
Abstract
Evaluating nursing competence is challenging and among many instruments the Nurse Competence Scale is one of the most used. This integrated literature review aimed to describe how ontological and contextual nursing competence becomes evident in evaluations done with it and the value of using it for professional development in nursing. The starting point was a former systematic review and additional searches were carried out using electronic databases with keywords and Boolean operators. The search followed the PRISMA search strategy and the articles were appraised against the JBI Critical Appraisal Checklist. Thirty-four original research articles published between January 2004 and April 2020 were included. The data were displayed and analyzed descriptively. Results showed that the Nurse Competence Scale covers both ontological and contextual competence, that the competence profiles vary in different cultures, cohorts and contexts, but that it is suitable for evaluating and following up competence development in nursing.
Introduction
In a world of changes, new competencies are needed. Mobility between countries is encouraged, and within the European Union, the educational aim is to ensure comparable and compatible systems and a competence that enables mobility within Europe. This has led to considerable changes in nursing education. 1 New knowledge and skills enter nursing, and one needs to consider what students need to learn during education and what kind of further education is needed in practice. Continuously defining, evaluating and developing competence in nursing is crucial. No general standards exist, but the trend shows a move against a holistic view of competence.2,3
In evaluating and developing nursing competence various perspectives need to be considered. A division of formal competence conferred by a degree certificate, subjective competence experienced and objective competence witnessed by others, is feasible. 4 The question arises about the general competence needed and about ways to evaluate it. Competence independent of context, transferable and unique for nursing sees caring as the core, with its roots in ethos, which throughout time has been formed by the idea of love and charity. 5 This ontological competence, illuminating caring in thought, words, attitude and deeds, affects the caring culture and thereby how nursing is performed. An ethos of human dignity shapes every caring act and makes ontological competence visible. 5
When caring is moved into context, structural features surface depending on the nature of the ward, diagnosis, different treatments and technology used. In some contexts, emphasis is placed on clinical performance of skills in specific fields, but ontology should manifest itself in all different clinical contexts. In context the caring/nursing culture on the ward as well as the organizational and leadership culture affects the nursing process and the way competence is viewed.6–11 and since evaluations often focus on specific contexts or even specific skills it raises the question what really is evaluated.11–14
Generic instruments have been developed to evaluate nursing competence in a holistic, broad way in different settings, 15 and one of the most widely used instruments is the Nurse Competence Scale (NCS) developed by Meretoja in 2003.16,17 The NCS is a structured instrument defining competence as a functional adequacy and capacity to integrate knowledge, skills, attitudes and values in specific contextual situations. 16 The theoretical framework is based on Benner’s (1984) work From Novice to Expert, and consists of 73 items, divided into seven categories Helping role (7 items), Teaching and coaching (16 items), Diagnostic functions (7 items), Therapeutic interventions (10 items), Ensuring quality (6 items), Manging situations (8 items) and Work role (19 items).16,18 The level of competence is measured with a visual analogue scale (VAS 0–100) and the frequency of the use of competencies with a four-point scale (0–3). The VAS corresponds to ≤ 25 low competence, 26–50 rather good competence, 51–75 good competence and 76–100 very good competence.16–18
Even though the NCS was developed to evaluate nurse competence in specialized care, there are clear indications that the instrument can be used in varying contexts and cultures and for evaluating the competence of both students and registered nurses in different stages of their careers. A systematic review has shown the value of the instrument, 17 but there is still a need to compare competence evaluations to fully understand the ontological and context-specific features of the competence and the variations of it. 19
Methods
Aim
This article aimed to describe how ontological and contextual competence becomes visible in evaluations done with the Nurse Competence Scale in different settings and in different stages of professional development, and further to consider how it could be used in nursing education and in planning further education for nurses.
Design
An integrated literature review was applied with a specific focus, including empirical and theoretical reports and diverse study methodologies. 20
Search methods, outcome and quality appraisal
The material for this article is taken from a total of 34 original studies published between January 2004 and April 2020. Twenty-three of the studies were found in a former review evaluating the psychometric value of the instrument, with a time frame from January 2004 to October 2015. 17 For this article, a further search using the same strategy was carried out in PubMed, CINAHL, SAGE, Science Direct and Google Scholar with the help of an information specialist. The search words used were NCS and Nurse Competence Scale and the time frame for this search was October 2015 to April 2020. All studies were peer-reviewed, full-text articles or dissertations and written in English or Nordic languages using a complete copyrighted NCS.
