
Abstract
Health care expenditures, patient satisfaction, and timely access to care will remain problematic if dramatic changes in health care delivery models are not developed and implemented. To combat this challenge, a Triple Aim approach is essential; Innovation in payment and health care delivery models is required. Using the Donabedian framework of structure, process, and outcome, this article describes a nurse-led employee-centered care model designed to improve consumers’ health care experiences, improve employee health, and increase access to care while reducing health care costs for employees, age 18 and older, in a corporate environment.
Keywords
Health care spending in the United States accounts for 18% of the gross domestic product (GDP) and has increased at a higher rate than the economy for 31 of the past 40 years (Institute of Medicine [IOM], 2013; Saria, 2014; Shahly, Kessler, & Duncan, 2014). In the past decade, health care costs have increased 76% compared with income growth at 30% (IOM, 2013). U.S. health care expenditures continue to rise at a rate higher than any other country, yet this investment has not led to better health outcomes for the American people (Block, 2014; Dahl, Reisetter, & Zismann, 2014; IOM, 2013; Shahly et al., 2014). In addition, Americans are experiencing a lack of timely access to primary care (Cheung, Wiler, Lowe, & Ginde, 2012; Shahly et al., 2014). With more individuals covered by health insurance, a growing population and fewer physicians specializing in primary care, individuals are either experiencing a delay in accessing care or are overutilizing emergency care (Chen, Mehrotra, & Auerbach, 2014; Phillips, Bazemore, & Peterson, 2014; Shahly et al., 2014). Furthermore, the lack of coordinated care results in significant costs with less quality, safety, and client satisfaction (Barnes, Unruh, Chukmaitov, & van Ginneken, 2014; Shahly et al., 2014). Berwick, Nolan, and Whittington (2008) call for a Triple Aim: improving the health care experience, improving the health of populations, and reducing health care costs.
The cost of, access to, and consumer satisfaction with health care will remain problematic without dramatic changes to health care delivery. Nurses have the essential knowledge and skills to address these health care challenges, yet they remain an underutilized resource in health care reform (Everett, 2013; Phillips et al., 2014). Mensik (2013) emphasized that “nursing is key to meeting the goals of the triple aim…It has been long noted in the literature that nursing care can reduce costs, improve patient satisfaction, and improve health” (p. 250). The overall purpose of this article is to describe a nurse-led, employee-centered model of care for workers in corporate environments supported by evidence and validated by experts. This model was developed to improve the health and wellness of an employee population and address health care costs, access, and satisfaction. Services are delivered by nurse practitioners (NPs), registered nurses, and health coaches via direct on-site care and telehealth are driven by the quality of the nurse–employee relationship.
Background
Health care spending and expenditures directly and indirectly impact the United States, corporate America and working Americans. Innovative solutions and alternative models of care could decrease costs and improve access to care and consumer satisfaction.
Direct and Indirect Costs
It has been projected that health care spending will comprise 19.6% of the U.S. GDP by 2024 (Bashshur et al., 2016). In comparison, the Netherland’s health care spending, second only to the United States, comprised 11.9% of its GDP in 2011 (Barnes et al., 2014). This difference does not reflect the additional US$750 billion lost annually in health care waste (IOM, 2013). The IOM defines health care waste in six domains: unnecessary services, services inefficiently delivered, prices that are too high, excess administrative costs, missed prevention opportunities, and Medicare fraud (IOM, 2013). Several additional factors have been identified as contributors to rising health care costs: increased costs of services (linked to advancements in technology), the use of incentives for reimbursement models, a growing aging population, and the likelihood of developing multiple chronic diseases (Dahl et al., 2014; Shahly et al., 2014).
An equally real, yet historically less addressed, problem relates to the significant indirect health care costs impacting corporate America. Indirect costs are defined as costs absorbed by corporations related to absenteeism, presenteeism, workers’ compensation, short-term disability, and long-term disability (Allen, Nobel, & Burton, 2012; Shahly et al., 2014). These costs are acknowledged as significant contributors to worker health and timely access to care. In 2012, the Integrated Benefits Institute estimated that Americans’ health problems cost the economy US$576 billion related to health care costs, pharmaceuticals, lost productivity, and wage replacement (Allen et al., 2012).
