
Abstract
Repositioning patients in bed to promote comfort and prevent impairments caused by continuously lying in a prone position is a task frequently performed by nurses and nursing assistants. Repositioning is a high-risk activity, frequently causing occupational injuries. These occupational injuries are attributed to excessive physical demands on nurses due to patients’ weight and awkward nurse postures. During repositioning, risk of injury can be lowered by reducing friction between the patient and the bed. Hence, certain friction-reducing devices have been developed to reduce the manual force required to move patients. Nevertheless, further research is needed to evaluate the potential effectiveness of these devices. Therefore, the aim of this review was to present current research about the risk factors, prevention strategies, and assistive devices that could reduce work-related musculoskeletal disorders caused by repositioning patients in bed.
Work-related musculoskeletal disorders (WMSD) are a major occupational health problem, affecting health care workers who provide direct patient care (Alexopoulos, Burdorf, & Kalokerinou, 2003; Ando et al., 2000; Bohdana, Waldemar, & Tadeusz, 2004; Goldman, Jarrard, Kim, Loomis, & Atkins, 2000; Khuder, Schaub, Bisesi, & Krabill, 1999; Nelson & Baptiste, 2004; Retsas & Pinikahana, 2000; Waters, Collins, Galinsky, & Caruso, 2006). For the past several decades, worldwide epidemiological studies have revealed a high incidence and prevalence of low back musculoskeletal complaints among nurses and nursing assistants (Alexopoulos et al., 2011; Menzel, 2004; Roffey, Wai, Bishop, Kwon, & Dagenais, 2010). Compared with other occupations, nurses and nursing assistive personnel are at the highest risk for back, neck, shoulder, wrist, and knee injuries (Hansen, Visack, & Pederson, 2004; Waters, 2008). Nursing assistants, orderlies, and attendants rank second while registered nurses rank sixth in a list of at-risk occupations for strains and sprains (U.S. Department of labor, Bureau of Labor Statistics, 2012). In Israel, a cross-sectional observational study revealed a 43.9 per 100 twelve-month prevalence rate of work-related low back pain (LBP) among nurses in a rehabilitation hospital (Alperovitch-Najenson, Treger, & Kalichman, 2013).
A growing body of evidence has demonstrated that WMSD among nurses are associated with patient-handling tasks (Alexopoulos et al., 2003; Alperovitch-Najenson et al., 2013; Pompeìì, Lipscomb, Schoenfisch, & Dement, 2009). Therefore, the aim of this review was to present current research about risk factors, prevention strategies, and assistive devices to reduce WMSD caused by repositioning patients in bed.
Method
PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Physiotherapy Evidence Data (PEDro), Institute for Scientific Information (ISI) Web of Science, and Google Scholar from database inception until December 2013 were searched using a predefined strategy. Keywords and phrases used in the online search included “work injuries,” “work related musculoskeletal disorders,” “work injury,” “low back pain,” “musculoskeletal,” “work loss,” “nurses,” “nursing aids,” “patient transfer,” “patient repositioning,” “patient-handling,” and combinations of them. Titles and abstracts of all articles were reviewed. Inclusion criteria included any type of publications about connections between WMSD, nurses, and patient repositioning in bed. Relevant papers of any methodological quality were included. All published materials in English were critically analyzed by the authors. Pertinent secondary references were also retrieved.
