across the three groups of workers described above.
Demographics and general health status measures were on the CDC (2011/2016a) core portion of the BRFSS survey and collected by all states. Health care access questions were included on the WA BRFSS surveys as optional modules; only select states collected these data (CDC, 2011/2016a). Lifetime prevalence estimates of health care conditions were collected by asking respondents whether a “doctor, nurse, or other health care professional has ever told you that you have” the specific condition. Lifetime prevalence of asthma, arthritis, diabetes, and depression was included on the CDC core (CDC, 2011/2016a). The Kessler Psychological Distress Scale (K6) was used to measure psychological distress, such as anxiety and depression (Kessler et al., 2002). This measure included questions about feelings of depression, hopelessness, restlessness, fatigue, worthlessness, and nervousness. A “falls” module has been rotated on the CDC core every other year and collected incidence of falls (unintentionally coming to rest on the ground or another lower level) among adults aged 45 years and older. Washington State included a state-added question on the WA BRFSS to collect work-related injury and illness incidence by asking, “In the past 12 months, have you been injured while performing your job, or has a doctor or other medical professional told you that you have a work-related illness?” Finally, smoking and binge drinking behaviors were included on the CDC core questionnaire each year. Binge drinking was defined as four or more drinks for a woman or five or more drinks for a man on an occasion during the past 30 days (CDC, 2018b).
Since 1995, the Washington State Department of Labor and Industries has sponsored additional questions on the WA BRFSS to collect working respondents’ current industry and occupation with the following questions: “What is your job title?” (occupation) and “What kind of work do you do?” (industry).
Data Analysis
Descriptive statistics of demographic and occupational characteristics, including means and proportions, were calculated with their respective 95% confidence intervals (CI) for comparison across workers. All estimates presented here were weighted, and missingness was not assumed to be completely at random (missing completely at random [MCAR]). BRFSS weights were developed using a standardized ranking procedure that took both survey design and population demographics into consideration. Employment status, industry, and occupation were not included in the weight calculations, however. Statistical significance was evaluated in this analysis by examining the overlap of CI. The coefficient of variation (CV) was calculated and reviewed for all estimates as a measure of instability; any estimate with a CV above 25% was flagged, and all estimates with a CV above 50% were suppressed (or not shown).
