
Abstract
Context. An instrument is needed to facilitate a brief, but effective, counseling interaction between a patient and a provider. Such an instrument should raise patients’ awareness of their behavioral patterns and indicate their likelihood of weight loss statistically. Objective. To determine if the Lifestyle Questionnaire–Weight Management (LQ-WM) contains statistical properties that discriminate subjects’ weight trajectories. Design and Participants. A convenience sample of 269 college students at Utah Valley University in Orem, Utah, were administered the LQ-WM and a weight history questionnaire. Main Outcome Measure. A Lifestyle Score was created by subtracting the amount of self-reported unhealthy behaviors from the amount of healthy behaviors in the previous week. Results. The Lifestyle Score was significantly different among subjects who reported recently losing, maintaining, or gaining weight recently (P < .001) and in the previous year (P < .05). The Lifestyle Score was also significantly different among individuals losing weigh rapidly, moderately, and slowly (P < .05). Conclusions. This pilot study of the statistical properties of the LQ-WM supports that higher Lifestyle Scores associate with weight loss cross-sectionally. Future studies should examine its statistical properties longitudinally and with diverse samples to assess its suitability for clinical practice.
‘Self-monitoring instruments can be helpful in counseling sessions to raise patients’ awareness of behaviors related to weight loss.’
Obesity and Counseling
Obesity is associated with adverse health outcomes, 1 and in the United States, approximately two thirds of adults are overweight or obese. 2 In response to the obesity epidemic, the 2012 United States Preventive Service Task Force recommended intense weight management counseling and behavioral interventions for obese patients. 3 Despite this, weight management counseling from health care providers to obese patients often does not occur during visits. One analysis found that rates of physicians providing counseling to obese patients actually declined from 39.9% to 29.9% from 1996 to 2006 despite the sharp increase in the prevalence of obesity in the United States. 4 It is unfortunate that more counseling interactions between physicians and patients are not undertaken since a meta-analysis found a positive association between physician encouragement for behavior change and weight loss success. 5 Physicians have cited avoiding weight management counseling with their obese patients due to discomfort with counseling, doubt that people can change behaviors, and time constraints. 4 However, avoiding counseling opportunities makes it less likely that patients will engage in multiple long-term behavior changes that are recommended for sustained weight loss.6,7 Additionally, since sustained weight loss has proven difficult, more strategies are needed to encourage the prevention of excess weight gain. A tool that facilitates counseling sessions for health care providers and allows the patient to track multiple behavior changes for long-term success and weight gain prevention is needed.
Self-monitoring instruments can be helpful in counseling sessions to raise patients’ awareness of behaviors related to weight loss. Furthermore, increased self-monitoring of behaviors has been associated with success in weight loss. 8 A review of self-monitoring devices highlighted that these instruments tend to focus on dietary monitoring, self-monitoring of exercise, and self-weighing. 9 Different modalities of self-monitoring consist of paper diaries and use of electronic devices. Despite the usefulness of these self-monitoring instruments in facilitating weight loss, such instruments have limitations for encouraging quality counseling sessions between patients and health care providers. For example, there appears to be a lack of attention toward tracking emotional states that are common during weight loss attempts and is essential to holistic treatment of the patient. The quality of a physician’s counseling session has been associated with increased patient motivation to engage in weight loss behaviors. 10 Behaviors such as emotional eating, depression, and body dissatisfaction can also serve as predictors of weight gain.11-13
Additionally, the patients’ level of motivation to change various behaviors is an important component of a counseling session, which does not seem adequately addressed in current self-monitoring systems. Motivational interviewing is a counseling technique commonly implemented to counsel patients when making behavioral changes are recommended for optimal health. The basic premises of motivational interviewing are to allow patients to explore their ambivalence regarding behavior change, show empathy, highlight discrepancies in their goals and behaviors, follow along with the patients’ resistance to change, and to support their self-efficacy for change. 14
The need for an instrument to address the appropriate dose for self-monitoring for success has been noted previously. 9 Recommendations for the proper behavioral dosage for weight loss success could be helpful to patients who view weight management as a confusing endeavor in which they have little hope for success. Consequently, this study is an initial effort to answer that unmet need, and the goals of the current project are to (1) assess whether the Lifestyle Score from the Lifestyle Questionnaire–Weight Management (LQ-WM) is associated with varying weight trajectories and (2) explore behavioral dose recommendations for weight loss based on differences between weight gainers, maintainers, and losers.
