
Abstract
Nursing personnel, particularly caregivers who frequently perform manual patient transfer tasks, are at risk for work-related musculoskeletal disorders (WMSDs). The purpose of this study was to perform biomechanical evaluations of bed-to-wheelchair transfer using two low-cost assistive devices: walking belt and gait belt. Twenty-eight college students, serving as caregivers, transferred 14 students, serving as patients. “Caregiver” spinal loading and strength requirements at major joints were measured using a 3D Static Strength Prediction Model. “Caregiver”-perceived stresses were assessed using the Borg CR-10 Scale. “Patient” safety and comfort ratings were determined using Likert-type scales. The findings indicated that transferring “patients” using walking belts with a pulling technique produced significantly lower biomechanical stress than using gait belts. “Patients” also felt more comfortable and safer during walking belt transfers. It is recommended that health care facilities should consider use of walking belts in place of gait belts to transfer partially weight-bearing patients.
Keywords
According to the U.S. Bureau of Labor Statistics, nursing personnel continue to experience a high incidence of work-related musculoskeletal disorders (WMSDs; Bureau of Labor Statistics, 2015; Long, Bogossian, & Johnston, 2013). In 2015, nursing assistants had the second highest incidence of WMSDs (181 per 10,000 workers), a rate about 6 times the national average for all occupations, and the fourth highest number of injuries and illnesses requiring days away from work (37,370), with 53% of lost days attributable to overexertion (Bureau of Labor Statistics, 2015).
Manual patient-handling tasks, such as lifting, transferring, and repositioning of patients, have been reported to be major risk factors for WMSDs among nursing personnel in all health care facilities (i.e., hospitals, long-term care facilities, and clients’ homes (Garg & Kapellusch, 2012; Kim, Dropkin, Spaeth, Smith, & Moline, 2012; Nelson, Harwood, Tracey, & Dunn, 2008; Waters, Collins, Galinsky, & Caruso, 2006; Waters, Nelson, & Proctor, 2007). Epidemiological studies have shown exceptional incidence and prevalence of low back pain among nursing personnel (i.e., between 30% and 60%; Hignett, 1996; Lagerström, Hansson, & Hagberg, 1998; Lee, Lee, & Gershon, 2015; Videman, Ojajärvi, Riihimäki, & Troup, 2005). High perceived stress on low backs and shoulders has been reported by caregivers during manual lifting and transferring of patients (Garg, Owen, Beller, & Banaag, 1991a, 1991b; Garg, Owen, & Carlson, 1992; Owen & Garg, 1989; Owen, Keene, & Olson, 2002); these manual tasks are physically demanding and often involve unfavorable conditions (e.g., awkward posture, forceful exertion, and strenuous movements) that may result in high mechanical load on caregivers’ shoulders and low backs (Belbeck, Cudlip, & Dickerson, 2014; Garg et al., 1991a, 1991b; Nelson et al., 2008; Owen et al., 2002). Biomechanical studies have reported that the compressive force on low backs associated with manual patient-handling tasks may exceed the National Institute for Occupational Safety and Health (NIOSH) recommended safe limit (3,400 newton [N]), thus increasing the risk for low back pain among nursing personnel (Daynard et al., 2001; Garg & Owen, 1992; Garg et al., 1991a, 1991b, 1992; Jäger et al., 2013; Keir & MacDonell, 2004; Lloyd & Baptiste, 2006; Marras, Davis, Kirking, & Bertsche, 1999; Marras, Knapik, & Ferguson, 2009; McGill & Kavcic, 2005; Skotte & Fallentin, 2008). Nelson and Baptiste (2006) suggested that this high incidence and prevalence of low back pain among nursing staff might be a major reason for nursing personnel leaving the nursing profession or considering job transfer.
To reduce WMSDs among nursing personnel, various interventions have been implemented, including worker education, organizational policies, ergonomics programs, and use of various types of assistive equipment (e.g., sit-to-stand lift, full body sling lift, ceiling lift, lateral transfer devices) designed to attenuate the biomechanical stressors associated with manual patient-handling tasks (Cohen et al., 2010; de Ruiter & Liaschenko, 2011; Garg & Kapellusch, 2012; McCoskey, 2007; Rogers, Buckheit, & Ostendorf, 2013; Tang, Poklar, et al., 2017; Wardell, 2007). In 2009, the Occupational Safety and Health Administration (OSHA) published Guidelines for Nursing Homes (“Guidelines”) to address WMSDs in long-term care facilities (OSHA, 2009). These Guidelines suggest gait belt as one of the recommended devices for bed-to-wheelchair transfers of cooperative patients with partial weight-bearing capacity. Based on six participants, Garg et al. (1991a, 1991b) reported that pulling a patient using a walking belt produced less spinal compressive force than manually lifting patients using a gait belt. However, it is not clear (a) whether the walking belt produces less stress on shoulder joints or (b) how safe and comfortable patients feel when transferred using a walking belt as opposed to a gait belt.
The objectives of this pilot study were to (a) perform biomechanical evaluations of bed-to-wheelchair transfer using gait belt and walking belt, (b) quantify the perceived stresses to simulated caregivers, and (c) quantify perceived comfort and safety for simulated patients.
Method
This study was approved by the Institutional Review Board (IRB) at the University of Wisconsin–Milwaukee. The study protocol was explained to the college students prior to any data collection. All participants provided written, informed consent.
