
Abstract
A preshift stretching program was implemented to evaluate its effectiveness in preventing work-related musculoskeletal disorders (WMSD). Workers in a Midwestern factory were assessed for WMSDs before and after the new 8-min stretching program was implemented. Aggregate WMSD data were evaluated and sick days used from the start of the new program were compared with the same 60-day period the previous year. Potential cost savings were also assessed. The researchers found a significant decline in injury rates and time-off requests. Cost savings were noted for both the employer and employees. Additional studies with more workers, as well as longitudinal designs are recommended to verify the findings in this program evaluation study.
Keywords
According to the Bureau of Labor Statistics (BLS; 2016), work-related musculoskeletal disorders (WMSD) are common in the United States perhaps due to the practice of acclimating workers to jobs rather than modifying jobs to meet the needs of workers (Gartley & Prosser, 2011). The WMSD incidence rate in the nation was 29.8 cases per 10,000 full-time workers in 2015; the workers who sustained WMSDs required a median of 12 days to recover before returning to work. Moreover, 80% of all WMSDs involved private industry workers (Berry & Zaidman, 2017; U.S. Department of Labor, 2016). Furthermore, WMSDs lead to significant health care costs to businesses or organizations (Gartley & Prosser).
In factories, certain activities such as manual handling and continuous lifting are associated with WMSDs (Gartley & Prosser, 2011). It has been noted that prework stretching programs can be beneficial in decreasing WMSDs (Moreira-Silva, Santos, Abreu, & Mota, 2014; Muyor, López-Miñarro, & Casimiro, 2012). Evidence suggests that primary prevention of worksite injuries and promotion of worksite wellness and stretching can improve workers’ satisfaction and productivity as well as decrease health care costs to employers (Aghilinejad et al., 2014; Cheng & Chang, 2009; Gartley & Prosser, 2011; Muyor et al., 2012). A gap in the literature was found regarding the effectiveness of workplace stretching programs. In addition, it is unclear whether employers benefit from sponsoring stretching programs.
Literature Review
The literature review incorporated information on types of WMSDs (i.e., neck, upper back/shoulders, lower back, waist/upper torso, thighs, hamstrings, inner thighs, and calves) as well as differences in worksite stretching programs and duration of the programs. Several studies noted a relationship between stretching and prevention of WMSDs. Aghilinejad et al. (2014) conducted a randomized clinical trial with 503 factory workers and suggested a workshop for automobile factory workers about ergonomics, and stretching was more beneficial than a lecture or print documents. Another study documented fewer reports of WMSDs after 6, 12, and 52 weeks of a physical activity/stretching wellness program in a factory setting (Cheng, & Chang, 2009; Edries, Jelsma, & Maart, 2013; Muyor et al., 2012). In a systematic review, da Costa and Vieira (2008) found beneficial effects of stretching in preventing WMSDs. However, the reported finding was questioned due to the methodological quality of the study.
Moreira-Silva et al. (2014) compared a group of factory workers who participated in 10 to 15 minutes of physical exercise training, focused on stretching exercises and general strength, three times a week with a group of workers who did not participate in the training. After 6 months, factory workers who participated in the training had a significant decrease in WMSDs. Gartley and Prosser (2011) found that injury rates decreased significantly after the initiation of a 90-day preshift 6-minute stretching program implemented at tin and beverage factories.
WMSD can also be costly. According to a Minnesota workers’ compensation system report in 2015, the percentage of paid WMSD indemnity claims with claimant attorney involvement rose from 17 to 24 percent from 1997 to 2014 (Berry & Zaidman, 2017). The cost of WMSDs included time off from work, health care costs (e.g., clinic, hospital, and rehabilitation), and overtime costs to replace injured workers. Costs of worker stretching programs can vary based on the time required to participate. Gartley and Prosser (2011) found that a 6-minute stretching program, “demonstrated substantial savings despite employees using company time to stretch” (p. 252).
Current studies suggest that stretching programs at work may reduce WMSDs (Cheng, & Chang, 2009; Edries et al., 2013; Gartley & Prosser, 2011). Limitations from previous studies have noted the need for additional studies to assess similar stretching programs with various types of employees. The purpose of this program evaluation study was to assess the impact of a new workplace stretching program on the number of WMSDs reported, days off work due to injuries and potential cost savings.
