
Abstract
Falls can occur in any occupational setting. Occupational health professionals may focus on creating a safe work environment and training programs to prevent falls. However, an important aspect of safety management is identifying at-risk employees. The purpose of this article is to identify personal risk factors and offer interventions to prevent falls in the workplace.
Keywords
The risk of falls is present in all occupational settings. According to the Bureau of Labor Statistics (BLS; 2015a), in 2014, falls in the workplace resulted in 793 deaths. These falls occurred on both low level and high level worksites. In 2014, 626,660 nonfatal occupational falls occurred at high and low levels (BLS, 2015b).
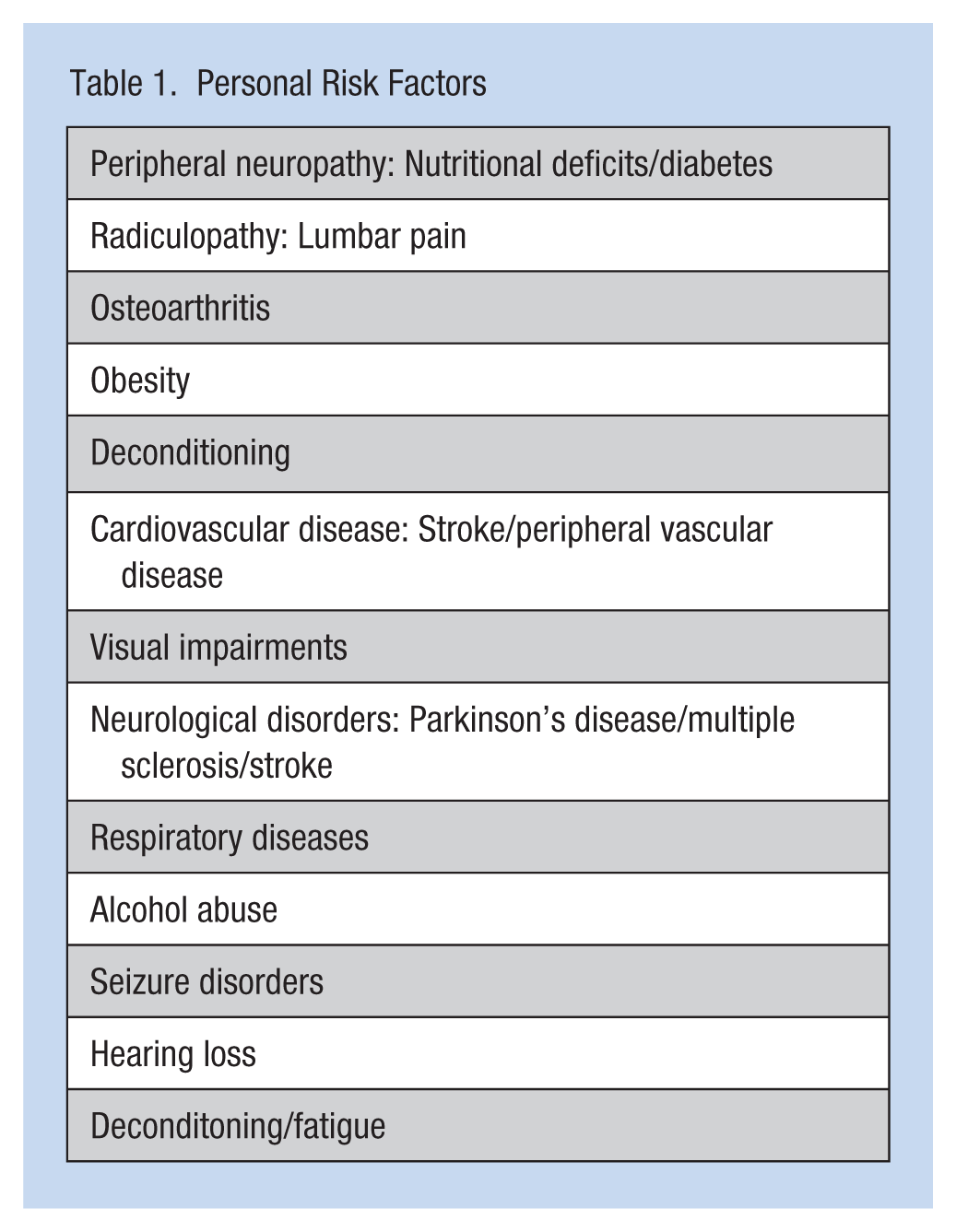
A fall can result from a slip or trip, or when employees are performing multiple tasks (e.g., carrying an item up a flight of stairs). According to Goetsch (2011), primary causes of falls include a foreign object on the walking surface, a design flaw (e.g., an uneven floor), slippery surfaces or the employee’s physical condition (Rhodes, 2006). Injuries from a fall may include lacerations, sprains and strains, or fractures. When investigating a fall, the occupational health nurse should focus on the environment and the mechanism of the fall as well as conduct a fall risk assessment (Table 1).