Method
Participants
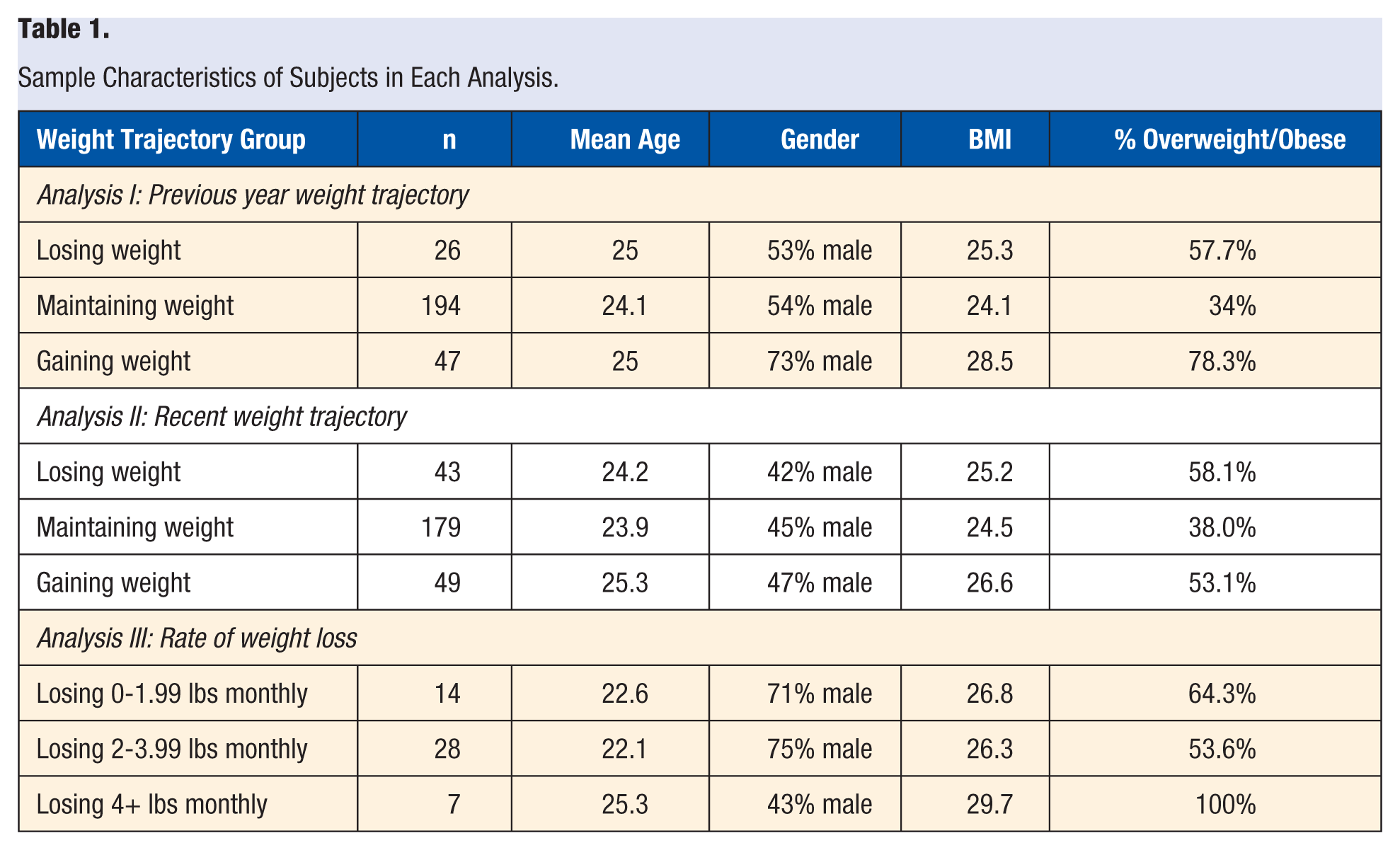
Two hundred and seventy-four participants were acquired from a general behavioral weight management project at Utah Valley University conducted from July to November 2015. Of those, 269 provided sufficient information to be included in the first analysis examining weight trajectories in the previous year and 271 were included in the second analysis examining recent weight trajectories. The third analysis included 49 participants who indicated they were currently trying to lose weight. The sample was predominately Caucasian. See Table 1 for more sample characteristics.
