
Abstract
Background/aims:
The idea that champions are crucial to effective healthcare-related implementation has gained broad acceptance; yet the champion construct has been hampered by inconsistent use across the published literature. This integrative review sought to establish the current state of the literature on champions in healthcare settings and bring greater clarity to this important construct.
Methods:
This integrative review was limited to research articles in peer-reviewed, English-language journals published from 1980 to 2016. Searches were conducted on the online MEDLINE database via OVID and PubMed using the keyword “champion.” Several additional terms often describe champions and were also included as keywords: implementation leader, opinion leader, facilitator, and change agent. Bibliographies of full-text articles that met inclusion criteria were reviewed for additional references not yet identified via the main strategy of conducting keyword searches in MEDLINE. A five-member team abstracted all full-text articles meeting inclusion criteria.
Results:
The final dataset for the integrative review consisted of 199 unique articles. Use of the term champion varied widely across the articles with respect to topic, specific job positions, or broader organizational roles. The most common method for operationalizing champion for purposes of analysis was the use of a dichotomous variable designating champion presence or absence. Four studies randomly allocated of the presence or absence of champions.
Conclusions:
The number of published champion-related articles has markedly increased: more articles were published during the last two years of this review (i.e. 2015–2016) than during its first 30 years (i.e. 1980–2009).
The number of champion-related articles has continued to increase sharply since the year 2000. Individual studies consistently found that champions were important positive influences on implementation effectiveness. Although few in number, the randomized trials of champions that have been conducted demonstrate the feasibility of using experimental design to study the effects of champions in healthcare.
Introduction
Implementation science is a relatively young field within health services research that is concerned with the systematic study of methods and strategies that promote the uptake of evidence-based interventions into routine clinical practice. 1 One factor often cited in this literature as crucial to effective implementation in healthcare is the role of the “champion.” Relatively little, though, is understood about how or why champions appear to be so important to successful healthcare-related implementation. 2 Few studies have attempted to isolate and measure a specific “champion effect,” or to describe and explain the particular mechanisms by which champions influence implementation processes and related outcomes.
One of the major challenges in investigating the role of champions in healthcare-related implementation is that different terms have been used over the last 35 years in the published literature to refer to the underlying construct of “champion.” This conundrum has been referred to elsewhere as the “jangle fallacy,” part of the larger “jingle-jangle fallacy.”3,4 For example, while the terms “change agent” and “opinion leader” typically refer to specific roles distinct and apart from the champion role, both terms have also been used in the literature to refer directly to the construct of “champion.” This instability in the use of language and the lack of fixed, formal, and universally accepted definitions for a construct like “champion” can lead to confusion and conflation of terms, making it more difficult to understand how and why champions are cited so often as key factors in the implementation process. Furthermore, this foundational gap prevents development of valid and reliable measurement instruments and approaches. 5
Furthermore, many variations on the term “champion” itself have appeared in the healthcare implementation literature, including clinical champion, program champion, internal champion, and change champion, among others. Champions also surface across the implementation spectrum: sometimes as part of an intervention, sometimes as part of an implementation strategy, and sometimes as neither, as when they reside naturally in the context in which implementation occurs. These issues present further challenges for analyzing champions across studies and contexts.
We conducted an integrative review of champions in healthcare-related implementation to bring greater clarity to an important construct in implementation science that has been hampered by inconsistent use across the published literature and to establish the current state of the literature on this key construct. The integrative review approach is particularly well-suited for reviewing a topic across diverse research designs and methodologies to provide a more comprehensive understanding of the phenomenon under study.6,7
Methods
Conceptual framework and the “champion” construct
In this integrative review, we define the construct of “champion” as an implementation-related role occupied by people who (1) are internal to an organization; (2) generally have an intrinsic interest and commitment to implementing a change; (3) work diligently and relentlessly to drive implementation forward, even if those efforts receive no formal recognition or compensation; (4) are enthusiastic, dynamic, energetic, personable, and persistent; and (5) have strength of conviction. The Consolidated Framework for Implementation Research (CFIR) serves as the conceptual and theoretical framework guiding this integrative review. 8 The CFIR draws upon 20 years of published literature in implementation research and contextualizes the construct of “champion” within the larger context of implementation science. In the CFIR, the construct of “champion” falls within the domain of “implementation process.”
