
Abstract
Work-related musculoskeletal disorders (WMSD) are a major safety concern in today’s health care environment due to the manual lifting of patients with higher acuity levels and obesity. Nurses move patients multiple times each day, incurring cumulative stress and trauma resulting in chronic pain and potential injury. The purpose of this study was to assess barriers to the use of assistive devices in safe patient handling and mobility (SPHM) that contribute to WMSD in health care workers. Interpersonal, situational, organizational, and environmental influences have both direct and indirect effects on workers’ commitment to use, or their actual likelihood of using, assistive devices. This study confirmed that time constraints contribute to fewer instances of assistive device use. Comprehensive ergonomic programs are needed to promote staff and patient safety. By providing safe environments for health care workers who engage in patient handling and mobility, the risk of injury can be significantly reduced.
Keywords
Registered nurses rank fifth in their incidence of work-related musculoskeletal disorders (WMSD) and nurses’ aides rank second, reporting more serious WMSD than workers in any other occupation. In 2011, hospitals reported 16,680 injuries that resulted in missed work. These injuries were mainly due to manual lifting of patients who now have higher acuity levels and weigh more. Challenges in transferring, repositioning, or lifting patients include variations in body size, physical disabilities, impaired cognitive function, varying levels of cooperation, and fluctuations in health-related conditions (Krill, Staffileno, & Raven, 2011). Patients are hospitalized for shorter periods, putting heavy emphasis on early mobilization despite being more dependent on others for physical assistance (Mayeda-Letourneau, 2013). These issues, combined with an aging health care workforce, demand a more rigorous approach to safe patient handling.
According to the Occupational Safety and Health Administration (2014a) in 2010, WMSD accounted for more than 600,000 injuries and illnesses among health care workers, costing employers nearly US$20 billion in direct costs (e.g., workers’ compensation [WC], health care expenses, legal services) and approximately 5 times that sum in indirect costs (e.g., pain and suffering, training for replacement employees, accident investigation, and lost productivity). Nurses (i.e., registered nurses, licensed practical/vocational nurses, and nurses’ aides) move patients multiple times each day; a nurse moves an estimated 3,600 pounds per shift (American Nurses Association, 2015). Over time, cumulative stress and trauma can affect their shoulders, backs, and joints resulting in chronic pain and potential injuries that can end their careers.
Background
Over a 12-year period (2003-2015), WC claims for patient-handling injuries increased by 43% in a 450-bed regional medical center in Virginia. In 2004, a large supply of mechanical lift equipment was purchased and supplemented with coach/super-user education by the vendor. However, the sustainment package to continue education and coaching was not purchased. Over the next 2 years, the number of WC claims increased 30% and 14%, respectively. From 2007 to 2013, the average number of claims rose 7% per year, including a 22% increase in 2010. From 2013 to 2014, an 11% increase in WC claims and a 98% increase in lost work time were related to patient-handling injuries. Of the total WC claim costs, 27% were attributed to strains, and 70% of strain injuries were to the lower back or shoulder. The majority of injuries were incurred by nurses (42%) and nurse’s aides (16%; Hartford Health Insurance, 2015).
Purpose and Hypothesis
This study assessed barriers to the use of assistive devices in safe patient handling and mobility (SPHM) that contribute to health care worker injuries. By identifying and reducing or eliminating these barriers, health care workers may be more likely to use assistive devices and prevent occupational injuries. Individual characteristics and experiences, behavior-related cognitions (i.e., perceived benefits and barriers, perceived self-efficacy (PSE), interpersonal and situational influences), and competing demands (i.e., independent variables [IDV]) have direct and indirect effects on workers’ commitment to use, or their actual likelihood of using, assistive devices in SPHM (dependent variable [DV]).
Review of Literature
Research supports the belief that manually lifting patients is extremely hazardous to health care workers (Anderson et al., 2014; de Castro, Hagan, & Nelson, 2006; Hudson, 2005; Mayeda-Letourneau, 2013). Nursing schools teach “body mechanics” for safe patient handling, and nurses are told that “if they lift properly, they won’t get hurt” (HCPRO.com, 2014; Waters, Collins, Galinsky, & Caruso, 2006). However, researchers have found that training in proper body mechanics does not prevent, and frequently causes, WMSD over time due to the long-term, cumulative effects of repeated high-risk patient-handling tasks (Charney, 2003; Edlich, Winters, Hudson, Britt, & Long, 2004; Mayeda-Letourneau, 2013). Traditional body mechanics includes neutral posture, leg muscles, and keeping the patient close to the worker’s body; these principles are intended for workers moving and lifting objects, not patients. Health care workers are frequently required to reach across beds, unable to use their leg muscles to move or turn patients (Wardell, 2007). Also, these workers are exposed to awkward positions (e.g., twisting) and patients with higher levels of acuity who are obese, agitated, or in pain often inadvertently contributing to workers’ risk of injury (de Castro, 2004). The recommended weight limit for lifting is 20.7 kg (46 lb). Despite this recommendation, nurses are lifting or transferring 100 kg to 135 kg (220 lb-300 lb) patients day after day, resulting in direct WMSD or cumulative muscle strain that could eventually lead to WMSD (Brown, 2003; Waters et al., 2006).