Results
During the period 2011-2016, a total of 385 WA BRFSS participants were identified as home health, personal, and home care aides working in the home environment (HB providers). The first comparison group, Health Care Support Occupations not in the home environment (non-HB providers), had a total of 229 respondents during the same time period. The second comparison group (All Other Occupations) comprised the remaining working respondents and consisted of 32,011 respondents.
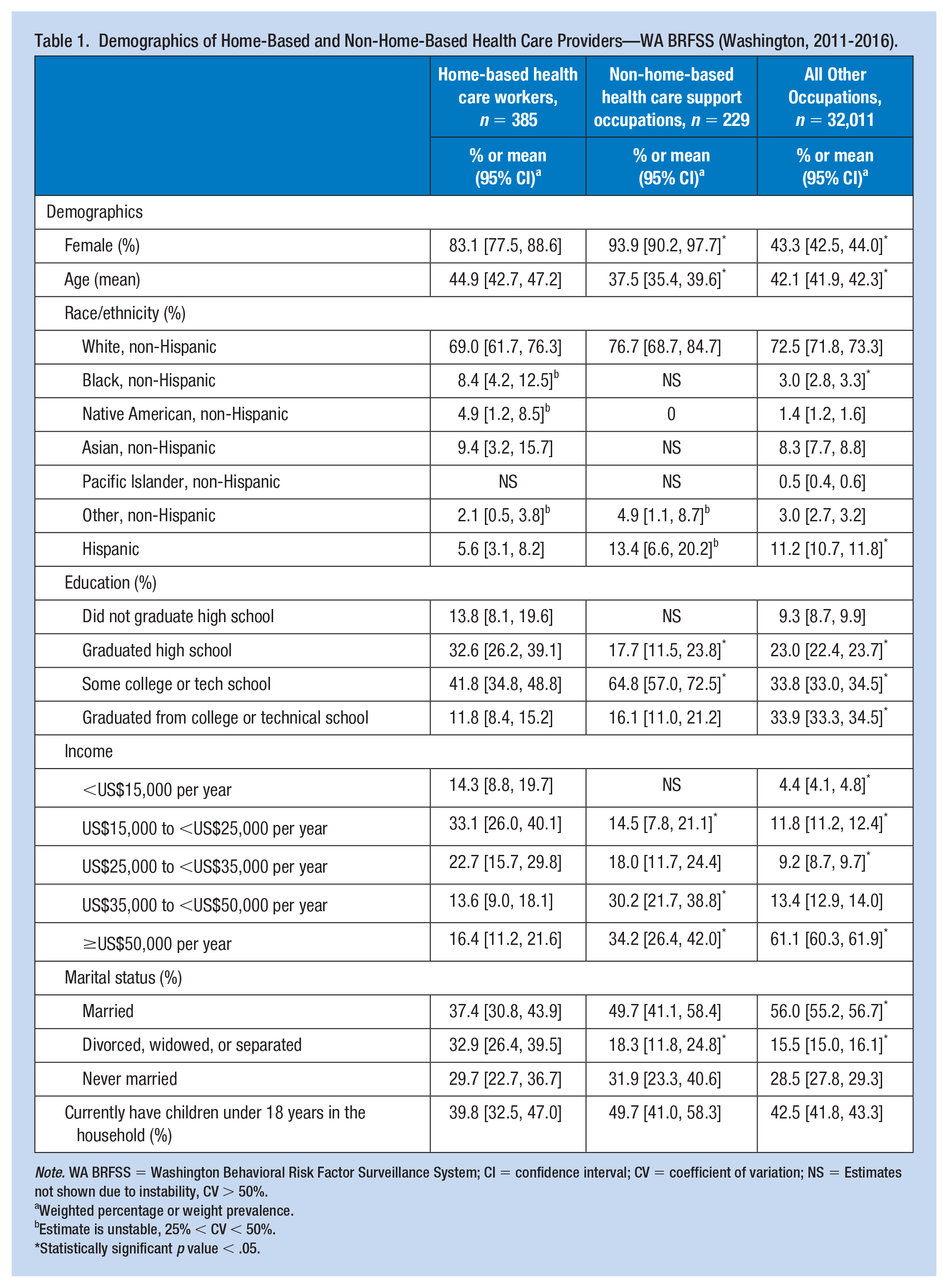
The demographics of the three groups (HB providers, non-HB providers, and All Other Occupations) are shown in Table 1. The health care occupations primarily comprised of women (83.1% HB providers, 93.9% non-HB providers). Home-based health care support providers had a mean age of 44.9 years, which was significantly older than non-HB providers by 7 years, and older than All Other Occupations by 3 years.
Demographics of Home-Based and Non-Home-Based Health Care Providers—WA BRFSS (Washington, 2011-2016).
Note. WA BRFSS = Washington Behavioral Risk Factor Surveillance System; CI = confidence interval; CV = coefficient of variation; NS = Estimates not shown due to instability, CV > 50%.
Weighted percentage or weight prevalence.
Estimate is unstable, 25% < CV < 50%.
Statistically significant p value < .05.
Although not significant, fewer HB providers were non-Hispanic White (69.0%) than non-HB providers (76.7%) and All Other Occupations (72.5%). Compared with All Other Occupations, significantly more HB providers were non-Hispanic Blacks and significantly fewer were Hispanic (8.4% vs. 3.0%, non-Hispanic Black; 5.6% vs. 11.2%, Hispanic). The HB provider sample also had more Native American (4.9%) and Asian workers (9.4%) than the All Other Occupations group (1.4% and 8.3%, respectively).
Significantly fewer HB providers graduated from college or technical school compared with non-HB providers and All Other Occupations. Annual household income was lowest among HB providers, with close to half (47.4%) reporting a household income of less than US$25,000 per year. More HB providers were divorced, widowed, or separated (32.9%) than the comparison groups (non-HB providers, 18.3%; All Other Occupations, 15.5%). There were no significant differences in currently having children in the household among the three groups.
