
Abstract
The purpose of this review was to examine workplace lactation accommodations, and their association with breastfeeding duration, and identify strategies occupational health professionals can use to promote lactation improvements. This study included literature published from 1985 through 2015 and listed in PubMed and CINAHL. Using Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), 11 articles were identified for review. Presence of a corporate lactation program, on-site child care, and return to work/telephone lactation consultation were consistently associated with breastfeeding at 6 months. Other breastfeeding accommodations (i.e., lactation spaces, lactation breaks, worksite lactation policies, and supervisor/coworker support) were not consistently associated with breastfeeding duration. Occupational health professionals can play key roles in improving the effectiveness of lactation accommodations. Assuring adequate implementation of accommodations, increasing communication and marketing of accommodations, and promoting supervisor and coworker support are areas that occupational health professionals should explore for improving lactation duration.
In the United States, the breastfeeding (BF) initiation rate is considerably higher than the breastfeeding rate at 6 months. Based on the 2016 United States Breastfeeding Report Card, the national BF initiation rate (percentage of infants ever fed breast milk) was 81.1%; however, only 51.8% of infants were still breastfed at 6 months of age (Centers for Disease Control and Prevention [CDC], 2016). One explanation for BF attrition is maternal employment. Data suggest that many women are employed outside the home shortly after giving birth (Han, Ruhm, Waldfogel, & Washbrook, 2008). In 2001, among women who were employed prior to the birth of a child, the proportion who returned to work by 1, 2, 3, and 9 months postpartum were 10%, 40%, 70%, and 90%, respectively, (Han et al., 2008).
In the literature, several variables have been associated with failure to initiate and continue BF. Some of the most influential variables include race, marital status, extended separation from the infant, age, income, and education (Ogbuanu, Glover, Probst, Hussey, & Liu, 2011). Return to full-time employment after the birth of a child has also been consistently associated with failure to initiate and continue BF (Attanasio, Kozhimannil, McGovern, Gjerdingen, & Johnson, 2013; Mandal, Roe, & Fein, 2010; Mirkovic, Perrine, Scanlon, & Grummer-Strawn, 2014b; Ogbuanu, Glover, Probst, Liu, & Hussey, 2011). Among working women, analyses of national data sets have supported positive associations between prolonged maternity leave (Mandal et al., 2010; Mirkovic, Perrine, Scanlon, & Grummer-Strawn, 2014a, 2014b), part-time employment (Mandal et al., 2010; Ogbuanu, Glover, Probst, Hussey, & Liu, 2011), and extended BF duration (number of weeks or months an infant receives breast milk). The Fragile Families and Child Well-Being Study, a U.S. longitudinal study of first-time and unwed parents and their children, demonstrated that mothers working outside the home were most likely to discontinue BF the month immediately before, during, or immediately after returning to work (Kimbro, 2006).
Longer BF duration is associated with health benefits for infants, including fewer acute illnesses (Section on Breastfeeding, 2012). The health of an infant may seem unrelated to the interests of an employer; however, infant health impacts corporate expenses and worker productivity. Parents of breastfed infants have half as many 1-day absences as parents of formula-fed infants, producing up to US$60,000 in cost savings related to absenteeism for some employers (U.S. Department of Health and Human Services [USDHHS], 2008). Corporate lactation programs (CLP), which promote and facilitate BF in the workplace, have aided some employers in decreasing their health care costs by US$240,000 as employees typically use fewer insurance benefits for their infants (USDHHS, 2008). Employee retention is also higher among companies with CLPs (94.2% retention rate compared with the national average of 59%; USDHHS, 2008). Retention may result from employees feeling supported in their parental roles and creating positive perceptions of and increasing loyalty to employers (USDHHS, 2008).
In response to low BF duration rates, the U.S. Congress enacted Section 4207 of the Patient Protection and Affordable Care Act (PPACA), which included the “Break Time for Nursing Mothers” law of 2010 (Garvin et al., 2013; United States Breastfeeding Committee [USBC], 2013). This law requires companies with 50 or more employees to provide reasonable time and a private secure space, other than a bathroom, to express milk. Employees who are paid hourly and covered by the Fair Labor Standards Act (FLSA) are eligible for lactation breaks for up to 1 year after the birth of a child (Garvin et al., 2013; USBC, 2013). Employers with less than 50 employees can apply for exemption from the law if allowing milk expression breaks causes insurmountable disruptions to work-flow (Garvin et al., 2013; USBC, 2013). National public health initiatives also reinforce the need for workplace lactation support. Healthy People 2020 Objective Maternal, Infant, Child Health (MICH-22) sets a goal of increasing the percentage of employers offering CLPs from 25% to 38% (USDHHS, 2016).