Sample
Twenty-eight college students (23 females and five males) served as caregivers. The requirements for inclusion in the study were (a) between 18 and 65 years of age, (b) no musculoskeletal problems at the time of enrollment, and (c) no chronic pain or restrictions by their physicians on lifting of loads or heavy physical work. Age, height, and weight of the sample were 26.7 ± 4.8 years (range = 22-34), 166.5 ± 8.9 cm (range = 154.9-188.0), and 64.5 ± 13.6 kg (range = 47.6-104.3), respectively. All “caregivers” were right-side dominant.
Fourteen female college students served as patients. The requirements were (a) weight ≤70 kg, (b) able to bear weight for 30 seconds or more, (c) no injuries or pain at the time of enrollment, and (d) able to follow instructions. Age, height, and weight for the “patients” were 26.4 ± 4.3 years (range = 22-39), 162.8 ± 7.6 cm (range = 154.9-177.8), and 58.2 ± 6.3 kg (range = 47.6-68.0), respectively. Both “patients” and “caregivers” were weighed using a mechanical platform scale (Sunbeam Products Inc., Boca Raton, FL, USA).
Study Design
This was a pilot study with healthy students serving as “caregivers” and “patients” in a lab-simulated setting. In this study, “patients” were manually transferred from a seated position on the edge of a hospital bed to a wheelchair by two caregivers using (a) a gait belt (Figure 1a) and (b) a walking belt (Figure 1b). The gait belt was 5-cm wide, had a belt-like loop closure to adjust the length, and had no handles. The walking belt was 13-cm wide and had two quick-release buckles on the outside. The walking belt was padded and had vertical handles on each side.
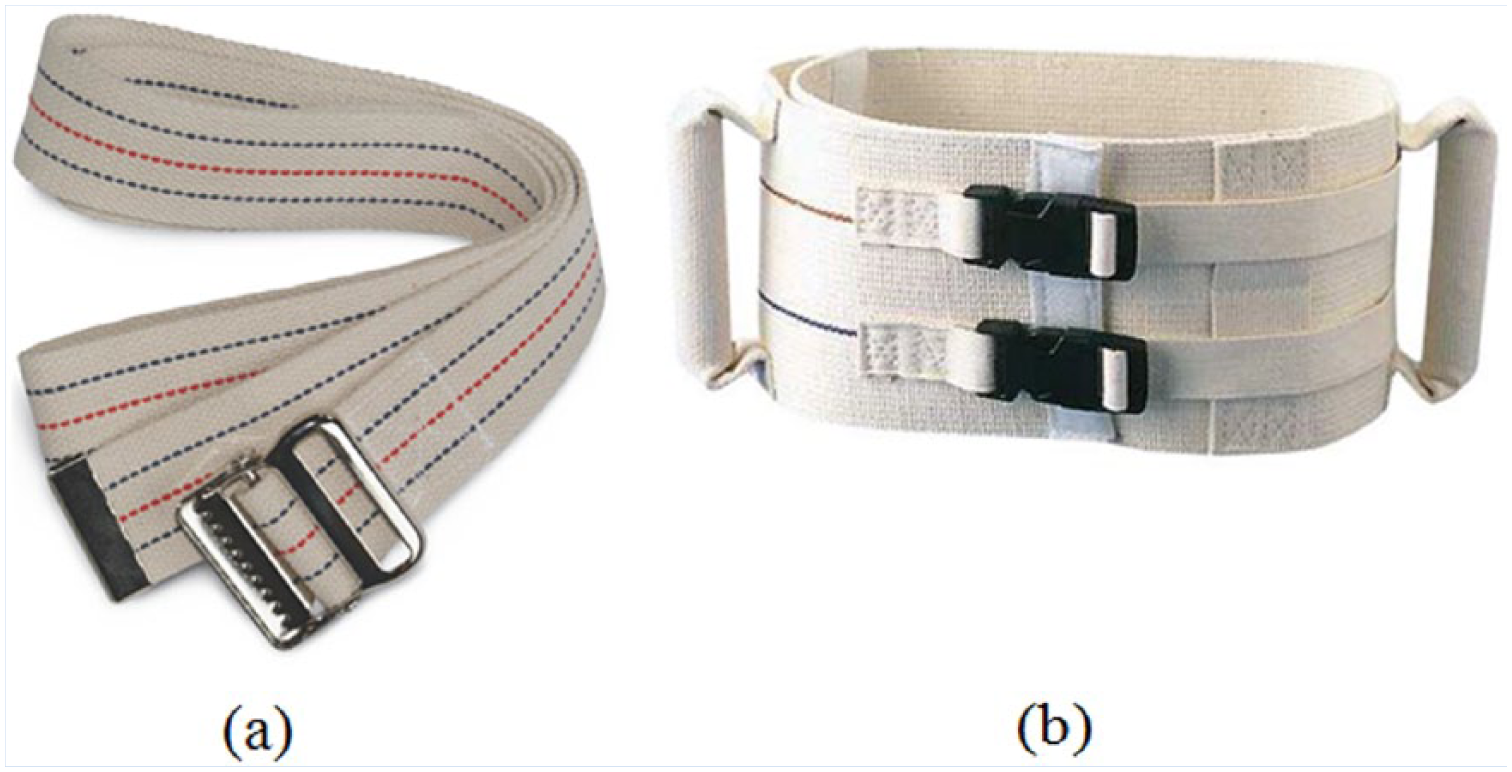
Examples of gait belt (a) and walking belt (b) used in this study.