Employee Costs
In 2015, the Kaiser Family Foundation published findings from the seventeenth Kaiser Family Foundation, Health Research and Educational Trust (Kaiser, HRET) Employer Health Benefits Survey on health care trends. These findings revealed that health care cost trends are directly impacting employees’ personal finances. In 2015, premiums increased 4% compared with income growth of 1.9%. Between 2005 and 2015, premiums increased 61% with the employee contribution increasing 83%. To counter these increases, many employees opted for high deductible health plans (HDHP). In 2015, 24% of employees selected HDHPs with an average annual deductible of US$2,099. In comparison, in 2006, only 4% of employees selected HDHPs (Claxton et al., 2015; Kaiser, HRET, 2015).
Additional contributions and cost-sharing out-of-pocket expenses by employees are common requiring copays and deductibles. In 2015, 68% of covered employees payed copays averaging US$24 to US$37 for every in-network office visit. Annual deductibles were an even greater financial burden; 81% of covered employees were required to satisfy an annual deductible before all or most health services were paid by the health plan. The average annual deductible for all covered workers in 2015 was US$1,077. This was a 255% increase when compared with the average annual deductible in 2006 at US$303. (Claxton et al., 2015; Kaiser, HRET, 2015).
Rising health care costs negatively impact the U.S. government, corporate America and individual employees. Current trends in health care costs are not only financially unsustainable but also pose barriers to employees seeking care.
Access to Care
Contributing to escalating direct and indirect health care costs is the decline in timely access to primary care (Cheung et al., 2012). The American Association of Medical Colleges projected that the United States will experience a shortage of 12,500 to 31,000 primary care physicians by 2025 (Bashshur et al., 2016). Other sources project the shortage to increase to 45,000 to 66,000 primary care physicians (Chen et al., 2014; Everett, 2013; Phillips et al., 2014). This physician shortage combined with a projected increase in individuals seeking care, a result of nine million uninsured Americans gaining access to insurance through the Affordable Care Act, could lead to Americans experiencing delays in accessing care or overutilizing emergency care (Chen et al., 2014; Phillips et al., 2014; Sisko, 2014). Furthermore, complexity of care for individuals with multiple chronic diseases place additional time demands on providers, thus reducing office visit availability. These delays and inappropriate use of the emergency care system diminish client satisfaction with the health care experience (Marcinowicz, Chlabicz, & Grebowski, 2010).
Many employees are forced to access care during work hours. Employees unable to seek care during work hours must seek care after hours through urgent care or emergency care or choose not to access care at all. According to Bodenheimer and Pham (2010), though four fifths of clients surveyed in 2006 identified a routine care provider, only 27% could access care after hours, thus leaving 73% seeking care in costly alternative environments, not seeking any care, or taking a vacation or sick day to seek care (Bodenheimer & Pham, 2010). These options contribute to escalating health care costs and diminished consumer satisfaction.
According to the Kaiser, HRET (2015) Employee Health Benefits Survey, 57% of nonfederal public and private employers offered some of their employees’ health care benefits, a decrease from 68% in 2000 (Kaiser, HRET, 2015). These numbers signify that a substantial percentage of the employee population is without health benefits, and cost-effective, timely access to care. The stated dilemma highlights an underserved population requiring additional focus and innovative ideas for addressing their health care needs. These statistics substantiate the need to develop innovative models to address this underserved working population.
Donabedian Framework
Donabedian’s framework was used to describe and validate this Employee-Centered Care Model. Donabedian’s framework of structure–process–outcomes was introduced in 1966 as a method for evaluating quality of care (Donabedian, 1966). Originally developed exclusively for the evaluation of medical care, the model has been well established in health care research, including nursing, as a strong empirical framework that has assessed the quality of nursing care and clinical practice (Cohen & Shang, 2015).
Donabedian’s framework proposes that quality “medical care” can be assessed through structure, process, and outcomes. Structure includes the human, physical, and financial resources needed to deliver quality “medical care” (Donabedian, 1966; Holt, Zabler, & Baisch, 2014). Process includes the methods that providers use to deliver care to a population (Donabedian, 1966). Finally, outcomes are measured through changes that occur in “health, knowledge, behavior and satisfaction of the target population that can be attributed to antecedent health care” (Holt et al., 2014, p. 430; Donabedian, 1966). Donabedian emphasized that each component of the framework (structure, process, and outcomes) is influenced by the previous component, highlighting the interdependence of all three components. The success of outcomes is influenced by the strength of the structure and process (Donabedian, 1966).