Sample Characteristics of Subjects in Each Analysis.
Measures
The Lifestyle Questionnaire–Weight Management
This instrument consisted of 23 items that enquire about the frequency of weight management behaviors in the previous week with regard to nutritional, emotional, and physical activity patterns. The questionnaire is divided into 3 main sections (available online at http://ajl.sagepub.com/supplemental). The items in the first section are related to healthy weight management practices and are provided below:
“In the last week, how many days did I . . .”
Read food labels
Track calories
Plan meals
Eat breakfast
Modify meals in a healthy way (eg, take smaller portion sizes)
Check my weight
Find opportunities for increased exercise (eg, take the stairs)
Consume 4+ cups of water
Receive adequate sleep
Perform 30+ minutes of exercise or take 10 000+ steps
Reach a calorie goal
The second section contains items enquiring about unhealthy behaviors and negative emotions as noted below:
Eat as a response to stress or boredom (emotional eating)
Feel significant sadness or negative emotions
Eat while watching TV
Eat fast food
Feel significant guilt or shame about eating
Drink soda or other sweetened drinks
Spend 2+ hours watching TV or playing video/computer games
“Binge” (eating a meal above 2000 calories) or “Purge” (trying to get rid of recently eaten food via throwing up or laxatives)
The third section of the questionnaire was designed for counseling purposes to assess motivation levels, body image concerns, and confidence in weight management. It contains the 3 questions noted below:
From 0 to 100 (0 = no motivation and 100 = very high motivation), please rate your current motivation level to engage in increased physical activity, modification of your diet, other behaviors (eg, calorie tracking).
On a scale from 0 to 100, how comfortable are you with the shape or size of your body? (0 = I am extremely uncomfortable with the shape or size of my body and 100 = I am extremely comfortable and confident with my body).
On a scale from 0 to 100, how confident do you feel with your ability to manage your weight? (0 = I feel I have no control over my weight and 100 = I feel totally in control of my weight).
Composite Scores and Groups
A composite Lifestyle Score was created for each subject based on the calculation below:
Food labels + Track calories + Plan meals + Eat breakfast + Modify meals + Check weight + Find opportunities for physical activity + Drink 4 cups of water or more + Get adequate sleep + Exercise 30 minutes + Reach a calorie goal − Hard emotional days − Eat while watching TV − Eat fast food − Consume drinks with calories − Watch TV or play video games 2 hours or more − Binge or purge − Eat due to stress or boredom
The Healthy Behavior Composite Score was calculated by summing the healthy behaviors listed above, whereas the Risk Factor Composite Score was calculated by summing the unhealthy behaviors noted above. Finally, Lifestyle Group Scores were created by assigning score ranges below 0, between 0 and 24, between 25 and 49, and more than 50 into different behavioral risk groups. Since a main purpose of this questionnaire is to create an easy-to-use instrument for clinicians, the cutoff scores for this pilot study were selected for practical and theoretical reasons, that is, intervals of 25 are simple to remember and that each score group would contain some face validity of lifestyles at high, moderate, low, and very low risk of weight gain. The sample sizes for each group in this sample are as follows: n = 18 for the below 0 group; n = 129 for the 0 to 24 group; n = 103 for the 25 to 49 group; and n = 17 for the 50+ group. Although the lowest and highest groups only represent 13% of the total sample, such a distribution seems adequate at this stage of research to assess outcomes of at-risk and exemplary lifestyles. However, as more data are gathered other cutoff scores that are practical, yet more statistically sound, may be preferable.
Weight History
A weight history questionnaire was also employed that contained 15 items related to participants’ demographics, average weight by year for the past 5 years, history of unhealthy weight management practices, and current fitness goals (see the appendix).