Search strategy and study selection
The lead investigator (EJM) searched the online MEDLINE database via OVID and PubMed using the keyword “champion,” which identified articles in the context of healthcare where the search term appeared anywhere in the multi-purpose set of fields that included title, abstract, and subject heading. Because other terms are often used to describe champions, we conducted additional searches using the following keywords: implementation leader, opinion leader, facilitator, and change agent. When MEDLINE search results yielded an abstract that potentially met inclusion criteria, the lead investigator retrieved and reviewed the full text of the article and conducted a second screening. Full-text articles that passed this second screening were forwarded to the study team for data abstraction. As a supplemental search strategy, bibliographies of full-text articles that met inclusion criteria were also reviewed for additional references not yet identified via the main strategy of conducting keyword searches in MEDLINE.
Inclusion and exclusion criteria
This integrative review was limited to research articles related to healthcare in peer-reviewed, English-language journals published from 1980 to 2016. All articles were indexed in MEDLINE and accessible in full-text format. Articles were excluded from the integrative review if they were written solely in a language other than English, appeared in journals that were not peer-reviewed, reported no data or outcomes, were review articles, were not retrievable in a full-text version, or were published before 1980 or after 2016. Articles could be from any country as long as they met all inclusion criteria.
Data extraction
A five-member doctoral-level team (EJM, NR, AAS, MEF, TMD) abstracted all full-text articles meeting inclusion criteria using a 27-field standardized template in NVivo10 specifically developed for this integrative review. Standardized data abstraction fields included basic bibliographic information (year published, lead author, journal, title), whether or not the article met specific inclusion criteria (English-language, peer-reviewed journal, included data or outcomes, published 1980 or later, full text available), search information (full text retrieved, search strategy used, database searched, forwarded for data abstraction), and information related to the content of the article (terms used in study for clinical champion, structured abstract, study design, conceptual framework of study, job position of champion, clinical area of champion, number of champions in study, champion activities described in study, outcomes associated with champion activities, facilitators to champion activities, barriers to champion activities, reported characteristics of effective clinical champions, reported mechanisms linking champion activities with outcomes). To ensure consistent abstraction of articles across study team members, a second reviewer (TMD, AAS) independently and blindly extracted 15% of all articles that met inclusion criteria. Any questions or disagreements among the study team related to data abstraction were resolved by discussion and consensus.
Data synthesis
Extracted data for all articles meeting inclusion criteria were merged into a single, unified NVivo10 project file. This NVivo10 project file allowed the creation of tables and matrices that summarized the data in both quantitative and qualitative format; text-based queries of the entire dataset by article, field, and keyword, including searches using Boolean operators; and data visualizations that cross-referenced quantitative and qualitative information from the combined dataset. The results of these analyses led iteratively to an overall synthesis of the role of the champion in healthcare-related implementation in the published literature.
This integrative review reports the following results: number of champion articles published over time, different types of champions reported in the literature, different terms used to refer to the champion construct, how champion was measured across studies, studies that experimentally manipulated the presence or absence of champions, odds ratios reported for champions, patterns in how studies reported out champion findings, studies that examined the role of multiple champions at the same site, studies that used other research designs, job positions and clinical areas of champions, number of champions reported in studies, facilitators and barriers, champion activities, and characteristics of effective champions.
Results
Number of champion articles
Search strategies yielded 4886 abstracts in MEDLINE that were potential matches. Of these, 469 articles passed the initial and second screening, were retrieved in full-text format, and forwarded for data abstraction. Upon further review, 270 of these 469 articles were later found not to meet full inclusion criteria and excluded. The final dataset for the integrative review consisted of 199 unique articles. (See S1 figure for a PRISMA diagram of study selection.)
As shown in Figure 1, the number of published articles on champions sharply increased over the last decade. While only a few articles meeting inclusion criteria were published prior to 2000, the number of champion articles nearly tripled between 2000–2004 and 2005–2009, and then tripled once more in 2010–2014. Nearly three-fourths of the articles meeting inclusion for this review (149/199) were published after 2009. More articles were published during the two years of 2015–2016 than in the combined 30 years from 1980–2009.