A height adjustable hospital bed and standard wheelchair (seat height = 48 cm) were used for all transfers. For each transfer, the hospital bed’s height was adjusted so that “patients” could sit on the bed with their feet flat on the floor. A wheelchair was placed at a slight angle (approximately 20° from orthogonal to the patient) and close to the bed (approximately 0.3 m) to allow room for “caregivers” to maneuver the “patients.” The wheelchair was locked and the foot pedals were removed.
During walking belt transfer, an appropriate sized walking belt (small, medium, or large) was placed snugly around the “patient’s” waist. The “caregivers” were instructed to face the “patient” and stand with feet far apart (approximately shoulder width), right foot facing the “patient” and the left foot toward the wheelchair to avoid trunk twisting while transferring. “Caregivers” were also instructed to keep their backs as straight as possible and bend their knees. They were asked to grasp the walking belt handle with their right hands and place their left hands on the “patient’s” shoulders. First, the “caregivers,” in synchronization, gently rocked the “patient” to create momentum. Then on a slow count of three they pulled the “patient” toward themselves using that momentum.
When the “patient” stood up, the “caregivers” shifted their weight to their left feet, pivoted to avoid trunk twisting, and lowered the “patient” into the wheelchair. Instructions given to the “caregivers” clearly stated, “Pull with your arms and not your back. Do not lift.”
During gait belt transfer, a gait belt was applied to the “patient’s” waist and tightened to prevent the belt from sliding up or down on the “patient” but loose enough that two “caregivers” could grasp the belt firmly and comfortably from the side. The foot placement for gait belt transfers was similar to foot placement for walking belt transfers. Then, the “caregivers” lifted the “patients” to standing postures. Once the “patients” were standing, the “caregivers” pivoted and lowered the “patients” into wheelchairs.
In both cases, “patients” were instructed to act as passive models and not to assist during transfers. “Patients” were also instructed not to support their body weight when moving from a sitting to standing position. However, once “patients” were standing, they were asked to bear their body weight. Each manual transfer procedure was demonstrated before any data collection. Participants were asked to practice study procedures using gait and walking belts multiple times until they felt confident and comfortable.
Measurements
Before each manual transfer, “caregivers” were asked to briefly hold an initial posture while “patients” sat on the edge of their beds. During this phase, an analyst measured the “caregiver” body joint angles using a JAMAR® Goniometer Kit (Performance Health, LLC, Akron, OH, USA) and photographed the postures. The measured joint angles were later verified from the photographs (difference between measurements and photographs ≤10%). During walking belt transfer, the pulling force applied by “caregivers” on each side was measured by an S-Type force sensor (maximum force: 100 kg, Phidgets Inc., Alberta, Canada) and processed using a LabVIEW™ program (National Instruments Corporation, Austin, TX, USA). The force sensors were calibrated using OHAUS® ASTM weight sets (OHAUS Corporation, Parsippany, NJ, USA). Hand forces during gait belt transfer were assumed to be half of the “patient’s” body weight (i.e., it was assumed that a given “patient’s” body was evenly distributed between the two “caregivers”).
Manual transfer tasks were simulated using the University of Michigan 3D Static Strength Prediction Program™ (3DSSPP, version 6.0.6; University of Michigan, Ann Arbor, MI, USA). The input to the model included (a) “caregiver’s” gender, (b) “caregiver’s” height and weight, (c) “caregiver’s” body joint angles, (d) nature of the task (lifting for gait belt and pulling for walking belt), and (e) hand force (50% of body weight for gait belt and measured pulling force for walking belt). Biomechanical evaluations included (a) estimated spinal compressive force, (b) anterior/posterior (A/P) and lateral shear force at the L4/L5 and L5/S1 disks, and (c) strength requirements of the task, expressed as the percent of female or male population (as applicable) capable of performing the task. The strength requirements were determined for body joints of interest: elbow, shoulder, and trunk.
After each manual transfer, “patients” were asked to rate how safe and comfortable they felt on a 5-point Likert-type scale (1 = uncomfortable, 2 = somewhat uncomfortable, 3 = neither comfortable nor uncomfortable, 4 = somewhat comfortable, and 5 = comfortable). A similar scale was used for safety ratings. Furthermore, “patients” were asked whether they preferred being transferred using gait belts or walking belts. The “caregivers” were asked to rate physical stresses they felt at the shoulder and low back on a Borg-CR10 Scale (Borg, 1982). Similar to the “patients,” “caregivers” were asked their preference between gait belts and walking belts. All experiments were repeated; the average of the two measurements was calculated and reported here.
Statistical Analyses
Paired sample t tests were used to compare “patient” safety and comfort ratings when transferred using walking belts versus gait belts. “Caregiver”-perceived stress ratings on low back and shoulders were also compared between the two devices, as were the biomechanical demands associated with walking belt transfers versus gait belt transfers. Statistical analyses were performed using SPSS Statistics (version 20, IBM Corp., Armonk, NY, USA). An alpha level of .05 was used for all statistical tests.
Results
Preliminary analyses demonstrated no statistically significant difference in hand forces of the “caregivers” placed on the right and left side of “patients” when using walking belts (p > .05). Similarly, no significant differences were found between the right and left “caregiver” body joint angles (p > .05). Therefore, right and left “caregiver” data were aggregated into one group.