Procedure
This study was approved by the institutional review board (IRB) at Utah Valley University (assigned IRB Tracking Number 01388). Participants were recruited in 2 ways: approximately half of the sample volunteered to participate in the hallways at Utah Valley University as research assistants stood by a table advertising the study. After providing informed consent verbally, participants first completed the weight history questionnaire followed by the LQ-WM. The second half of participants were recruited from Introductory to Psychology classes, which required students to either participate in original research or write a paper about research—only one student chose the latter.
The first analysis divided participants into 3 groups based on their weight history in the last year. The groups consisted of individuals who had lost at least 10 lbs in the previous year (weight losers), those who have kept their weight within 5 lbs of the previous years’ weight (weight maintainers), and those who have gained at least 10 lbs in the previous year (weight gainers). Only 7 participants were dropped from the analysis for not meeting the criteria described above. Further characteristics of the remaining participants are provided in Table 1.
A second analysis examined recent weight loss patterns by dividing respondents based on their answers to the question, “Recently it seems like I’ve been gaining, maintaining, or losing weight.” A third analysis examined differences in individuals based on their rate of self-reported intentional weight loss. Subjects were classified as rapid weight losers if they exceeded 4 lbs weight loss monthly, moderate weight losers if their weight loss was between 2 and 4 lbs monthly, and slow weight losers if their average weight loss was between 0 and 2 lbs monthly.
Data Analysis
One-way ANOVAs were employed to assess differences based on groups of participants who were losing, maintaining, or gaining weight, and the threshold for significance was set at P ≤ .05 for comparisons. T tests were used to compare Weight Gainers versus Weight Losers and Fast Weight Losers versus Slow Weight Losers. Composite scores of healthy behaviors risk factor behaviors by group were compared for differences, and the utility of a composite Lifestyle Score that combines healthy and unhealthy behaviors was assessed by ANOVA and t tests to examine how well it could discriminate between individuals losing, maintaining, or gaining weight. After data examination dosage recommendations were explored for individuals seeking to maintain or lose weight and warning signs were examined for avoiding weight gain patterns.
Results
Group Differences in Weight Management Behaviors
As described previously, the composite Lifestyle Score was calculated by subtracting the total of risk behavior from the total of healthy behaviors. A one-way ANOVA revealed significant differences between all groups with regard to Lifestyle Scores with weight losers scoring higher than weight maintainers or gainers (see Table 2). With one exception, group differences were also found between the total amounts of healthy and risk behaviors. The exception to this was that the composite healthy score was not significantly different between fast, moderate, and slow weight gainers. However, a low sample size likely explains this lack of significance.