Results
Association Between Work-Related Musculoskeletal Disorders (WRMSD) and Repositioning Patients in Bed
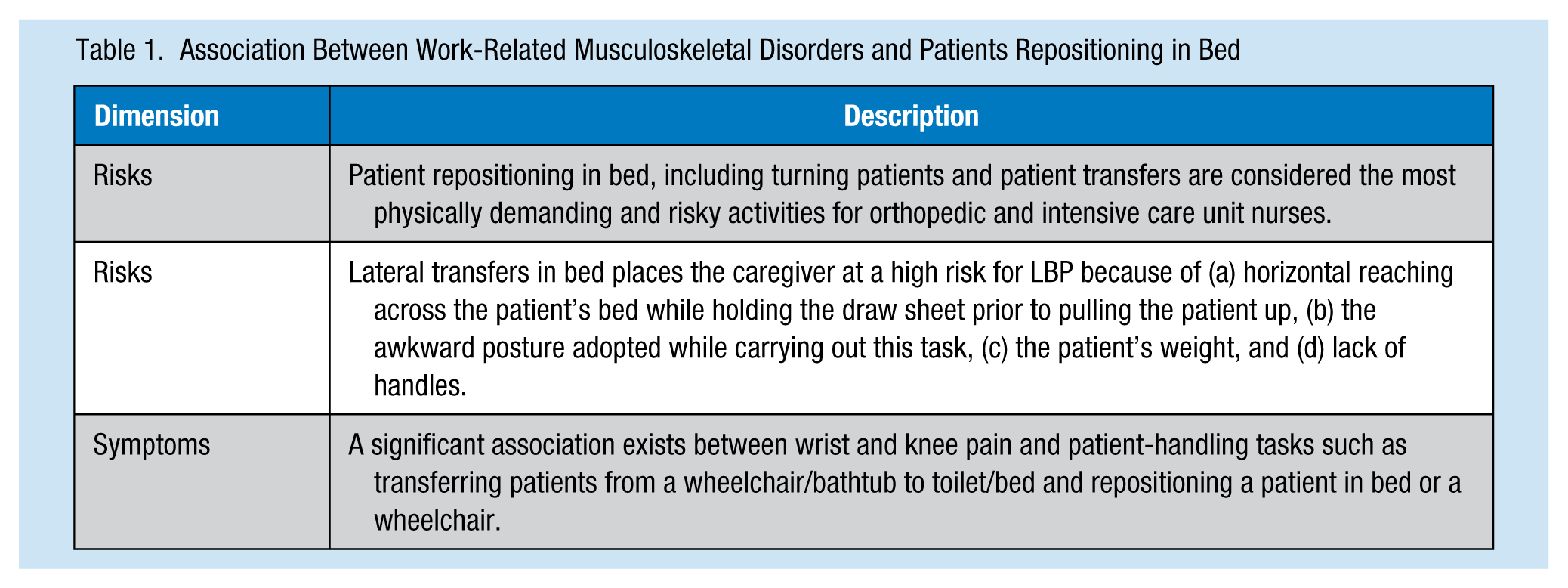
A cross-sectional study of 113 nursing staff members working in a veteran’s hospital in Tampa, Florida (Menzel, Brooks, Bernard, & Nelson, 2004), demonstrated a significant association between wrist and knee pain and patient-handling tasks such as transferring patients from wheelchairs or bathtub to toilet or bed and repositioning patients in bed or wheelchairs. Fragala and Bailey (2003) collected data from insurance records of seven hospitals in the northeastern United States during a 24-month period. Four of the top five activities contributing to worker injury were related to patient-handling tasks including repositioning patients in bed. Clinical experience and research have demonstrated that repositioning patients in bed is one of the highest risk activities for occupational injuries among health care workers (Fragala, Fragalg, & Bailey, 2005; Nelson, Menzel, & Gross, 2003; Peterson, Reno, Delia, & Isaacs, 2007; Schibye, Skotte, Hye-Knudsen, Faber Hansen, & Essendrop, 2000; U.S. Department of labor, Bureau of Labor Statistics, 2012; Waters, 2008). Pompeìì et al. (2009), at Duke University Medical Center, reviewed human resource data from 19,487 workers’ compensation claims over a 7-year period (1997-2003) to identify WMSD. Workers’ descriptions of their injuries were used to identify those injuries resulting from patient handling. The authors found that 32% of WMSD resulted from repositioning patients, pulling patients to an upright position in bed, and catching patients who fell.