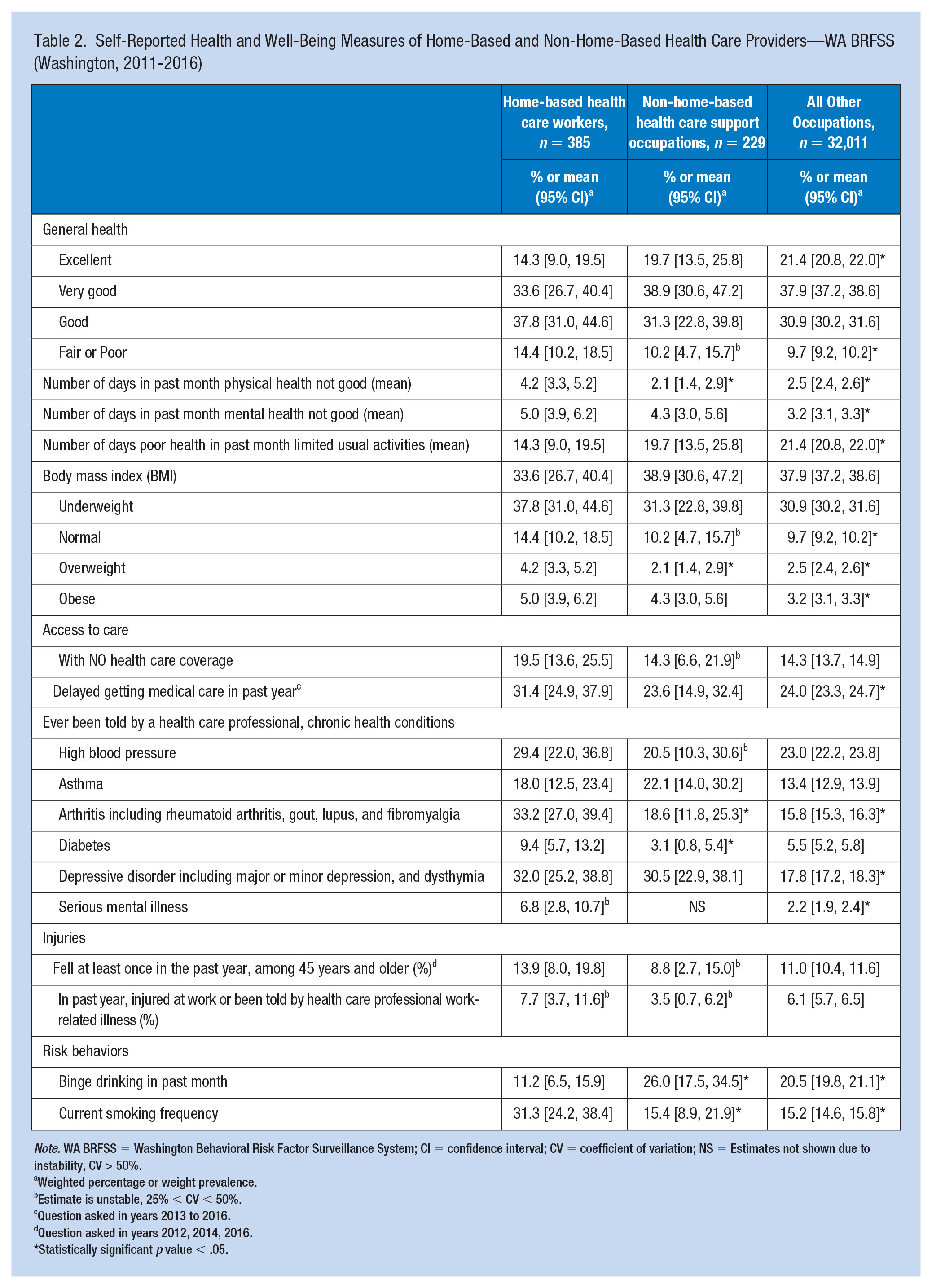
Self-reported measures of health and behavior between the three occupational groups are described in Table 2. General health status was not as good for HB providers compared to non-HB providers and the general working population. More HB providers reported fair or poor health (14.4%) relative to non-HB providers (10.2%) and significantly more than All Other Occupations (9.7%). Conversely, fewer HB providers reported excellent health (14.3%) compared with non-HB providers and All Other Occupations (19.7% and 21.4%, respectively). Home-based health care support providers reported approximately twice as many days in the past month when physical health was not good compared with non-HB providers (4.2 days vs. 2.1 days) and All Other Occupations (2.5 days). The number of days mental health was not good in the past month was similar among HB and non-HB providers, but the provider groups reported significantly more poor mental health days compared with All Other Occupations (5.0 and 4.3 days vs. 3.2 days, respectively). More HB providers reported barriers to accessing health care than the other two occupation groups, although the wide CIs around the HB provider estimates generally overlapped and were therefore not statistically significantly different using the criterion outlined in the methods.