Inclusion criteria were that NCS measurements should contain all categories, and that the evaluation should be of nurses’ or nursing students’ competence. For this reason only 23/30 studies from the earlier review could be included. Two doctoral theses21,22 used the same sample as published articles23–25 and therefore only the articles were included in the analysis. Also, two articles18,26 used the same sample and were viewed as one. The search process is illustrated in Figure 1.
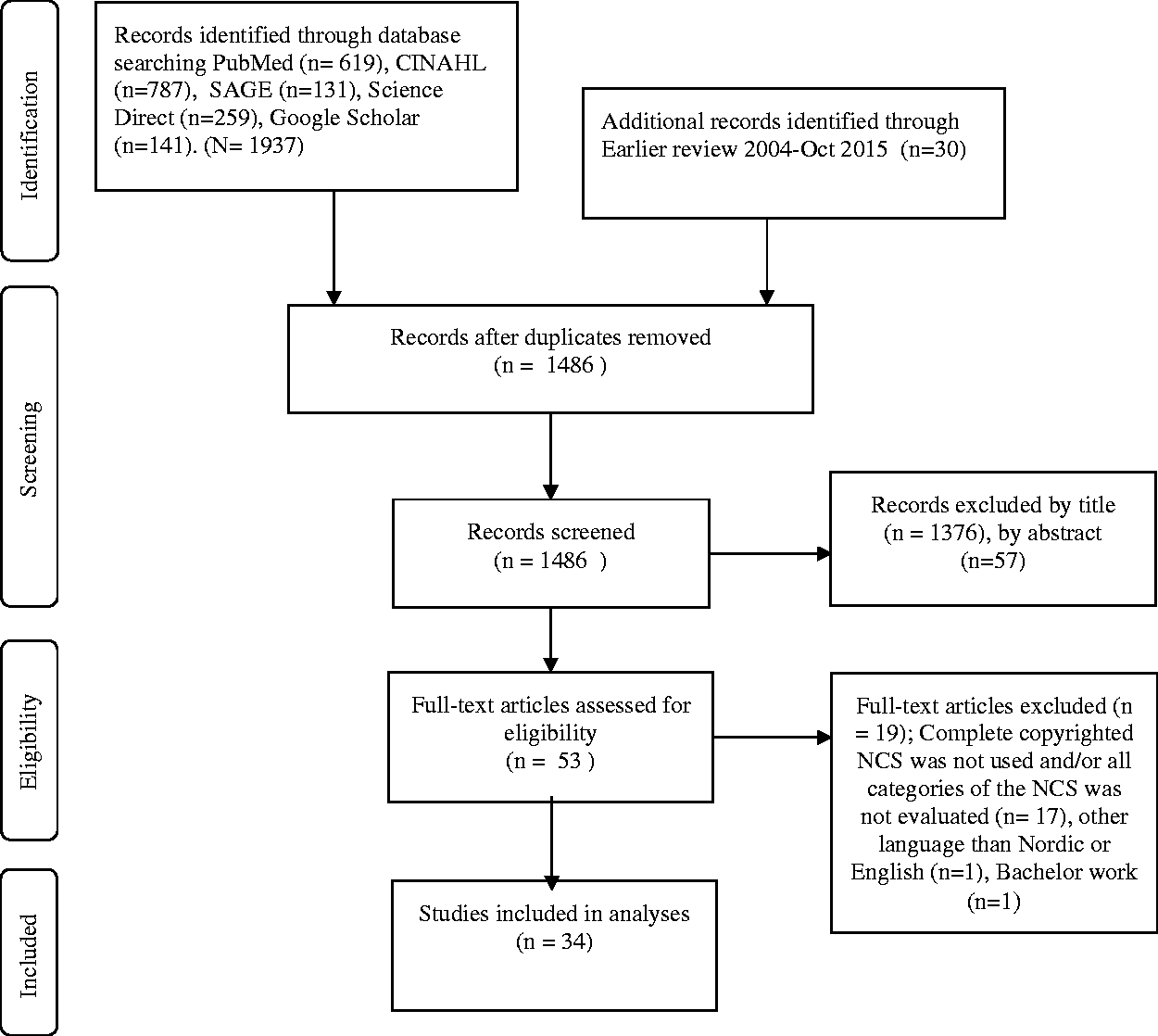
The PRSIMA flow diagram for the search and selection process. 27
The quality of the included studies was appraised independently by the two researchers using the JBI Critical Appraisal Checklist for Analytical Cross-Sectional Studies (n = 29), Cohort Studies (n = 2), Quasi Experimental Studies (n = 2) and RCT studies (n = 1). The methodological quality of the articles was mainly qualified (29 studies), four studies were rated as good and only one of the quasi-experimental studies, which lacked a control group, was rated as fair. 28
The studies are from Finland (n = 16), Australia (n = 3), Iran (n = 5), USA (n = 2), Italy (n = 3), Norway (n = 2), Lithuania (n = 1), Saudi Arabia (n = 1) and the United Arab Emirates (n = 1). They offer the views of registered nurses (RNs) (n = 29), which, in four studies is combined with the managers views, the views of nursing students (n = 5), and in one study in combination with the views of the students’ mentors. The studies and the result of the quality appraisal are presented in Table 1, where each study also has its reference number.