A systematic review by Schlossmacher and Amaral (2012) showed that 9.1% of nurse-reported LBP was attributed to patient repositioning in bed. Vieira (2007) used a combined methodology (i.e., epidemiological reviews, questionnaires, qualitative analysis, functional capacity evaluations using direct measures of force, muscle activity, joint motion, and physical demand analyses using video-recording, photogrammetry, motion analysis, and spinal load estimation) to identify specific risks for work-related LBP associated with nursing tasks. The authors concluded that patient repositioning in bed (i.e., turning patients and patient transfers) is the most physically demanding and risky activity for orthopedic and intensive care unit nurses.
In a survey of staff nurses at a large tertiary care hospital, the task of lifting or pulling patients toward the head of the bed was reported most likely to cause LBP (Harber et al., 1985). Lifting or pulling patients up in bed was recognized as a high-frequency activity, actually the highest task frequency of all heavy, physically demanding tasks in a survey of staff nurses at a large tertiary care hospital in Athens, Greece (Vasihadou, Karvountzis, Soumilas, Roumehotis, & Theodospoulou, 2008). Lifting or pulling patients up in bed was reported to be the cause of back pain by 29% of the respondents.
Nelson and Baptiste (2004) summarized evidence from interventions designed to reduce caregiver injuries finding that turning patients in bed is performed frequently by nurses, placing caregivers at increased risk of injury. The authors identified repositioning patients in bed as one of 19 high-risk tasks. In rehabilitation/spinal cord injury units, repositioning patients in bed and vertical patient transfers were identified as high-risk tasks for LBP. The authors declared that lateral transfers place caregivers at high risk for LBP for several reasons: (a) horizontal reaching across the patient’s bed while holding the draw sheet prior to pulling the patient up in bed, (b) awkward postures while performing this task, (c) the patient’s weight, and (d) lack of handles.
Most studies of WMSD investigate patient lifts and transfers, even though these two nursing activities constitute only a small portion of all nursing tasks (Collins, Wolf, Bell, & Evanoff, 2004; Edlich et al., 2005; Gonzalez, Howe, Waters, & Nelson, 2009; Hart, 2006; Nelson & Baptiste, 2004; Owen, Keene, & Olson, 2002; Yip, 2001). Hodder, Holms, and Keir (2010) recorded work tasks of health care professionals who care for long-term hospitalized patients by observing 20 nurses throughout an 8-hr work shift and recording the duration of each performed task. They reported that patient lifts and transfers accounted for less than 4% of shift time; patient care and miscellaneous tasks (i.e., bathing, feeding, and dressing; pushing, moving, or walking patients) accounted for 85% of shift time. In contrast, turning patients in bed and pulling patients toward the head of the bed are frequently performed tasks (Fragala, 2011; Nelson & Baptiste, 2004).
One of the repositioning tasks frequently repeated over the course of a workday is pulling patients toward the head of the bed (Fragala, 2011). McCoskey (2007) conducted a survey of 175 nurses aimed at evaluating patient-handling demands on military hospital units during a 24-hour period. Levels of discomfort, physiological effects, and productivity were measured. The results demonstrated that lateral transfers and repositioning of patients in bed were more than twice as frequent as other transfers. Most of the transfers (e.g., repositioning in bed, turning in bed, moving the patient to the head of the bed, and transferring patients from bed to bed) were rated by staff members as requiring great exertion.
In conclusion, it can be stated with high confidence that repositioning and pulling patients up in bed are frequent tasks, conducted in different facility departments, constituting significant risk for WMSD among nurses and nursing assistants. A crucial need exists to understand the precise ways in which these tasks cause injury (Table 1).