Use of mechanical lift equipment reduces the risk of WMSD due to patient handling. Biomechanical and lift intervention studies show significant reductions in biomechanical stress, musculoskeletal pain, injury rates, WC claims, and patient comfort when mechanical lifts are used to move patients (Edlich et al., 2004; Engst, Chhokar, Miller, Tate, & Yassi, 2005; Evanoff, Wolf, Aton, Canos, & Collins, 2003; Li, Wolf, & Evanoff, 2004; Zhuang, Stobbe, Collins, Hsiao, & Hobbs, 2000). According to Anderson et al. (2014), U.S. and Australian studies have reported up to a 44% reduction in WC claims after the implementation of assistive devices and “no-lift” policies.
An essential step in implementing a health care ergonomic program is the identification of barriers to changing work practices. Numerous studies have identified individual factors (i.e., lack of perceived need, lack of knowledge) and organizational factors (i.e., limited staffing, lack of appropriate policies, lack of equipment, room congestion, lack of management support) that hinder program implementation (Holman, Ellison, Maghsoodloo, & Thomas, 2009; Koppelaar, Knibbe, Miedema, & Burdorf, 2011; Wardell, 2007). Perceived time constraints are another barrier to mechanical lift use. According to Zhuang et al. (2000), the extra time needed to use lift equipment functionally offsets the decreased fatigue and patient and employee safety that results from lift use.
The National Institute for Occupational Safety and Health (NIOSH) conducted several studies related to best practices for safe patient handling. One study evaluated a multifaceted intervention program that included lift equipment, a safe lifting policy, and training for nursing care units. The results showed a 62% decrease in WMSD, an 86% and 64% decrease in lost work time and restricted days, respectively, and an 84% decrease in WC claim costs. The initial investment and training costs were recovered in less than 3 years. Intangible benefits included improved patient safety and comfort, less back soreness and end-of-shift fatigue for staff, and pregnant and older workers were able to work longer in the pregnancy or before retiring, respectively (Waters et al., 2006).
Best WMSD-prevention program practices are based on a multidimensional approach which includes lift equipment, “no-lift” policies, education, ergonomic risk assessments, and peer safety coaches (Anderson et al., 2014; Collins, Wolf, Bell, & Evanoff, 2004; de Castro et al., 2006) who provide expertise and support to coworkers during SPHM activities. Also, The Joint Commission (TJC) emphasizes the importance of an organizational culture of safety for both patients and health care workers (TJC, 2012). According to White (2010), the option of lift teams was shown to decrease the incidence of injuries, but these teams are expensive and not always available. Therefore, the consistent use of mechanical lift equipment is a more reasonable option.
Nurses are at risk of WMSD when handling and ambulating patients. Reduction or elimination of barriers to the use of assistive devices and mechanical lifts is essential in reducing employee injuries that result in WC claims. By providing a safe environment for health care workers who are responsible for patient handling and mobility, the risk of occupational injuries can be significantly reduced. Personal issues (e.g., time away from work and restricted duty to recover from injuries, possibly less income, and physical and emotional distress) can be avoided. Organizational concerns (e.g., staffing issues, lack of assessment tools, and availability and access to assistive devices) can be addressed and corrected to establish and maintain a culture of safety which is significant for employees and patients. Providing assistive devices and lifts that are readily available, mandatory ongoing safety education, “no-lift” policies, and a culture that supports and encourages equipment use are essential steps to program success. The investment in assistive devices and lift equipment will be offset by savings from fewer and less costly WC claims and lost productivity as well as adverse patient events.
Theoretical Framework
The theoretical framework for this study was the Health Promotion Model (HPM; Figure 1). The model identifies multiple health behavior influences and describes health as an evolving life experience requiring constant adjustments to maintain structural integrity and harmony with the environment (Pender, 2011). Pender’s model explains factors that influence health-promoting behaviors and well-being (Polit & Beck, 2012) and acknowledges the multidimensional nature of individuals as they interact with the environment to pursue health in unique ways. The HPM explains how three groups of factors (i.e., individual characteristics and experiences, behavior-specific cognitions and affect, and behavioral outcomes) have direct and indirect influences on health-promoting behaviors (Pender, 2011).