An overview of included articles and their appraised quality.
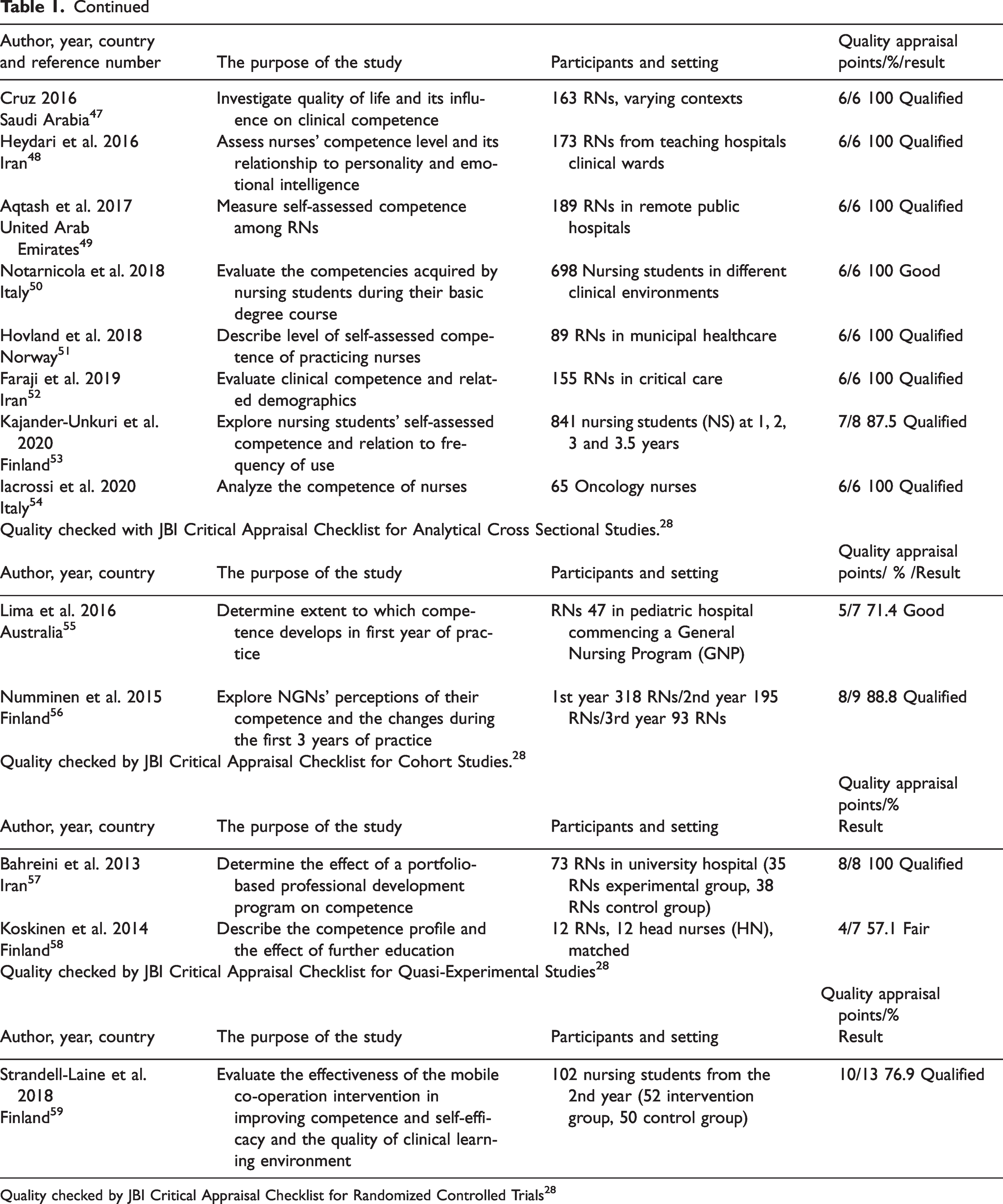
Quality checked by JBI Critical Appraisal Checklist for Randomized Controlled Trials 28
Analysis
The material being so heterogeneous the analysis was descriptive, inspired by Whittemore and Knafl’s way synthetizing data. 20 The first step was data extraction, data were displayed in tables (Tables 2–5) giving an overview of the main tendencies in the competence evaluations. Next a comparison of data was carried out, and the question why was posed. Explanations for the differences were considered. Finally, the contextual differences of experienced competence were highlighted and conclusions drawn. In the discussion, ontological and contextual features of the nursing competence were described during different stages of competence development and tied to the categories of the NCS instrument.