Employee-Centered Care Model
The Employee-Centered Care Model is a hybrid approach combining on-site care with virtual health appointments for employees working in corporate environments. The model schematic in Figure 1 shows the relationship of the model’s structure, process, and outcomes, acknowledging the goals of the Triple Aim. This schematic specifically highlights how the nurse–employee relationship is activated for workers’ minor health problems and how care is provided to address these problems.
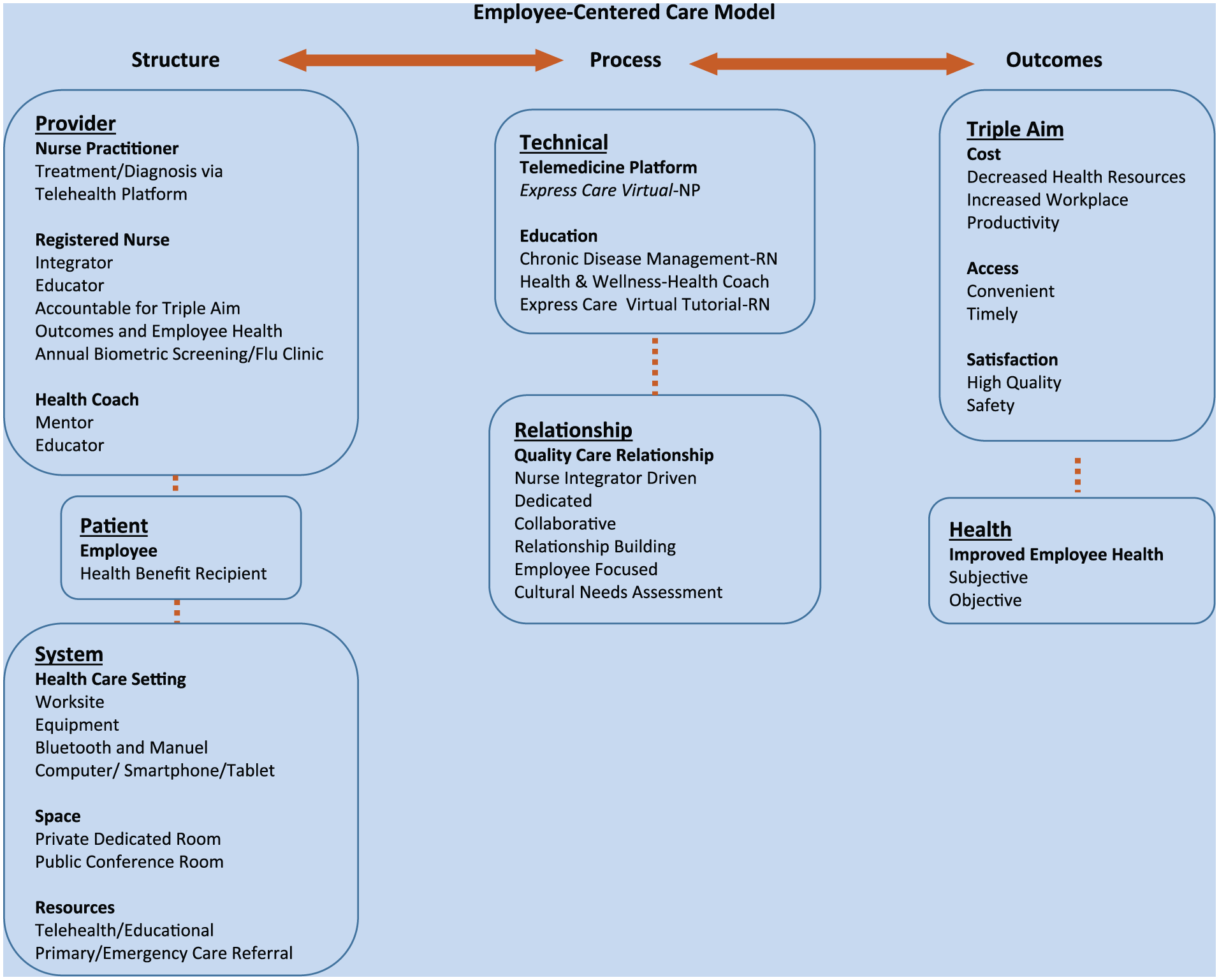
The employee-centered care model schematic.