Mean Comparisons Between Weight Trajectory Groups, One-Way Using ANOVA and t Tests a .
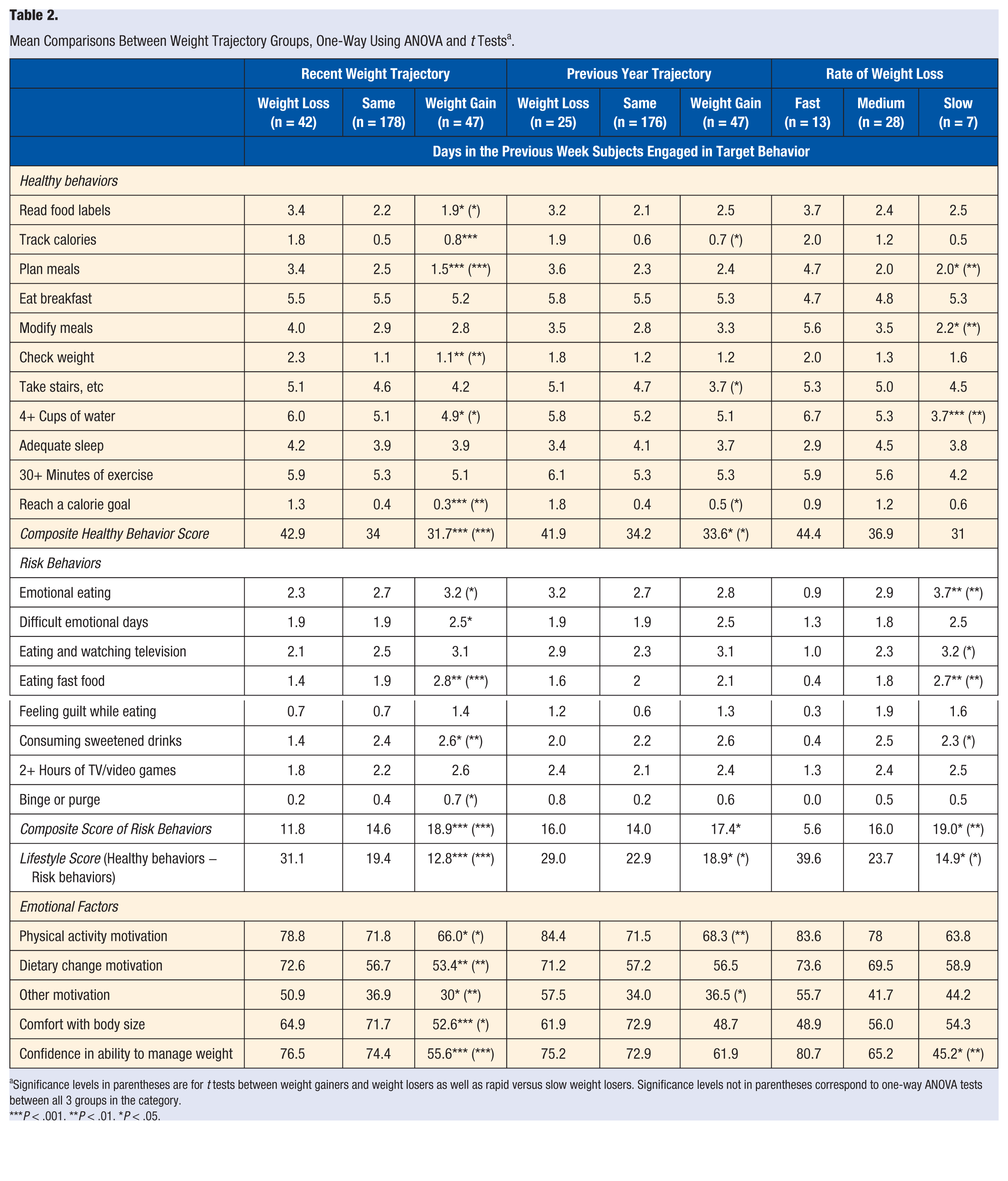
Significance levels in parentheses are for t tests between weight gainers and weight losers as well as rapid versus slow weight losers. Significance levels not in parentheses correspond to one-way ANOVA tests between all 3 groups in the category.
P < .001. **P < .01. *P < .05.
Groups were significantly different in their frequency of several health behaviors such as reading food labels, tracking calories, planning meals, checking weight, and water consumption. However, these differences were observed mostly for recent weight trajectories and not for weight gain in the previous year. Groups were also significantly different in their frequency of several risk behaviors such as eating while stressed or bored, difficult emotional days, and fast food and sweetened drink consumption. Again, these differences were found more often in recent weight trajectories and the participants’ rate of weight loss than when examining the previous year’s weight trajectory (see Table 2).
Group Differences in Emotional Factors
For recent weight trajectory groups, differences were observed for motivation to engage in physical activity, modify diet, and use other weight management behaviors (eg, calorie tracking) as well as comfort with one’s body and confidence in weight-management abilities. However, for groups based on the previous year’s weight trajectory, only subjects’ motivation to increase physical activity and willingness to use other weight management behaviors reached significance between weight gainers and weight losers. When comparing fast, moderate, and slow weight losers only confidence in one’s weight management skills reached significance—low sample size likely played a role in the lack of significance for the other comparisons (see Table 2).
Exploration of Dosage Recommendations
Given that the composite Lifestyle Scores demonstrated utility in discriminating between individuals losing, gaining, or maintaining weight, Lifestyle Score Groups were created to assess the relationship between membership in a particular score group and risk for weight gain and likelihood of weight loss (see Table 3). Such information could be useful to clinicians while discussing lifestyle patterns and risk for weight gain during counseling scenarios. Chi-square tests showed that Lifestyle Score Groups were significant predictors of participants’ recent weight trajectory group (P < .01) and the previous year’s weight trajectory (P < .05). However, the Lifestyle Score Group was not significantly associated with rapid, moderate, or slow weight loss although a small sample size may explain the lack of significance. A post hoc analysis of 3 subjects who have lost at least 50 lbs revealed their Lifestyle Scores were 52, 58, and 67, respectively. Approximately 44% of subjects with Lifestyle Scores below zero reported a weight gain of at least 10 lbs in the previous year. Given such information, Lifestyle Scores below 0 and above 50 warrant further investigation as possible guidelines to warn patients of future weight gain and guide them toward weight loss.