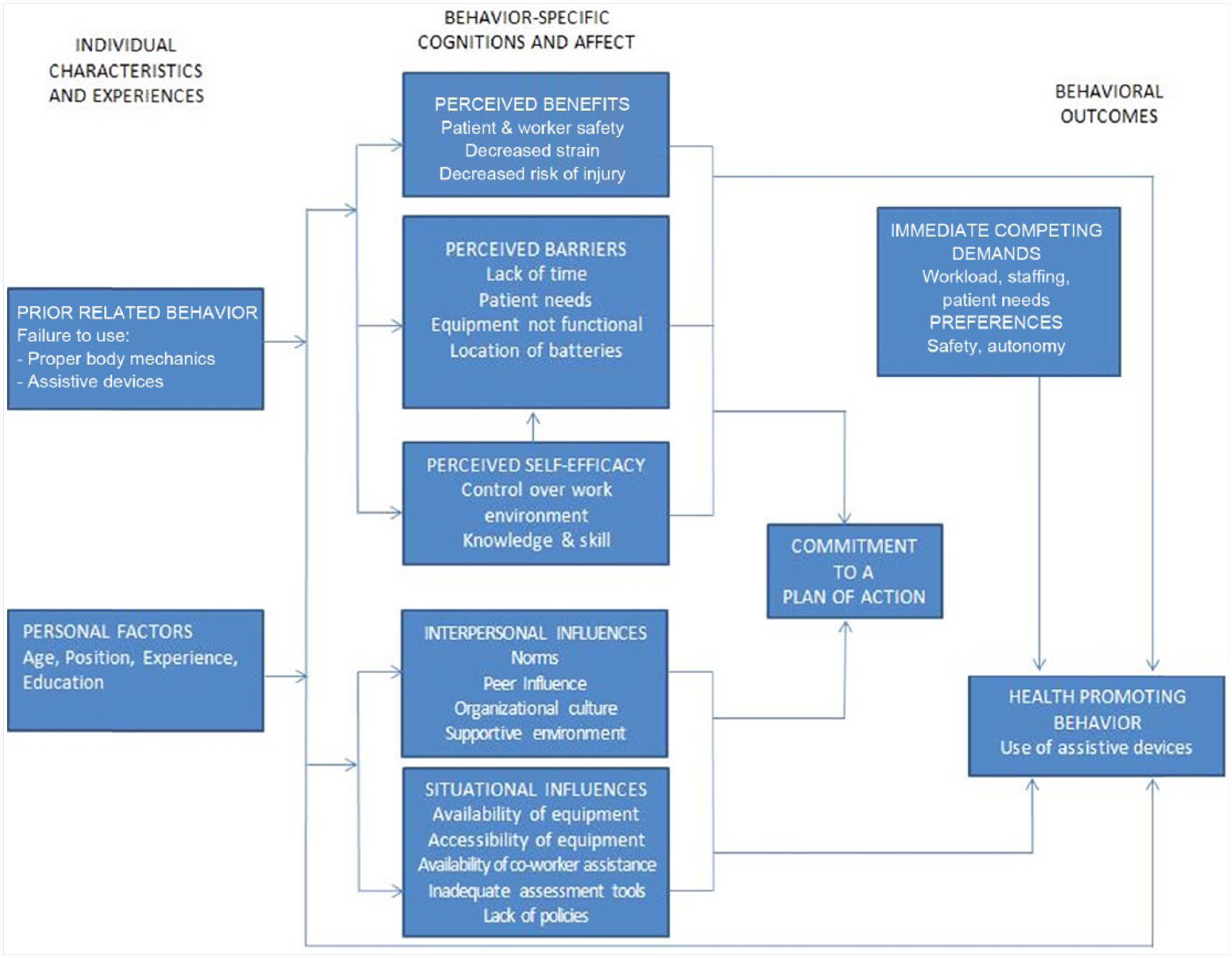
Application of Pender’s health promotion model.
Behavior and personal factors influence beliefs about and performance of health-promoting behaviors (e.g., the use of assistive devices in SPHM). Individuals commit to healthy behaviors based on their perceived benefits (e.g., safety, fewer muscle strains, reduced or eliminated risk of injury), whereas barriers (e.g., lack of PSE, interpersonal and situational influences (II/SI), and intermediate competing demands [ICD]) can constrain commitment to action and prevent health-promoting behavior.