Association Between Work-Related Musculoskeletal Disorders and Patients Repositioning in Bed
Risk Factors for WMSD During Patient Repositioning in Bed
In health care, the word “repositioning” refers to body repositioning or reposturing including manual handling and transporting or supporting a load (i.e., lifting, lowering, pushing, pulling, carrying, or moving) by using hands or bodily force. When repositioning patients in bed, assistance is needed to move patients who have difficulty moving themselves (e.g., unconscious patients during basic tasks such as moving in bed or turning, health-related treatments in bed). Repositioning reduces the risk of developing secondary complications from bed rest (e.g., pulmonary embolus, deep vein thrombosis, or respiratory infections). Repositioning patients can also maximize the benefit of other interventions such as suctioning or hygiene (Dougherty & Lister, 2011; Taylor, Lollis, & Limone, 2001).
Bohdana et al. (2004), in a systematic review of 31 studies, found that both physical and psychosocial work-related factors can increase the risk of musculoskeletal injuries among nurses. However, the etiologic mechanisms are still poorly understood, and the reported evidence of a relationship between psychosocial factors and musculoskeletal disorders are not consistent.
Marras, Davis, Heaney, Maronitis, and Allread (2000) evaluated the effects of psychosocial stress on muscle activity and spinal loading in a laboratory setting. Twenty-five study participants performed sagittally symmetric lifts under stressful and non-stressful conditions. Trunk kinematics, torso kinetics, electromyography (EMG) activities of 10 trunk muscles, and peak spinal loads were measured. A personality inventory, anxiety inventories, and blood pressure measured the participants’ psychosocial reaction to stress. The authors found that psychosocial stress may manifest itself by increasing muscle activity only during low physical demands. However, during high demand, the physical requirements imposed may negate any stress-induced increase in activity. The authors hypothesized that the effect of psychosocial stress could be more prominent during low physical demand activities than the biomechanical demand with heavier loads.