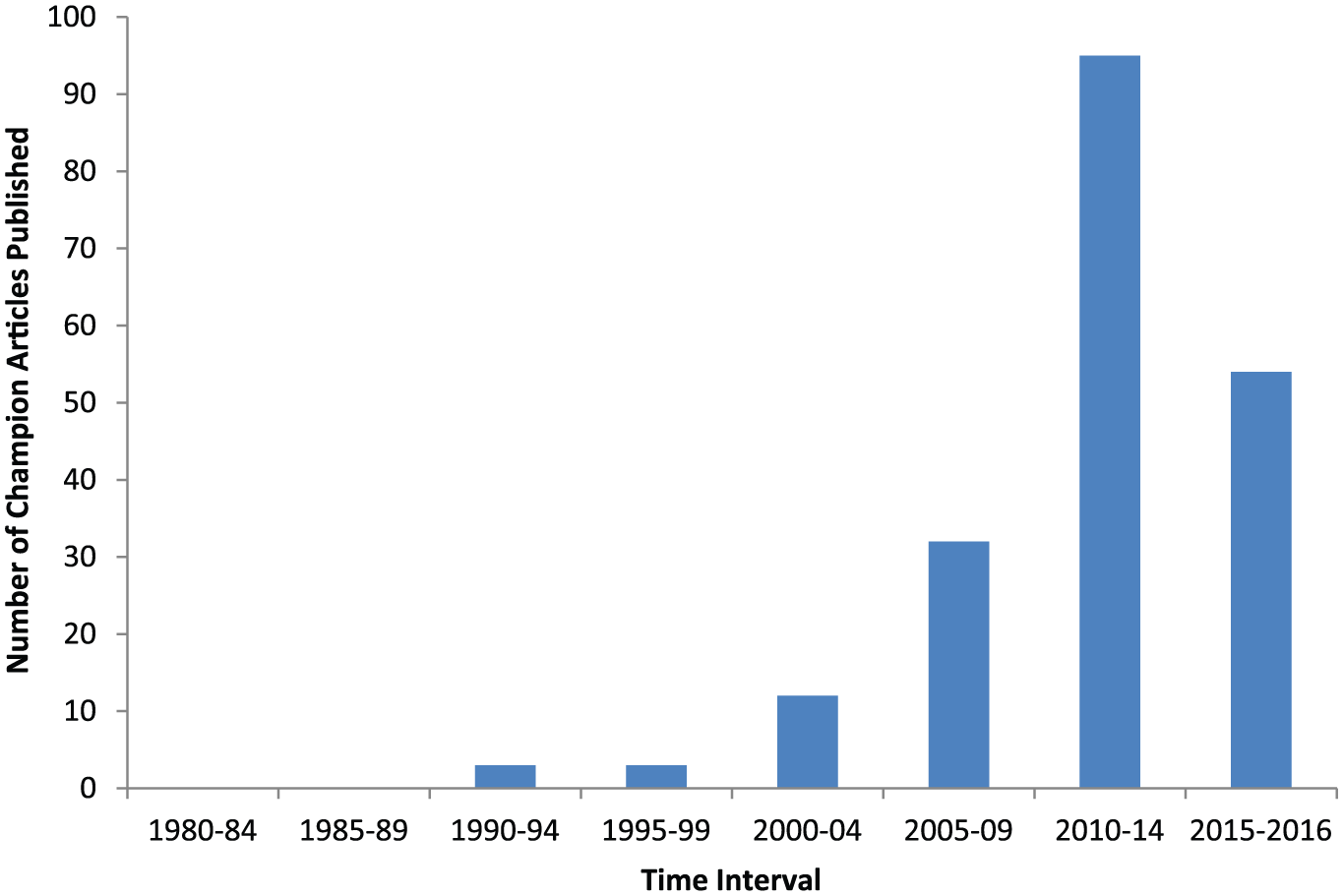
Number of articles published that met inclusion criteria by 5-year intervals from 1980–2014 and the 2-year interval of 2015–2016.
There were 188 unique first authors listed across the 199 articles; no single author stood out from the others as closely identified with champion research.
