
Abstract
This cross-sectional study investigated the prevalence and risk factors of work-related musculoskeletal disorders among intensive care nurses in the Hunan Province of China. Nurses working in mixed intensive care units of 20 tertiary hospitals in this province participated in an online survey regarding work-related musculoskeletal injuries. The seven-part questionnaire included basic demographics; job and workplace characteristics; risk perception; physical, psychosocial, and workplace organizational factors; and musculoskeletal symptoms. The response rate was 70.7% (702 of 993 nurses). Approximately 97% of the respondents reported experiencing at least one work-related musculoskeletal disorder within the previous year. Low back pain was the most commonly reported musculoskeletal disorder (80.1%), followed by neck (78.6%) and shoulder pain (70.4%). The multivariate logistic regression analysis indicated that work-related musculoskeletal disorders were significantly associated with female gender (odds ratio [OR] = 0.115), unmarried status (OR = 0.136), a greater perception of risk (OR = 2.352), and lack of a safe work environment (OR = 1.056). These findings underscore the need for nurses and managers to reinforce risk awareness, improve physical and psychosocial working conditions, and promote a safer work environment.
Keywords
Introduction
Work-related injuries are defined as bodily injuries that occur at the job site (Gossman & Knoblauch, 2017). Factors contributing to work-related injuries may be poor ergonomics, misuse of equipment, or inadequate safety training (S. J. Lee, Lee, & Gershon, 2015; Tinubu, Mbada, Oyeyemi, & Fabunmi, 2010). Work-related musculoskeletal disorders (WRMDs) are common (Bai, Wang, & Yue, 2009) and can involve muscles, nerves, tendons, joints, cartilage, and intervertebral disks (Freimann, Coggon, Merisalu, Animagi, & Paasuke, 2013; Wang, Yan, Huang, & Dai, 2017). Work-related musculoskeletal disorders are seldom life threatening but do cause loss of labor time, lower the quality of life, increase financial burden, and are a major public health problem. For example, in the state of Washington from 1999 to 2013, WRMDs accounted for more than 40% of all workers’ compensation claims (Marcum & Adams, 2017). In Great Britain in 2016-2017, ~8.9 million working days were lost due to WRMDs.
For nurses, musculoskeletal disorders are a major occupational health problem. Worldwide, the annual prevalence of WRMDs among nurses is 40% to 85%, as reported by studies from Brazil and Italy (Carugno et al., 2012), Estonia (Freimann et al., 2013), Uganda (Munabi, Buwembo, Kitara, Ochieng, & Mwaka, 2014), Nigeria (Tinubu et al., 2010), and California (S. J. Lee et al., 2015). In China, the prevalence of WRMDs among nurses is 56% to 92% (Cheng, Wang, Wu, Shen, & Jing, 2017; Liu et al., 2015; Wang et al., 2017; Zhang, Li, & Gui, 2016), most commonly affecting as pain of the lower back, neck, and shoulder.
In China, the patients in intensive care units (ICUs) are often immobile with severe physical weakness and little ability to care for themselves (Gao & Zhang, 2008; Sun, 2012). Nurses in the ICU have a heavy burden of care. Compared with other wards, the stressful environment of the ICU demands greater physical strength and mental stability of the medical staff (Kong, Liu, & Chen, 2016; Liu, Huang, & Chen, 2016).
Work-related musculoskeletal disorders are very common among ICU nurses in China (Sezgin & Esin, 2015), with an estimated prevalence of 95% to 98% (Zhang et al., 2016). Work-related musculoskeletal disorders can lead to absence at work or seeking other employment (Attar, 2014). Chen and Li (2017) reported that 28.9% of ICU nurses in China requested time off or a transfer to another unit due to low back pain. Therefore, the prevention of WRMDs is important to the well-being of ICU nurses and the stability of ICU teams.
The nursing occupation is prone to WRMDs due to awkward body positions held for extended periods, repetitive movements (Ribeiro, Serranheira, & Loureiro, 2017), and unsafe working conditions (Hoe, Kelsall, Urquhart, & Sim, 2012; S. J. Lee, Faucett, Gillen, Krause, & Landry, 2013). Differences in the estimated prevalence of WRMDs across countries may reflect differences in working environments, facilities, and the nature of the work, resulting in inconsistent reporting of risk factors (Attar, 2014; Mo & Zhang, 2011). For example, in Pakistan, risk factors of WRMDs in nurses include working in the same positions for long periods, attending to an excessive number of patients per day; however, lifting or transferring patients is often performed by male nursing assistants (Rathore, Attique, & Asmaa, 2017). In China, staff shortages and the large number of patients mean that the most common risk factors are heavy workload and repetitive movements (Wu & Cao, 2015; Zhang et al., 2016).
Risk factors of WRMDs also vary by hospital department (Du et al., 2016). In the ICUs of China, nurses work 8-hour shifts and may have only one or two short breaks, depending on the workload. Daily, ICU nurses conduct multiple procedures such as airway management and pressure sore prevention. Identifying the risk factors pertinent to ICU nurses may aid in the development of tailored prevention strategies.
The present study was based on a conceptual framework proposed by S. J. Lee et al. (2013) that included perception of risk and work behavior as indirect factors related to WRMDs (Figure 1). Of note, both perception of risk and work behavior are reciprocal with the occurrence of WRMDs; the internal biomechanical or psychological responses of nurses can influence the occurrence of musculoskeletal injuries, symptoms, or illnesses. Direct factors associated with WRMDs include the individual, job, and workplace organization.