Nurses experience higher physical workloads with higher patient acuity and shorter hospital stays resulting in patients’ greater dependence on nurses for assistance. During the course of most severe illnesses, patients may lose the ability to ambulate on their own and require assistance for repositioning and movement, which in turn becomes the nurse’s responsibility. Patients are repositioned to prevent pressure ulcers, blood clots, and pneumonia and promote comfort and circulation (Collins & Menzel, 2006). Furthermore, it is common for patients to slide down from the head of the bed, requiring assistance to regain their position in bed (Fragala et al., 2005). Manual repositioning, which requires high physical demands due to excessive patient weight and awkward postures (e.g., leaning over the bed or working in confined space), is associated with increased risk of pain and injury, particularly to caregivers’ backs (Fragala, 2011; Nelson, Fragala, & Menzel, 2003; Nelson, Owen, Lloyd, et al., 2003; U.S. Department of Labor, Occupational Safety and Health Administration, 2003).
The Influence of Assistive Devices and Methods for Reducing WMSD
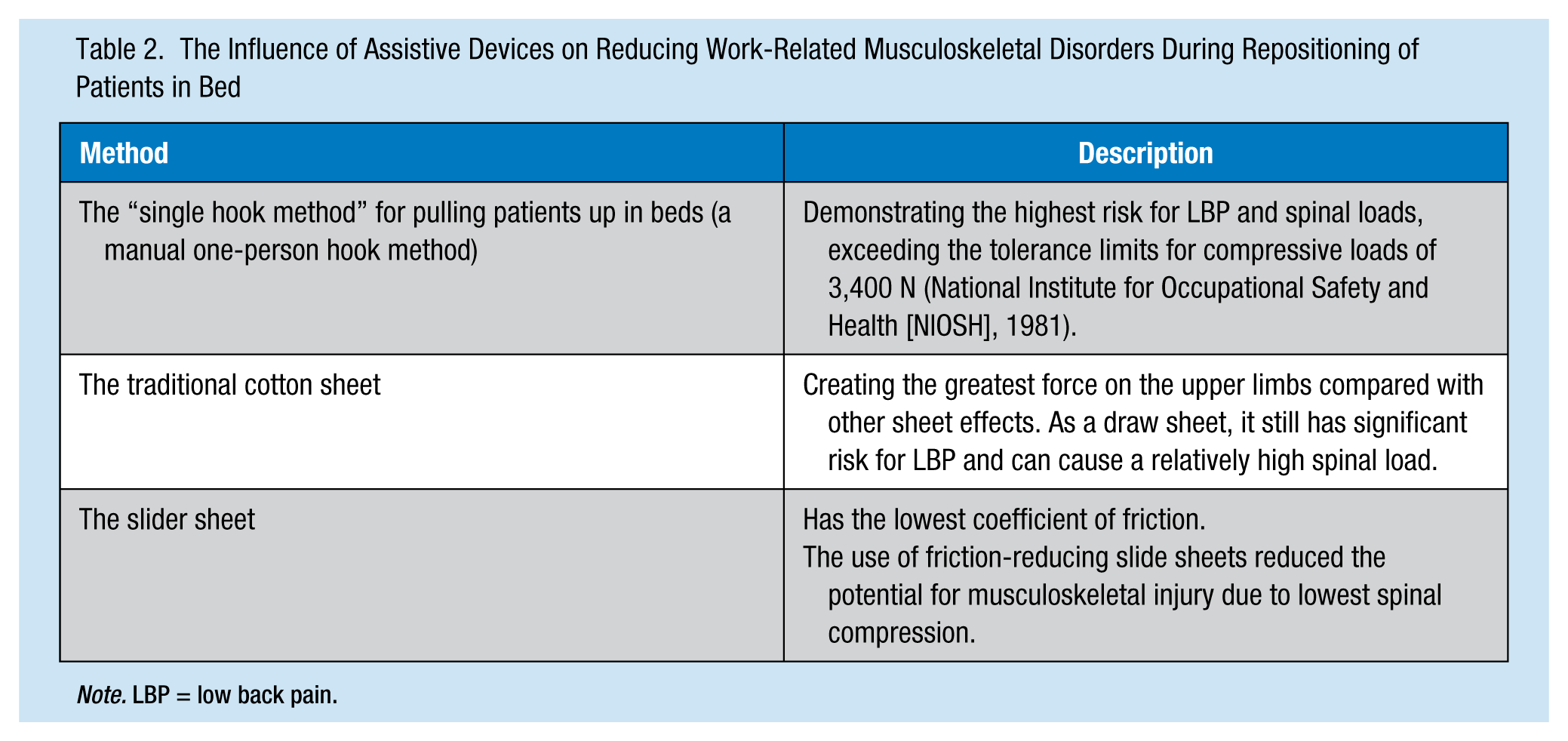
Various ergonomic devices have been developed during the past several years to reduce the mechanical load during patient-handling activities, thereby preventing the occurrence of back injury (Table 2). Skotte and Fallentin (2008) investigated low back load during repositioning of patients in bed and assessed the influence of patients’ weight and disability on back load. In a laboratory, they examined six patient-handling tasks (i.e., turning, transversal repositioning, head elevation, lying to sitting, sitting to lying, pulling toward the head of the bed). The patients were divided into weight groups (i.e., light, 59 kg; medium, 83 kg; heavy, 110 kg) and handicap groups (i.e., hemiplegia, paraplegia, near paralysis). The tasks were performed with the optional use of simple, low-tech assistive devices (i.e., draw sheet, slide sheet, plastic bags [decrease friction], and foam rubber cloth mats [increasing the friction between the feet and bed]). To determine the torque at caregivers’ L4/L5 joint, the researchers used a dynamic 3-D biomechanical model of the lower part of the body by measuring the Ground Reaction Forces (GRF) of health care workers by means of four force platforms. GRF of the bed was measured when health care workers pressed their legs against the bed. Analogue data were collected from videotapes of the experiments using five cameras. The results of this study confirmed that most repositioning tasks frequently exceeded the National Institute for Occupational Safety and Health (NIOSH) action level of 3,400 N, with 25% labeled high risk. Furthermore, weight, type of disability, and method (i.e., technique or assistive devices) used by these workers had a significant influence on low back loading.