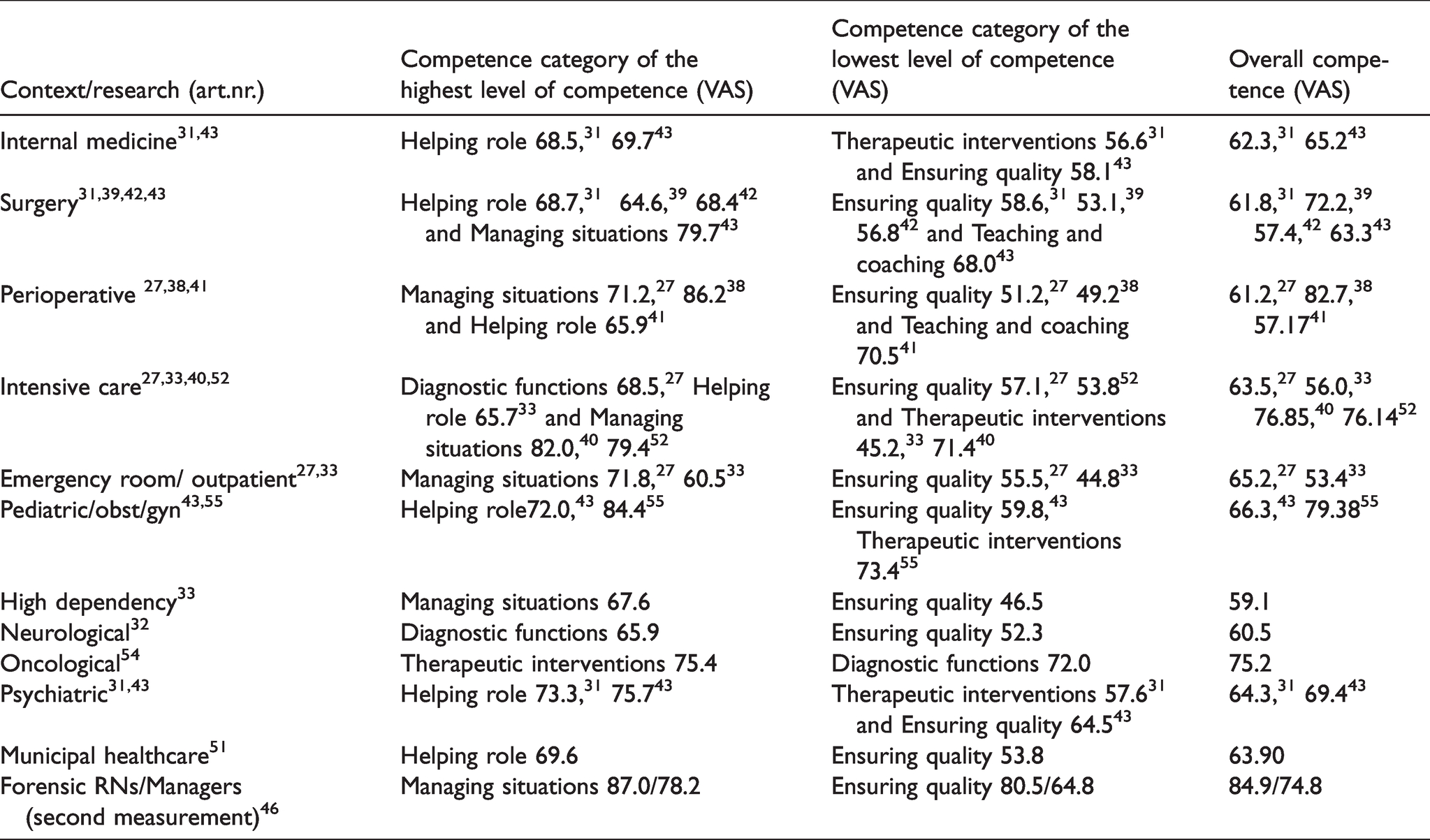
Nurses’ contextual competences levels expressed as visual analogue scale (VAS) means.
Competence evaluations made by nurses and their managers expressed in visual analogue score (VAS) means.