Manual transfer task measurements, biomechanical evaluations, population strength requirements, “patient” safety and comfort ratings, and “caregiver”-perceived stress ratings are summarized in Tables 1 to 4.
Trunk Angles and Hand Forces Associated With Gait Belt and Walking Belt Transfers (M ± SD [Range])
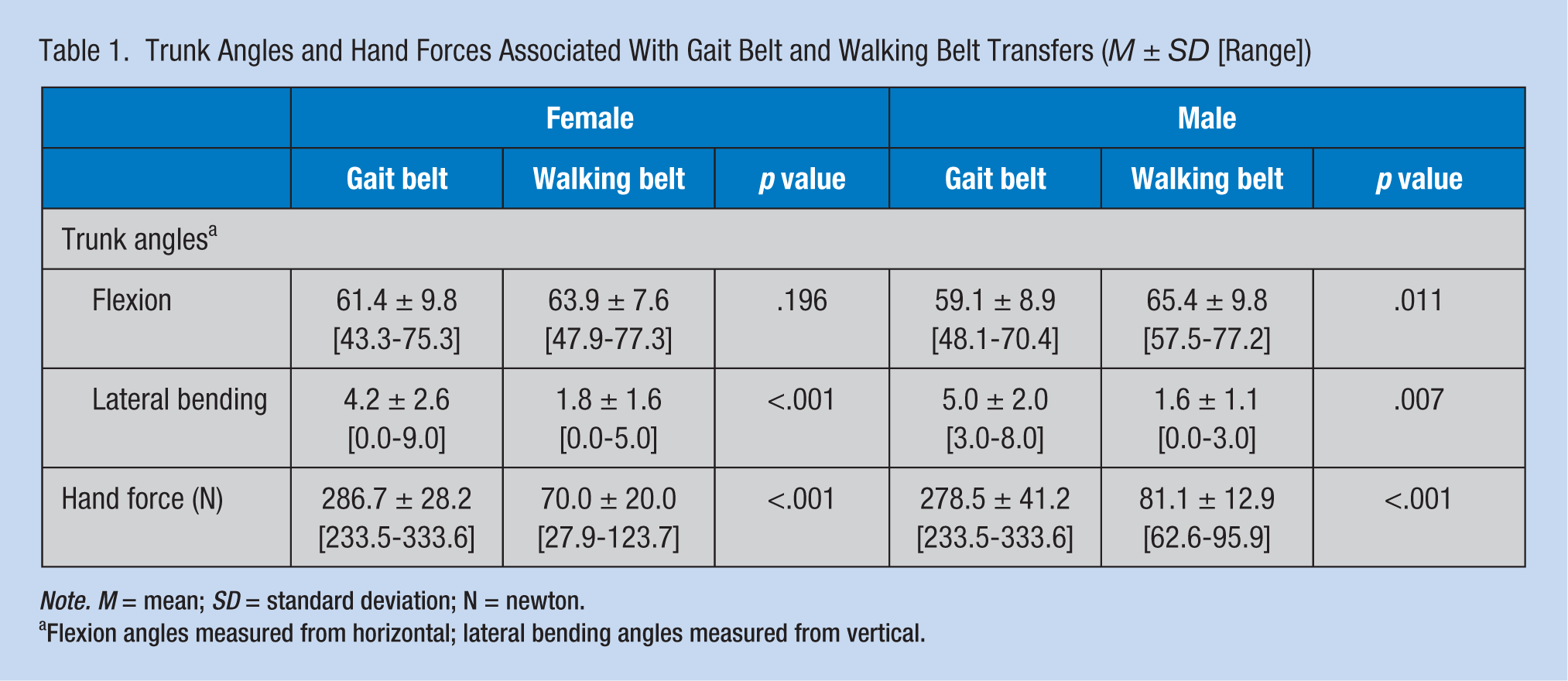
Note. M = mean; SD = standard deviation; N = newton.
Flexion angles measured from horizontal; lateral bending angles measured from vertical.