Most of the articles considered champions as one of several implementation components or organizational factors that could potentially mediate or moderate a study’s main outcomes; champions did not constitute the central focus of the study. Over time, however, the number of articles explicitly focused on champions themselves markedly increased, accompanying the jump in the number of champion articles in general. For example, the term “champion” itself only appeared twice between 1980 and 2008 in the title of any articles that met inclusion criteria, a period that represented the entire first half of the integrative review’s 35-year timeframe. In the year 2009 alone, however, the term “champion” surfaced in article titles three times2,9,10 and then at least once every year thereafter, including five times in 2012.11–15
Different types of champions
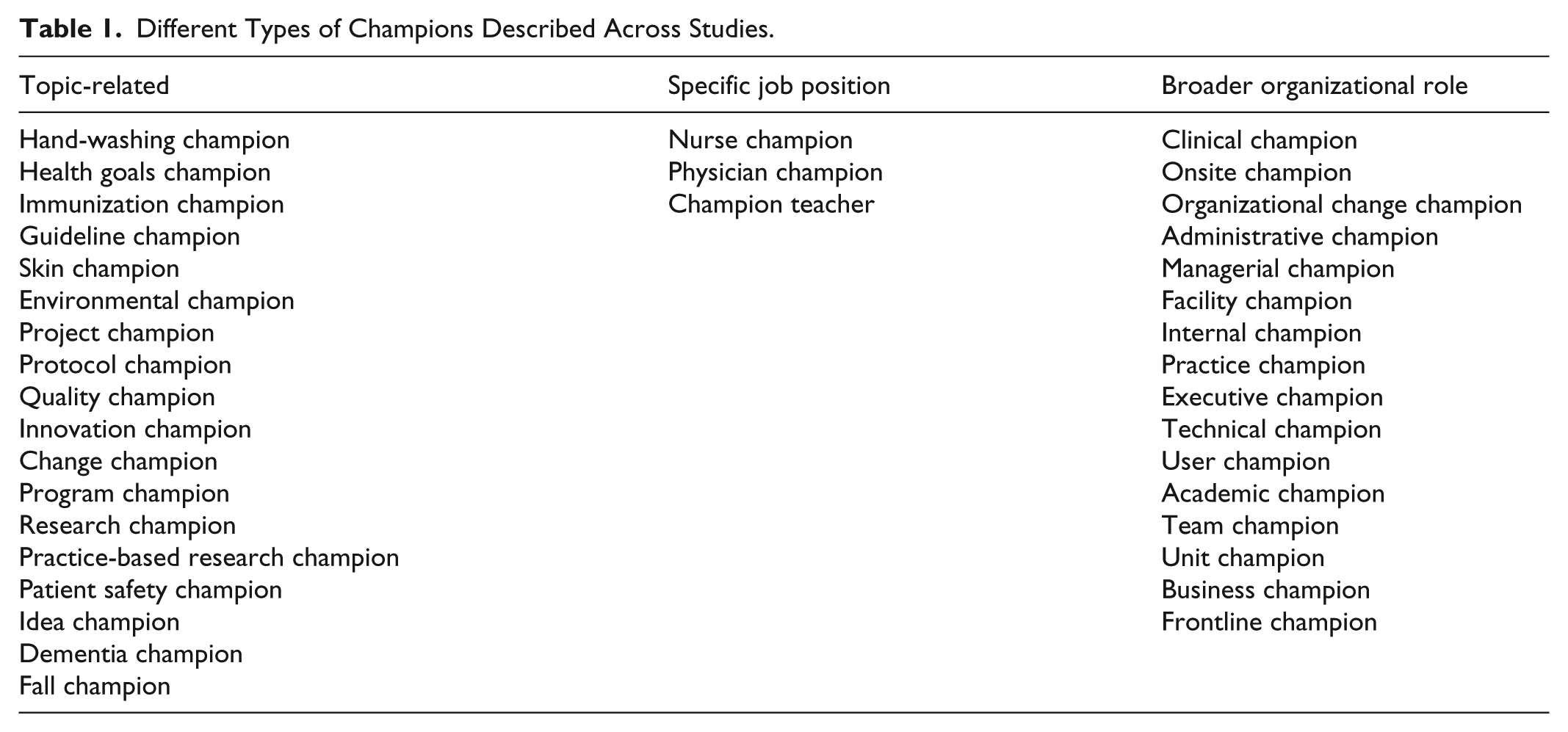
Use of the term “champion” varied widely across the articles with respect to (1) topic (e.g. hand-washing champion, guideline champion, program champion), (2) specific job positions (e.g. physician champion, nurse champion), or (3) broader organizational roles (e.g. executive champion, clinical champion), especially in studies where multiple champions operated simultaneously at single sites. Table 1 lists the variations of champions across these three categories.
Different Types of Champions Described Across Studies.