Program Evaluation Study
A certified stretching specialist was consulted to develop a new stretching program based on the Mayo Clinic (2016) 10 Basic Stretching Protocol. The program consisted of 10 stretches targeting the neck, shoulders, upper and lower back, quadriceps, hamstrings, arms, and ankles. Mayo Clinic (2017) also provided an online slide show about the basics of stretching that was used as a resource. Each stretch was to be held for 10 to 15 seconds. All 10 specific stretching exercises were completed in a standing position without the use of equipment to maximize space and time and reduce cost. The exercises were repeated three to four times for a total of 8 minutes. One week prior to the commencement of the stretching program, employees received a printed pamphlet and wall-sized posters of the stretches, and an electronic version on the break-room screen monitors. During this week, the occupational health provider and occupational therapist certified in Physical Medicine and Rehabilitation (stretching specialist) provided education on stretching routines to safety managers, safety engineers, supervisors, and lead line workers.Their role was to teach workers how to complete stretching exercises and lead employees in completing the exercises, including ensuring proper body mechanics and postures during the program. Wall-sized posters of the stretches were also hung in the stretching areas. The workers were to complete the 8-minute stretching program before the start of every shift.
On program initiation day (August 1, 2016), informational displays including balloons and banners were hung and light snacks were provided to the workers in the break room. As the stretching program progressed, verbal positive reinforcement was provided to encourage continued dedication. On days 30 and 60 balloons and banners were hung again to create a sense of continuous health and safety awareness within the factory and to support the new stretching program. At the end of the 60th day of the program, fruits and snacks were provided to all workers to support continuing the new stretching program.
To determine the effects of the new preshift stretching program, the following questions were explored: Can an 8-minute preshift stretching exercise reduce WMSDs and days off work? Does a worksite stretching program result in cost savings?
Method
This program evaluation study was conducted at a food factory located in Minnesota. At the time of the intervention in August 2016, 146 line and production workers, 98 males and 48 females, worked for the company. The workers ranged in age from 18 to 64 years; their tenure at the factory ranged from 1 week to 44 years. The job description in the food factory line/production included the following activities: lifting, carrying, pushing, and pulling up to 50 pounds per task throughout an 8-hour shift. All uninjured workers (e.g., workers without active WMSD or physical restrictions) were required to participate in the new stretching program. Stretching took place in an open workstation area in the factory so that the assigned safety personnel could effectively lead the exercises and ensure use of proper techniques. Safety managers, safety engineers, supervisors, and lead line workers identified employees with active WMSD or physical restrictions and exempted them from the new program.
Study Design
The retrospective program evaluation study was conducted after initiation (August 1, 2016) of the new stretching program. The Workplace Health Model (Centers for Disease Control and Prevention [CDC], 2013) was used for this study, specifically evaluating this new program for “Improved Health Outcomes” (WMSD/days off work) and “Health Care Costs.” Data were collected on factory forms that documented WMSDs and time-off requests. The safety manager and Human Resources staff compiled aggregate data related to the number of WMSDs and days off work from factory workers’ records during the 60-day period from August to September 2015 and during the intervention period from August to September 2016.
Descriptive data were collected on minor problems or issues related to the implementation of the new program by the safety manager. For factory workers who were unable to complete some components of the stretching program due to body habitus or previously resolved injury, the stretching specialist customized the program to ensure the alternative activity was still 8 minutes in duration. In addition, safety managers, safety engineers, supervisors, and lead line workers identified workers who had incurred WMSD within the first 60 days of the program. An injured worker was not allowed to participate in the preshift stretching program to prevent reinjury; possible work restrictions were accommodated as necessary. The advance practice registered nurse (APRN) completed a spot check one to two times a week to assess workers’ participation in the new program as well as consistency in following the exercise routine from Week 1 through Week 8.
Approximately, 3 months before the program’s initiation, the management of the food factory was given information about the proposed new stretching program. Prior to the initiation of the new program and collection of data, study protocol was approved by a university institutional review board and factory management.