Research has supported the role of health care professionals, such as occupational health nurses and certified lactation consultants (LCs), in promoting, facilitating, and administering worksite lactation benefits and CLPs (Rietz & McCullagh, 2010). Occupational health nurses can lead the following initiatives critical for a CLP: develop workplace lactation policies, facilitate conversations between employees and employers regarding needed lactation accommodations, provide care and maintenance of lactation equipment and spaces, research liability insurance requirements and providers, promote CLPs and educate all employees about the benefits of BF, evaluate the program, maintain program records and conduct benefit analyses for program justification, and support BF mothers at the workplace (Mills, 2009; Ortiz, McGilligan, & Kelly, 2004; Rietz & McCullagh, 2010).
A gap in the available literature is a summary of the association between various workplace lactation accommodations and BF duration in working mothers who use the accommodations. The purpose of this review was to examine data regarding the impact of workplace lactation accommodations on BF duration. Another purpose was to identify which accommodations are consistently associated with longer BF duration and identify areas for improvement. The answers to these questions are of benefit to various occupational health professionals as the accommodations may optimize the effectiveness of current programs and facilitate development of comprehensive new programs. As the relationship between BF duration, parental leave, and employment status are well documented in the literature, those factors will not be addressed in this review.
Method
The authors conducted a literature review using PubMed and CINAHL databases. Search terms included workplace lactation support, workplace BF duration, BF and employment, and workplace BF. Inclusion criteria for this review were (a) article written in English, (b) data collected in the United States, (c) examination of individual worksite lactation accommodations or a CLP, (d) availability of descriptive and/or inferential statistics on BF duration in women using worksite accommodations or a CLP, and (e) published between 1985 and 2015. Studies conducted outside the United States were excluded to ensure findings reflected the unique cultural and workplace environment and BF practices in the United States. Studies published more than 5 years previous to the review were included to provide historical context to current research. These studies also form the foundation for current knowledge about best practices for supporting BF in the workplace.
Articles were excluded if they were not based on U.S. data; did not relate to workplace lactation accommodations; did not relate to BF; were commentaries, editorials, reviews, news briefs, or training modules; were focused on employers’ responses to BF, the development of workplace BF assessment tools, or discussions of theory; and did not compare BF duration with use of lactation accommodations or a CLP. Articles that focused on the association between maternity leave and full- or part-time work status and BF duration were also not included in this analysis as the focus of this research is on the impact of the work environment on BF duration. To gain understanding of barriers to workplace BF, qualitative studies focusing on women’s experiences combining BF and working were also reviewed. However, these studies were not included in the analyses as they did not provide numerical data on the association between BF duration and lactation accommodations.
One author searched the databases and reviewed abstracts and full texts for literature meeting the inclusion criteria during June and July of 2015. Using PRISMA Analysis, quantitative analyses of workplace lactation accommodations and their association with BF duration were reviewed, and associations were noted in tabular form. Correlations and p values were included in the tables and are representative of their presentation in original studies.
Results
The search terms identified 1,030 references in PubMed and 481 references in CINAHL (Figure 1). After duplicates were removed, 981 references remained. From these, 910 were excluded based on the title or brief abstract because they were not based on U.S. data, did not relate to workplace accommodations, or did not relate to BF. Full-text articles for the remaining 71 references were closely reviewed for eligibility. Upon review of the abstracts, additional 60 articles were excluded because they were commentaries/editorials; practice papers, reviews, or conference proceedings; discussed only theory; international; presented only qualitative data; did not compare BF duration with lactation accommodations; focused on the development of assessment tools; or reviewed only parental leave. Eleven articles (Alvarez, Serwint, Levine, Bertram, & Sattari, 2015; Bai & Wunderlich, 2013; Balkam, Cadwell, & Fein, 2011; Cohen & Mrtek, 1994; Dabritz, Hinton, & Babb, 2009; Hills-Bonczyk, Avery, Savik, Potter, & Duckett, 1993; Jacknowitz, 2008; Katcher & Lanese, 1985; Ortiz et al., 2004; Sattari, Serwint, Neal, Chen, & Levine, 2013; Waite & Christakis, 2015) met study inclusion criteria and were reviewed (Table 1).