Self-Reported Health and Well-Being Measures of Home-Based and Non-Home-Based Health Care Providers—WA BRFSS (Washington, 2011-2016)
Note. WA BRFSS = Washington Behavioral Risk Factor Surveillance System; CI = confidence interval; CV = coefficient of variation; NS = Estimates not shown due to instability, CV > 50%.
Weighted percentage or weight prevalence.
Estimate is unstable, 25% < CV < 50%.
Question asked in years 2013 to 2016.
Question asked in years 2012, 2014, 2016.
Statistically significant p value < .05.
Significantly more HB providers reported arthritis (33.2%) and diabetes (9.4%) than non-HB providers (18.6% for arthritis, 3.1% for diabetes). More HB providers reported depressive disorders than non-HB providers (32.0% vs. 30.5%), although this difference was not significant. Compared with All Other Occupations, HB providers reported a significantly higher rate of serious mental illness (2.2% vs. 6.8%). Nearly 30% of the HB providers indicated that they suffered from high blood pressure (HBP), although this was not significantly different from the other two occupational groups. There were no statistically significant differences in falls among those 45 years of age and older, nor in work-related injuries and illnesses, although the estimates were over 1.5 times greater for HB providers compared with non-HB providers for both injury indicators. Binge drinking was reported among significantly fewer HB providers compared with the other two groups. Approximately twice as many HB providers reported currently smoking (31.3%), a significantly higher prevalence than non-HB providers (15.4%) and All Other Occupations (15.2%).
Discussion
With the increasing demands for home-based care, it is imperative that this industry attract and retain HB providers. However, the results of this analysis suggest that HB providers may have differing underlying health issues or work environment issues from other occupational groups that make meeting the demand difficult. In addition to understanding the health and well-being of this little studied working population, comparisons with other occupational groups will provide insight into the value placed on HB providers and the implications for the safety, quality, and effectiveness of care in the home environment. The WA BRFSS provides a population-based sample of Washington adults that allows us to describe the socioeconomic status, health and well-being, and risk behaviors of HB providers and to compare this sample with non-HB providers and all other occupations (the general working population).
Like non-HB providers, the majority of HB providers in this BRFSS data sample were female, as has been described by other studies of home-based care providers (Hayashi, Gibson, & Weatherley, 1994; Kim, Geiger-Brown, Trinkoff, & Muntaner, 2010; Schoenfisch et al., 2017). Women’s participation in health care professions dominated by males is expanding, although traditionally women’s role in health care has been centered around support occupations such as nursing.
The HB providers were, on average, 7 years older than non-HB providers. According to a 2014 report by the Paraprofessional Healthcare Institute (PHI, 2014), approximately 70% to 80% of the paid long-term health care services is provided by home-based care providers where the proportion of women aged 55 years or older is increasing. In 2014, 28% of home care providers were 55 years or older (PHI, 2016). Bercovitz et al. (2011) found that 27% of the 2007 NHHAS population was 55 years or older. As the overall population is aging, so are HB providers. In general, HB providers appeared to be in poorer health than non-HB providers. Significantly more HB providers reported being overweight, and having more days when physical health was not good, whereas only slightly more reported depressive disorders. Home-based health care support providers also reported the highest rates of arthritis, diabetes, HBP, and smoking. Type 2 diabetes (Abdullah, Peeters, de Courten, & Stoelwinder, 2010), knee osteoarthritis (Lee & Kean, 2012), and hypertension (Ostchega, Hughes, Terry, Fakhouri, & Miller, 2012) have been associated with obesity. Although there is no direct link between smoking and HBP, the combination of the two increases the risk of cardiovascular disease (Department of Health and Human Services, 2010a). The results of this study suggest that HB providers are experiencing the same age-related diseases, impairments, and functional limitations as the general population, which may require greater accommodation to do their job. Caregivers may also be leaving the home-based support professions at a faster rate than the younger population of non-home-based health care support workers.