In this article, the authors present advantages of applying the Employee-Centered Care Model which includes provider utilization, overhead costs, and employee-centered/personalized care. Contract services of a registered nurse or health coach and an established telemedicine platform, versus employment of an on-site multilayer health clinic team, can immediately reduce costs. A registered nurse and health coach on-site, and a virtual care clinic, increase immediate access to care and convenience for employees. In addition, ensuring patient-centered care reinforces a personalized relationship based on trust and patient satisfaction (Chenoweth, Matin, Pankowski, & Raymond, 2008). This model is not intended to replace employees’ primary care providers but serves as a bridge between primary and urgent care for employees who seek immediate access to care during or after work hours. Currently, this model has been implemented as a pilot at a self-insured corporation in Portland, Oregon. A self-insured corporation is an entity that assumes financial responsibility for employee health care costs. For future publication, ongoing data analytics are being collected on the effectiveness of this Employee-Centered Care Model.
Description of the Model
Applying a patient-centered philosophy, using direct personalized care, and telehealth, this model includes a team comprising a NP, registered nurse, and health coach. The objective of this nurse-led model is to provide health and wellness services and education to employees working in corporate environments.
Structure, the first component of the employee-centered model, includes employee, provider, and the delivery system. These components are vital to the delivery of care. Employees are defined as individuals hired by corporations and receive health care benefits. The general age of employees ranges from 18 to 65 years. Providers include a NP who is available to employees via a telehealth platform and an on-site registered nurse (RN) and health coach. Services provided by this team include diagnosis and treatment of minor illnesses and injuries, triage for major health conditions, preventive and wellness health education, chronic disease management, biometric screenings, and an annual influenza vaccination clinic.
The NP, a licensed, board-certified health care provider, and an employee of the telehealth platform, diagnoses and treats employee illnesses and injuries via virtual telehealth appointments provided through Express Care Virtual. The roles of the on-site RN are integrator and educator. The RN triages employees to Express Care Virtual or an urgent care or emergency department, depending upon severity of the conditions presented. The RN also provides chronic disease management and health education. Annually, the RN facilitates biometric screenings and an influenza vaccination clinic. A minimum of a bachelor’s degree in nursing is required for this position. Services provided by a health coach include activities of health and well-being, diet and exercise, and social wellness. Health coaches “educate and support clients to achieve their health goals through lifestyle and behavior adjustments” (Institute of Integrative Nutrition, 2016).
Services are provided at the corporate workplace on a limited basis Monday through Friday during day hours. A dedicated private room is used for health assessment, chronic disease management, and consultation. A public conference room is available for preventive, wellness, and health education activities. Equipment on site includes Bluetooth and manual stethoscopes, a sphygmomanometer, and educational literature. The RN and health coach are on site 2 days each week. In addition, employees’ personal computers, smartphones, or tablets are required to access the telehealth platform. Employees can access Express Care Virtual for treatment of minor illnesses and injuries with or without the assistance of the RN. Express Care Virtual operates 7 days per week between the 8:00 a.m. and midnight in Oregon, Washington, and Montana and 8:00 a.m. to 8:00 p.m. in California. This model does not provide emergency department services (Providence Express Care Virtual, n.d.). Emergencies are triaged to the appropriate facility.
Process, the second component of the model, was identified by Donabedian as the methods used to deliver care to a population. The primary process components of this model are the use of a telehealth platform offered through Express Care Virtual and the role of a nurse integrator fostering a dedicated, caring relationship. Express Care Virtual provides same-day, online health care visits with a NP. No appointment is necessary. Employees access care via their personal computers, smartphones or tablets. After online registration is completed, general wait time to start the virtual visit is approximately 4 minutes. Virtual visits allow both the NP and the employee face-to-face contact. Pictures can be downloaded and sent by the employee to the NP for additional objective data needed for diagnosis. Examples of common conditions diagnosed and treated are shown in Figure 2. If needed, X-ray and laboratory tests can be ordered at a nearby facility and prescriptions can be sent to a local pharmacy. A postvisit e-mail is sent to employees outlining the diagnosis, treatment, and plan of care. An additional phone call is made by the NP to the employee 1 to 2 days after the virtual visit. Employees can request a summary of the virtual appointment be sent to their primary care providers. The virtual visit is documented in an Epic electronic medical record. All interactions and correspondence are confidential, secure, and HIPPA (Health Insurance Portability and Accountability Act)-approved. Reimbursement for virtual visits is a flat fee of US$39 per visit (Providence Express Care Virtual, n.d.).