To apply the model to this study, it was first necessary to identify perceived barriers and frequency of assistive device use. Sustained health-promoting behaviors are more likely to occur when barriers are addressed and a strong commitment to a plan of action is exhibited (Current Nursing, 2012; Polit & Beck, 2012, p. 128, 135). Ultimately, adopting health-promoting behaviors is the desired quality outcome of patient care and desired behavioral outcome to improve patients’ well-being
Method
A quantitative design using both descriptive and correlational methods was used to explore the relationships between perceived barriers to the use of assistive devices (IDV) and the frequency of assistive device use in SPHM (DV). One facility, a 450-bed acute-care trauma hospital, was the site for this study. Ten years ago, the facility invested in mechanical lift devices and education, but the accompanying educational program was not sustained, making the facility an ideal setting for this study. Despite the availability of assistive devices, they were rarely used.
The survey instrument was developed by the research team to evaluate factors that influenced nursing staff decisions to use assistive devices in patient handling and mobility. Items were selected from questionnaires used in prior studies that specifically addressed the research questions in this study (Anderson et al., 2014; Evanoff et al., 2003; Holman et al., 2009; Koppelaar et al., 2011; Miner, Laramie, & Davis, 2013; Silverstein, Howard, Cullen, Lee, & Goggins, 2005; Wardell, 2007). A 5-point Likert-type scale assessed agreement (i.e., 1 [strongly disagree] to 5 [strongly agree]) and frequency (i.e., 1 [never] to 5 [always]) with instrument statements. Nursing peers completed the survey and provided feedback regarding relevance and appropriateness of survey items to establish content and construct validity. These recommendations were evaluated and the survey was revised accordingly.
Three emails, which included an explanation of the study and Survey Monkey access, were sent at 1-week intervals to a potential pool of 353 nursing staff assigned to inpatient units and directly involved with patient handling and mobility. A total of 107 (30%) surveys were returned and included in the final analysis. Participant demographics are shown in Table 1.
Demographics.
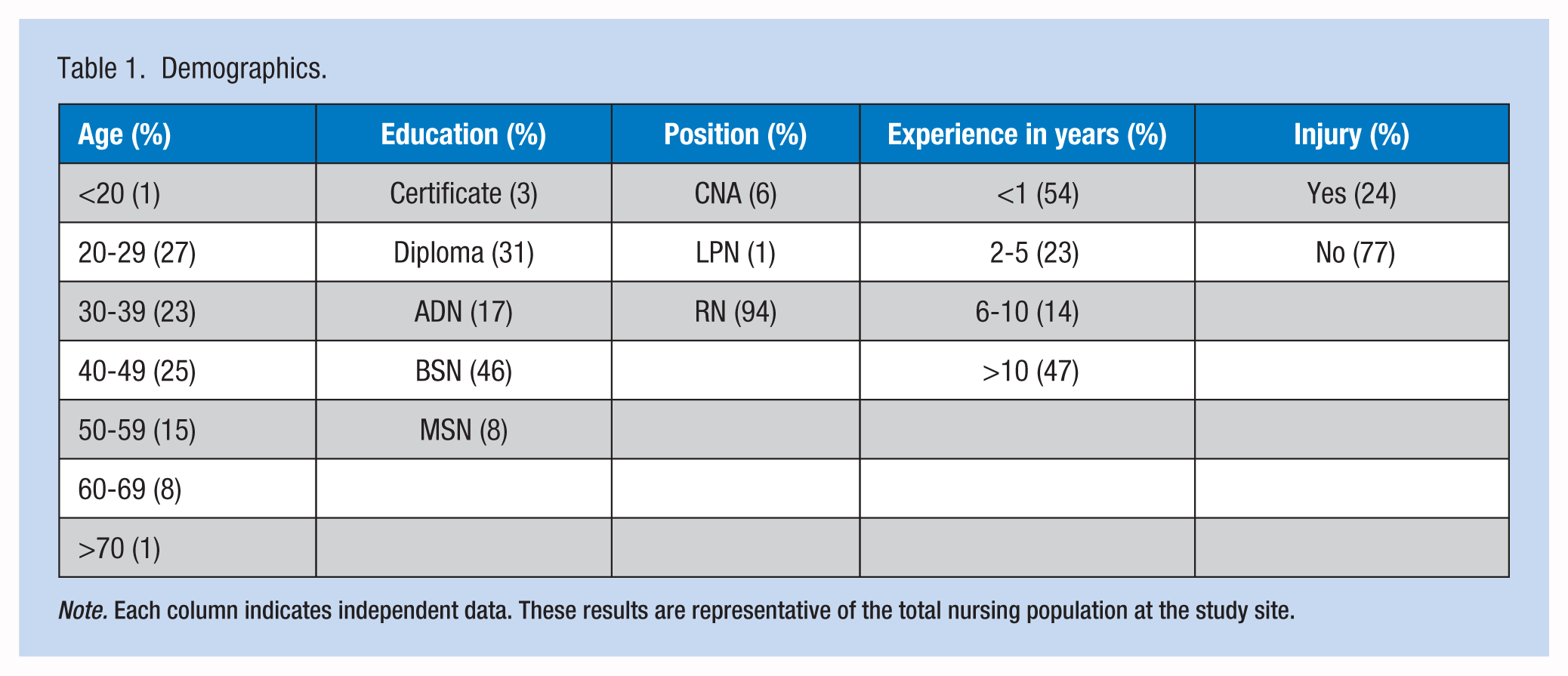
Note. Each column indicates independent data. These results are representative of the total nursing population at the study site.
