
Abstract
Health care workers suffer from musculoskeletal disorders at a significantly higher rate than workers in other industries. Consequently, a growing demand for patient handling devices to reduce worker injury has evolved. This article reviews the literature regarding interventions designed to reduce injuries among health care workers. A PubMed search was conducted using the terms “occupational health [Mesh Terms] patient lifting.” Fourteen articles were identified that assessed interventions to improve worker safety. Of the 14 articles, 7 discussed technological interventions, 4 educational approaches, and 3 policy change. All three types of interventions were generally effective at improving worker safety, with the ideal intervention consisting of elements of all three types. Although adopting a new intervention may be expensive, the reduction in workers’ compensation costs associated with injured nurses can easily outweigh the costs of interventions.
Keywords
According to the U.S. Bureau of Labor Statistics, health care workers suffer from musculoskeletal disorders at a significantly higher rate than workers in many other demanding fields such as manufacturing, construction, and mining (Collins, 2010). The majority of health care workers’ musculoskeletal injuries result from repositioning, moving, and assisting patients (Schoenfisch, Lipscomb, Pompeii, Myers, & Dement, 2013). In 2008, the National Institute for Occupational Safety and Health (NIOSH) estimated the costs associated with musculoskeletal-related injuries reported by health care workers to be approximately US$7.4 billion annually (Waehrer, Leigh, & Miller, 2005). This risk of injury is expected to worsen due to an aging workforce and the ever increasing obesity epidemic in America, increasing the weight of patients being lifted (Collins, 2010). The average critical care nurse currently lifts three tons per day, making patient lifting the primary reason that 52% of nurses report back pain and 18% leave the profession each year due to injury (American Nurses Association [ANA], 2012; J. Li, Wolf, & Evanoff, 2004).
The ANA, NIOSH, the National Association of Orthopedic Nurses (NAON), and the Association of Perioperative Registered Nurses (AORN) have all adopted guidelines regulating the weight that health care workers are allowed to lift manually. Any task that entails movement of a patient greater than the limit requires an assistive device. Based on these guidelines and the growing rate of obesity in America, an increasing demand for assistive devices and technology-based safe patient handling programs has emerged in the health care field (Collins, 2010). In testimony to the U.S. Senate, Collins (2010) emphasized the need for technology-based solutions to the high risk of musculoskeletal injuries in health care.
In this current review, the authors’ goal was to review literature on technological and other interventions aimed at reducing occupational musculoskeletal injuries among health care workers.
Method
To identify relevant literature regarding various interventions used to reduce musculoskeletal injuries among health care providers, the database, PubMed, was searched using the terms “occupational health [Mesh Terms] patient lifting.” This search yielded 167 results. Inclusion criteria included the following: (a) studies that were published prior to April 2014 that implemented an intervention aimed at improving worker safety, (b) studies that assessed the efficacy of a particular intervention, (c) study participants had health care backgrounds, and (d) studies published in English. After the 167 results were assessed for relevance, content, and language, 14 articles met the criteria.
After the list of studies was established, data were collected on sample size, intervention type, personnel involved, and outcome measures. For the purposes of this review, articles were categorized by intervention type into three areas: device intervention, education intervention, and policy change intervention (Table 1).