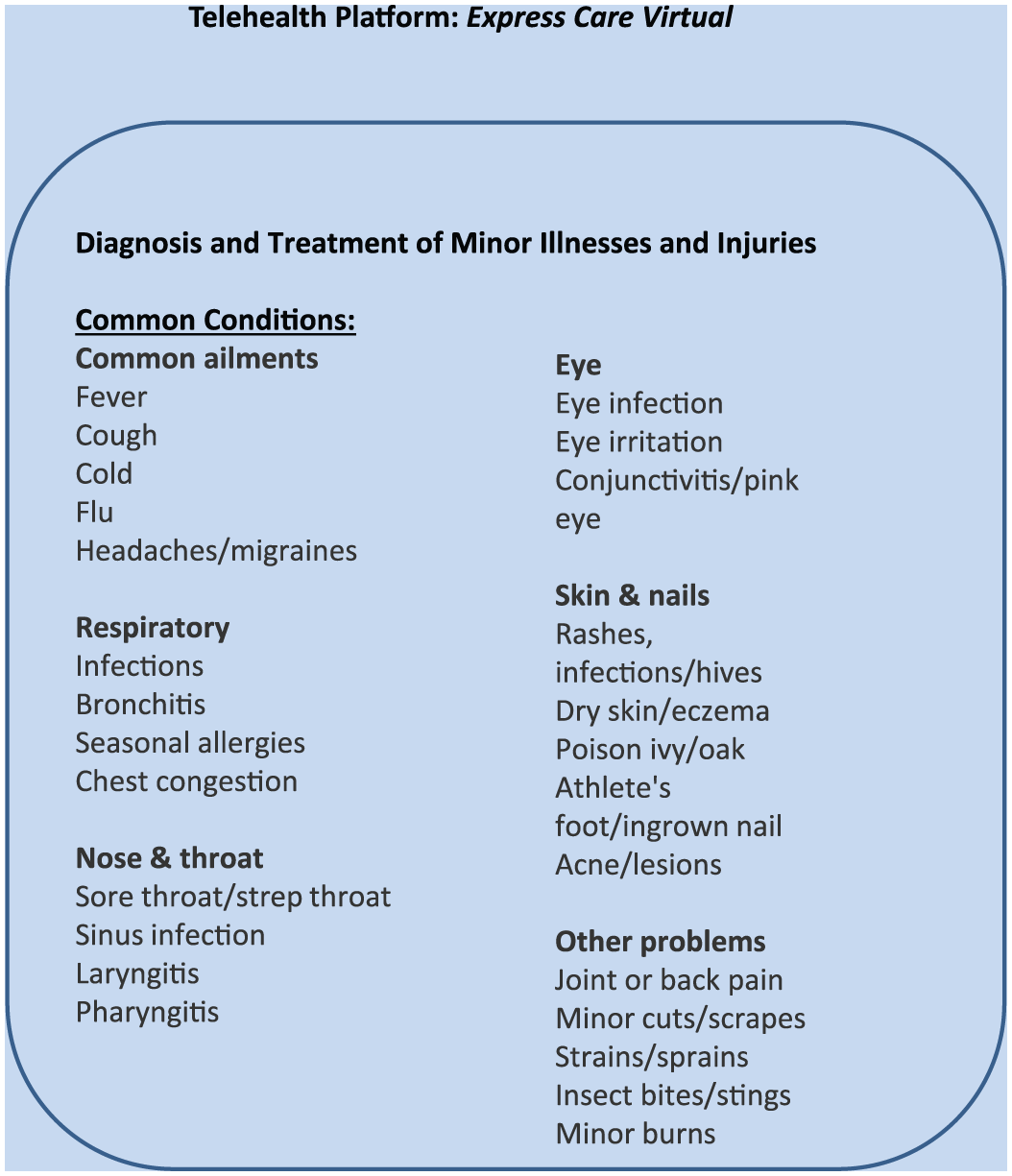
Examples of common conditions diagnosed and treated by nurse practitioners via telehealth platform, Express Care Virtual.