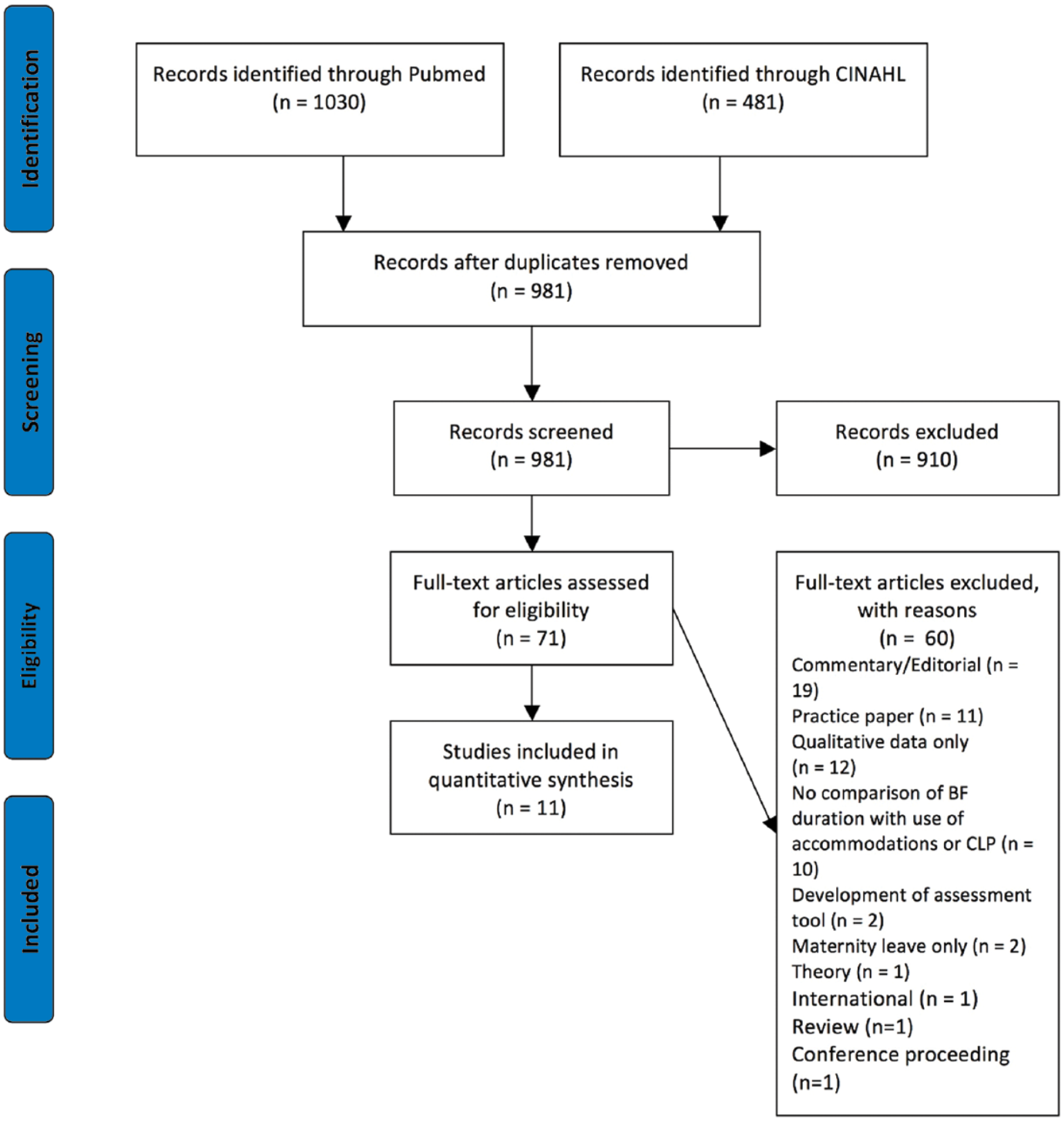
PRISMA flow diagram for workplace lactation accommodations review.