The Influence of Assistive Devices on Reducing Work-Related Musculoskeletal Disorders During Repositioning of Patients in Bed
Note. LBP = low back pain.
Marras, Davis, Kirking, and Bertche (1999) found that specific techniques used by health care workers to move patients in bed reduced the risk of LBP. The aim of the study was to quantify the risk of specific tasks on patient handlers. Seventeen health care workers were evaluated for LBP risk while repositioning several patients. The risk of LBP was evaluated using a low-back disorder risk model (i.e., maximum sagittal flexion position, lift rate, maximum external moment, maximum lateral velocity, and average twisting velocity) and biomechanical spinal loading evaluated by an EMG. The results showed various repositioning techniques created significant risk for LBP. The single hook method, used by one worker standing beside the bed holding the patient under the shoulder by the elbow joint while moving the patient up in bed, created the highest risk for LBP and spinal loads, exceeding the tolerance limits for compressive loads of 3,400 N (NIOSH, 1981). The two-person draw sheet technique had the lowest, but still significant, risk for LBP and could cause a relatively high spinal load.
Theou et al. (2011) used a portable surface EMG, a Borg Rating of Perceived Exertion scale, and coefficient of friction to compare the physical and physiological measures of muscle activity between a new slider sheet system and traditional hospital bed sheets. Two patient transfer movements were used: boost and turn a female volunteer, weighing 51 kg. The findings revealed a greater number of burses and longer duration muscle contraction in the EMG data and greater perceived exertion on the Borg rating scale during both repositioning movements on the traditional bed compared with the slider sheet system. Furthermore, the slider sheet device had the lowest coefficient of friction.
Bartnik and Rice (2013) investigated the forces required for moving a patient up in bed using a variety of friction-reducing slide sheets. The authors used a 3-D motion capture system with four cameras to evaluate the sheer force on the lumbar region in addition to force gauges to estimate the hand force while moving a patient up in bed. Two types of slide sheets (e.g., perishable for single patient use and washable for multiple patients use) and a traditional cotton sheet were used. The results suggested that the use of friction-reducing slide sheets reduced the potential for musculoskeletal injury among caregivers compared with traditional cotton sheets due to lower spinal compression. Furthermore, traditional cotton sheets created the greatest force on caregivers’ hands among all three sheet types.
Fragala et al. (2005) demonstrated in a survey of 459 caregivers in 12 hospitals that caregivers required mechanized assistance for pulling patients up and repositioning them in bed. These authors also provided additional data supporting the perception that direct caregivers in hospitals must frequently reposition clients for whom they care. Knowing that most repositioning tasks frequently exceed the NIOSH action level of 3,400 N with 25% at high risk (Skotte & Fallentin, 2008), evaluation of patient repositioning techniques and devices, meant to reduce caregivers’ occupational injury risk, is needed.
Additional Research Opportunities
Worker transfer techniques remain a critical determinant of back load. Nursing staff should be educated about the effectiveness of sliding devices when manually transferring patients (McGill & Kavcic, 2005). Strategies to prevent or minimize injuries associated with patient handling are often based more on tradition and personal experience than scientific evidence (Nelson & Baptiste, 2006).
In Koppelaar, Knibbe, Miedema, and Burdorf’s (2012) study on the influence of ergonomic devices on mechanical load during patient handling, caregivers used slide sheets for repositioning patients in bed in only 14% of these situations. The authors attributed this finding to organizational and individual factors, which might have influenced the minimal use of slide sheets, such as lack of time, availability, and knowledge. Caregivers should use appropriate mechanical devices when caring for patients to prevent potential injuries for both patients and caregivers (Gonzalez et al., 2009). The goal of ergonomics is to design an efficient workplace and safe work tasks with appropriate equipment enabling workers to achieve high productivity and efficiency (Spratt et al., 2012). Unfortunately, little consensus exists as to which ergonomic interventions or workplace designs are best for patients and nurses.