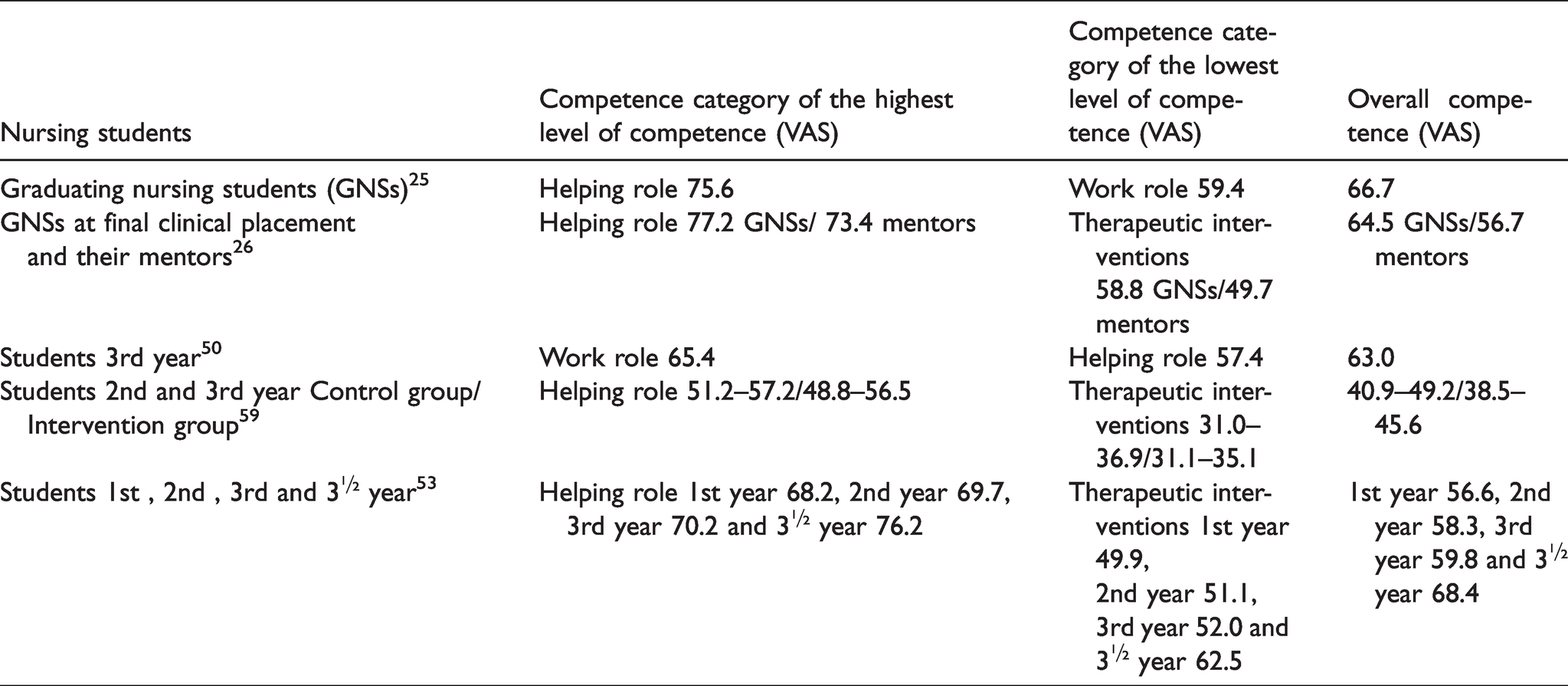
Nursing students’ competence levels expressed in visual analogue scale (VAS) means.
Newly graduated nurses’ (NGNs) competence levels expressed in visual analogue scale (VAS) means.