Results of Quantitative Studies Examining the Effect of Workplace Lactation Accommodations on BF Duration
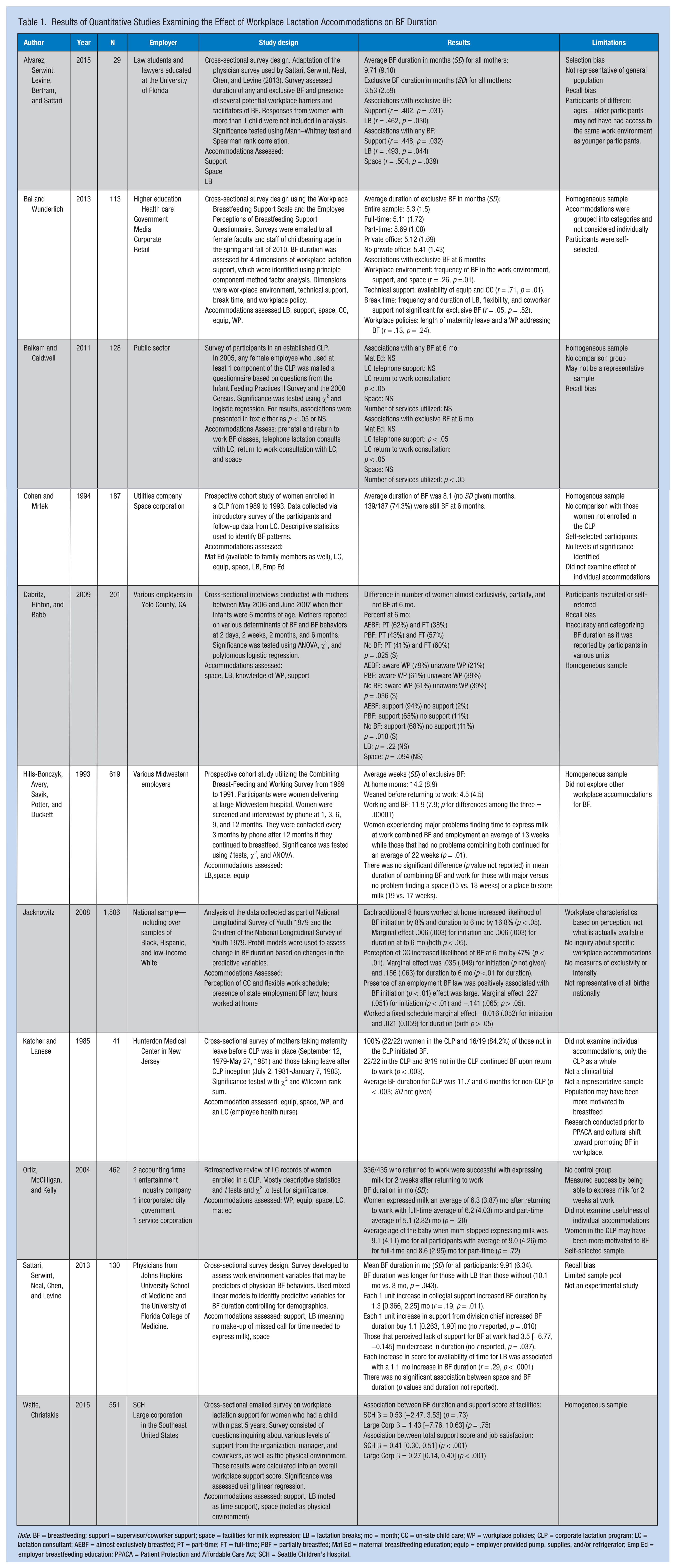
Note. BF = breastfeeding; support = supervisor/coworker support; space = facilities for milk expression; LB = lactation breaks; mo = month; CC = on-site child care; WP = workplace policies; CLP = corporate lactation program; LC = lactation consultant; AEBF = almost exclusively breastfed; PT = part-time; FT = full-time; PBF = partially breastfed; Mat Ed = maternal breastfeeding education; equip = employer provided pump, supplies, and/or refrigerator; Emp Ed = employer breastfeeding education; PPACA = Patient Protection and Affordable Care Act; SCH = Seattle Children’s Hospital.
Five of the 11 identified studies were cross-sectional surveys (Alvarez et al., 2015; Bai & Wunderlich, 2013; Dabritz et al., 2009; Sattari et al., 2013; Waite & Christakis, 2015). One article was a prospective cohort study of various employers regarding the availability and use of lactation accommodations compared with BF duration among female employees (Hills-Bonczyk et al., 1993). Two studies were cross-sectional surveys of participants in a CLP (Balkam et al., 2011; Katcher & Lanese, 1985). Other articles described a prospective cohort study of participants in a CLP (Cohen & Mrtek, 1994), a retrospective record review of participants in a CLP (Ortiz et al., 2004), and an analysis of national data that included questions about workplace lactation accommodations (Jacknowitz, 2008). No clinical trials or experimental studies were identified.