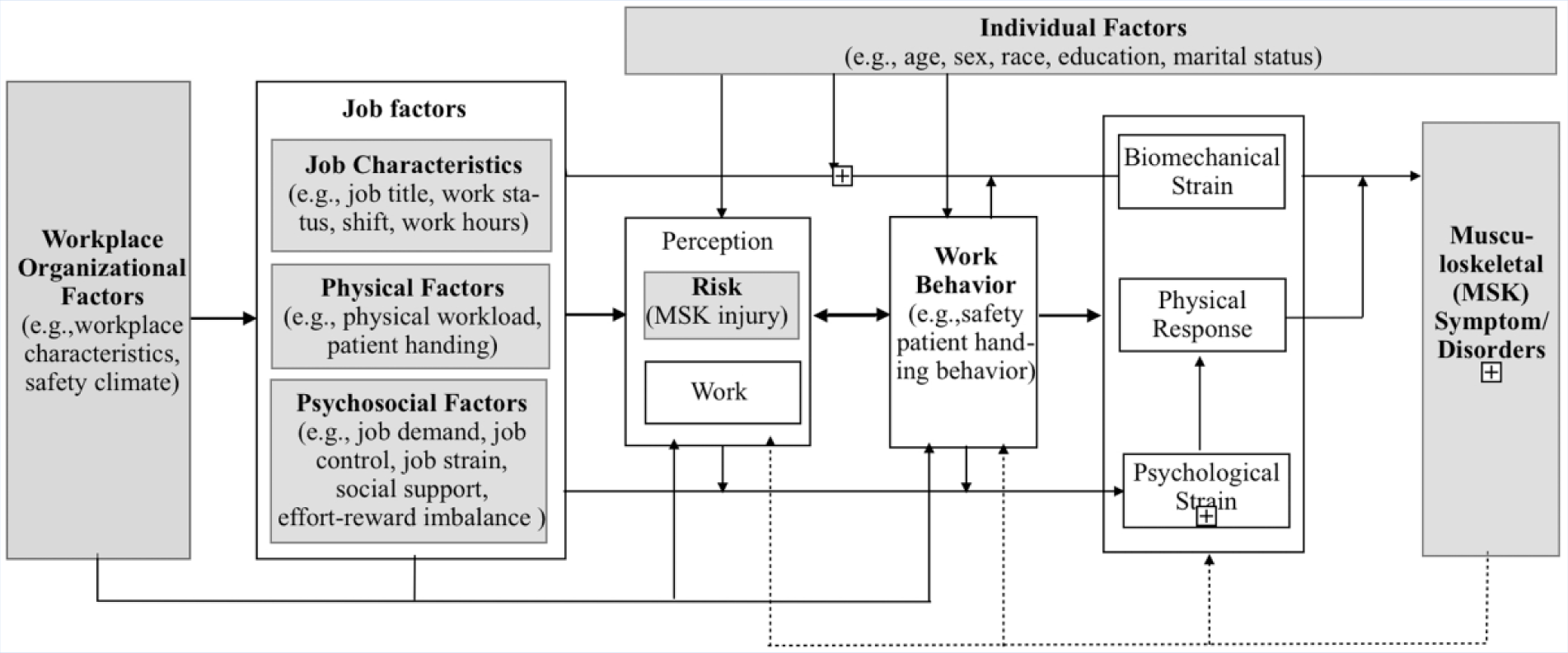
A conceptional framework for work-related musculoskeletal disorders.
S. J. Lee et al. (2013) proposed workplace organization and risk perception in a U.S. hospital setting. Risk perception is a relatively new variable proposed by Bauer (1960). Some studies have shown that the risk perception, or the self or coworkers, may be a determinant of preventive measure (Jumean et al., 2012; Yang, Qian, & Xie, 2017), with an important role in the occurrence of WRMDs.
The present study investigated the occurrence and risk factors of WRMDs, both direct and indirect, among ICU nurses in Hunan Province of China.
Method
The Research Ethics Committee of Xiang Ya Nursing School of Central South University approved the research procedures before the study commenced. In addition, approval was sought from the directors of the nursing departments and the charge nurses in the hospital study ICUs.
Study Design and Sample
This study was a cross-sectional survey of registered nurses working in mixed ICUs in Hunan Province (i.e., ICUs with critically ill patients transferred from any department). All the ICUs of tertiary hospitals in Hunan Province, except one, were willing to participate. In total, 993 nurses in ICUs were invited to participate, of which 702 (70.7%) responded. Thus, the study was comprised of nurses from 20 ICU sites in 20 tertiary hospitals. For inclusion, each nurse was a registered nurse, engaged in patient care in their daily work, and with more than 1 year of work experience. Those nurses who performed only administrative work, and thus were not involved directly in patient care, were excluded from this study.
The purpose of our study, the definition of WRMDs, and instructions for filling out the questionnaire were explained to the subjects during a face-to-face meeting. Two postgraduate nursing students and the first author were responsible for sending the questionnaire invitations to the charge nurses for dissemination to their teams. Data were collected using an online questionnaire. The questionnaire was available for completion between July and September 2017.
The survey was administered as an online questionnaire that was developed using the Chinese-based questionnaire software Sojump (Sojump, Hu Xiao, China). The software generated an online link and a quick response two-dimensional image code, to be scanned by the WeChat app on a mobile device, for participants to access and complete the questionnaire. The questionnaire was designed so that the nurses could save a partially completed questionnaire to complete later, which they had 2 weeks to complete. The WeChat app was linked to a mobile phone account. To prevent repeat submissions, each account allowed only one completion of the questionnaire. The questionnaire contained mandatory fields, to avoid incomplete surveys. As an incentive, all respondents who completed the questionnaire received $1.0 Yuan (about US$0.15) via the WeChat mobile payment red envelope function.
Of the 702 respondents, 23 ICU nurses were excluded from the sample because they did not meet the inclusion criteria: 17 and four, respectively, had less than 1 year’s work or were not employed in an ICU. In addition, two nurses were excluded because there were inconsistent or nonlogical answers. The final data analysis included questionnaires completed by 679 ICU nurses.
Study Variables and Measures
The single dependent variable of the study was musculoskeletal symptoms (Figure 1). Work-related musculoskeletal disorders were defined as musculoskeletal symptoms of ≥1 week’s duration, occurring ≥1 per month, of at least moderate intensity, which were due to a work-related event (S. J. Lee et al., 2013). Independent variables included basic demographics, factors related to the job and workplace, physical and psychosocial factors, environmental factors, and risk perception.
Musculoskeletal symptoms
Musculoskeletal symptoms were measured based on the Nordic Musculoskeletal Questionnaire translated into Chinese (Fang et al., 2013), which was designed for either self- or interviewer-administration. The first section of the questionnaire recorded history of symptoms (past 7 days, and the previous year) and the symptoms at onset in nine body regions (pain, numbness, tingling, aching, stiffness, and burning). A diagram of the body was included to allow the participant to identify affected areas. The participant reported the occurrence of WRMDs by checking the items of the affected body regions. The second section consisted of fixed-response items regarding musculoskeletal symptoms in the nine body regions that prevented normal work, and whether medical advice was sought.