The role of the nurse integrator is essential to the process of the Employee-Centered Care Model (see Figure 3). The magnitude of success and use of the telehealth platform is dependent on the presence of the nurse integrator. The nurse integrator develops a trusting relationship with employees and assumes responsibility for achieving the Triple Aim with the employee population. Through relationship building, the nurse integrator assesses the culture and needs of the employee population. Through these assessments, monthly health lectures are offered on topics that directly address the needs of the employees. Weekly blood pressure screenings and health and wellness consultations are offered. The nurse integrator educates the employee population on the role and value of Express Care Virtual. When on site, the nurse integrator assists employees with virtual visits. In addition, the nurse integrator fosters a working relationship with the Express Care Virtual providers and employees’ primary care providers. These collaborative relationships reinforce the delivery of safe, quality care for both the employee and provider. The nurse integrator role is vital in driving the outcomes of cost, access, satisfaction, and employee health. Reimbursement for services is a monthly retainer of a per employee/per month fee.
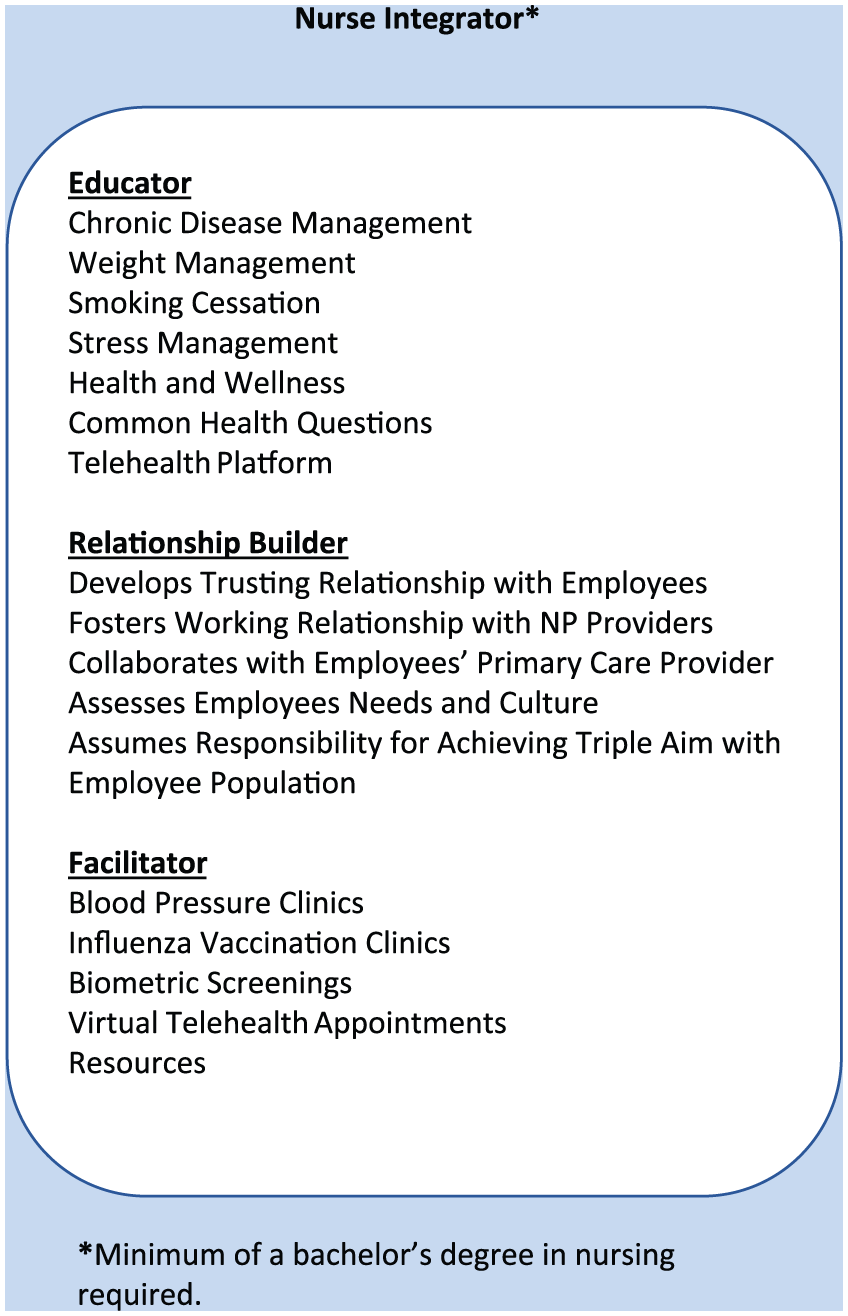
Description of the role of the nurse integrator.