Data Analysis
Descriptive statistics were calculated to provide a summary of the demographic characteristics of factory workers. A paired-sample t test, percentages, and rates of requested days off per 100 workers were calculated for purposes of comparing the pre- and postintervention periods. The t-test analysis was performed using SPSS for Windows, and the significance level was set at p < .05. Cost-saving analysis was guided by a similar program evaluation study by Gartley and Prosser (2011).
Program Evaluation Results
For the 60-day period, August-September 2015, six of 158 workers (3.8%) WMSD injuries were reported before the stretching program was implemented, and during the first 60 days of the program in 2016, two of 146 workers (1.4%) reported WMSD injuries after the stretching program (Figure 1; p = .04). This resulted in a decreased rate of requested days off from 84.8 days per 100 workers to 62.3 days per 100 workers in the first 60 days of the program period (p = .01), respectively (Figure 2). Noted causes for time-off work included sick time, personal reasons, workers’ compensation injuries, and Family and Medical Leave Act (FMLA). No adverse outcomes were reported due to the program and all eligible workers participated in the program.
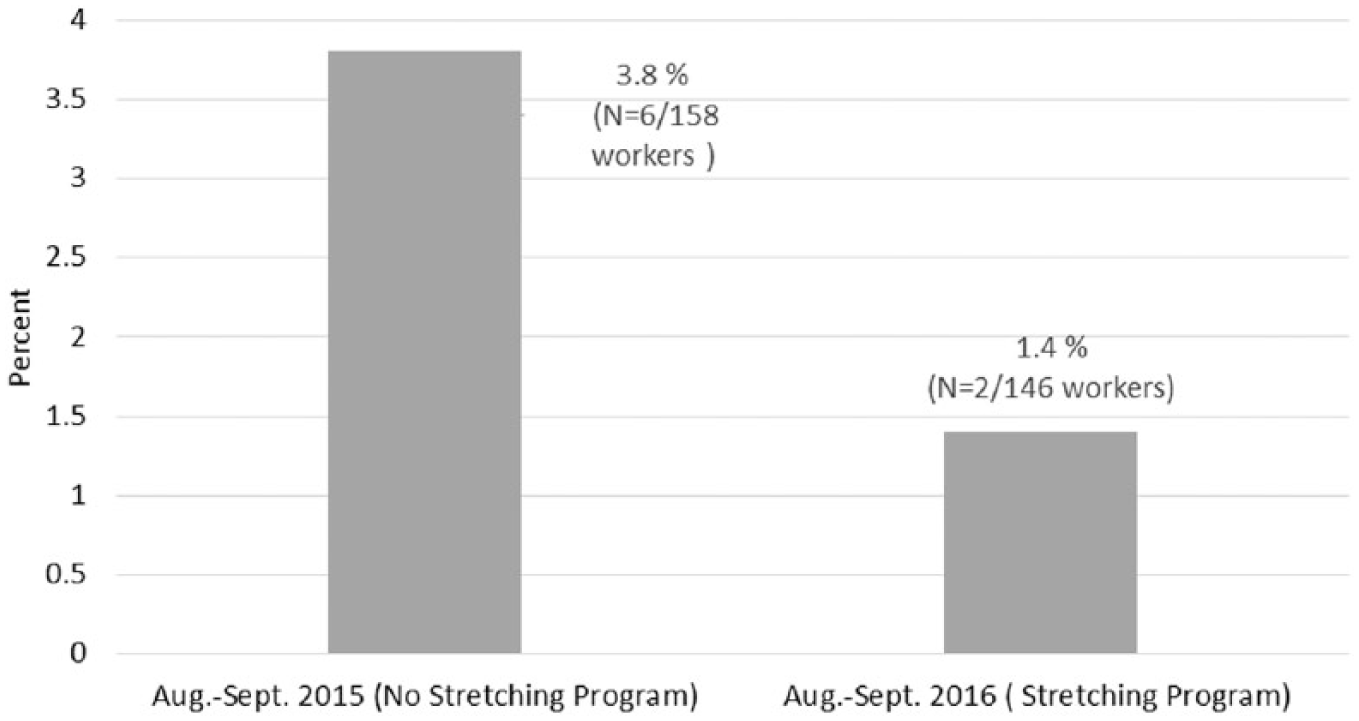
Percent of WMSD injury before and after stretching program.