Alternative terms for champion
Terms other than “champion” were used to refer to this construct. Alternatives included change agent, opinion leader, advocate, liaison, facilitator, main supporter, practice leader, key influencer, cheerleader, and key stakeholder. When authors employed these alternative terms to refer to the champion construct, they typically did not use the term “champion” itself in their articles—the alternative terms served as wholesale substitutions. A notable exception to this substitution pattern, though, was the term “opinion leader”: authors on multiple occasions applied the term “opinion leader” and “champion” in the same study to refer to the same person, often in the same sentence. For example, question 13c on the Organizational Readiness to Change Assessment (ORCA) instrument asked respondents to rate their level of agreement with the statement “The Project Clinical Champion is considered a clinical opinion leader”; 16 an intervention arm of a trial of guideline dissemination in surgery was randomized to a web-based resource “championed by opinion leaders”; 17 and a program designed to help nurses detect delirium superimposed on dementia relied on “unit champions,” defined as “local or external opinion leaders who are seen by others as trustworthy and who can persuade others to implement evidence-based practice.” 18
Operationalizing champions
Authors used various approaches for operationalizing “champion” for purposes of analysis. By far, the most common method across studies was the use of a dichotomous variable designating champion “presence or absence,” employed in over 90% of articles. Most of these articles simply designated if a champion was present or not, though a few operationalized the dichotomous variable as the presence or absence of an effective champion, with effectiveness defined with the context of the individual study.19,20 A few articles operationalized champions in non-dichotomous ways based on skills or effectiveness: these strategies included introducing an intermediate value midway between present and absent to designate champions with limited influence 21 or “questionable effectiveness”; 22 using a performance index that ranged continuously between 0 and 1 based on the presence or absence of six champion components; 23 rating champions using a Likert-type scale on degree of leadership and advocacy effectiveness; 24 and rating champions between −2 and +2 based on the relative strength (strong or weak) and direction (positive, negative, or neutral) of their influence on the implementation process. 25
Studies with random allocation of presence or absence of champions
In terms of research design, only 4 of the 199 champion studies randomly allocated the presence or absence of a champion. Three of these studies randomly allocated champions within a randomized-controlled trial (RCT), and a fourth used a quasi-experimental design. All four of these studies were conducted outside of the United States (see Table 2).
Results from Four Studies Randomly Allocating Presence or Absence of Champions.

RCT: randomized-controlled trial; RR: risk ratio.
One of these studies was conducted in Australia and evaluated a multicomponent staff education intervention to improve staff detection of depression in residential aged care settings. 26 In this three-arm RCT, randomization was carried out at the facility level, and the intervention group (n = 2 facilities) was compared with a control group (n = 3) as well as with an “intervention plus” group where the educational program was enhanced by the addition of a screening process and the formal identification and designation of a “study champion” (n = 3). The effects of the champions in this RCT were mixed: the champion group performed better with respect to one of two outcomes but the other two arms performed better on the other outcome. 26
A second RCT with random allocation of the presence or absence of a champion was a study of 180 neonatal units in the United Kingdom. Neonatal units were randomly assigned to either a control arm (n = 93) where clinicians received information about evidence-based preterm baby care for babies born with a gestation period of fewer than 27 weeks through passive dissemination channels (sent a copy of a report, slides and position statement) or to an active arm (n = 87) where the same dissemination activities were enhanced through the recruitment and training of volunteer clinicians in those units to act as champions for the active dissemination and local implementation of evidence-based preterm baby care. Results were once again mixed: the champion arm performed better with respect to only two of four main outcomes. 27
A third RCT to allocate the presence or absence of a local champion using randomization was a Canadian cluster randomized trial of a school-wide program to improve elementary school children’s physical activity that took place in 2003–2004. Schools were randomly assigned to one of three conditions: to implement the program with support from an external facilitator (n = 4 schools); to implement the program with support from an “internal champion,” a designated teacher who worked at the same school (n = 3); or to usual practice (n = 3). This RCT found that the external facilitator condition and the champion conditions both outperformed the usual practice condition in terms of the main outcome but the external facilitator and champion conditions did not significantly differ from one another. 28
A fourth study employed a quasi-experimental design to assess the effect of local champions on increasing influenza vaccination rates among staff at a Canadian acute care facility. Work units within this site were randomly assigned to champion present (n = 23) or champion absent (n = 23) conditions. The champion arm significantly outperformed the no champion arm with respect to the main outcome. 29
Calculating a summary statistic of the effect of champions based on these four studies was not possible, given the small number of studies, and the broad diversity in settings, research questions, outcome measures, and types of champions. However, these four studies collectively demonstrated the feasibility of randomly allocating the presence and absence of champions within the broader context of healthcare.