Outcomes are the third component of the Employee-Centered Care Model. Two types of outcomes are addressed: Triple Aim and employee health. Through the structure and process of this Employee-Centered Care Model, deliverables include improved access to care, less health care costs, and improved employee health and satisfaction. Improved employee health can be subjective or objective, quantified through employees’ feelings about their health and well-being or supportive health data. Evaluation of the employee experience is collected through an anonymous evaluation tool. Furthermore, health services rendered at the worksite improve access, workplace productivity, and culturally competent care (Betancourt, Corbett, & Bondaryk, 2014; Chenoweth & Garrett, 2006; Shahly et al., 2014).
The described components of structure and process in this model positively impact the outcomes of improved access and cost outlined in the Triple Aim. Outcomes are dynamic and dependent upon the relationship between structure and process. Continual improvements are directly related to the multidirectional relationship between structure and process.
Model Validity
A two-step process was used to ensure the validity of the model description. First, the description was documented by the first author and reviewed by the second author after completion of the following: (a) content was identified through a systematic literature review; (b) content was organized into 20 specific components; and (c) similar components were grouped into categories (Lazenby, Dixon, Coviello, & McCorkle, 2014; see appendix). Second, once both authors agreed on the accuracy of the model based on the evidence, a panel of four experts was identified and asked to review the article and model. Selection of experts was based on professional expertise and contributions to the literature. A structured form was constructed for recording experts’ ratings of components, reflecting sections of the manuscript and the three figures.
Each expert independently reviewed and rated the components for relevance and clarity using a standardized form with binary response options of “yes” or “no” for relevance and “high” or “ low” for clarity (Lazenby et al., 2014). The form also included a column for suggestions. For Relevance, each of the 20 components received rating of “yes” from each of the four experts. Based on standardized method for calculating the content validity index (CVI), this data may be regarded as a Relevance Index (similar to CVI) of 1.0. For Clarity, 16 of 20 components received ratings of “high” from each of the four experts, and four of the components received ratings of “high” from three experts and “low” from one expert (no component received a low rating from more than one expert). These data yielded a Clarity Index of .95 by averaging component clarity values across the components (Polit, Beck, & Owen, 2007). Thus, both the Relevance Index and Clarity Index exceeded the standard of .90 proposed by Polit et al. (2007) for assessing content validity of instruments. Based on Clarity ratings and accompanying comments by experts, the authors revised the article to include a section on the cost–benefit of the model.
Cost–Benefit Analysis
This model is an example of an innovative model of care addressing the Triple Aim. Further cost analysis between an on-site clinic and this Employee-Centered Care Model demonstrated that the model can be cost-effective and sustainable. McCaskill, Scwartz, Derouin, and Pegram (2014) identified the operating expenses for human resources of an on-site clinic at US$574.73 per day (cost includes time and labor for company-employed NP, registered nurse, and certified nursing assistant). Assuming the clinic operated Monday through Friday, excluding holidays, the clinic would cost US$144,257.23 per year.