Personal Risk Factors
Personal Fall Evaluation
It is the responsibility of the employer to create a safe work environment (i.e., safe physical environment and continuous training) to reduce the risk of falls. Housekeeping (e.g., cleaning oily or wet surfaces) is also critical to a safe work environment as well as specific work clothes (e.g., nonskid footwear). However, it is the responsibility of the occupational health nurse to identify at-risk employees during the preplacement or annual examination, and upon return to work for those workers who may have experienced a stroke or recent eye surgery.
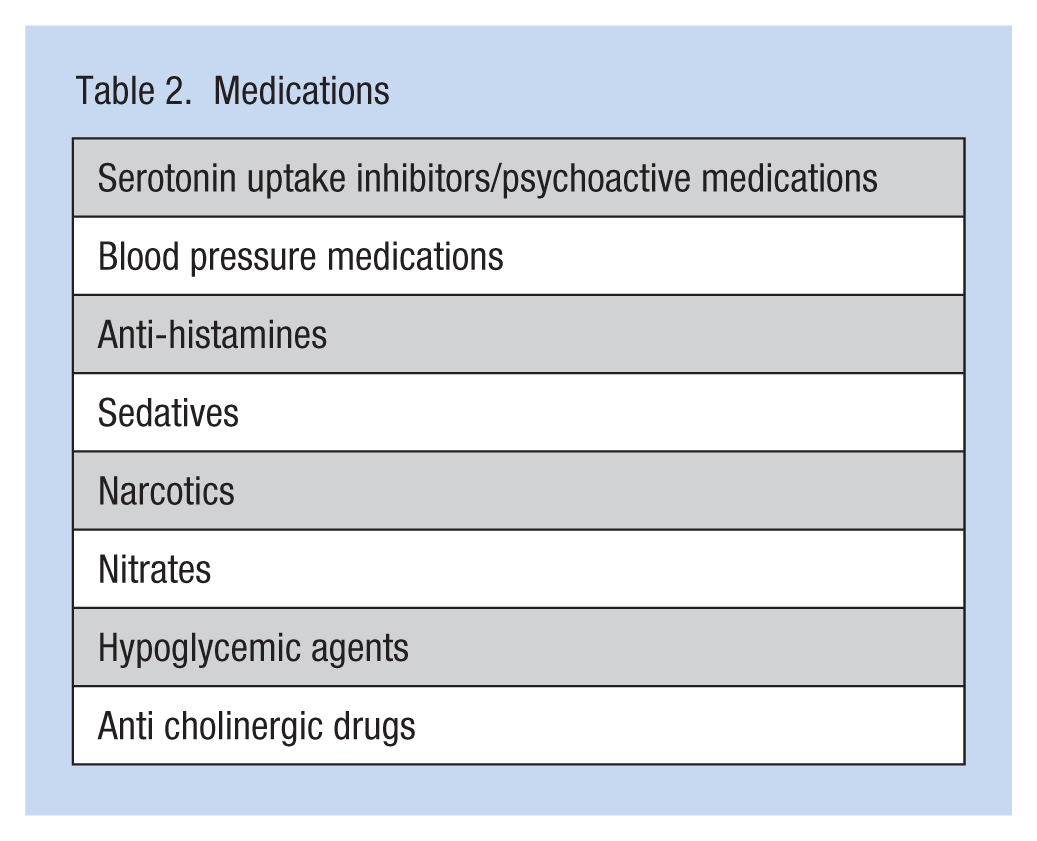
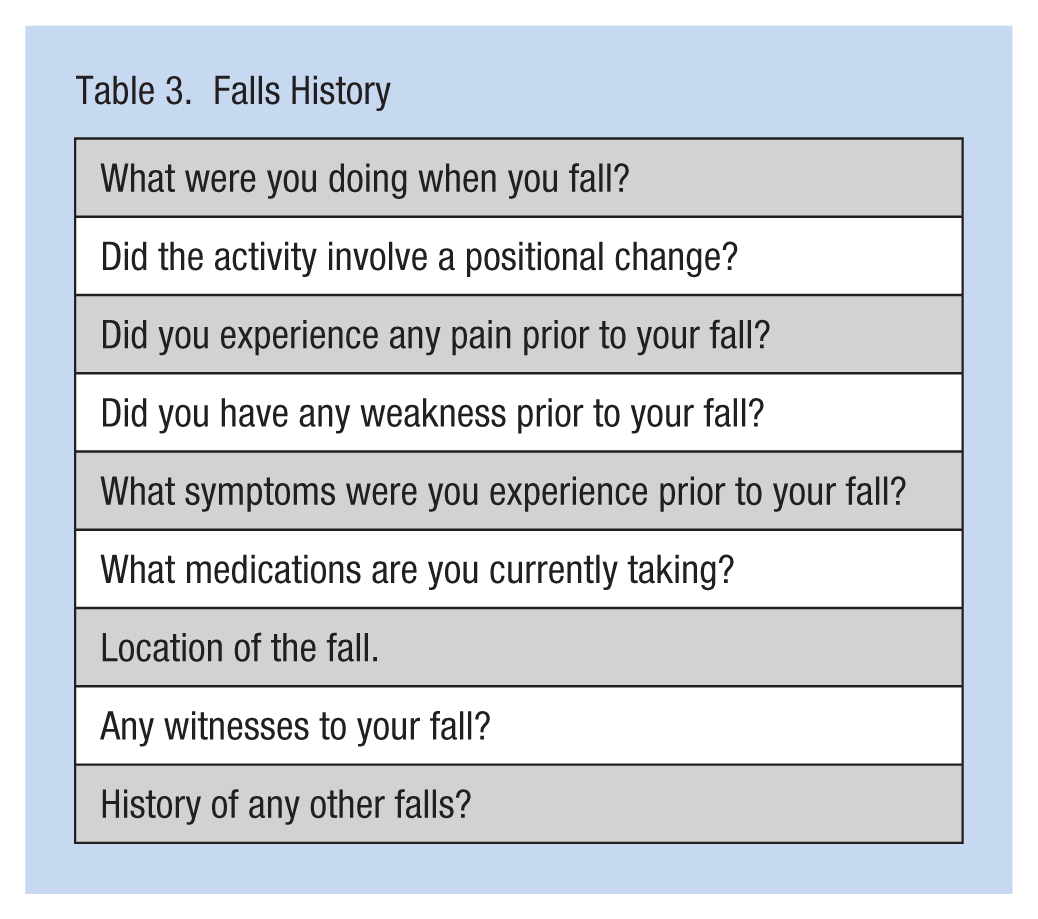
During a physical examination, the occupational health nurse gathers a comprehensive health history and a complete physical examination. Past health history should focus on disease processes (e.g., stroke or diabetes) that may increase an employee’s risk for falls (Table 2). Disease processes that may lead to sensory loss or muscle weakness need further evaluation. Other disease processes (e.g., altered glucose or hypotension) may lead to balance disturbances. Evaluation of medications should focus on side effects of dizziness or unsteadiness (Table 3).