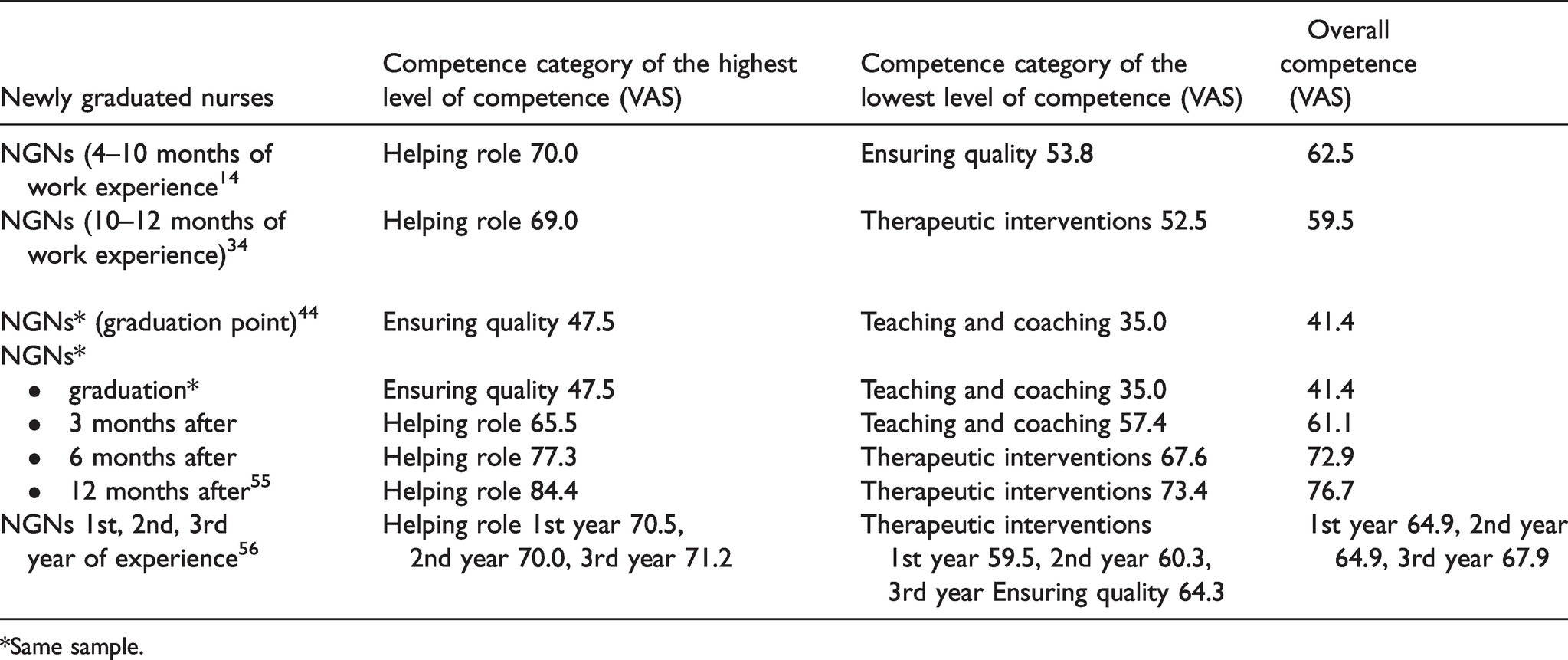
*Same sample.
Rigor and ethics
In this study the literature selected was scientifically relevant for the study and double-checked by both authors. The material has been ethically and properly handled, approached impartially and accounted for honestly. The work of other researchers has been taken into account and has been cited appropriately. 29
Results
Of the 34 studies, 20 described different nursing contexts, four of them offering the view of both nurses and nurse managers. Five studies considered the competence of newly graduated nurses, five the competence of nursing students, of which one also gave the view of the mentors. Different types of hospitals were compared in two studies, one study looked at the competence of three different nurse cohorts and one concentrated on instrument validation (Table 1).
Ontological competence
Ontological clinical competence puts emphasis on the core of nursing: caring. It constitutes the independent work of nurses, when still much of nursing is based on directions and medical orders. How to encounter patients, ethical conduct, responsibility and the will to help are what makes nursing what it is.5,15 Most studies using the NCS are conducted in specific contexts, but regardless of age, experience, education or context the ontological competence should be found, and data showed that all nurses considered themselves competent in the Helping role. In 21/34 studies the Helping role was rated highest. In only two studies the Helping role stayed on a rather good level (<50 VAS).44,59 In a study by Lima et al., one could see a significant increase of the competence level, the Helping role from 45.5 to 84.4 after 12 months of practice. 55 In 11 studies no attention was paid to which kind of wards the nurses worked in. In specific contexts, the Helping role rated the highest in medical, surgical, psychiatric and pediatric care, but was high in all contexts and highest in six of the studies,14,30,34,45,56,57 Managing situations rated high in four,36,37,47,48 and the Work role in one, 5 but even in these studies the Helping role was high (Table 2). Newly graduated nurses rated the Helping role highest.14,34,56
Both experienced nurses and newly graduated nurses mainly evaluated their competence in the Helping role from to be good14,25–27,30,31,34,41,42,45,46,51,53,56 to very good43,45,46,53,57 increasing with experience. In the experimental study, 59 at the start the students’ competence in the Helping role was on a rather good level in the intervention group, but increased to a good level after the intervention.
Contextual competence
Therapeutic interventions develop in context and were rated high in more specialized contexts such as in cancer care. 54 It was evaluated low by newly graduated nurses, as was Teaching and coaching.34,44
In different contexts, variations in the level of competence appeared and competence categories were given different levels of importance. The variations can be seen in Table 2.