During the 1-year study period, a total of 976 employee visits for all diagnoses were documented (McCaskill et al., 2014). Comparing the cost of the Employee-Centered Care Model, if all 976 employee visits were serviced by Express Care Virtual and reimbursed at US$39.00 per visit, the total cost of care would be US$38,064. Additional costs to the model is the contracted monthly retainer of per employee/per month fee paid for services provided by the registered nurse and health coach. Recommended spending for wellness plan services ranged from US$8.33 to US$12.50 per employee/per month or US$100 to US$150 per employee/per year (Wellness Council of America, 2016). Using the US$8.33 to US$12.50 per employee/per month fee range and the 267 employees provided by McCaskill et al. (2014), the total additional costs are US$2,224.11 to US$3,337.50 per month or US$26,689.32 to US$40,050 per year. Using the provided data, the overall 1-year cost for the Employee-Centered Care Model equals US$64,753.32 to US$78,114. This range results in a savings of US$66,193.23 to US$79,503.91 per year (McCaskill et al., 2014). These numbers only reflect operating costs and do not reflect the additional savings of health costs for the employer and employee by model implementation. Added benefit for employees is cost-free care beyond their primary care providers.
Discussion
Innovation in care delivery models is essential to meet the demands of an uncertain health care climate. Building on the strong and dedicated history of occupational health and community health nurses, the nursing profession is equipped to propose and implement solutions that will improve the quality and safety of employee health care while addressing the goals of the Triple Aim.
As noted, this Employee-Centered Care Model offers an innovated approach to caring for an employee population. Building on the demonstrated successes of worksite clinics, nurse-managed health centers (NMHCs), telehealth, and quality-care relationships published in the literature, this model introduces a unique hybrid approach not yet in use today. The strength of this model is highlighted in the process related to the dedicated role of the nurse integrator and the use of a telehealth platform. In addition, sustainability is demonstrated by a reimbursement model that is more cost-effective than treatment of minor illness and injury at a worksite clinic, urgent care, or emergency department. Corporations already allocate funds for worksite wellness programs. This author suggests that these funds would be more effectively allocated to the Employee-Centered Care Model. With added services in telehealth and an on-site dedicated registered nurse, the corporation could have superior service, healthier employees, and better return on investment (ROI).
The implications of the Employee-Centered Care Model on the practice of occupational and environmental health nurses are explicit. Occupational and environmental health nursing is a unique specialty that focuses on the care of a worker population by providing for and delivering services that improve health and safety (American Association of Occupational Health Nurses, 2017). This Employee-Centered Care Model compliments the practice of occupational health nurses by incorporating on-site education and activities for health promotion and chronic disease management and enhances specialty nursing practice by offering immediate access to a board-certified provider for care of minor illnesses and injuries via a telehealth platform. The additive component of telehealth directly increases access to, decreases cost of, and improves satisfaction with employee care but additionally has potential to address the collateral impact of untreated or off-site treated employees on worksite productivity.
Conclusion
In this article, the authors presented an innovative Employee-Centered Model of Care designed to improve employee health by addressing the Triple Aim. Specifically, using a nurse-led, Employee-Centered Care Model for corporate employees can potentially improve the health of this population while reducing cost, increasing access to care, and improving consumer satisfaction. Due to the uncertainty surrounding the Patient Protection and the Affordable Care Act, a crucial need exists for innovative models of care to improve population health. This article offers one example of an innovative care model that may be applicable to other populations. The next phase of this project is to report on the effectiveness of the model from the data analytics collected during the pilot stage.
Footnotes
Appendix
Acknowledgements
The authors are grateful to the expert panel for their review of the manuscript and the model. They included Dr. Mary Bartlett, DNP, APRN, FN-BC, Former Medical Director and Founder of Fair Haven and Assistant Professor of Nursing, Linfield University; Dr. Sherrie McCaskill, DNP, FNP-C, Director of The Health Center, Wingate University; Jeannie Tomlinson, MSN, RN, COHN-S, FAAOHN, AVP, Director of Health and Wellness at The Hartford; and Dolores Foglio, MSN, FNP, RN, Express Care Virtual Provider. The authors acknowledge the editorial assistance of Nicholas Pasacreta, the literature search expertise of Janene Batten, and the expert panel rating contribution of Dr. Jane Dixon.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Kelly Fox is founder and president of Healthcare Professionals of Portland in Portland, Oregon, and adjunct instructor at the University of Portland School of Nursing.
Ruth McCorkle is the Florence S. Wald Professor of Nursing and a professor of epidemiology at Yale University. She teaches in the Post-Masters’ Doctorate of Nursing Practice Program at Yale School of Nursing.