Results
IBM SPSS Statistics 23.0 software was used for data analysis. The confidence level for all tests was set at 95% (p < .05). To facilitate analysis, Likert-type scale responses for agreement and frequency were collapsed into two categories. Strongly agree and agree responses were combined into a single agree category; and strongly disagree and disagree were combined into a disagree category. Always, often, and sometimes were combined into a yes category, and rarely and never into a no category. Neutral responses were discarded because they did not contribute to answering the research questions.
The influence of individual and organizational determinants on the DV, use of assistive devices, was analyzed using frequency tables, chi-square, and contingency coefficients. The correlations were tested on the frequency of assistive device use for a variety of patient activities and perceived barriers that may have influenced that use. No statistically significant correlation was found between demographics and frequency of assistive devices use (range ρ = .053-.914).
Perceived Barriers
Staffing levels (79%), workload (78%), availability of mechanical lift equipment (78%), and emergent patient needs (73%) were the most commonly reported barriers to the use of assistive devices as illustrated in Figure 2. Availability of mechanical equipment was a frequent barrier primarily due to equipment being stored too far from the unit, not quickly accessible, and difficult to retrieve. Lack of time appeared to be the underlying theme with these barriers.
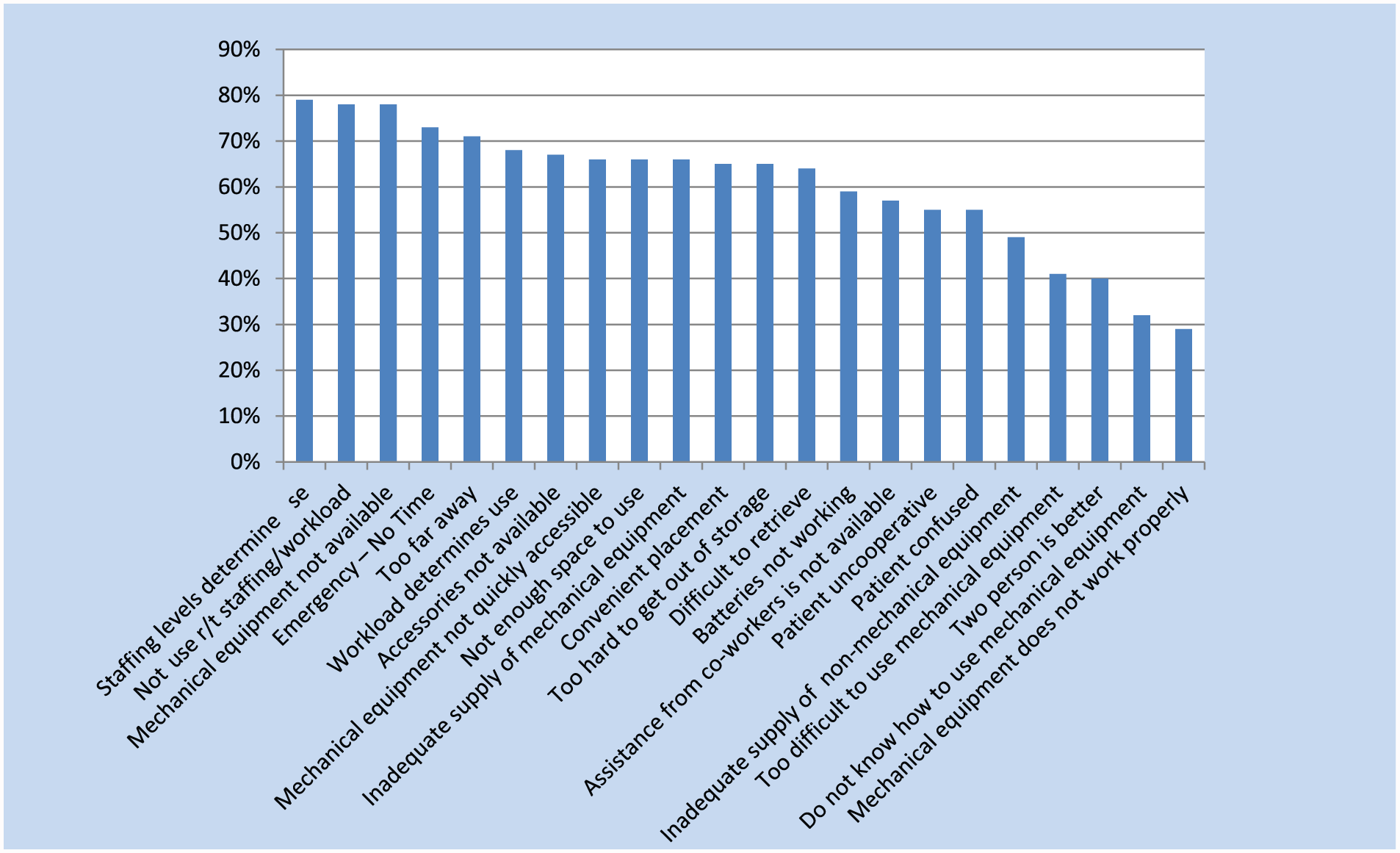
Barriers to the use of assistive devices.