Accommodations studied and their associations with BF duration are summarized in Table 2. Accommodations were grouped into six categories (i.e., support, education, access to infant, milk expression, policy, and availability of a CLP) to simplify data presentation. As noted in Table 2, the methods used to measure BF duration varied among studies. Several studies measured any or exclusive BF at 6 months; other studies examined total BF duration.
Summary of Workplace Lactation Accommodations and Association With BF Duration
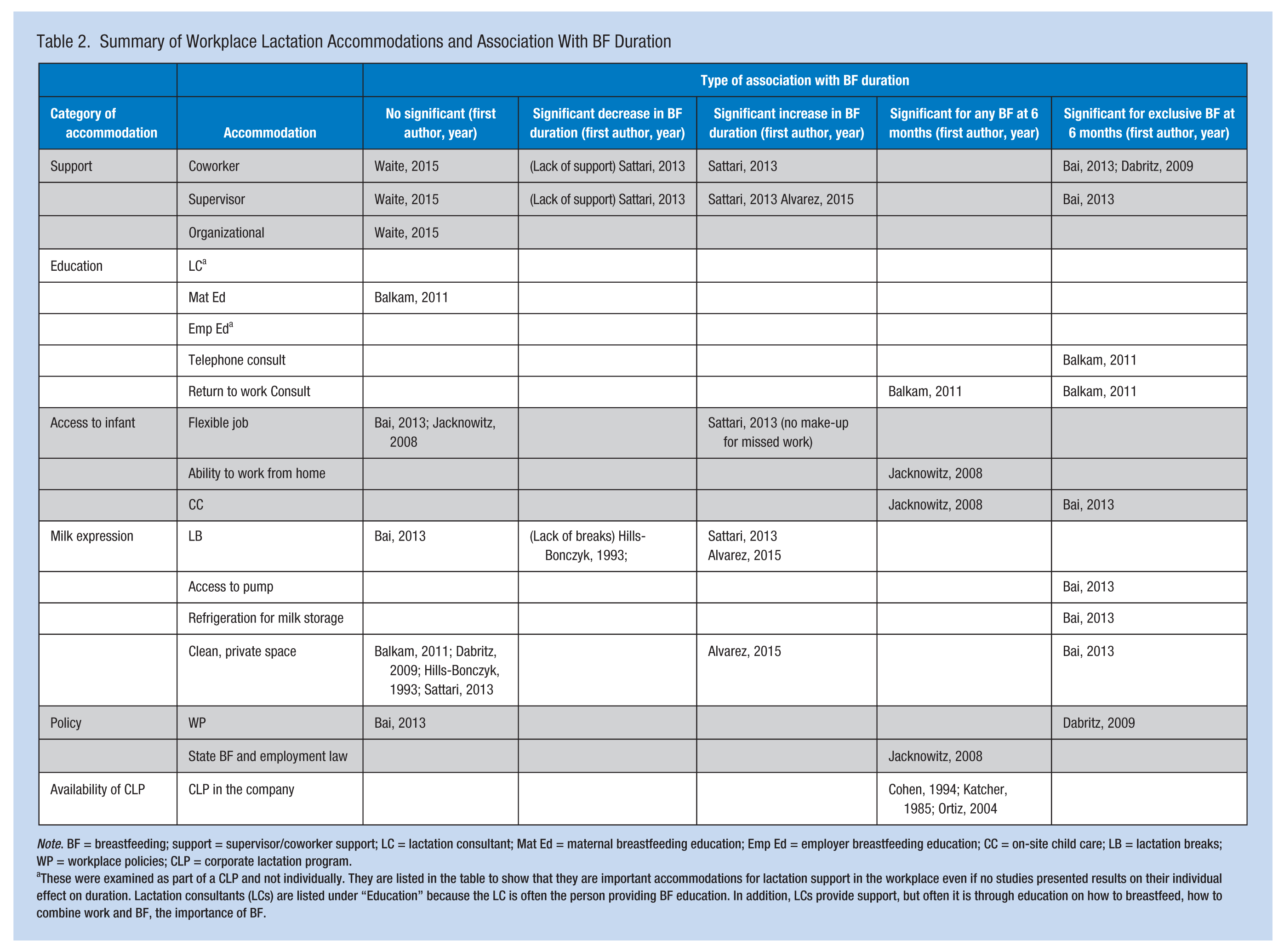
Note. BF = breastfeeding; support = supervisor/coworker support; LC = lactation consultant; Mat Ed = maternal breastfeeding education; Emp Ed = employer breastfeeding education; CC = on-site child care; LB = lactation breaks; WP = workplace policies; CLP = corporate lactation program.