Several studies have supported the use of slide sheets for repositioning patients in bed as part of injury prevention programs (Bartnik & Rice, 2013; Fragala et al., 2005; Marras et al., 1999; Skotte & Fallentin, 2008; Theou et al., 2011). Despite these findings, slide sheets have significant disadvantages including the inconvenience of additional layers on bedding, a tendency for slide sheets to wrinkle under patients, and slide sheets being overly slippery for certain patients (Filek, Leach-Macleod, Brims, Binsted, & Jakobi, 2010).
Maneuvering forces required to reposition patients in bed were found to be significantly different when using mechanical devices, perhaps due to the design of these devices. Thus, assistive devices may need additional improvements (Bartnik & Rice, 2013; Zhuang, Stobbe, Hsiao, Collins, & Hobbs, 1999). Despite the importance of these devices in improving nurse safety when repositioning patients in bed, their actual application has not been adequately studied (Peterson et al., 2007; Skotte & Fallentin, 2008).
Conclusion
WMSD are a major occupational health problem affecting nurses and nursing assistants who provide direct patient care. Compared with other occupational groups, nursing assistants, orderlies, and attendants ranked second, and registered nurses sixth, on a list of at-risk occupations for strains and sprains.
Most WMSD studies focused on patient lifting and transfers, even though these two nursing activities constitute only a small portion of all nursing tasks. In contrast, repositioning patients in bed is a task frequently performed by nurses and nursing assistants, placing caregivers at increased risk of injury.
Occupational health nurses need to better understand the precise risk of injury and develop prevention strategies to reduce WMSD caused by repositioning patients in bed. It has been confirmed that the methods (e.g., technique/assistive devices) used by nursing personnel have a significant influence on low back loading while repositioning patients in bed. Despite this knowledge, strategies to prevent or minimize injuries associated with patient handling are often based on tradition and personal experience rather than scientific evidence.
A number of studies have recommended using slide sheets as part of an injury prevention intervention for repositioning patients in bed; however, significant hindrances to their use have been identified. Despite the potential positive effect of assistive devices for safe repositioning of patients in bed, their actual effect on nursing staff and patients has not been adequately studied. Future research should focus on which devices to use in particular situations, and resulting patient and nurse outcomes.
In Summary
Repositioning patients in bed is a task frequently performed by nurses and nursing assistants. It is an activity, frequently causing occupational injuries, attributed to excessive physical demands on nurses due to patients’ weight and awkward nurse postures. This risk of injury can be lowered by reducing friction between the patient and the bed, during repositioning the patient. Hence, certain friction-reducing devices have been developed to reduce the manual force required to move patients. Further research is needed to evaluate the potential effectiveness of these devices.
Footnotes
Acknowledgements
The authors thank Mrs. Phyllis Curchack Kornspan for her editorial services.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Chava Weiner is the director of the Zeide School of Nursing, Bnai-Zion Medical Center, Haifa, Israel.
Deborah Alperovitch-Najenson is a lecturer in the Department of Environmental and Occupational Health, School of Public Health, Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel, and in the Department of Physical Therapy, Recanati School for Community Health Professions, Faculty of Health Sciences at Ben-Gurion University of the Negev, Beer-Sheva, Israel.
Joseph Ribak is a professor at the Department of Occupational and Environmental Health, School of Public Health. Sackler School of Medicine, Tel Aviv University, Tel Aviv Israel.
Leonid Kalichman is the head of the Master’s Degree Program, Department of Physical Therapy, Recanati School for Community Health Professions, Faculty of Health Sciences at Ben-Gurion University of the Negev, Beer-Sheva, Israel.