In the context-specific studies, the overall competence was on a good level and even on a very good level in the operating theatre, 38 critical care,40,52 pediatrics, 55 cancer care 54 and forensic care. 46 The highest competence VAS means were found in both navy and civilian operating room nurses, 38 in critical care nurses 40 and in a forensic setting. 46
Managing situations, the Helping role and Diagnostic functions were highly rated in all contexts. In more technology dependent units Managing situations and Diagnostic functions got higher scores, while Teaching and coaching and Ensuring quality got low rates.38,40,41,57 In the neurological context Teaching and coaching, helping the patient to become independent was rated high. 32 A study by Bahreini et al 2011 36 showed that nurses felt most competent in Managing situations and Teaching and coaching, estimating their overall competence as very good, while in the study by Notarnicola et al., 50 the competence remained on a rather good level and nurses felt most competent in their Work role and in Ensuring quality. In the study by Bahreini et al., 36 46 of 190 of the nurses had less than two years’ work experience, but a bachelor’s, or a master’s degree.
Competence increases with experience,45,53,55,56 as shown in the study by Lima et al. 55 The overall competence increased from 41.4 to 76.7 (35.3 VAS points) in 12 months.
Nurses aged 40 years and above reached the highest mean VAS scores in all studies where age was considered. Competence increased in all categories and items except in using research evidence to develop care in the units. 56 Also, frequency of use correlated with the estimated level of competence,14,22–27,32,34,36,40,46,50,51 as did the possibilities to participate in further education, good nursing equipment, good leadership and support and permanent employment.26,36,37
The nurse managers seemed to evaluate the level of competence of nurses higher than the nurses themselves30,36,46 except in the study by Bahreini et al., 57 where the head nurses evaluated the nurses’ competence lower in every category (see Table 3).
Competence in early stages of professional development in nursing
Nursing students
The competence of nursing students reached a good level and highest VAS means were found in the Helping role, except in the study by Strandell-Laine et al. 59 where the overall competence of students remained on a rather good level, even after an intervention. The Helping role reached the level of good 59 (Table 4).
Most challenging for nursing students was the category of Therapeutic interventions, and the Work role. Comparing the mentors’ evaluations and the students’ self-evaluations, the students evaluated their competence on a higher level than the mentors did in every category. 26
Newly graduated nurses
Newly graduated nurses evaluated their competence as mainly good, and the overall competence varied between VAS mean 59.5 and 76.7 depending on time since graduation (Table 5).14,34,44,55,56
The Helping role had the highest VAS means in all studies, except in the study by Lima et al.44,55 where newly graduated nurses evaluated their competence level as lower than others in the beginning. The competence level increased after three months of practice, being highest 12 months after graduation. Teaching and coaching and Therapeutic interventions got low rates at the beginning of a nursing career but were improved to a good level after six months of practice.55,56
Discussion
The Nurse Competence Scale has shown its value for evaluating nursing competence. 17 Of 73 items in the NCS, 28 can be seen as focusing directly on the patient. Adding the four that have to do with the knowledge needed in situations with the patient, these form the ontological competence and become visible in the nurse–patient relation, encountering the patient individually, meeting his/her needs, supporting and following ethical values and developing a caring culture in the unit. 5 This core of nursing is independent of context, and is what makes nursing what it is. In the NCS, these items are found in the Helping role, and hence the studies showed students and newly graduated nurses evaluated the Helping role the highest in all included studies with one exception. 44
Nursing education should give the ontological base. Ethos and ethical standards are basic, and transferable into different contexts. 5 The other parts of the NCS focus on relevant parts of the nursing process as well as on developing the nursing culture, coaching other staff members and students, co-operation and quality ensuring, but are contextual. 26 Since all contexts have their specific features due to the different patients, diagnosis, treatments, equipment and structure of the ward, the contextual differences became evident, and the need for being familiar with the context affected the experience of competence. With growing competence, Managing situations and Therapeutic interventions developed and appeared very differently in the different contexts. This might lead to a situation where ontological competence disappears behind the contextual and outer factors take over. Nursing then becomes technicalities and tasks and the patient stays invisible. Still, in all contexts the Helping role got high scores suggesting that when the contextual competence increases, the ontological deepens.27,33,38,46
In different stages of students’ professional development or in the nursing career, different parts of the NCS are more relevant. In the beginning, students concentrate on helping one patient (Helping role) develop into helping more patients or tending to a whole ward. The Teaching and coaching role concerning patient education develops early, like diagnosing patients’ needs for care and support. Recognizing threats to the patient’s life, acting accordingly and planning the care of the patient are also basic competencies. These together with the Helping role form the ontological base, are independent of context and offer students and newly graduated nurses the experience of being clinically competent.