Summary of Biomechanical Evaluation of Gait Belt and Walking Belt Transfers (M ± SD [Range])
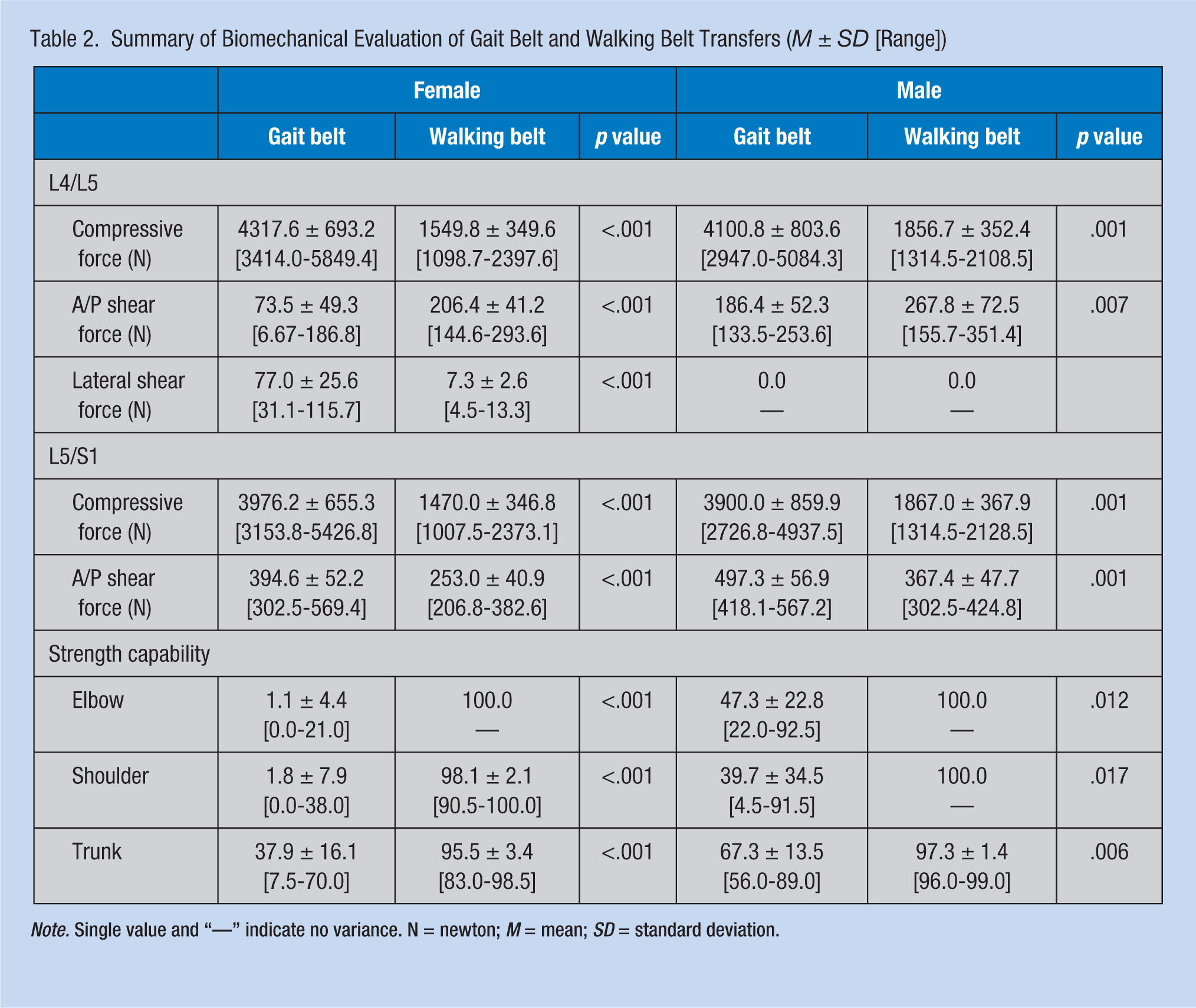
Note. Single value and “—” indicate no variance. N = newton; M = mean; SD = standard deviation.
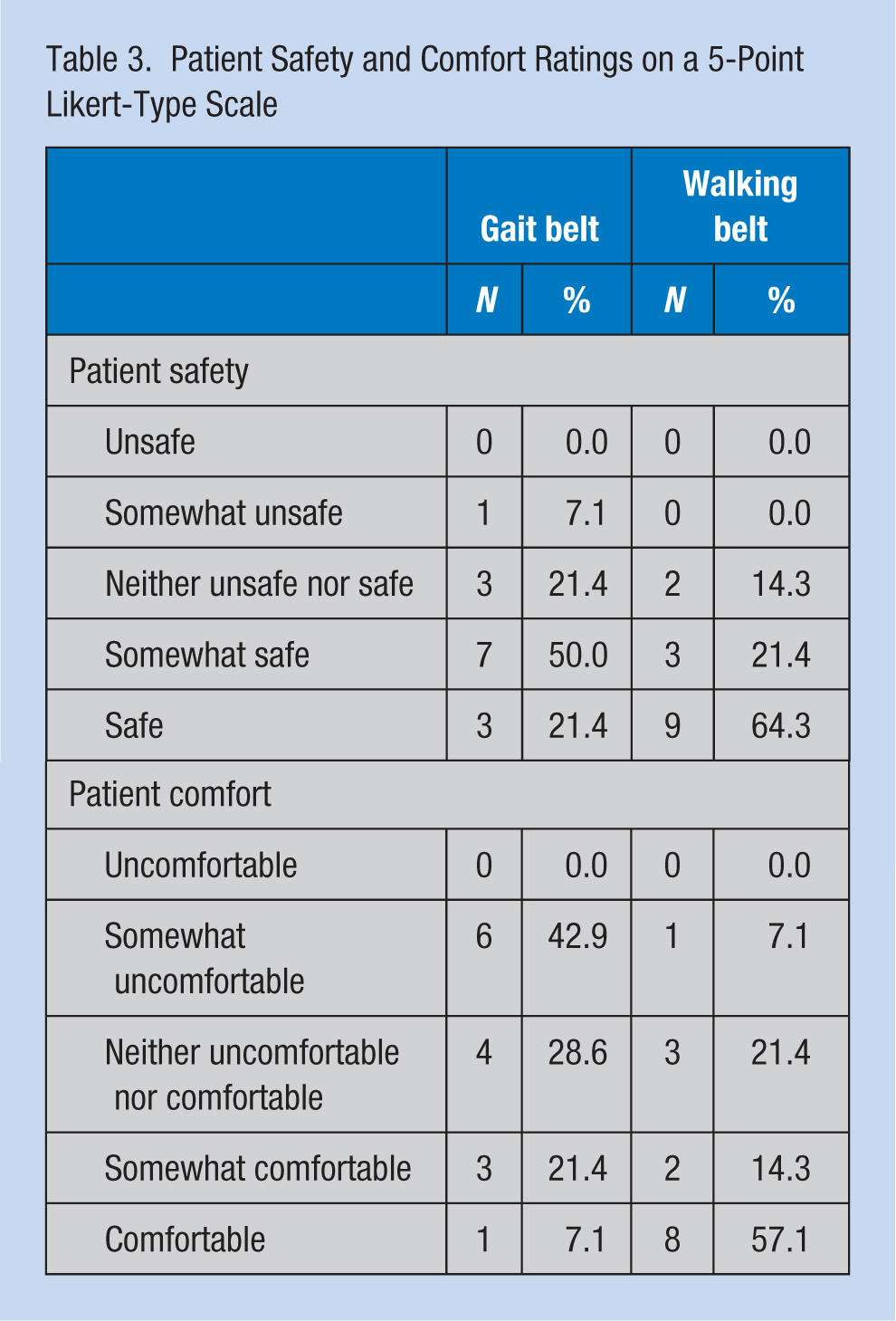
Patient Safety and Comfort Ratings on a 5-Point Likert-Type Scale
Caregiver Perceived Stress Ratings on Borg-CR10 Scale
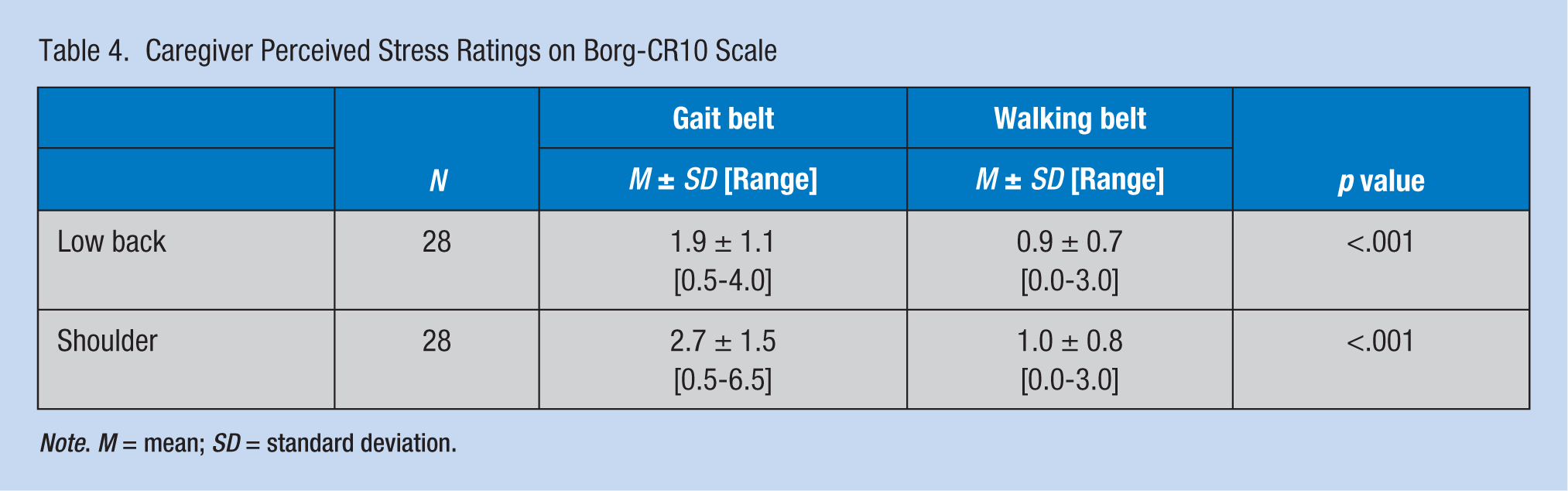
Note. M = mean; SD = standard deviation.
Body Joint Angles and Force Measurements
With respect to body segment angles (Table 1), the “caregivers” assumed almost identical body postures to raise “patients” from the bed (i.e., about 60° of trunk flexion (measured from horizontal plane), less than 10° of trunk lateral bending, and practically no axial rotation) regardless of whether gait belts or walking belts were used for the manual transfer. As expected, use of gait belts required significantly more hand force than walking belts (p < .001). The mean force required to pull “patients” using walking belts was about 25% of the mean force required to lift “patients” using gait belts for female “caregivers” (70 N vs. 287 N) and about 30% for male “caregivers” (81 N vs. 279 N; Table 1).
Biomechanical Evaluations
Walking belt transfers produced significantly less spinal compressive force than gait belt transfers (p < .001; Table 2). This finding was true for both L4/L5 and L5/S1 disks (Table 2). Compared with gait belt transfer, pulling “patients” with walking belts also resulted in a significantly lower anterior/posterior (A/P) shear force at the L5/S1 disk (p < .001; Table 2) but a higher A/P shear force at the L4/L5 disk (p < .01; Table 2). Lateral shear forces were negligible for both walking belt and gait belt transfers (Table 2). Regarding strength requirements, compared with the walking belt transfer, the gait belt transfer produced substantially greater stresses at all three body joints (p < .05; Table 2). Upper limbs (elbow and shoulder) were stressed the most by gait belts (Table 2). Biomechanical analyses showed that less than 2% of female “caregivers” and less than 40% of male “caregivers” had the required strength in upper extremity joints (elbow and shoulder) to safely lift and transfer “patients” using gait belts. However, about 95% of female “caregivers” and practically all male “caregivers” had sufficient strength to safely pull “patients” using walking belts.