Designs of champion studies
The vast majority of studies featured research designs other than random allocation of the presence or absence of champions. These represented a wide spectrum of designs used in implementation research and health services research, including case studies, cross-case comparisons, surveys, interview studies, formative evaluation, program evaluation, pre/post repeated measures design, Qualitative Comparative Analysis, action research, quality improvement (QI), demonstration projects, and secondary data analyses.
Odds ratios for champions
Seven studies reported odds ratios specifically for champions, six of which featured positive results (i.e. 95% confidence intervals non-overlapping with 1.0) as summarized in Table 3. Six of the seven studies relied on surveys.
Results from Seven Studies Reporting ORs Specifically for Champions.

OR: odds ratio; CI: confidence interval; EBSCT: evidence-based smoking cessation treatment.
Champions as key factors
A fundamental finding that recurred across more than 80% of champion articles involved the identification of champions as one of several key factors associated with implementation success. Examples included the following: Effective leadership, the presence of a system champion, availability of technical training and support, and adequate resources are essential elements to the success of the electronic medical record (EMR)
37
A focus on patient satisfaction, the presence of a team champion, and the involvement of the physicians on the team were each consistently and positively associated with greater perceived team effectiveness
38
Contributions to success included having a protocol champion, a sepsis education program, and a nurse educator
39
Factors significantly associated with high implementation were high level of involvement from the administrator or director of nursing, high level of nurse manager participation, presence of in-house dietitian, high level of participation of staff educator and QI personnel, presence of an internal champion, and team’s openness to redesign
40
One study used Qualitative Comparative Analysis to determine how 17 different conditions—including champions—combined in support of implementation success. One of four identified solutions for successful implementation of the VA MOVE! Program across 22 VA Medical Centers involved the combination of an active physician champion with low program accountability to facility leadership. 20
Solo versus multiple champions
Five articles raised questions about the effectiveness of a solo champion, finding instead that multiple champions had to work simultaneously in a coordinated way at a single site in order for implementation success to occur. Damschroder et al.
9
found that: it was possible for a single well-placed champion to implement a new technology, but more than one champion was needed when an improvement required people to change behaviours. Although the behavioural change itself may appear to be an inexpensive and simple solution, implementation was often more complicated than changing technology because behavioural changes required interprofessional coalitions working together.
Soo et al. 2 found that multiple champions had to leverage their respective organizational position and networks to forward the implementation process, including executive champions who held senior leadership positions within the organization; managerial champions who were responsible for managing clinical departments, wards, or units; and clinical champions who were frontline clinicians. Marsteller et al. 41 found that small office practices most likely to engage in QI practices successfully “had a strong physician champion determined to make QI changes and a strong office manager (in offices with multiple staff members) equally determined to make changes.” Shaw et al. 13 found that ambulatory practices with two discrete types of champions—project champions and organizational change champions—were most successful in implementing and sustaining diabetes care processes. Kuehl et al. 42 found that a “Champ-and-Chief Model” directly connected to successful implementation of a firefighter wellness program, requiring both the presence of an enthusiastic local champion along with a fire chief who was willing to grant permission for the program to proceed.
Champion characteristics
Champion activities reported across studies included tenaciously advocating for an initiative within the work environment; facilitating reflection; serving as team leader; motivating staff; engaging in planning activities; educating and training staff about the initiative; making a business case to leadership; persuading staff that the initiative was important and worthwhile; developing pamphlets, stickers, and posters; building relationships with key stakeholders; boundary-spanning across service lines; spending one-on-one time with staff; being visibly identified with the initiative; recruiting team members for implementation; using data to persuade peers; and troubleshooting problems that emerge during implementation.
Specific characteristics of effective champions included negotiation skills; advocacy; communication across organizational boundaries; enthusiasm and energy to drive the implementation process; fully understanding both the initiative and the local context; maintaining a positive focus; strong educator and presentation skills; a personal belief in the initiative and commitment to its successful implementation; being personable, respected, credible, and well-liked by peers; having political acumen; leading teams and recruiting new team members; providing vocal, highly visible support and encouragement for the initiative; collaborating well with others; engaging in team planning and goal-setting; and collecting data, tracking progress, and providing feedback.