Medications
Falls History
During the skin examination, the first step in the physical examination, the occupational health nurse should assess for signs of falls (e.g., bruises, contusions, localized swelling, or lacerations). Further questioning is warranted if the employee is prescribed anticoagulants. The respiratory and cardiac examination should identify abnormal breathe or cardiac sounds that could affect mobility due to fatigue or pain. Gastrointestinal and genitourinary examinations may reveal bowel or bladder incontinence that may contribute to employees rushing to the bathroom and not focusing on hazards in the physical environment. Obese workers are at risk for falls due to altered postural balance, pain, or deconditioning (Mitchell, Lord, Harvey, & Close, 2014). Visual impairments may alter depth perception and visual acuity. At-risk employees for visual impairments are older workers and workers with hypertension and diabetics who should be encouraged to schedule annual ophthalmology examinations including assessment of depth perception which is critical for judging distance to an object. Workers with strabismus or monovision may have impaired depth perception due to their inability to accommodate for distance or see three-dimensional (3D) objects accurately.
The neurological and musculoskeletal examination is a critical part of fall assessment. Musculoskeletal changes include mobility issues that may result from decreasing muscle strength or pain (e.g., arthritic changes in the older adult). Foot disorders such as bunions may contribute to pain when walking. Neurological disorders may impair balance and reduce reaction time.
Physical Examination
The first step in assessing for falls is inspection of the skin for bruises, lacerations, localized swelling, or contusions. The next step is to assess for visual acuity, extraocular movements, PERRLA (
Respiratory examination may reveal abnormal breathe sounds indicating impairment of gas exchange that could contribute to fatigue or dizziness. The cardiac examination should include auscultation for murmurs and extra heart sounds as well as assessing orthostatic blood pressure. The peripheral vascular system assessment should include palpating peripheral pulses and identifying signs of venous stasis or arterial insufficiency.
The musculoskeletal system assessment includes the palpation of all joints, particularly assessing for crepitus in any joint; while assessing range of motion, the occupational health nurse should also record muscle strength, muscle tone and bulk, and muscle atrophy. To assess the spinal accessory nerve, the trapezius and sternomastoid muscles should be investigated as well as the ability to turn the head quickly. The neurological assessment includes Romberg testing to determine balance and detect disease of the dorsal columns of the spinal cord, cerebellar disease, or vestibular dysfunction. Proprioception testing is used to determine body positioning. Deep tendon reflexes and clonus with hyperflexia can indicate upper motor neuron disease; decreased or absent reflexes indicate lower motor neuron disease. Multiple sclerosis is an example of an upper motor disease, and a herniated disk with radiculopathy is considered a lower motor neuron disease. Reflexes should be symmetrical; however, in the example of a herniated disk with radiculopathy, reflexes may be diminished on the affected side. Sensory testing of the upper and lower extremities should be considered with fine or thick monofilaments. A decrease in the sensory pathway may indicate peripheral neuropathy.
Vibratory testing is used to determine early sensory or vibratory loss. A tuning fork at 128 or 256 Hz may be used. Audiograms are used to diagnose hearing loss. Further assessment of hearing may determine conducive or sensorineural loss. Inspection of the outer ear and ear drum is required.
Abnormal gait, rapid alternating movements or point to point movements, can indicate cerebellar disease. Weakness in one arm, pronator drift, can be a sign of contra lateral lesion of the corticospinal tract. When asked to walk heel to toe (tandem walking), workers who walk on their toes or heels (plantar flexion or dorsiflexion) may have a disease of the corticospinal column or cerebellar disease. Finally, employees should hop in place to complete balance testing. However, the occupational health nurse should use caution if the patient is obese, or has neurological or musculoskeletal impairments. For example, an employee with degenerative joint disease of the knees, hips, or ankles may experience pain when hopping in place.
Functional assessments are often performed by a physical therapist. Two specific tests, Timed Up and Go and gait analysis, are usually included in these assessments. Timed Up and Go consists of testing mobility, gait speed, and static and dynamic balance. Gait analysis measures body movements and body mechanics which may indicate the need for an assistive device.