The differences in mental health between HB providers and the general working population may present a challenge to providing care for HB providers. Significantly more HB providers reported depressive disorders and serious mental illness. Poor mental health among health care professionals has been found to be associated with reduced patient safety (Hall, Johnson, Watt, Tsipa & O’Connor, 2016; Suzuki et al., 2004; Welp, Meier & Manser, 2015).
Though not statistically significant, more HB providers above the age of 45 reported a fall in the past year than non-HB providers (1.5 times more). This question is only asked of a subgroup of BRFSS respondents (age 45 years and older) and only included every other year, so a small sample size is likely influencing the ability to achieve statistical significance for these estimates. However, the fall risk for HB providers is clear. With aging, and declines in postural control, reflexes, muscle strength, and tone, the ability to arrest a fall after a trip or slip is impaired (Rubenstien, 2006). Age-associated declines in vision and hearing may also contribute to slip, trips, and falls (STFs). Howard and Adams (2010) reported that the second most common type of accident workers’ compensation claims among home care services in Washington was falls on the same level. Patient care factors associated with STFs in home health care include feeling rushed or hurried, the total number of patients in a week, and patient weight-bearing status (Merryweather et al., 2018). Home conditions, in which home-based health care providers may not have control over, were also associated with STFs, including access to the bed or toilet, hazardous stairways, and walking obstacles (Merryweather et al., 2018). Finally, comorbid conditions such as diabetes are also known to increase fall risk (Yang, Hu, Zhang, & Zou, 2016).
More HB providers reported a work-related injury or illness than non-HB providers and the general working population, though not statistically significantly different. Other research has described the risk of work-related injuries and illnesses in home-based care (Faucett et al., 2013; Merryweather et al., 2018; Meyer & Muntaner, 1999; Quinn et al., 2016). Torgén et al. (1995) described the high physical demands of home-based care. Home-based health care support providers are caring for a heavier population with more needs. The proportion of adults, 20 years and older, with a body mass index of 30 or more increased between 1999 and 2014 (NCHS, 2016). Caffery, Sengupta, Moss, Harris-Kojetin, and Valverde (2011) reported that among home health care patients with at least one ADL limitation in 2007, just over half had four to five ADL limitations and more than one fifth had three limitations. And in the home setting, because of lack of control of environment and lack of assistance, musculoskeletal risk factors are magnified (Galinsky, Waters, & Malit, 2001). Patient handling equipment, such as sit-to-stand or total body lifts, is not as pervasive in the home setting as it is in the clinical setting. While this type of equipment is available to non-HB providers by a facility as part of patient care, the same is not true for HB providers where the patient must provide the equipment. Consequently, non-HB providers have more control of their surroundings and have more access to additional help, equipment, and devices that reduce risk of injury.
The majority of HB providers reported their general health status as good or better; however, previous research suggests that underreporting of injuries occurs in this working population. It has been found that despite the high prevalence of injuries, home-based care providers most often self-report their health status as good (Anderson et al., 2013; Faucett et al., 2013; Yoon, Probst, & DiStefano, 2016). Hansell, Knaster, and Phillips (2018) described that over a third of respondents of a home care survey reported moderate to high levels of hesitancy in reporting on-the-job injuries. To reduce the severity of injuries and illnesses, the barriers to reporting or seeking treatment for work-related injuries and illnesses must be identified.