Patient Safety and Comfort Ratings
Overall, 7% of “patients” rated gait belt transfers as either somewhat unsafe or unsafe, and about 70% of “patients” reported gait belt transfers were either somewhat safe or safe. In comparison, none of the “patients” rated walking belt transfers as either somewhat unsafe or unsafe, and over 85% of “patients” thought walking belt transfers were either somewhat safe or safe. With respect to comfort, over 40% of “patients” rated gait belt transfers as either somewhat uncomfortable or uncomfortable and less than 30% of “patients” thought gait belt transfers were either somewhat comfortable or comfortable. In comparison, 7% of “patients” rated walking belt transfers as either somewhat uncomfortable or uncomfortable and over 70% of “patients” reported walking belt transfers were either somewhat comfortable or comfortable.
Caregiver Perceived Stress Ratings
Compared with walking belts, gait belt transfers were perceived to be more stressful by “caregivers” (p < .001; Table 4). For gait belt transfers, perceived stresses on the shoulder were reported to be higher than perceived stresses on the low back with a mean rating of 2.7 and 1.9, respectively. About 40% of “caregivers” rated gait belt transfers either as “somewhat hard” or “hard” on shoulder joints. However, perceived stresses for walking belt transfers were very low with mean ratings of 1.0 and 0.9, respectively. In addition, none of the “caregivers” rated stresses on either body part more than “moderate.”
Patient and Caregiver Preference
The vast majority of “caregivers” and “patients” preferred walking belt transfers over gait belt transfers (86% each). The most frequently cited reasons for “caregivers” choosing walking belt transfers over gait belt transfers were (a) required less physical effort and (b) easier to perform transfers. The main complaint about walking belt transfers was that even the smallest size was too large for underweight “patients” and the walking belt is relatively difficulty to adjust.
Discussion
Physical Stresses to Caregivers
This lab-simulated study showed that the compressive force on low back is significantly lower when transferring a partially weight-bearing “patient” using a walking belt and a pulling technique compared with lifting a “patient” using a gait belt. NIOSH has established a safe compression load limit of 3,400 N for compressive force (NIOSH, 1981; Waters, Putz-Anderson, Garg, & Fine, 1993). In this study, regarding walking belt transfers, the estimated compressive forces at the L4/L5 (Female: 1,549 N; Male: 1,857 N) and L5/S1 (Female: 1,470 N; Male: 1,867 N) disks were well below the NIOSH-recommended safe limit. However, for the same “patients,” gait belt transfers produced mean compressive forces of 4,318 N for female “caregivers” and 4,101 N for male “caregivers” at the L4/L5 disk and 3,976 N for females and 3,900 N for males at the L5/S1 disk, respectively, exceeding the NIOSH-recommended safe limit. Based on compressive force considerations for transferring partially weight-bearing patients, study findings suggest that walking belt transfers using a pulling technique is safer than lifting patients using gait belts. The finding that gait belt transfers exceed the NIOSH-recommended safe limit for compressive force is consistent with prior reports (Garg et al., 1991a, 1991b; Marras et al., 1999). In addition, some studies have reported associations between body anthropometry and the geometry of lumbar spine and paraspinal muscles (Gungor et al., 2015a, 2015b; Tang, 2013; Tang et al., 2016; Tang et al., manuscript submitted for publication); however, the relationships between anthropometric characteristics and risk of low back pain remain unclear (Frymoyer, 1992; Manchikanti, 2000; Rubin, 2007; Sesek et al., 2014), and must be addressed in future investigations.
With respect to shear forces, previous studies have suggested that caregivers might experience high shear forces at the L5/S1 disk with manual transfers (i.e., gait belt and underarm lifts; Garg et al., 1991b; Marras et al., 1999). Suggested safe limits for shear forces range from 500 N to 1,000 N (Gallagher & Marras, 2012; McGill, 1997; Sonoda, 1962). In this study, lateral shear forces were negligible (i.e., ≤116 N) both for walking and gait belt transfers. The average A/P shear forces estimated from this current study (i.e., ≤395 N for female “caregivers” and ≤498 N for male “caregivers”; Table 2) were below the minimum safe limit of 500 N and thus no evidence was generated that “caregivers” are exposed to unsafe levels of shear forces for “patient” weights studied. However, the maximum A/P shear force at the L5/S1 disk was 569 N for female “caregivers” and 567 N for male “caregivers” performing gait belt transfers, modestly exceeding the 500 N safe limit recommended by Gallagher and Marras (2012). It should be noted that the static biomechanical model (3DSSPP) used in this study might underestimate shear forces on spinal structures (Marras et al., 1999). Last, it is suspected that shear forces might exceed 500 N when transferring heavier patients with either gait belts or walking belts, which must be investigated in the future.