Percentage of Membership in Weight Trajectory Groups Based On Lifestyle Score Groups a .
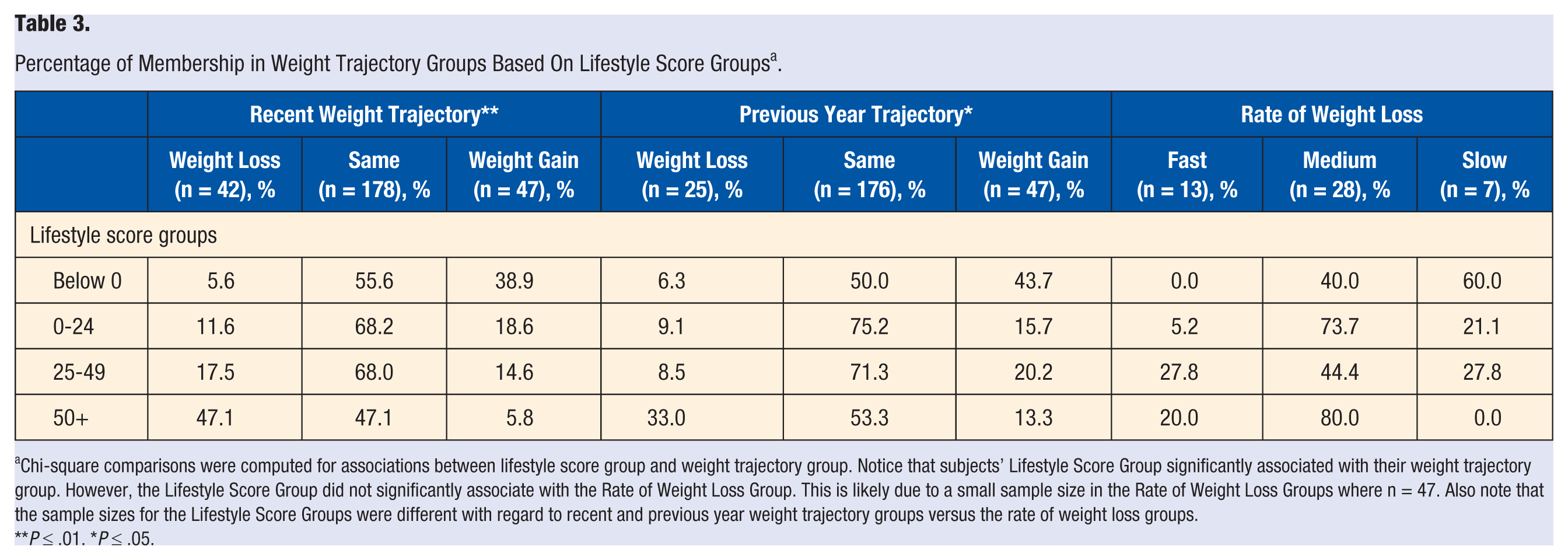
Chi-square comparisons were computed for associations between lifestyle score group and weight trajectory group. Notice that subjects’ Lifestyle Score Group significantly associated with their weight trajectory group. However, the Lifestyle Score Group did not significantly associate with the Rate of Weight Loss Group. This is likely due to a small sample size in the Rate of Weight Loss Groups where n = 47. Also note that the sample sizes for the Lifestyle Score Groups were different with regard to recent and previous year weight trajectory groups versus the rate of weight loss groups.
P ≤ .01. *P ≤ .05.