Relationship Between Perceived Barriers and Use of Assistive Devices
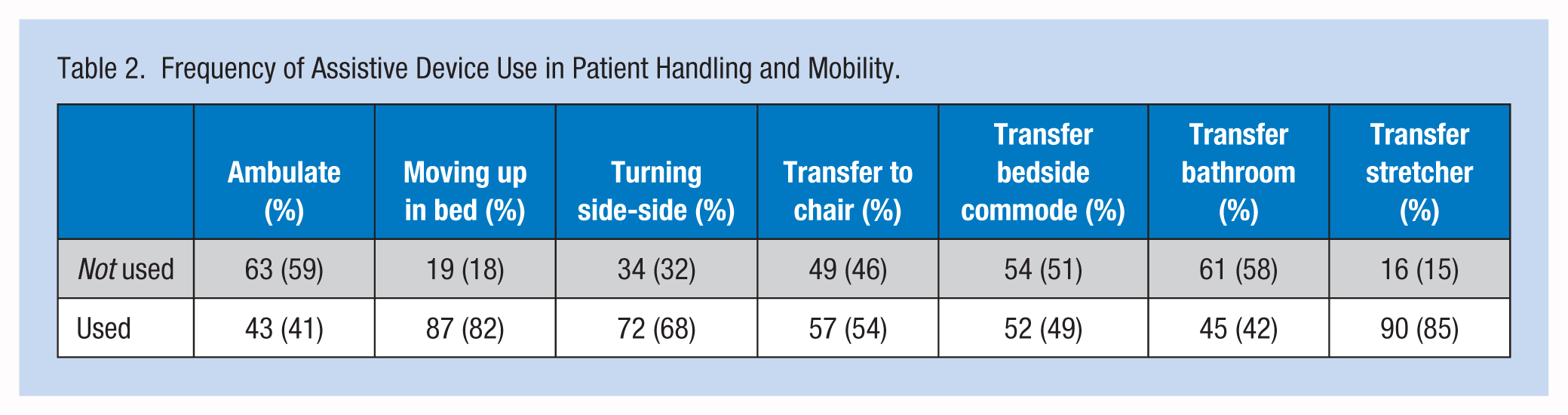
Table 2 displays the frequency of responses to the use of assistive devices based on patient activity. Assistive devices are used most often when repositioning a patient in bed, either moving patients up in bed (82%) or turning patients side to side (68%). When transferring patients to a stretcher, 85% of respondents reported using slide boards, which are readily available on each unit. Assistive devices are used least often when assisting patients with ambulation (59%), transferring to the bathroom (58%), and transferring to the bedside commode (51%).
Frequency of Assistive Device Use in Patient Handling and Mobility.
Staffing and Workload (ICD)
The majority of respondents (78%-79%) agreed that staffing and workload can affect the time available to use mechanical equipment. Of these, failure to use assistive devices in patient handling occurs most often with ambulation (60%), assisting to the bathroom (59%), and transferring to a chair (52%). Assistive devices are most frequently used when transferring patients from bed to stretcher (83%) and repositioning patients in bed (64%-78%). The differences in the frequencies of these activities were not statistically significant (range ρ = .136-.766).