Demographic and occupational information
The study questionnaire included items related to basic demographics, job factors, and workplace factors. Specifically, the demographic data consisted of the following: hospital name, gender, age, marital status, religion, height, weight, job title, education, years working in an ICU, and whether the nurse exercised. Job factors included shift frequency, monthly overtime frequency, length of break time, and the frequency of breaks per shift. The workplace factors were availability of lifting devices or a transport team, whether there was enough space to carry or transfer patients, whether taking a break in a comfortable place, risk of slips or falls in the workplace, and whether there was adequate staffing.
Perception of risk
Perception of injury risk was assessed using the Risk Perception of Musculoskeletal Injury (RPMI) measure, an instrument developed by S. J. Lee, Faucett, Gillen, Krause, and Landry (2010). After obtaining the author’s permission, the Chinese version of RPMI was translated from English to Chinese, back translated to ensure accuracy, and adjusted for cultural differences. The eight-item Chinese version of the RPMI asked about the likelihood of experiencing WRMDs within the last year, in the following four categories: nursing work in general, work tasks not related to patient handling, patient-handling tasks performed manually, and patient-handling tasks performed using a mechanical lifting device. Respondents were asked to estimate the risk to themselves or to other nurses in their units. A maximum of 48 points were possible, and the final score was the mean of the eight items. A higher score demonstrated greater perception of risk. The Cronbach’s alphas for subscales were 0.72 and 0.76. The Cronbach’s alpha for total scale was 0.78.
Physical factors
Physical factors were measured by the Nursing Physical Factors Evaluation Questionnaire, a questionnaire specifically designed for this study, based on the relevant literature (Caspi et al., 2013; Mo & Zhang, 2011). In addition, two musculoskeletal experts and an ergonomist expert were consulted, each of whom have more than 10 years of experience in musculoskeletal research and as professors in their respective fields. A 5-point Likert-type scale (0 = never to 4 = very often) was applied to measure the frequency of patient handling and the physical workload.
Specifically, the frequency of handling patients was judged according to the frequencies of the following six items: lift or transfer of a patient; use of a lifting device when a patient needed to be moved; use of a sling or sheet to move a patient; use of hands to tightly grip a belt or article of clothing to pull, lift, or reposition a patient; the transfer of patients who could not bear weight, without the use of equipment but with the help of a coworker; and lift or move a patient using just one side of the nurse’s body.
Physical workload was measured based on whether nurses were required to do any of the following: keep the hands above the shoulders, stand for a long time, sit for a long time, continuously bend or turn for a long time, hold the neck forward or back for a long time, perform the same action repeatedly, carry or transfer goods >10 kg and <20 kg, carry or transfer goods >20 kg, work that required maximum strength for a short time. The final score was the total score of the 15 items, where higher scores indicated greater ergonomic risk. The scale had good reliability and validity. The item-level content validity index of the scale was 1, and the scale-level content validity index was 0.87. Cronbach’s alphas for subscales were 0.72 and 0.81; Cronbach’s alpha for total scale was 0.73.
Psychosocial work factors
Psychosocial work factors were measured using the Job Content Questionnaire, translated into Chinese (Sha, Liu, Li, & Na, 2003). This included questions concerning skill discretion (seven items), decision authority (three items), psychological demands (nine items), physical job demands (five items), supervisor support (five items), and coworker support (six items). All items were answered with a 4-point Likert-type scale (1 = strongly disagree to 4 = strongly agree).
Decision latitude, a measure of job control, was defined as the sum of skill discretion and decision authority. Job stress was considered the combination of high job demands and low job control, and was calculated by dividing the score for psychological demands by the decision latitude score, multiplied by a correction factor (0.9) to account for the differences in the number of items. A greater ratio indicated greater job stress. Social support was the sum of scores for supervisor support and coworker support. Higher scores indicated greater social support. Cronbach’s alpha for each subscale ranged from 0.69 to 0.78. Cronbach’s alpha for the scale was 0.72.
Psychosocial work factors were also measured using the Effort-Reward Imbalance Questionnaire translated into Chinese (Zhang & Zhang, 2011), which assessed areas of effort (six items), reward (11 items), and overcommitment (6 items). A 5-point Likert-type scale (1 = strongly disagree to 5 = strongly agree) was applied to each. High effort and low reward lead to an effort-reward imbalance, which can contribute to job stress. The effort-reward imbalance ratio was calculated by dividing the effort score by the reward score and multiplying by a correction factor (0.55) to account for the difference in the number of items. A greater ratio indicated a greater imbalance. Cronbach’s alpha for each subscale was 0.88, 0.86, and 0.92, respectively. Cronbach’s alpha for the total scale was 0.91.
Environmental factors
Environmental factors were measured using the Hospital Safety Climate Questionnaire translated into Chinese (Xu, Zhang, & Wang, 2013), which was modified slightly to fit the context of this study. The questionnaire was used to measure the perception of workplace safety and environment. The main areas assessed included management support, barriers to working safely, feedback and training, conflict and communication, and cleanliness. A 5-point Likert-type scale (1 = strongly agree to 5 = strongly disagree) was used. A total of 100 points could be obtained, and the final score was the total score of the 20 items. Lower scores indicated a perception of a safer environment. Cronbach’s alpha for each subscale ranged from 0.87 to 0.92. Cronbach’s alpha for the scale was 0.94.
Data Analysis
Data analysis was performed with SPSS 19.0 (IBM, NY, USA). All online data were exported from the Sojump survey software to SPSS 19.0. Two-tailed tests with 95% confidence intervals (CIs) were used to test for statistical significance. Descriptive statistical analysis was applied to summarize the study variables. The chi-square and rank-sum tests were used for categorical variables. Student’s t test examined a bivariate association between groups of study variables.
Multivariate logistic regression analysis was performed to identify significant risk factors of WRMDs. Variables that were statistically significant at p < .05 in the univariate analysis (including chi-square test, rank-sum test, and Student’s t test) were screened and entered into the multivariate regression model. In addition, the psychosocial factors (job stress and effort-reward ratio) were included in the regression model, as we considered them important in the theoretical model. Risk perception, physical factors, and safety environment are continuous variables, and the median was used as the cutoff point to convert them to discrete variables. Odds ratios (OR) and 95% confidence intervals (CIs) were obtained using the entry method.