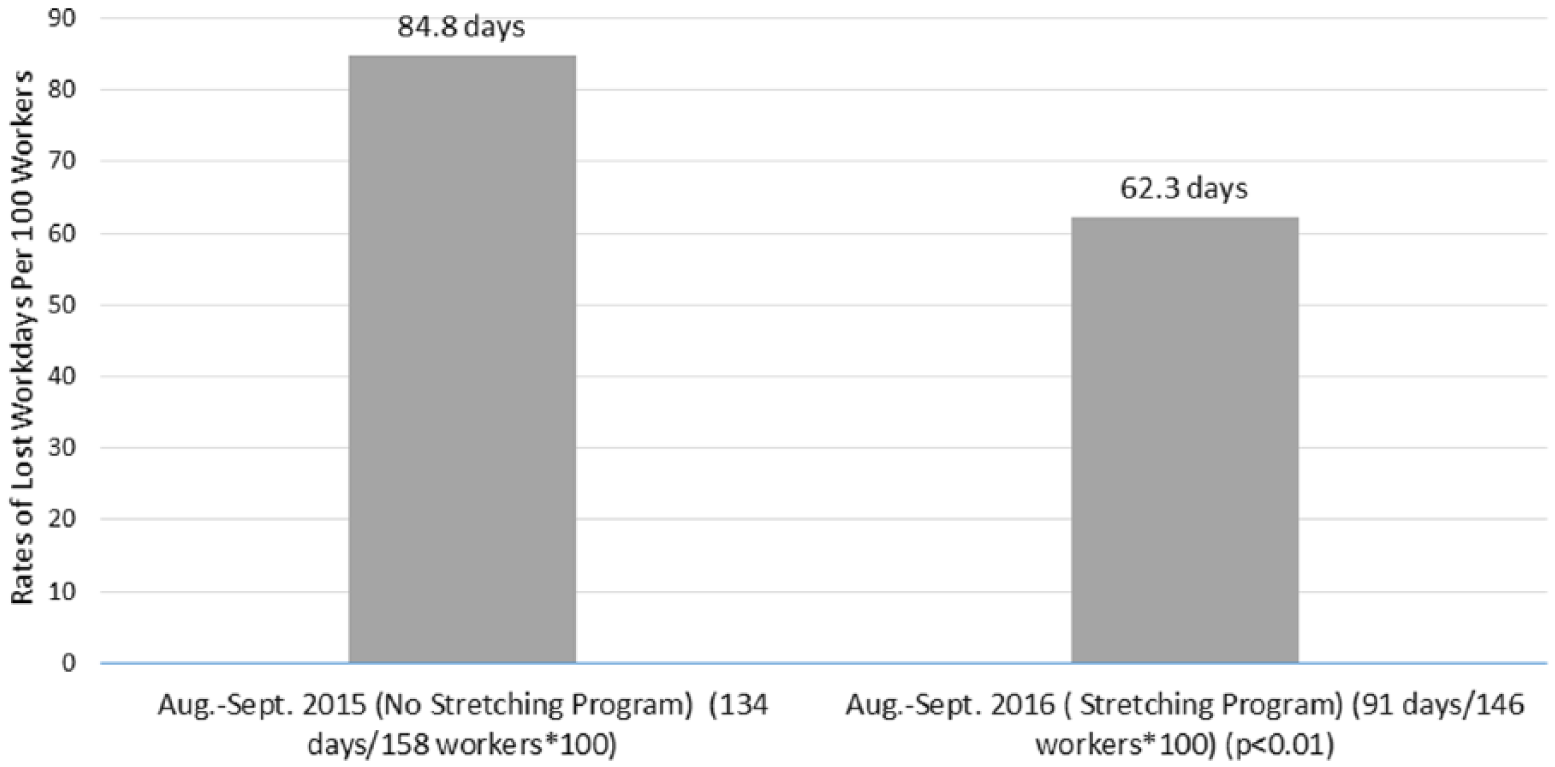
Percent of requested days off work before and after stretching program.