In terms of psychometric studies and instrument development, three secondary data analyses examined the validity and reliability of the champion construct as an item measure or subscale within a broader measure of organizational readiness.16,19,35 No studies in the review involved the development or validation of a standardized instrument that could identify champions, measure champion effectiveness, or differentiate among champion types.
Discussion
Champion research has increased sharply in recent years. An inflection point in champion research appeared to take place in 2009, when champions started to become the focal point of studies themselves. That year, the term “champion” first appeared consistently in the titles of articles; studies on multiple champions were first published; and the seminal article introducing the CFIR appeared in Implementation Science, identifying champions as 1 of 39 key constructs linked to implementation success. After 2009, the number of champion articles spiked sharply upward, tripling in 2010–2014 over the previous 5-year period and reaching a total of nearly one hundred articles. In several respects, since 2009 champions have begun to move from the left side of the equation to the right, becoming an outcome of interest in their own right in addition to being studied as mediators and moderators of implementation success.
Evidence from the handful of trials with random allocation of the presence or absence of champions was generally positive but mixed. Nearly all studies reporting odds ratios for champions found positive and significant associations with implementation outcomes. More than 80% of champion articles identified champions as one of several key factors associated with implementation success. Individual champion studies consistently found that champions were important to implementation. Considered together, these studies collectively indicated that champions represented a “necessary but not sufficient” condition for implementation success: champions alone were inadequate to bring about change, yet in combination with other factors proved essential to implementation success.
This cross-study “necessary but not sufficient” finding could help move the literature beyond the basic, recurring finding that “champions are important.” Next logical steps for future champion research include examining how and why champions are so important to implementation by conducting additional studies with random allocation of the presence and absence of champions; expanding upon and extending the excellent in-depth qualitative work already conducted in studies like Damschroder et al., 9 Soo et al., 2 and Henry et al.; 43 using configurational comparative methods like Qualitative Comparative Analysis, as in Kahwati et al.; 20 operationalizing champions using methods more nuanced than presence/absence, such as those outlined in Damschroder and Lowery; 25 and pioneering new approaches like Process Tracing 44 that have not yet been applied to the champion literature.
Limitations
This review included only articles published in English and thus did not benefit from work on champions published in other languages. 45 With its goal of understanding the role of champions in healthcare-related implementation, the review focused entirely on champions in healthcare settings, and did not integrate findings on champions from fields and disciplines not indexed in MEDLINE. Despite best efforts, the search strategy used in the review likely missed articles that could have met inclusion criteria due to wide variation in terms being used to refer to underlying champion construct. This review was not able to isolate or calculate an effect size for champions due to the small number of studies with random allocation of the presence and absence of champions.
Conclusion
This integrative review brings greater clarity to an important construct in implementation science that has seen a sharp increase in the number of published articles in recent years. Randomized trials on champions in healthcare have been few in number but include the random allocation of the presence or absence of champions, demonstrating that this type of research is feasible. Individual studies consistently found that champions were important to implementation.
Supplementary Material
Supplementary Material, S1_Figure_ – Inside help: An integrative review of champions in healthcare-related implementation
Supplementary Material, S1_Figure_ for Inside help: An integrative review of champions in healthcare-related implementation by Edward J Miech Nicholas A Rattray, Mindy E Flanagan, Laura Damschroder, Arlene A Schmid and Teresa M Damush in SAGE Open Medicine
Footnotes
Acknowledgements
The authors wish to thank Anne Sales for her original suggestion to conduct a review on this topic and Brian Mittman for his review of an earlier version of this manuscript. Preliminary findings from an earlier version of this review were presented as an internal work-in-progress during a VA HSR&D Cyberseminar in June 2016.
Authors’ Contribution
All authors made significant contributions to the manuscript. EJM conducted the searches and reviewed articles for inclusion. EJM, NR, MEF, AAS, and TMD extracted data. EJM, MEF, and TMD analyzed and interpreted data. EJM drafted and revised the manuscript and prepared figures and tables. NR, MEF, LD, AAS, and TMD made important intellectual contributions by providing detailed feedback on different iterations of the manuscript. All authors have read and gave final approval of the version of the manuscript submitted for publication.
Data availability
All relevant data are within the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for a review article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This integrative review was sponsored through internal funding provided by the VA Stroke QUERI Center based at the Roudebush VAMC in Indianapolis, Indiana (STR-03-168). The authors retain sole responsibility for the content of this review.
Informed consent
Informed consent for patient information to be published in this article was not obtained because it is a review article.
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.