Results
Demographic Data
All the nurses worked in mixed ICUs of public hospitals caring for adult patients (Table 1). Most of the ICU nurses (mean age = 28.2 years) were women (88.5%), married (55.7%), and had completed a bachelor’s degree or higher in nursing (90.8%). The total time working in an ICU ranged from 1 to 32 years, and the average was 6 years.
Characteristics of Intensive Care Unit Nurses (N = 679)
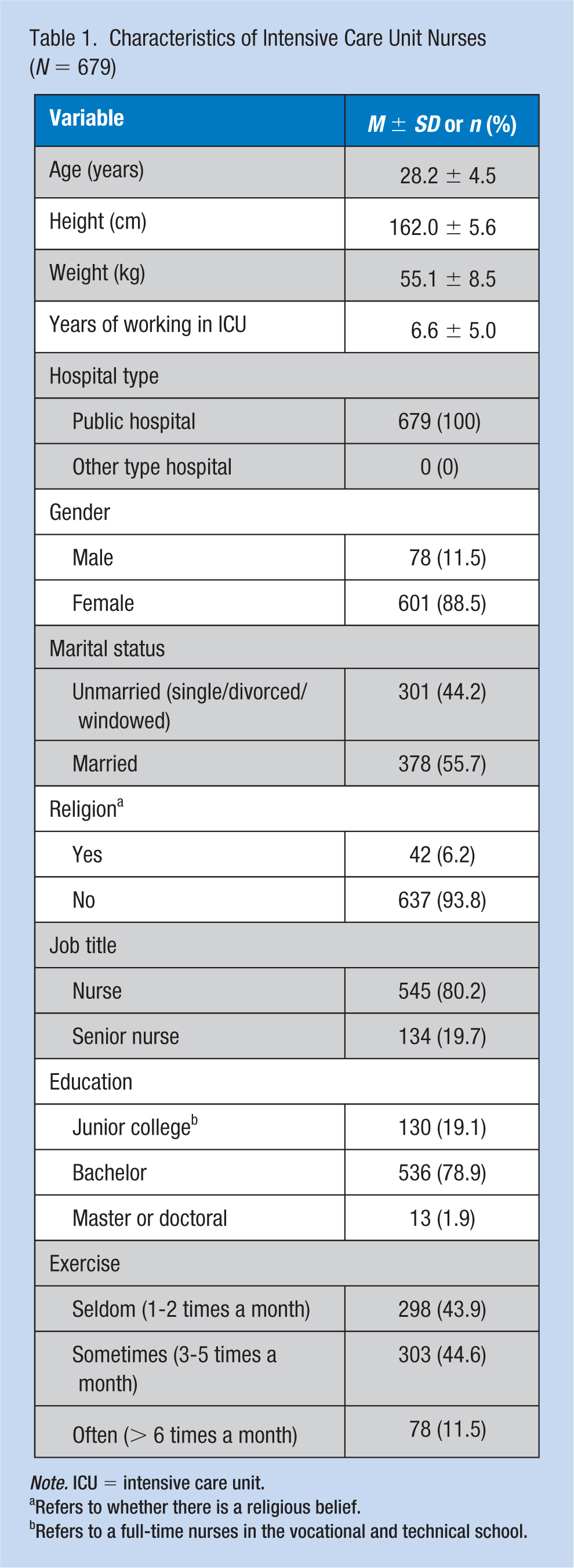
Note. ICU = intensive care unit.
Refers to whether there is a religious belief.
Refers to a full-time nurses in the vocational and technical school.
Prevalence of WRMDs
The overall prevalence of WRMDs is shown in Table 2. The 12-month prevalence of self-reported WRMDs was 97.1% (data not shown). Low back pain was the most commonly reported WRMD (80.1%), followed by neck pain (78.6%) and shoulder pain (70.4%). The prevalence of WRMDs at only one body site was 11.6%, while two or more sites had a prevalence of 88.4% (data not shown).
Prevalence of WRMDs in Intensive Care Unit Nurses (N = 679)
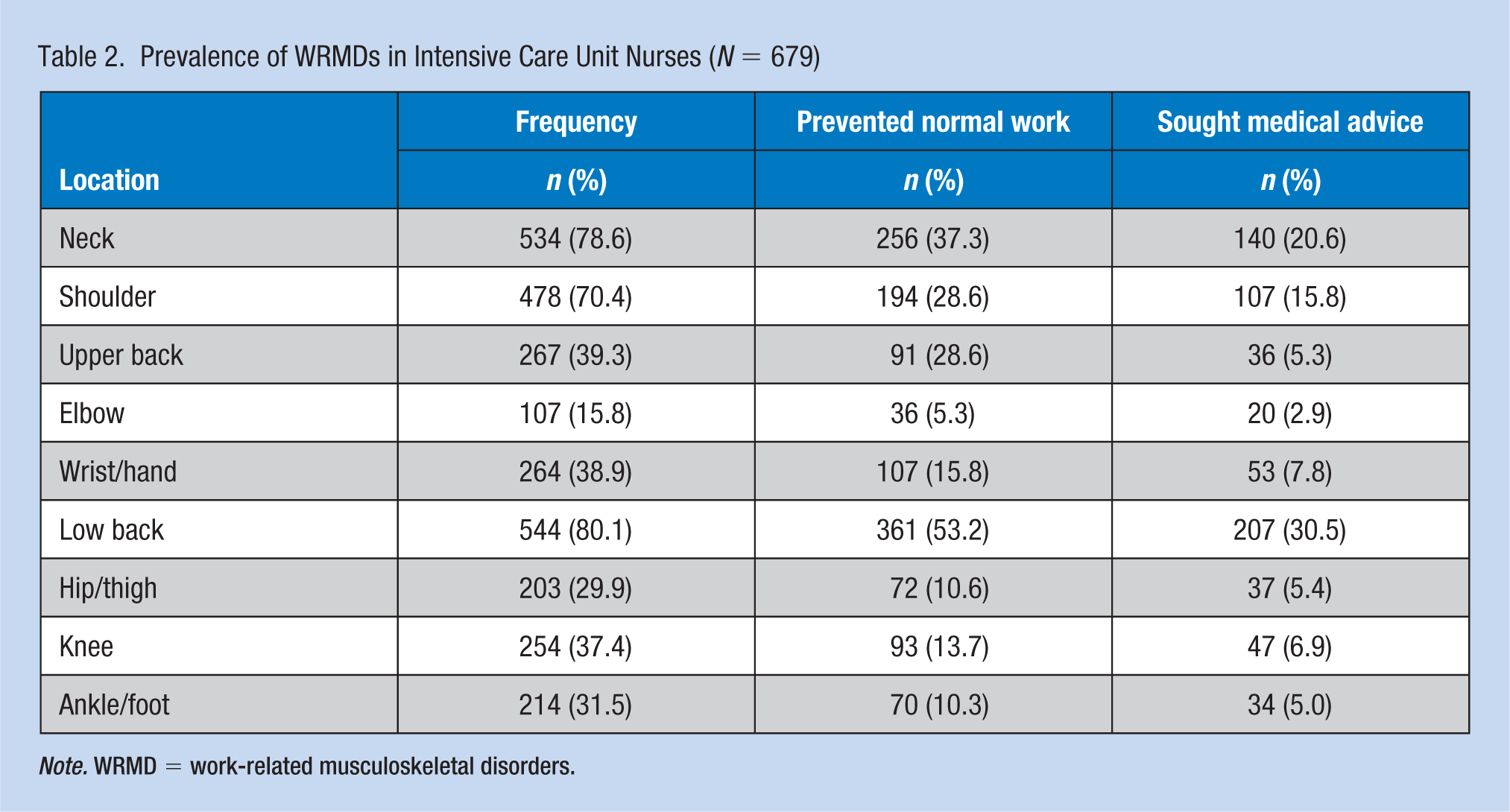
Note. WRMD = work-related musculoskeletal disorders.