Minimal resources were needed to initiate the worksite stretching program. The highest cost was the workers’ time, 8 minutes, for preshift stretching which was paid for by the company (Table 1). The cost of US$5,800 per WMSD was based on average cost data provided by human resources and the workers’ compensation carrier from August to September 2015. These costs included nonsurgical treatment that required a minimum of two visits, sometimes 10 to 12 physical therapy sessions were required. Company data were used to calculate all potential cost savings of the stretching program.
Potential Cost Savings From an 8-Minute Prework Stretching Program
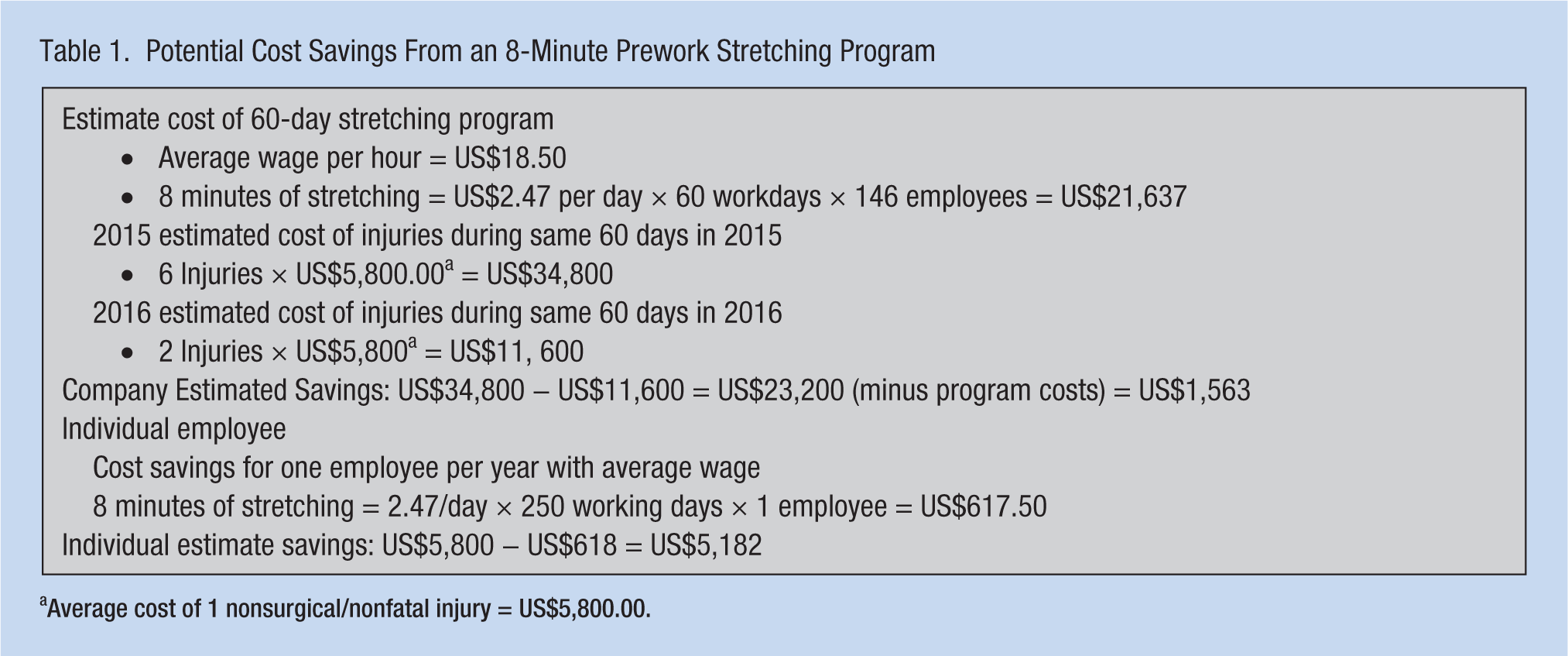
Average cost of 1 nonsurgical/nonfatal injury = US$5,800.00.