Effects of Interventions to Reduce Health Care Worker Injuries Related to Patient Lifting
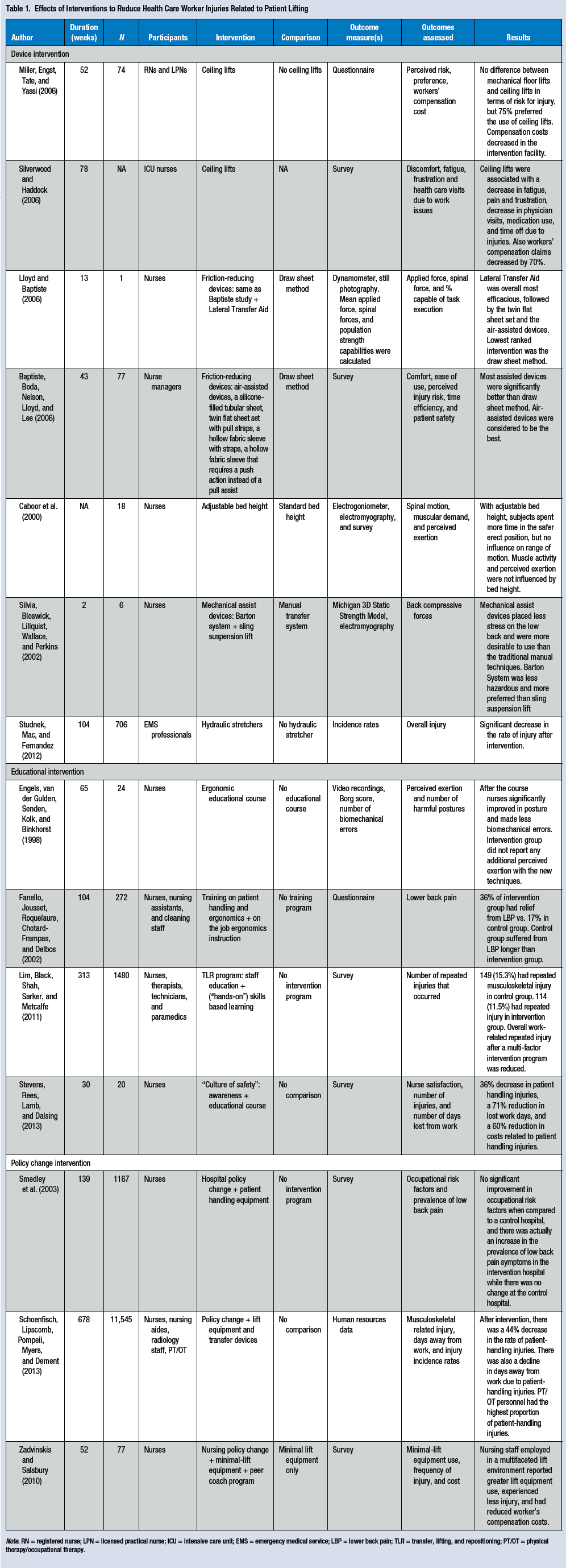
Note. RN = registered nurse; LPN = licensed practical nurse; ICU = intensive care unit; EMS = emergency medical service; LBP = lower back pain; TLR = transfer, lifting, and repositioning; PT/OT = physical therapy/occupational therapy.
Results
The authors identified seven publications about devices to reduce occupational safety risk. Two of the articles assessed the efficacy of ceiling lifts in moving patients. Miller, Engst, Tate, and Yassi (2006) conducted a pre-/post-intervention study in which researchers compared an intervention facility with ceiling lifts to a control facility without these lifts. The nursing staff felt at less risk of injury when using ceiling lifts compared with manual lifting methods. Furthermore, 75% of staff preferred ceiling lifts over other methods of patient transfer. At 1 year post-implementation of ceiling lifts, a 70% decrease in claims costs at the intervention facility were realized; at the comparison facility, a 241% increase in claims cost over the same time period was documented. Silverwood and Haddock (2006) surveyed intensive care unit (ICU) nurses at a Richmond hospital about fatigue, pain, and frustration before and after installation of ceiling lifts. The ICU nurses reported that ceiling lifts decreased fatigue, pain, and frustration. In addition, a significant 70% reduction in workers’ compensation claims was documented within the first year after lift introduction. The musculoskeletal injury rates at this particular hospital continued at the lower level for over 2 years after the intervention was implemented.
Two studies explored the performance of friction-reducing lateral transfer devices compared with the traditional draw sheet method. The first study reported the findings of a biomechanical evaluation of 11 transfer devices (Lloyd & Baptiste, 2006), including air-assisted devices, a silicon-filled tubular sheet, twin flat sheet set with pull straps, a hollow fabric sleeve with straps, a hollow fabric sleeve that requires a push action instead of a pull, and the Lateral Transfer Aid (LTA), a two-sheet device (one padded, one slippery) with handles. The primary outcomes measured included applied force, spinal force, and the percentage of the population capable of task execution. These three outcome measures were used to develop an overall ranking system that demonstrated the LTA to be the most efficacious device, followed by the twin flat sheet set and air-assisted devices. The lowest ranked intervention was the draw sheet.
The other study was a clinical evaluation of all the same devices mentioned in the Lloyd study with the exception of the LTA (Baptiste, Boda, Nelson, Lloyd, & Lee, 2006). Efficacy of each device was rated based on caregiver surveys that focused on five areas: comfort, ease of use, perceived injury risk, time efficiency, and patient safety. Based on the results of the surveys, an overall rating scale was calculated and the air-assisted devices had the best overall performance.