Discussion
The composite scores in the LQ-WM displayed significant differences between weight losers and weight gainers such as tracking calories, reaching calorie goals, taking advantage of daily exercise opportunities, checking their weight, fast food and sweetened drink consumption, and so on. Lifestyle Score Groups were also significantly associated with participants’ weight trajectories. Subjects with Lifestyle Scores below 0 were at an increased risk for reporting at least a 10-lb weight gain in the previous year as well as recent weight gain. Subjects with Lifestyle Scores above 50 were the most likely to report losing weight in the previous year. Such information may be helpful to warn patients of risky behavioral patterns for weight gain as well as to increase their awareness of behavioral patterns to promote weight loss.
A strength of the LQ-WM is that it can be completed in a short amount of time, perhaps while a patient is waiting to see a provider, and be quickly scored to serve as a conversation piece between the patient and provider. It also provides statistical information to allow the patient to examine how their lifestyle compares to others who are losing, maintaining, or gaining weight while considering their motivation for behavior change. A strength of the current study is that it took into account an array of behavioral patterns and emotional factors that the literature has identified are related to weight management. Since multiple behavior changes are characteristic of individuals who have successfully kept off large amounts of weight, 15 further studies examining the influence of multiple behaviors are desired. This study also attempted to create a composite scoring system of many behaviors in search of behavioral dosage recommendations for weight loss. To address potential recommendations, it should be noted that a significant association was found between higher composite Lifestyle Scores and weight loss although individual differences should be taken into account. For example, only one participant out of 17 with a Lifestyle Score above 50 was found to be in the recent weight gainers category. Consequently, it may often be wise to suggest to a patient that a score above 50 is optimal for their weight loss goals, although it is not a guarantee. Since a main intention of the LQ-WM is to serve as a conversation piece between the health care provider and the patient, the statistical information is simply meant to provide context with which to discuss the patient’s likelihood of success in their current weight management approach. Conversely, it is not at all impossible for patients to discover effective weight management strategies that yield low Lifestyle Scores—although it would be less likely than with a higher score. Additionally, the data showed that individuals can be successful at weight loss while emphasizing different weight loss behaviors that highlight the need to consider individual differences in weight loss counseling. It also supports the notion that there is not one single “right way” to lose weight.
This study also has several limitations that should be addressed. Due to limitations in subjects’ ability to accurately self-report weight management behaviors, some inaccuracy is likely. However, to reduce historical inaccuracies weight management groups were assigned by using a threshold of having gained or lost at least 10 lbs in the last year, which is a noticeable amount of weight for many people. Furthermore, nearly half (49%) of the participants indicated they checked their weight within the last week, which suggests they may be reliable reporters. Nonetheless, future studies could build on this research by employing more objective measurements of weight history and weight management behaviors. Additionally, Lifestyle Scores were more strongly associated with recent weight patterns than 1-year weight patterns. These stronger associations between health behaviors and recent weight patterns may be partly explained because the questionnaire asks about behavioral patterns in the last week rather than the last year. Consequently, the instrument may be a better predictor of recent weight patterns rather than longer patterns. Therefore, when trying to assess a patient’s likely weight trajectory in the next year clinicians would be well advised to assess stable patterns and refer to Item 23, which reads, “To what extent was the past week a typical week for you regarding your health efforts?”
Second, this study utilized a sample of predominately Caucasian, middle-class, college students attending a university where the predominant religion is of Latter Day Saints (Mormons). Consequently, how well these results would generalize to other samples such as older age groups, bariatric surgery patients, different cultures, and so on, is in need of clarification through additional research on those populations. Third, this study employed a cross-sectional design that does not allow for causal inferences between the specific behaviors to weight loss. Future studies that employ longitudinal designs and require participants to complete the LQ-WM consistently for multiple data points are warranted. Utilizing designs that can infer causal relationships between behaviors and weight loss could also help in adding appropriate weights to individual items—this study did not employ differential weighting on items for that reason. Finally, studies that examine patient and provider attitudes regarding the questionnaire are warranted as well as studies that assess the impact of utilizing the questionnaire on successful weight management outcomes.
In conclusion, since the LQ-WM was associated with weight trajectory patterns cross-sectionally, it may be a helpful tool for weight management counseling to highlight behavioral and emotional patterns associated with weight gain. Although this is the initial study, more research is underway that will increase the sample size and assess more diverse populations. Further research on the instrument using causal research designs with clinical populations would clarify the usefulness of the LQ-WM in clinical practice.