Association Between Demographic and Work-Related Factors and WRMDs
Regarding individual factors, the occurrence of WRMDs was associated with gender (p = .005), marital status (p = .007), and exercise (p = .016; Table 3). Job and workplace factors associated with WRMDs were length of break times (p = .006), frequency of breaks in one shift (p = .008), and whether taking a break in a comfortable place (p = .024; Table 4). Other variables that were associated with WRMDs were risk perception (p = .003), physical work factors (p = .005), and safety environment (p < .001; Table 5).
Associations Between Worker Demographics and WRMDs (N = 679)
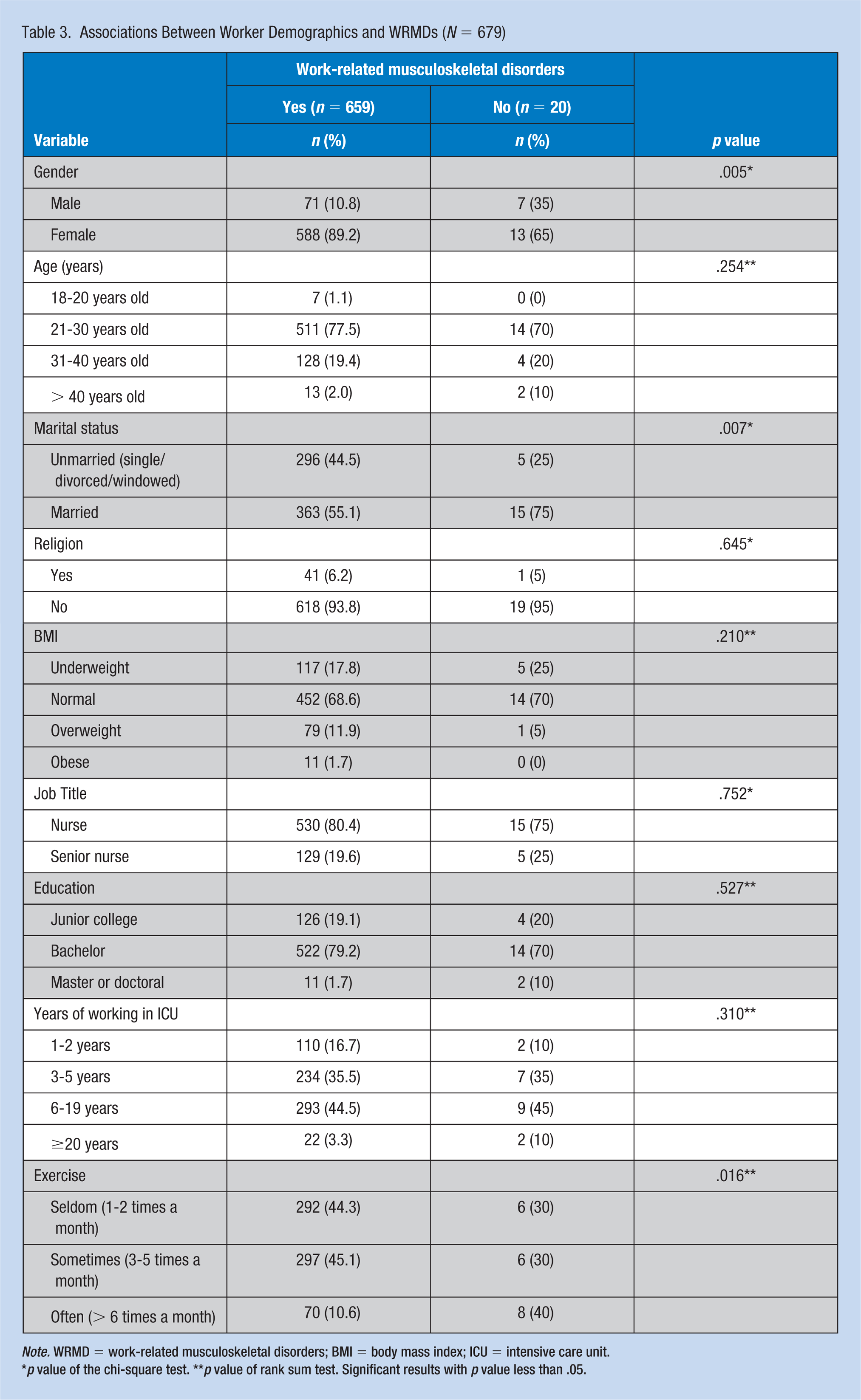
Note. WRMD = work-related musculoskeletal disorders; BMI = body mass index; ICU = intensive care unit.
p value of the chi-square test. **p value of rank sum test. Significant results with p value less than .05.