Discussion
This program evaluation study found that an 8-minute stretching program was associated with fewer WMSDs and days off work. The new stretching program demonstrated statistically significant results despite the small number of workers participating in the program. Moreover, similar studies have found similar positive results (Gartley & Prosser, 2011; Moreira-Silva et al., 2014; Muyor et al., 2012). Although attendance sheets compiled by the safety manager found fewer days off requests during the program, it was unclear whether the day off requests after the implementation of the new stretching program were directly related to work injuries because time-off requests included personal sick time, personal reasons, workers’ compensation injuries, and FMLA.
Potential company cost savings were small but are more significant for individual employees. Estimated costs were based on an average cost of a clinic visit for nonsurgical/nonfatal injury. Costs could rise significantly if a WMSD required surgery, long-term hospitalizations, and rehabilitation or resulted in death. Moreover, company costs did not include the cost of overtime or temporary workers to cover the shifts of employees injured at work nor potential litigation costs. Overall cost of the program was low, including the cost of workers’ absence from the production line.
Limitations
There were several limitations to this new program evaluation. Data were collected in a very short time frame, only 2 months the year before program implementation and 2 months after the start of the new program. Although Edries et al. (2013) found benefits of an exercise work program after only 6 weeks, the study would have been strengthened if data had been collected for a longer period and if additional information had been collected on the type and severity of WMSDs. It is possible that the implementation of the preshift stretching induced the workers to maintain individual accountability and responsibility for work injury prevention, possibly reducing injury rates and days off requests. A variety of promotional items (i.e., flyers, pamphlets, wall posters, and periodic refreshments) that increased safety awareness could have also influenced program outcomes. In addition, weather, job/task allocation, and equipment condition may also have played a role in injury incidence from year to year. The Hawthorne effect may also have contributed to strong participation from all workers. Although financial savings was a reasonable outcome, additional studies with longer duration could result in more accurate findings. As a retrospective study that includes only generalized expenses, costs savings can only be estimated. Moreover, the frequency and/or acuity of an injury may be significantly below or above actual costs to the company and the employees.
Implications
Factory work can require manual labor, which predisposes employees to WMSDs. Fewer WMSDs were reported during the 60-day program period compared with the same period in the previous year. Findings suggest that occupational health clinicians (e.g., APRN) can reduce WMSDs among food factory workers and potentially among workers in other similar work settings.
The cost-saving analysis completed for the organization illustrated potential savings for workers participating in the stretching program on company time. Thus, other companies could reduce WMSDs costs by implementing a similar preshift stretching program. After completing the initial 60-day stretching program, the food factory continued the stretching program and management is considering expansion of the program to their other facility located in California.
Conclusion
Factory environments are inherently dangerous. An effective and affordable stretching program is a feasible clinical intervention in factory work settings. This program demonstrated that workers can remain committed to a customized set of interventions that produce significant, evidence-based health promotion outcomes. These findings are highly beneficial to prominent stakeholders including employees, employers, and occupational health clinicians. Additional studies with larger samples/workers and longitudinal designs are recommended to confirm the findings of this program evaluation study.
Applying Research to Practice
Factory environments are inherently dangerous. An effective and affordable stretching program can be a feasible clinical intervention in a factory work setting. The preshift stretching program focused on reducing work-related musculoskeletal disorders which not only benefits employees by decreasing injury rates but also benefits employers with fewer requests for time off and potential cost savings.
Footnotes
Acknowledgements
The authors thank Dr. Bossou Kodjo, the lead physician for I-90 Mayo Clinic Health Systems (MCHS), Ms. Patricia Peterson, occupational therapist and stretching specialist from the Physical Medicine Rehabilitation Department of MCHS, and Mr. Dan Brant, the health and safety manager of the food factory.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Omotolu Olaitan Aje is the Occupational Health and Family Nurse Practitioner for Mayo Clinic Health Systems, a healthcare facility where Ventura Food Factory’s current/prospective employees receive health care services.
Betty Smith-Campbell is a professor at Wichita State University and teaches Population and Social Determinants of Health in the School of Nursing graduate program.
Carol Bett is an instructor at Wichita State University and teaches evidence based practice courses in the School of Nursing undergraduate and graduate programs.