Availability of Mechanical Equipment (SI)
The majority of respondents agreed that mechanical equipment is not available when needed (78%), and the supply of mechanical equipment is inadequate (66%). Respondents did not use assistive devices for transferring patients out of bed (59%) to a chair, to the bedside commode, or to the bathroom. Of the 21% who reported that mechanical equipment was available, most still did not use the equipment for ambulation (63%), transfer to a chair (57%), or moving to the bathroom (58%). Eighty-eight percent of respondents did report using assistive devices for moving patients up in bed. This correlation was statistically significantly (ρ = .022).
The majority of respondents reported that mechanical equipment was too far away (71%), not convenient to the unit (65%), and too difficult to retrieve or remove from storage (65%). Significant correlations regarding convenience and difficult retrieval were found. Conveniently located storage areas significantly influenced device use when moving patients from bed to chair (ρ = .009), from bed to commode (ρ = .010), and from bed to bathroom (ρ = .007). Use was also significantly correlated to ease of retrievability for ambulation (ρ = .009), moving the patient from bed to chair (ρ = .019), and moving the patient to the bathroom (ρ = .000).
In an emergency, 72% of respondents reported insufficient time to find and retrieve assistive devices. If assistive devices and equipment are, indeed, too far away or inconvenient to access, the additional time needed to retrieve it creates a significant barrier to the use of assistive devices.
Uncooperative or Confused Patients (ICD)
An uncooperative or confused patient was reported by 55% of respondents as a reason not to use assistive devices. However, the majority of respondents who perceived these patients as a barrier did, in fact, use assistive devices for repositioning in bed, but not for ambulation or assisting patients to the bathroom. However, the data for this barrier were not statistically significant (ranges: uncooperative ρ = .349-.960, confused ρ = .319-.941).
Manual Lifting (II/SI)
Ninety-three percent of respondents agreed that “it is safer to lift patients with mechanical equipment,” and 60% agreed that “two-person lifting is not better than using mechanical equipment.” These results suggest that staff believe in the value of safe patient handling for both patient and personal safety. However, reports of actual use did not support these beliefs (range ρ = .089-.987). Of the 40% of respondents who indicated that “two-person lifting is better than using mechanical equipment,” 74% did not use assistive devices. This finding was significantly correlated with refusing to use assistive devices for ambulation (ρ = .026).
Even though 57% of respondents reported that assistance from coworkers is not always available, the majority still did not use assistive devices to ambulate (69%) or assist patients to the bathroom (51%). Of the respondents who perceived that coworkers were available to assist (43%), the majority did not use assistive devices for ambulating patients (54%), or transferring patients to chair or bedside commode (59%). If coworkers were not available, staff were still unlikely to use assistive devices. Yet the results of this study suggest that availability of coworkers is not always a factor in staff choices about using mechanical equipment.
Knowledge/Equipment Difficulty (PSE)
Even though 32% of respondents reported a lack of knowledge as a reason to refrain from using mechanical equipment, the majority of staff did not use assistive devices when transferring patients to chairs (60%), bedside commodes (54%), and bathrooms (62%). Fifty-eight percent of respondents reported that mechanical equipment is not too difficult to use. However, of these, 64% did not use assistive devices. This barrier was not statistically significant (range ρ = .248-.992). These findings imply that respondents understood how to use mechanical devices, but chose not to use them. This barrier was not statistically significant (range ρ = .070-.955).
Conclusion
According to Holman (2010), nurses reported that they spend nearly 20% of their time on tasks associated with patient handling. This study confirmed that time constraints and difficult patient-handling situations contribute to less frequent use of assistive devices, especially mechanical devices that are difficult to retrieve or not readily available. These barriers and understaffing were the most influential factors in the decision not to use assistive devices for patient transfers.
Overall, nurses’ perceived staffing levels and workload, availability and accessibility of equipment, and emergent patient needs as the leading time constraints contributing to the lack of assistive device use in patient handling and mobility. Accessibility of equipment is particularly significant because the majority of nurses reported that equipment is too far away and too difficult to retrieve or remove from storage. This finding correlates with the infrequent and sporadic use of mechanical assistive devices. When time is scarce, the most convenient, but not necessarily the safest, method of patient handling will most often prevail over team member safety. It appears that when nurses have a higher workload, competing demands from increased responsibilities result in more expeditious choices instead of taking time to retrieve mechanical devices. This finding is consistent with other published research; the increased time required to use devices and lack of perceived need to use mechanical lifting devices are among many reasons for not using lifting equipment (Holman, 2010; Li et al., 2004; Wardell, 2007).