Estimates of race and ethnicity were largely unstable among the HB and non-HB providers due to small numbers; however, overall fewer HB providers were non-Hispanic White than non-HB providers and All Other Occupations. A greater proportion of HB providers self-reported as non-Hispanic Black and Asian compared with the group of All Other Occupations excluding health care support. Racial disparity may actually be greater than what was found in this analysis because WA BRFSS interviews are conducted only in English and Spanish, and a larger sample size is needed for more stable estimates among the HB and non-HB providers. Population (not sample) data find double the proportion of non-Hispanic Blacks in the Health Care and Social Assistance sector than BRFSS reports. In Washington State during the first quarter of 2017, 74% of the workers in Health Care and Social Assistance were White, and 16% were Black of non-Hispanic heritage (Washington State Employment Security Department, Workforce Information and Technology Services, 2017). Racial distributions appear to be regionally based. While Montgomery, Holley, Dichert, and Kosloski (2005) found more than half of the personal and home care aides in the 2000 Census were White and a quarter were African American, in a study of home care providers in a large West Coast city, Kim et al. (2010) found the majority to be non-Caucasian. Another study, conducted in Maine, had a sample of predominantly White respondents (Butler, Brennan-Ing, Wardamasky, & Ashley, 2014), while the study sample of Quinn et al. (2016) had equal proportions of White and Black HB providers.
A living wage is essential to attracting people to a profession. High wages and health benefits have been found to reduce turnover, as well (Butler et al., 2014; Butler, Wardamasky, Brennan-Ing, 2012; Morris, 2009; Rosen, Stiehl, Mittal, & Leana, 2011). The annual income of HB providers in WA BRFSS was significantly less than that of non-HB providers and All Other Occupations. Close to half, 47.4%, of the HB providers in this study reported less than US$25,000 annual household income, suggesting many may only be working part-time or part-year. A similar finding of part-time work was reported by Montgomery et al. (2005). Non-HB providers are better paid, with less than 15% reporting an annual income of less than US$25,000. Nationally, the median annual pay for home health aides and personal care aides in 2017 was US$23,130 (Bureau of Labor Statistics, U.S. Department of Labor, 2017). In Washington State, the annual wage for home health aides is US$26,336 and for personal care aides, US$26,614 (Washington State Employment Security Department, Workforce Information and Technology Services, 2017). This salary is barely above the 2018 federal poverty level for a household of four (US$25,000 per year). A greater proportion of the HB providers also reported being divorced, separated, or widowed, which indicates more of these workers may be the head of single-income households compared with other workers. Montgomery et al. (2005) found the same result in a comparison between aides in home care, nursing homes, and hospitals.
Estimates from WA BRFSS indicate greater barriers to health care for HB providers than the other two groups—36% more HB providers were estimated to not be insured and 24% more delayed getting needed medical care than the other groups, although estimates were not statistically significantly different. Home-based health care support providers may be working longer with injuries than non-HB providers, potentially increasing the severity of their injuries and negatively affecting patient care. Bercovitz et al. (2011) found that aides working for home health agencies were less likely to have access to health insurance than aides working for agencies offering hospice care. The lack of health care coverage or the inability to seek medical care due to costs has also been associated with poorer health outcomes (Hoffman & Paradise, 2008).
In this BRFSS sample, HB providers had overall lower educational attainment than non-HB providers. Home-based care requires minimal education (a high school diploma or equivalent), experience, or training, making this profession an easily entered occupation. In Washington State, caregivers in the home are certified by the Department of Health, with the exception of family members. Certification involves 75 hours of training and the successful passing of the certification examination. The WA BFRSS sample representing non-HB providers included dental assistants, massage therapists, medical assistants, and occupational and physical therapy assistants, all of which are considered health care support occupations and all of which have higher educational requirements than the occupations representing HB providers. Unlike the occupations in the non-HB provider group, those in the HB provider group can be characterized as low-status occupations—low wages, lack of health coverage, and low education attainment. The combination of lower wages creating financial pressures on HB providers and less opportunity for economic mobility due to low education attainment compared with other workers makes them especially vulnerable to unsafe working conditions (Steege, Baron, Marsh, Menéndez, & Myers, 2014).