Case Studies
TB is a 58-year-old male worker who was recently diagnosed with macular degeneration. Macular degeneration is characterized by a loss of central vision, impaired depth perception, and decreased visual acuity. TB, assigned to work on a scaffold, was looking up in an attempt to grab a side rail, misjudged the distance of the side rail, and fell forward. Luckily, the worker was wearing a safety harness or he would have fallen two stories. TB was referred to his ophthalmologist who was provided with TB’s job description to determine whether he could continue to perform his job safely. The physician determined that TB could no longer work safely and was offered disability retirement.
JS is a 67-year-old female with a body mass index of 35, a history of bilateral osteoarthritis of the knees, and recently diagnosed with osteoporosis. She complains of knee pain when she walks and, to make matters worse, her left knee “locks” on occasion, also affecting her mobility. JS was walking in the parking lot when her left knee “locked”; she was unable to lift her left leg over a small step, fell on her side, and sustained a fractured hip.
CC is a 34-year-old female receptionist at a physician’s office who returned to work 8 weeks after the birth of her first child. CC states she was prescribed a Serotonin Reuptake Inhibitor (SSRI) for postpartum depression. She complains of fatigue because she has multiple sleep interruptions each night when her newborn requires feeding. CC states that the SSRI is relieving her symptoms of depression, but she feels “a little off balance and lightheaded,” especially when standing from a sitting position. When one of her coworkers needed CC’s assistance immediately, CC quickly rose from her chair to assist, became lightheaded, fell forward, and hit her head on the wall.
Implication for Occupational Health Nurses
When a fall occurs, the occupational health nurse should complete a comprehensive history and physical to identify personal risk factors. When abnormal findings are identified, referral to a primary care provider should be made for diagnosis and management, even if the cause is work related. Management of the disease processes may decrease the risk of falls. For examples, diabetic workers must manage blood glucose and blood pressure to reduce the risk of ocular disease and neuropathy. Cognitive screening should be offered to those employees who have experienced stroke or other neurological disorders. Hearing deficits or employees who wear hearing protection are at risk for falls because they have less awareness of their environment, diminished auditory clues, and possible postural imbalance (Vitkovic, Le, Lee, & Clark, 2016). Hearing tests should be offered, and if a hearing loss is discovered, referral to an audiologist for hearing aids may be indicated.
It is critical to review medications prescribed for workers. Employees should be counseled about using prescribed controlled substances while at work. If employees are prescribed antihypertensive medications, orthostatic blood pressures should be measured. Employees should be instructed to change positions slowly if prescribed medications may impair balance or cause dizziness. Diabetic workers should be allowed to check glucose levels at work as well as offering these employees the opportunity to check blood pressures. If employees are prescribed anticoagulant medications, occupational health nurses should provide appropriate protective equipment (e.g., knee pads or helmets) to protect workers from fall injuries.
Exercise is highly recommended. Employees may be referred to physical therapy for strength training, if employees have muscle weakness or are deconditioned. Workers with peripheral vascular disease are at risk for neuropathies; exercise and controlling underlying risk factors may decrease fall risk in this population. Pain associated with osteoarthritis may be treated with nonsteroidal medications or heat. Weight loss may improve postural balance and relieve pain from osteoarthritis.
Maintaining bone health can decrease the risk of injury for both men and women. Recommendations include bone density scans to assess for osteoporosis, weight bearing exercises, and calcium/vitamin D supplements, if not contraindicated. Smoking cessation and less alcohol intake can also improve bone health. The employee may need counseling on proper footwear.
For workers with neuropathy or diseases of the nervous system, physical therapy may be ordered for gait and balance training. Physical therapists may also evaluate employees for assistive devices as allowed in the workplace or employees may have to be reassigned if unable to perform their current job duties.
Conclusion
Fall causation is multifactorial. Employers must provide a safe workplace and safety training for employees. Occupational health nurses can contribute to safety programs by identifying worker risk factors and providing interventions to reduce the risk of falls. Determining whether employees can perform their jobs safely without endangering themselves and others is the ultimate goal of occupational health and safety. Occupational health nurses have a critical role to play in workplace safety by understanding and communicating how disease processes can increase workplace falls and injuries and implementing interventions that promote safety.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Ann Regina Lurati is a nursing lecturer at California State University at Monterey Bay and specializes in community/public health nursing.