Associations Between Job and Workplace Factors and WRMDs (N = 679)
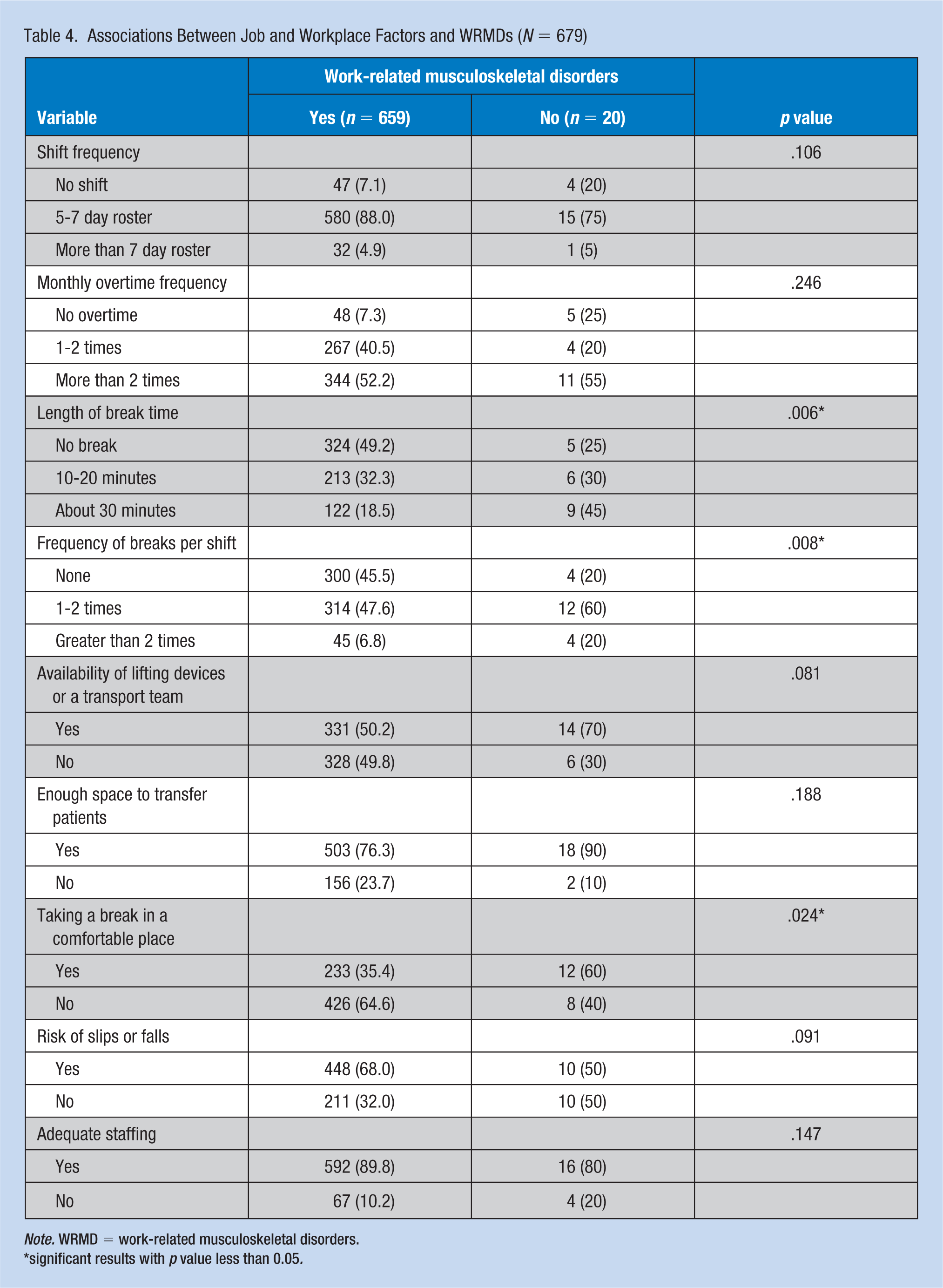
Note. WRMD = work-related musculoskeletal disorders.
significant results with p value less than 0.05.
Associations Between Risk Perception, Physical and Psychosocial Factors, and Environmental Factors and WRMDs (N = 679)
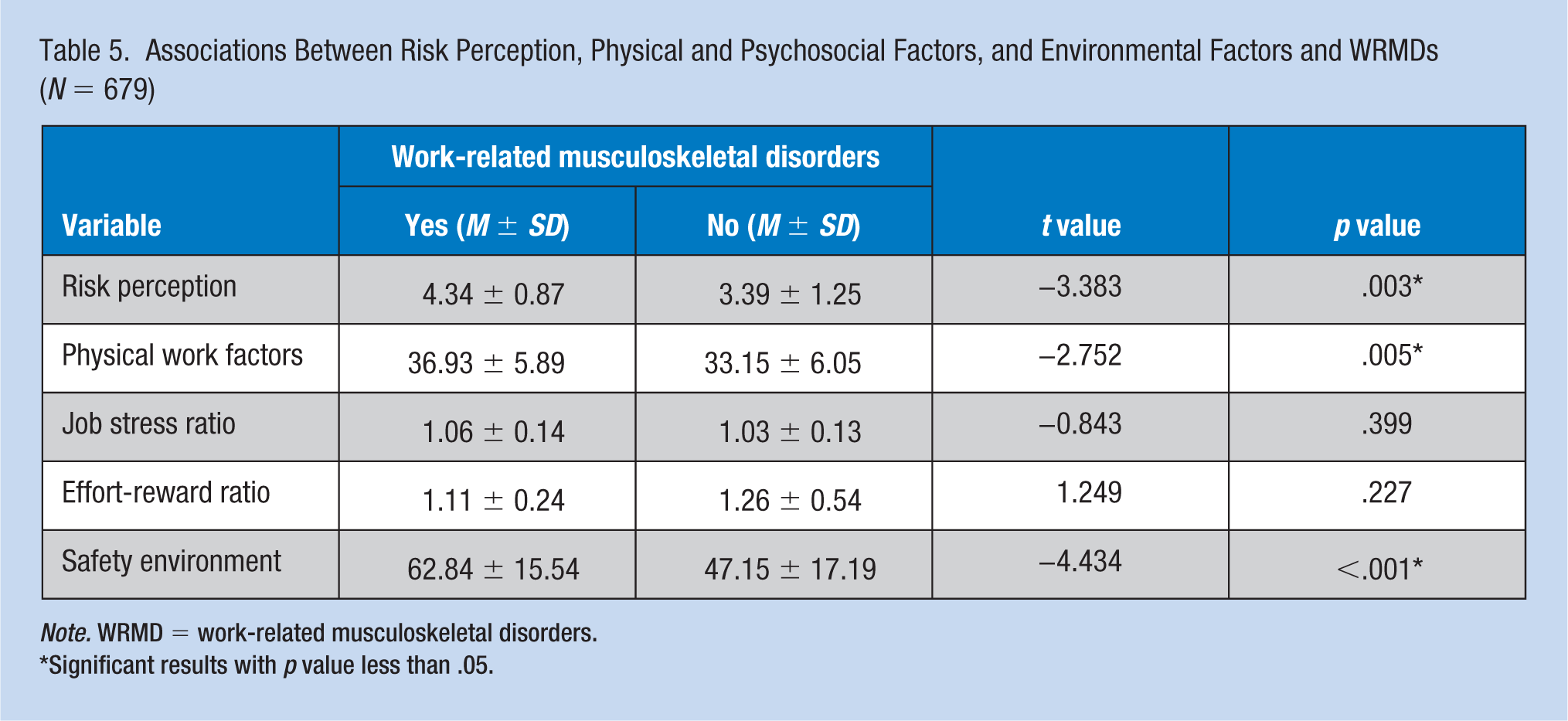
Note. WRMD = work-related musculoskeletal disorders.