Therapeutic interventions require contextual awareness and co-ordination skills that develop during practice and use. The Teaching and coaching competence develops to include the co-ordination of patient education, educating family members, mentoring students and co-workers. Diagnostic functions develop into arranging expert help when needed and coaching others in using diagnostic equipment and interpreting results. Managing situations requires understanding of the resources available and mastering rapidly changing situations, skills that require experience. The Work role develops through self-evaluations and the evaluations of others showing the limitations of the competence. Independent acting develops alongside teamwork, but requires much experience before the student/nurse is ready to co-ordinate the patient’s overall care and to orchestrate the whole situation on a ward. Different contexts offer different challenges. 26
The students evaluated their competence generally as good, but students work under supervision and they are not taking care of the most critical and demanding patients on their own. The students’ competence was evaluated lower by mentors than by the students themselves. The base for evaluations differs. Mentors working in highly specialized environments often have excessively high expectations of the students, while the students’ abilities to fully grasp the responsibility of the profession are limited.25,60 Contextual evaluations often focus on demonstrated skills that usually require both training and experience.61,62 Evaluations are essential and the evaluator needs evaluation abilities, needs to understand the instrument, and to know what is expected in the context.15,63
Registered nurses evaluated their competence development quite in the same way as did the students. Moving from the stage of novice to expert requires age and experience, but both younger and more experienced nurses evaluated their competence as good. 26 Newly graduated nurses evaluated their competence on a high level,37,48,52 but they, as new workers, are often protected from the most critical and demanding nursing in the unit. 64 The highest level of competence was found in patient-related nursing tasks and ethical care and the lowest in developmental work and in use of evidence-based knowledge. 27 A contextual competence develops with age, experience and frequency of use,45,53,55,56 and shows in evaluations of Therapeutic interventions, Managing situations and Diagnostic functions. In the included studies, Managing situations was evaluated the highest in technology-dependent contexts, such as in operating rooms and emergency units. Factors influencing the experience of feeling competent were age, experience, participation in further education, good nursing equipment, good leadership and support and permanent employment.26,36,37 Also the quality of care was important for job satisfaction and feeling of competence,27–32 still Ensuring quality was the competence category getting most of the low VAS means, except in the study by Lima et al. 44 The items in this category are demanding, encompassing critically evaluating the units’ care philosophy, utilizing research findings to further develop patient care and making proposals for further development and research and require both knowledge and experience. 26
Due to contextual differences, specific instruments for specific contexts have been developed, such as the operating theater 9 and anesthetic care 7 and for specific skills as medical administration 65 and wound care. 66 Nursing managers seemed to have a good understanding of nursing work and if competence were to be evaluated on the basis of performance, there would be no differences in the evaluations between managers and nurses.
The regular use of the NCS seems to be a good instrument to follow up and evaluate both students’ and nurses’ competence, and could also be used to discover the needs for further education and to plan targeted education for nurses. It covers both ontological and contextual competence and can be used in both in nursing education and practice.
Limitations of the study
The study design is descriptive based on the heterogeneity of the material. We included only studies in Finnish and English, thus language bias could be an issue. The quality of included studies was determined by the researchers based on their subjective understanding. Despite the criteria used, caution is required when interpreting the quality assessments. The challenges in the analysis lay in the lack of insight into the different cultures, educational systems and contexts.
Conclusion
The Nurse Competence Scale evaluates what nurses do in a broad perspective and covers both ontological and contextual features of nursing competence. It is sensible for experiences in context as well as for educational issues. It is, however, important to consider different viewpoints in the evaluations, emphasizing the students’ or nurses’ competence development. Nursing education should provide students with more opportunities to learn ontological competence, contextual requirements are learnt more deeply in practice after graduation.
Repeated evaluations follow up the professional development and as the contextual competence develops, the ontological in the same extension should deepen. Emphasizing different parts of the NCS in different stages of the nursing career creates different competence profiles for students, newly graduated and experienced nurses. The competence profiles should be developed alongside the increase in competence and more of the demanding items from the categories should be added. Context-specific competence profiles could help to understand the specific requirements of each context and the need for further education.
The NCS covers the whole spectrum of nursing responsibilities, and the complexity of the items within each category varies from basic to demanding. This explains the results ‘flattening out’ being mainly on a good level. Variation between educational and healthcare systems and different cultures seemed not to influence the overall competence level.
Footnotes
Acknowledgements
Information specialist Marketta Fredriksson has helped in developing the search strategy and in performing the search for material. Professor Riitta Meretoja, responsible for creating the Nurse Competence Scale (NCS) initiated the study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.