More than half of respondents reported not using assistive devices for patient mobility (e.g., transfer to bed, bedside commode, or bathroom). This finding may be due to patient’s level of functional mobility. However, when repositioning patients in bed, more than 81% of respondents use some type of assistive devices. This may also be due to the immediate availability of the bed pad under the patient. However, since bed pads are designed not to slip on bed sheets, more effort may be needed to lift these patients, which may increase the risk of serious injury. Because slide boards are readily available and easily retrieved, the majority of respondents (89%) reported using slide boards when transferring patients to stretchers.
Limitations
One of the most significant limitations of this study was the wording of questions on the survey tool. This tool was self-designed based on three published studies that previously identified barriers to assistive device use. Due to the complexity of the questions, respondents may have interpreted items differently resulting in inconsistent data. The survey tool could be improved using specific references to mechanical versus nonmechanical lift equipment and limiting the options related to patient mobility and handling activities to simplify data analysis. The sampling strategy captured a representative sample of all nurses within the facility, but may not have taken into account the differences between nursing units or different shifts. Another potential weakness of this study is the small study population within one acute-care setting. Although results were consistent with research in other settings, variances between larger or smaller facilities, as well as between acute-care, long-term care, and nontraditional locations, may exist.
Implications for Practice
This study has particular implications for occupational health nurses who possess the knowledge and skills to present business plans to support the implementation of comprehensive ergonomics programs. This study’s focus on barriers and why nurses choose not to use assistive equipment provides evidence-based explanations to improve employee safety, reduce absenteeism due to injury, and limit time away from work. Occupational health nurses must educate their colleagues and administrators on the effects of WMSD associated with patient care. With an increasing emphasis on reduced spending through increased efficiency, quality outcomes, and patient satisfaction, it is essential that worker safety be an overriding priority. Based on the top barriers identified in this research, evidence-based solutions include making assistive equipment easily accessible, implementing patient mobility assessment protocols and “no-lift” policies, and developing an organizational culture that emphasizes protecting the well-being of staff as well as patients.
Staff perceptions can be a formidable obstacle to implementing and sustaining a successful, comprehensive SPHM program. This study confirmed that team members disregarded the potential for personal injury when choosing not to use assistive devices. Peer leaders and coaches can influence the likelihood of assistive device use through education and mentorship that supports healthy behaviors. Nurse leaders must be empowered to advocate for positive work environments and organizational cultures of safety for all.
More research is needed on the incidence and severity of work-related injuries among health care workers, especially in the areas of cost benefit or return on investment from the implementation of an SPHM program. Also, the effectiveness of unit-based peer leaders and clinical tools, such as patient assessment protocols, should be further evaluated and refined. So far, most research has focused on “average-size” patients in the hospital and long-term care. More research is needed in other settings such as home health care and emergency response, as well as with obese and morbidly obese patients.
Summary
It is imperative that the incidence and severity of work-related injuries among health care workers be reduced, if not eliminated. This study contributes to the literature regarding the factors that influence the use of assistive devices in handling and moving patients. The findings support the implementation of comprehensive SPHM programs.
Comprehensive planning, strategic implementation, continued monitoring, and modification of programs, as needed, will assure successful outcomes. The benefits of SPHM programs include improved quality of patient care related to improved patient mobility, fewer falls, pressure ulcers, and skin tears; improved patient and caregiver satisfaction; fewer work-related injuries; and less WC costs (Beauvais & Frost, 2014; A. Hepburn & S. Kuperman, personal communication, March 5, 2012). Improving the work environment promotes recruitment and retention of qualified staff, a reduction in lost time or restricted duty due to injury, and prevention of unnecessary early retirement. A supportive culture will discourage caregivers from reverting to old behaviors without concern for their personal safety. An organizational culture of safety and accountability for both patients and team members, which supports the appropriate use of patient-handling techniques and equipment, must be embraced by every employee, including management and caregivers.
Applying Research to Practice
This study confirmed that the most influential factors in the decision to use assistive devices for patient transfers are time constraints and difficult patient-handling situations. These factors lead to infrequent use of assistive devices, especially mechanical devices that are difficult to retrieve or not readily available. With a focus on reduced spending and patient satisfaction, worker safety must be an overriding priority. Comprehensive safe patient handling and mobility (SPHM) programs must be implemented using evidence-based solutions to include making assistive equipment easily accessible, implementing assessment protocols, developing “no-lift” policies, and fostering an organizational culture that protects staff as well as patients. The benefits to both staff and patients far outweigh the cost of failing to implement a sustainable SPHM program.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Nancy L. Noble serves as adjunct faculty, DNP Nurse Executive Program at ODU and nursing professional development practitioner for Riverside Health System.
Nancy L. Sweeney is the program director and professor of practice for the Nurse Executive DNP Program, and faculty advisor at ODU, Norfolk, Virginia.