Significant results with p value less than .05.
In the multivariate logistic regression analysis, four variables were significant in the final regression model and accounted for 36.7% of the variability in WRMDs (R2 = .367, p < .001). Nurses who were male (OR = 0.115, 95% CI [0.030, 0.432]) and married (OR = 0.136, 95% CI [0.034, 0.545]) had lower odds of WRMDs. Nurses with a greater perception of risk (OR = 2.352, 95% CI [1.357, 4.075]) and lack of a safe work environment were more prone to WRMDs (OR = 1.056, 95% CI [1.021, 1.093]) (Table 6).
Multivariate Logistic Regression Analysis for Risk Factors of WRMDs (N = 679)
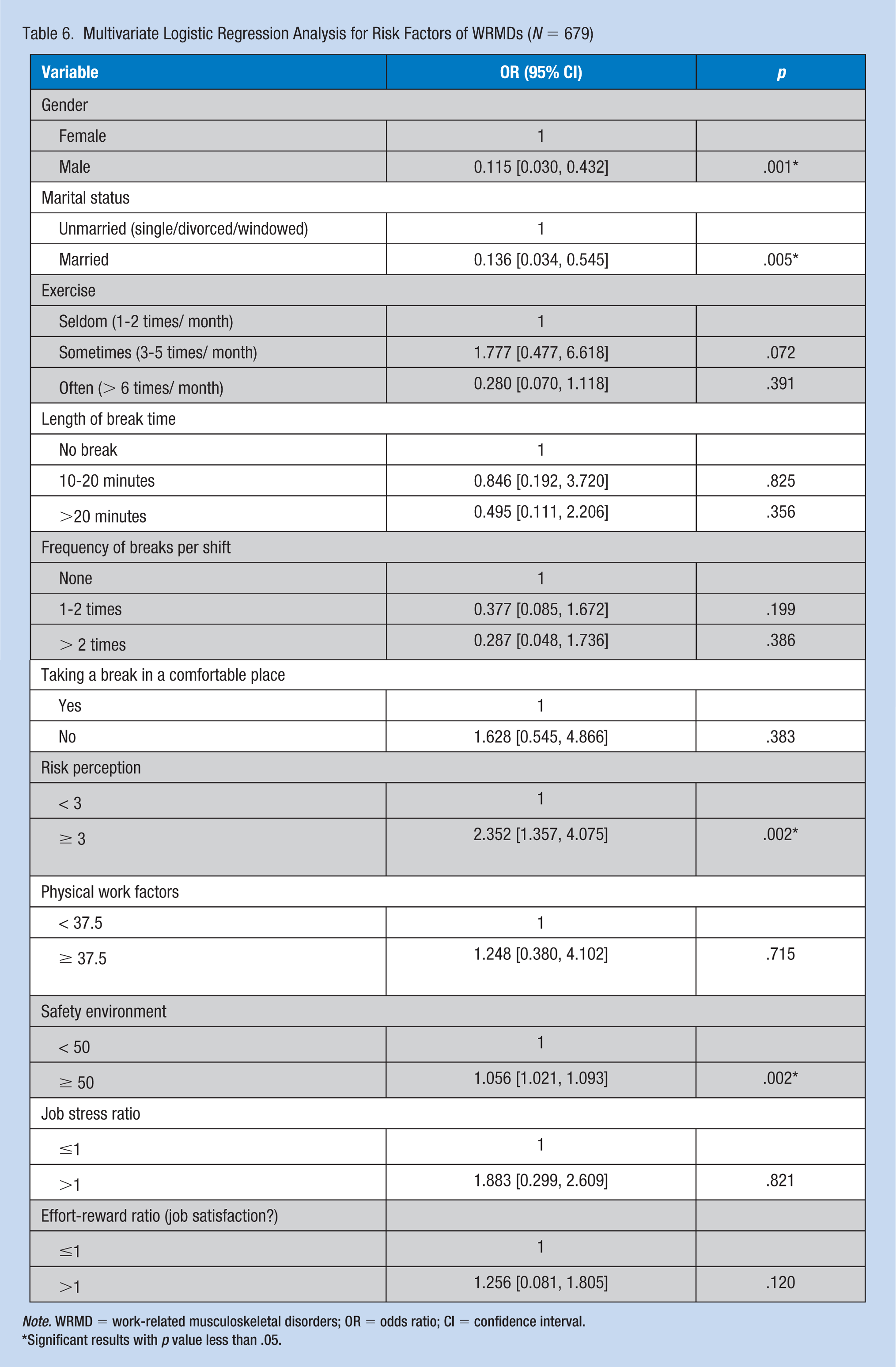
Note. WRMD = work-related musculoskeletal disorders; OR = odds ratio; CI = confidence interval.
Significant results with p value less than .05.
Discussion
The present cross-sectional study investigated the occurrence of WRMDs among nurses in mixed ICUs in Hunan Province and the direct and indirect risk factors associated with WRMDs. A self-report survey of nurses was conducted by online questionnaire, with 679 included in the final analysis. The prevalence of WRMDs among the ICU nurses was 97.1%. The most common body site affected was the low back and then the neck. This is consistent with reports from Italy, Estonia, and Australia (Carugno et al., 2012; Freimann et al., 2013; Smith & Leggat, 2004). The present analysis determined that the significant risk factors associated with WRMDs were gender, married status, risk perception, and safety environment.