Regarding the strength requirements of nursing tasks, this study clearly showed that practically all female “caregivers” (>95%) have sufficient strength to safely transfer a partially weight-bearing “patient” using walking belts and a pulling technique; however, less than 2% of female “caregivers” have sufficient strength to safely lift and transfer “patients.” Thus, from a strength perspective, this study suggests that walking belts and a pulling technique are much safer than gait belts for transferring partially weight-bearing patients.
Caregiver Perceived Stresses
Interestingly, “caregivers” perceived fairly low stresses for both walking belt and gait belt transfer techniques. Perceived stresses for gait belt transfers in this study were lower than perceptions reported in prior studies (Garg & Owen, 1992; Garg et al., 1991b). This inconsistency may due to lighter “patients” being transferred in this study compared with the aforementioned work. Nevertheless, over 40% of “caregivers” found gait belt transfers as either “somewhat hard” or “hard” on their shoulder joints; most “caregivers” (93%) found walking belt transfers to be “very light” or “light.”
Patient Safety, Comfort, and Preference
In this lab-simulated study, “patients” felt safer and more comfortable when transferred using walking belts as compared with gait belts, consistent with the findings of Garg et al. (1991b). Perhaps the wider design of walking belts eases their discomfort at the waist. Because gait belts have no handles, caregivers must grasp belts themselves, in some cases, causing bruising or skin irritation to patients (Garg & Kapellusch, 2012; Owen, Garg, & Jensen, 1992). Although a majority of “patients” in this study preferred the walking belt technique, a few preferred the gait belt technique. The primary complaint about walking belts was poor fit. Because walking belts do not need to be tightly fastened to patients’ waists, it is possible that the relatively tighter fit of gait belts provides a better sense of security to some patients.
Study Strengths and Limitations
Major strengths of this study include (a) both “caregiver” body joint angles and hand-pulling forces were measured for biomechanical model evaluations, (b) both “caregiver”-perceived stresses and “patient” safety and comfort were also quantified. A major limitation of this study is the use of college students who served as “patients,” which may not be representative of the actual patient population. For example, the current student sample did not have any physical or mental limitations, which is often not true for patients in a health care setting. Second, in this study, students serving as caregivers were relatively young and healthy. Therefore, the perceived stresses reported in this study may not reflect the opinions of actual caregivers with a history of performing manual patient-handling tasks. Third, “patient” weight was limited to 70 kg in this study. Thus, study findings may not be applicable to caregivers transferring patients who weigh more than 70 kg. Last, the current findings were based on a static biomechanical model, which may underestimate compressive and shear forces on spinal disks. Future studies of bed-to-wheelchair transfers should consider using dynamic biomechanical models based on measurements of actual caregivers and patients with diverse anthropometric characteristics in health care settings.
Implications for Nursing Practice
Consideration should be given to the finding that using walking belts to transfer partially weight-bearing patients from bed to wheelchair substantially reduces spinal loading on caregivers’ low backs. Furthermore, while practically all female caregivers have sufficient strength to transfer patients using a walking belt using a pulling technique, very few female caregivers have sufficient strength to safely lift and transfer partially weight-bearing patients. Thus, more caregivers should transfer patients using walking belts to decrease the risk of injury. From patients’ perspectives, being transferred with a walking belt offers a greater sense of safety and comfort compared with a gait belt transfer.
Conclusion
This lab-simulated study provides empirical data on the biomechanical stresses associated with two manual patient transfer techniques: gait belt and walking belt. Study data suggest that transferring partially weight-bearing patients using walking belts and the pulling technique produce less compressive force on caregivers’ low backs than transferring these patients using gait belts and a lifting technique. A larger percentage of caregivers have sufficient muscle strength to safely transfer partially weight-bearing patients with walking belts than with gait belts. The current findings suggest that the walking belt transfer technique is an effective ergonomic intervention to reduce work-related injuries resulting from manual patient transfer activities.
Applying Research to Practice
Health care facilities should consider using walking belts with a pulling technique to transfer partially weight-bearing patients to reduce shoulder and low back injuries to caregivers. Use of walking belts with a pulling technique may also improve patient comfort and safety.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Ruoliang Tang is a postdoctoral fellow in the Department of Occupational Science and Technology (OST), University of Wisconsin-Milwaukee (UWM). His research interests are in prevention of work-related musculoskeletal disorders and development of personalized ergonomic assessment tools.
Margaret Holland graduated from the UWM Master of Science in Occupational Therapy (MSOT) program. She has a bachelor’s degree in biopsychology. She is interested in occupational therapy practice among geriatric population in hospitals or skilled nursing facilities.
Michelle Milbauer graduated from the UWM MSOT program. She has a bachelor’s degree in conservation biology. She shifted interests from restoring the health of ecosystems to restoring function to individuals with disabilities.
Elise Olson graduated from the UWM MSOT program. She has a bachelor’s degree in human biology with an emphasis on exercise science. She is interested in occupational therapy practice in outpatient orthopaedic centers or acute care facilities.
Janelle Skora graduated from the UWM MSOT program. She has a bachelor’s degree in exercise and sports science. Her interests are in productive aging and improvement of life quality for individuals with dementia and their caregivers.
Jay M. Kapellusch is an associate professor and Chair of the OST Department, UWM. His primary research interests are in development of quantitative ergonomics job design algorithms that can be proactively used to design highly productive, safe jobs in manufacturing and service industries.
Arun Garg is the UWM Distinguished Professor in the OST Department. He is a pioneer and leader of health care ergonomics and safe patient handling.