To understand the influence bed height has on musculoskeletal risk, researchers investigated the effects on spinal motion, muscular demand, and perceived exertion when nurses were able to adjust bed height (Caboor et al., 2000). No differences were found in muscular exertion activity or perceived exertion when nurses were given the opportunity to adjust bed height as opposed to working with a standard height. The adjustable bed height did improve the quality of spinal motion, promoting a safer, more erect posture.
When mechanical transfer-assist devices were compared with manual patient transfer, the mechanical assistive devices were preferred by caregivers and superior in placing less stress on the lower back according to electromyography measurements (Silvia, Bloswick, Lillquist, Wallace, & Perkins, 2002). The two mechanical devices studied were the Barton patient transfer system and the sling suspension system. Of the two, the Barton system was considered less hazardous and more often preferred by hospital staff.
In a retrospective study, hydraulic stretchers were associated with a significant decrease in injuries among emergency medical service (EMS) personnel (Studnek, Mac, & Fernandez, 2012). Due to the retrospective nature of this study, researchers addressed the possibility that the decrease in injury rate could be attributed to other causes such as maturation of the study population and more ergonomic awareness at the same time hydraulic stretchers were introduced. Without a control group, it is difficult to recommend hydraulic stretchers.
Educational intervention
Four publications discussed educational interventions. All four studies reported positive findings after educating health care workers. An ergonomic course provided nurses with education about the proper technique and form for patient lifting and other nursing activities (Engels, van der Gulden, Senden, Kolk, & Binkhorst, 1998). After the intervention, nurses improved their posture and made fewer biomechanical errors compared with a control group that received no intervention. Having participants receive on-the-job ergonomic instruction while preforming their usual work tasks reduced the number of individuals with low back pain (Fanello, Jousset, Roquelaure, Chotard-Frampas, & Delbos, 2002). In another, more recent study, staff education on patient handling procedures and proper equipment use reduced the rate of repeated musculoskeletal injuries (Lim, Black, Shah, Sarker, & Metcalfe, 2011).
A “culture of safety for safe patient handling” was created in phases for another health care study; the first phase required a few select peer leaders to identify high risk patient handling tasks at the workplace, and then these leaders worked to educate the staff on ergonomic behaviors and provide additional equipment for patient handling (Stevens, Rees, Lamb, & Dalsing, 2013). After 1 year, costs related to patient handling injuries decreased 60%, patient handling injuries decreased 36%, and lost work days decreased 71%.
Policy Intervention
Three publications reported studies about the impact of policy change on occupational health risk. A hospital-wide manual handling policy to minimize unassisted patient handling engaged all levels of management from the operational board to the health and safety advisory committee to the rest of the staff (Smedley et al., 2003.) The hospital purchased patient handling equipment such as slide sheets, hoists, and transfer belts and distributed them to the floors. Researchers measured the outcome of this intervention using surveys. No significant improvement in occupational risk factors was found when compared with a control hospital that received no intervention. In addition, the prevalence of low back pain symptoms associated with the intervention increased. Researchers concluded that the policy intervention attempted at this hospital was unsuccessful; however, due to a number of limitations described by the authors, it is difficult to draw any meaningful conclusions. This study did demonstrate the difficulty of executing effective interventions in complex organizations such as hospital systems.
Schoenfisch et al. (2013) reported more success with their large scale hospital-based policy change. This study introduced a “minimal manual lift environment” (MMLE) policy to a community-based hospital. Nurses were educated on the policy and provided with lift equipment and transfer devices. Following intervention initiation, patient handling injuries and days missed due to handling injuries were reduced. However, other institutional-level changes occurred outside of the study; these changes were likely to have contributed to the findings as well.
The last study focused specifically on nursing policy. The intervention group received minimal lift equipment and a peer coach program to instruct study nurses on how to use the equipment; the comparison group received only minimal lift equipment (Zadvinskis & Salsbury, 2010). The intervention group used minimal lift equipment more frequently, experienced fewer injuries, and had lower workers’ compensation costs.
Discussion
The extent of and estimated costs associated with musculoskeletal injuries among health care workers is alarming. The testimony by Collins clearly outlined the problem as well as addressed the need for change at the workplace. Based on the findings of this review, device and educational interventions may improve worker safety. Eleven states have already enacted “safe patient handling laws” or established regulations that require health care facilities to provide proper equipment, education, and policies that promote worker health and safety (American Nurses’ Association, 2014). The advocacy efforts of organizations such as the ANA, and statements made by NIOSH and other government agencies, suggest that no-lift policies, incorporating device and educational interventions, should become law nationwide.