The differences in age, race, education, and gender found between HB providers and All Other Occupations may have implications for the relationship between HB providers and care recipients, affecting the care provided. As the racial diversity in the United States continues to grow, the importance of patient–provider concordance may play a role in quality of care. Although the specific relationship between HB providers and care recipients has not been examined, nor the effect of concordant patient–provider relationships on the provider experience, concordance between physicians and patients has been heavily studied with regard to quality of care. Blanchard, Nayar, and Lurie (2007) found that the association between racial concordance between patients and providers and perceived disrespect varied by patient racial group. Perceived personal similarities in beliefs, values, and communications can strengthen the patient–provider relationship and have been associated with higher ratings of trust, satisfaction, and intention to adhere by the care recipient (Street, O’Malley, Cooper, & Haidet, 2008).
Strengths and Limitations
Using the WA BRFSS data, we were able to describe individual characteristics among specific populations of workers at the state level. This study provides descriptions of an at-risk group of workers, home health care providers, that can be used to inform occupational safety and health prevention messaging. Other similar data sources are not able to provide state-level estimates on this specific population, nor do they collect information on demographics, health, and risk behavior indicators. This study is also subject to several limitations. Some estimates for specific indicators among HB and non-HB providers were unstable and had relatively wide CIs, inhibiting the ability to achieve statistical significance among indicators where point estimates were substantially different. This is an indication of high variability, which would likely be reduced with an increased sample size. The BRFSS is a self-report survey and is therefore subject to recall and social desirability biases. Although responses to BRFSS are weighted to the general adult population in Washington State, weighting neither includes industry nor occupation. Therefore, responses here may not be representative of the HB provider population in Washington.
Implications for Occupational Health Nursing Practice
It is imperative to maintain good health among home-based health care providers, as the shortage of these workers is exacerbated by the increased demands for services and trained providers leaving the profession. The limited data on the work environment and the factors that may contribute to occupational injuries make it difficult to inform the development of policies and prevention strategies for workplace injuries. Occupational health professionals need a comprehensive understanding of the unique work environment of home-based care. The results of this study suggest that occupational health professionals will need to develop and implement health and safety programs and services that consider a working population that is older and suffering from more chronic health conditions than those providing care in hospitals or nursing homes.
Besides the mitigation of commonly identified physical risk factors, such as manual patient handling, injury prevention must consider other factors that increase the vulnerabilities to injury. A human-systems perspective considers the interaction between these factors, which includes low compensation, the intimate relationship between care recipient and provider, the health status and capabilities of the care recipient and provider, the complexities of the care tasks, and the technologies available.
Total Worker Health (TWH), an integrative approach from the National Institute of Occupational Health and Safety, may provide a basis for improving worker health and safety in this population. The approach of TWH integrates the prevention of work-related health and safety hazards with activities that promote overall well-being of workers. TWH expands the traditional focus of occupational health and safety to identify and reduce the potential harm from the work itself to include the work experience. In the home environment, where there may be very little control over the built environment, interventions may include the design of work schedules that reduce stress and increase worker control, policies that promote healthy supervision and increase the value of and respect for workers, and programs that encourage worker engagement and recognition.
Applying Research to Practice
The demand for home-based health care support providers (HB providers) is growing as health care shifts to private homes. Our study compared health status indicators for HB, non-HB healthcare providers, and all Other Occupations and found that, in general, HB workers were more likely to have adverse health outcomes, and were more likely to engage in unhealthy behaviors, such as smoking than the other work groups. The health of HB providers is critical to ensuring that these workers are able to deliver care to those who need it most.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by grant number U60 OH008487 from CDC-NIOSH and the Washington State Department of Labor and Industries. The Washington BRFSS (WA BRFSS) is supported in part by the Centers for Disease Control and Prevention, Cooperative Agreements U58/SO000047-2 (2012), U58/SO000047-3 and 3U58SO000047-02W1 (2013), U58/SO000047-4 and 3U58SO000047-03W1 (2014), U58/DP006066-01 (2015), and U58/DP006066-02-02 (2016).
Author Biographies
Ninica Howard, MS, CPE, a research ergonomist with the SHARP Program, received her MSc in Work Environment from the University of Massachusetts Lowell. She has performed research in several health care settings, including hospitals and nursing homes.
Jennifer Marcum, DrPH, an epidemiologist with the SHARP Program, received her DrPH from the University of Kentucky. She has performed research in injury surveillance at the state and local government setting.