In this study, nurses who were female or unmarried were more likely to report WRMDs compared with nurses who were male or married. This is in accord with previous evidence supporting the significant role of gender and marital status in reports of WRMDs (Smith & Leggat, 2004; Sugano & Nomura, 2000). The influence of gender is expected, as women are generally smaller in stature and have less muscle strength compared with their male counterparts, and the physical requirements of the occupation are prone to a higher risk of WRMDs (Munabi et al., 2014; Ribeiro et al., 2017). The spouses and families of married nurses may help buffer the effects of injuries (C. S. Lee & Dik, 2017), making them less likely to report WRMD symptoms compared with unmarried nurses.
A greater perception of risk in the ICU was associated with a higher prevalence of self-reported WRMDs. It is plausible to assume that the perception of risk is based on personal experiences and behaviors (Huffman et al., 2014). Nurses who have experienced WRMDs may have a heightened awareness of the risk of injuries and pay more attention to their musculoskeletal symptoms. S. J. Lee et al. (2013) also found that nurses who perceived themselves to be at less risk of musculoskeletal injury reported fewer musculoskeletal symptoms. The finding of a significant association between WRMDs and perception of risk is meaningful. Education and skill training provided by the hospital administration can improve awareness of the risk of injuries, promote healthy working behaviors, and ultimately prevent the occurrence of WRMDs (Ran et al., 2015).
The present study also found that the lack of a safe work environment was associated with higher odds of WRMDs. This is in accord with previous studies (Eriksen, Bruusgaard, & Knardahl, 2004; Felknor, Aday, Burau, Delclos, & Kapadia, 2000; Stone & Gershon, 2009). Nurses who perceived that the environment was safe were less likely to report WRMDs. This may be because nurses who work in an unsafe environment may feel more vulnerable concerning their health, or be more aware of the negative aspects of their working conditions. Our findings indicate a need for instituting a culture of safety in the ICU and improving working conditions (Vendittelli, Penprase, & Pittiglio, 2016).
The multiple regression analysis of the present study indicated no significant correlation between physical or psychosocial factors and WRMDs. The lack of correlation between physical factors and WRMDs is not consistent with some studies that showed that nurses who were exposed to high physical demands were more prone to WRMDs (Carugno et al., 2012; Fonseca & Fernandes, 2010). Other investigators found that physical loads or occupational lifting were not prominent risk factors (Hoe et al., 2012; Smith, Wei, Zhao, & Wang, 2004). The incongruities may be due to differences in study populations.
The lack of significant associations between psychosocial factors and WRMDs in the present study is contrary to previous reports (Cote et al., 2009; Palmer & Smedley, 2007). A possible explanation is that ICU nurses in tertiary hospitals (as in our survey) work in groups that include nurses, senior nurses, and supervisory nurses. In this setting, teamwork is common, and the stress of work is better distributed among team members. More studies are needed to explore links between physical factors, psychosocial factors, and WRMDs.
There is sparse data concerning ICU nurses in China. The present study contributes evidence from a relatively large sample. The response rates from each hospital were very good, ranging from 55.6% to 94.4%. However, there are limitations for which caution is due when interpreting the findings. First, due to the cross-sectional study design, establishing causal links between variables and WRMDs was not possible. Second, the online survey was based on self-reports, and the findings may have been affected by information bias from errors of recall or misclassification of some exposures. Third, an analysis of the validity of the questionnaire was not conducted, as it was based on four questionnaires whose validity was demonstrated in previous studies, with the sole exception being the Physical Factors Evaluation Questionnaire. Finally, data were collected only from ICU nurses in tertiary hospitals in Hunan Province and may not be representative of ICU nurses in other settings.
Conclusion
Among the ICU nurses who participated in this survey, WRMDs were highly prevalent, although contributing factors varied. Among the individual factors, female gender and being unmarried were significantly associated with WRMDs. Other significant factors included a greater perception of risk and lack of a safe work environment. By recognizing these risk factors, specific intervention strategies can be developed. Hospital and nursing managers should consider improving the workplace environment and reducing staff shortages. Nurses themselves may best identify the factors that put them at risk. Ultimately, these efforts should contribute to maintaining a healthier nursing workforce. Future research is needed to explore how these risk factors interact in the context of WRMDs.
Work-related musculoskeletal disorders are a major occupational health problem among nurses in the ICU, which may lead to absence from work or seeking other employment. Individual factors, physical factors, psychological factors, and environmental factors are identified as important factors that affect work-related musculoskeletal disorders of nurses. Some programs have been implemented to reduce the risk of musculoskeletal disorders, but with limited effect. We found that female gender and being unmarried were significantly associated with WRMDs among ICU nurses in China. Other significant factors included a greater perception of risk and lack of a safe work environment. By recognizing these risk factors, specific intervention programs can be developed to maintain a healthier nursing workforce. Hospital and nursing managers should consider improving the workplace environment and physical and psychosocial working conditions. Nurses themselves may best identify the factors that put them at risk and reinforce awareness of risk to improve individual well-being.
Footnotes
Acknowledgements
The authors express their sincere gratitude to all the critical care nurses who participated in the study, and the heads of the hospital nursing departments and the ICU charge nurses for their support and cooperation throughout this study.
Author Contributions
S.Y. designed the study, collected the data, and was a major contributor in writing the manuscript. J.L. was responsible for research, data analysis, and interpretation. L.W. and J.Z. collected data. Y.L. designed the study and assisted in drafting parts of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Shuai Yang is a PhD student at Xiang Ya Nursing School, Central South University. She interests in nursing occupational safety. She led the research project and research designed, and is the major contributor in writing the manuscript.
Jingmei Lu is a head nurse and working at Xiang Ya Hospital, Central South University. She provided overall scientific leadership and direction of the research project. She also provided statistical guidance.
Jiaqi Zeng is a master student at Xiang Ya Nursing School, Central South University. She co-led the data collection and management.
Liqian Wang is a master student at Xiang Ya Nursing School, Central South University. She participated in the data collection and management.
Yinglan Li is the director of the nursing Department of Xiang Ya Hospital, Central South University. She also is the doctoral tutor of Xiang Ya Nursing School, Central South University. She contacted the participating hospital throughout the duration of the research project.