Some limitations of this study are that the articles reviewed tested only a limited range of strategies, and therefore, it was not possible to precisely define best practices. It is likely that lifting teams, core training, and conditioning might be helpful in reducing injuries, but these strategies were not tested in the articles reviewed.
Implications
Provider offices and hospitals should be proactive in implementing strategies and using devices aimed at improving worker health and safety. Most of the devices discussed in the review are merely assistive; however, the goal should be to develop technology that eliminates patient lifting (e.g., a wheelchair that becomes an exam table; Martin Innovations, 2014). By developing innovative technological solutions, health care workers can avoid safety hazards. Adopting new technology may appear to be expensive, but the reduction in workers’ compensation costs and loss of nurses’ productivity can easily outweigh the costs of these devices. In a NIOSH-supported study, researchers implemented a safe lifting program that established a lifting policy and provided mechanical lifting equipment and associated education. The total expenditure on this intervention was US$158,556; however, this cost was easily recovered in less than 3 years due to savings of US$55,000 per year in workers’ compensation costs alone (S. Li, McAlpine, Liu, Li, & Collins, 2004).
Conclusion
Based on the findings presented in this review, existing technologies can reduce worker lifting risks. Health care institutions can improve worker safety by implementing cost-effective strategies that improve technological devices, worker education, and policy development. Given the occupational hazards currently being faced by health care workers, further research should be undertaken to create a no-lift environment and enhance both patient and worker safety.
Applying Research to Practice
Most studies assessing device, educational, or policy interventions to reduce health care worker injuries from patient lifting have shown some success. However, the goal should be to eliminate the need for lifting altogether as much as possible. Interventions that eliminate lifting can recoup the initial investment in 3 years or less. In addition, legislation is expected to mandate nationwide no-lift policies within the next few years. Given the benefits in terms of worker safety, further development of technology that allows safe patient transport without lifting should be a top priority.
Footnotes
Conflict of Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Martin is the founder and CEO of Martin Innovations, manufacturer of lift equipment. Dr. Feldman has received research, speaking, and/or consulting support from a variety of companies including Galderma, GSK/Stiefel, Leo Pharma, Baxter, Boeringer Ingelheim, Mylan, Celgene, Pfizer, Valeant, Abbvie, Amgen, Anacor, Astellas, Janssen, Lilly, Merck, Merz, Novartis, Qurient, National Biological Corporation, Caremark, Advance Medical, Suncare Research, Informa, UpToDate and National Psoriasis Foundation. These are not related to the topic of this article. Dr. Feldman is a consultant and speaker for Galderma, Stiefel/GlaxoSmithKline, Abbott Labs, Warner Chilcott, Janssen, Amgen, Photomedex, Genentech, BiogenIdec, and Bristol Myers Squibb. Dr. Feldman has received grants from Galderma, Astellas, Abbott Labs, Warner Chilcott, Janssen, Amgen, Photomedex, Genentech, BiogenIdec, Coria/Valeant, Pharmaderm, Ortho Pharmaceuticals, Aventis Pharmaceuticals, Roche Dermatology, 3M, Bristol Myers Squibb, Stiefel/GlaxoSmithKline, Novartis, Medicis, Leo, HanAll Pharmaceuticals, Celgene, Basilea, and Anacor and has received stock options from Photomedex. Dr. Feldman is the founder and holds stock in Causa Research. Mr. Aslam and Mr. Davis have no conflicts to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Center for Dermatology Research is supported by an unrestricted educational grant from Galderma Laboratories, L.P.
Author Biographies
Imran Aslam is a fourth year medical student from Northeast Ohio Medical University.
Scott A. Davis is former Assistant Director of the Center for Dermatology Research at Wake Forest School of Medicine, and a doctoral student at UNC Eshelman School of Pharmacy. His research focuses on outcomes research and interventions to improve adherence to healthy behaviors.
Steven R. Feldman is Director of the Center for Dermatology Research and Professor of Dermatology, Pathology, and Public Health Sciences at Wake Forest School of Medicine. His research interests include patient safety, occupational health, and patient satisfaction with medical care.
Willis E. Martin is the founder and CEO of Martin Innovations. His research focuses on developing zero-lift devices to avoid the need for manual lifting during patient transfers.