These were examined as part of a CLP and not individually. They are listed in the table to show that they are important accommodations for lactation support in the workplace even if no studies presented results on their individual effect on duration. Lactation consultants (LCs) are listed under “Education” because the LC is often the person providing BF education. In addition, LCs provide support, but often it is through education on how to breastfeed, how to combine work and BF, the importance of BF.
In general, the presence of a CLP promoted BF at 6 months (Cohen & Mrtek, 1994; Katcher & Lanese, 1985; Ortiz et al., 2004), as did on-site child care (Bai & Wunderlich, 2013; Haider, Jacknowitz, & Schoeni, 2003). Of the three studies examining CLPs, the average BF duration for employees using the program was 8.1 months (Cohen & Mrtek, 1994), 11.7 months (Katcher & Lanese, 1985), and 9.1 months (Ortiz et al., 2004), respectively. Only Katcher and Lanese (1985) included a comparison group to identify differences in BF duration between employees enrolled in the CLP and those study participants not enrolled (11.7 months for the CLP vs. 6 months for non-CLP, p < .003). This study was conducted before U.S. workplace lactation laws went into effect. With regard to on-site child care, one study found that the perception of available on-site child care significantly increased the likelihood of BF at 6 months by 47% (p < .01; Jacknowitz, 2008). In the second study, factor analysis was used to develop four dimensions of BF accommodations. The dimension of technical support, which included on-site child care, was significantly positively associated with BF duration (r = .71, p = .01; Bai & Wunderlich, 2013). Telephone and return to work consultations with an LC were examined in only one article and significantly positively associated with any and exclusive BF at 6 months (p < .05; Balkam et al., 2011). Other accommodations examined in the literature had inconsistent associations with BF duration.
In four studies (Alvarez et al., 2015; Bai & Wunderlich, 2013; Dabritz et al., 2009; Sattari et al., 2013), coworker and supervisor support for BF was significantly positively associated with overall BF duration and exclusive BF at 6 months (p = .032, .01, .018, .011, respectively); one study (Waite & Christakis, 2015) did not find any significant association between coworker and supervisor support and BF duration at either of two study sites (p = .73 and .75). In addition, one study found that the perception of unsupportive colleagues was significantly associated with a 3.5-month decrease in BF duration (no r value reported, p = .037; Sattari et al., 2013).
Lactation spaces for milk expression and lactation breaks were not consistently associated with BF duration. Two studies (Alvarez et al., 2015; Bai & Wunderlich, 2013) examining availability of a lactation space found a significant positive association with BF duration (r = .504 and .26, p = .039 and .01, respectively), but the other four (Balkam et al., 2011; Dabritz et al., 2009; Hills-Bonczyk et al., 1993; Sattari et al., 2013) found no significant association with BF duration (p = NS, .094, and two are not reported, respectively). Lactation breaks were not consistently associated with BF duration either. Two studies (Alvarez et al., 2015; Sattari et al., 2013) found a significant positive association with total BF duration (r = .493 and .29 and p = .044 and < .001, respectively); one study (Bai & Wunderlich, 2013) found no significant association (r = .05, p = .52). In addition, one study found that women who could not find time to express milk during the workday had significantly shorter BF duration than those reporting no problems finding time to express (13 weeks vs. 22 weeks total duration, p = .01; Hills-Bonczyk et al., 1993).
Worksite policies were examined in two studies (Bai & Wunderlich, 2013; Dabritz et al., 2009) with differing results. One (Dabritz et al., 2009) found that a worksite policy was significantly associated with any BF at 6 months (p = .036) while the other (Bai & Wunderlich, 2013) found no significant association between worksite policy and exclusive BF at 6 months (r = .13, p = .24). One study conducted prior to enactment of the 2010 PPACA reported a significant positive association between the presence of a state law regarding BF at work and any BF at 6 months (p < .01; Jacknowitz, 2008).
Discussion
This review identified several workplace BF accommodations that occupational health professionals can implement to promote BF among working mothers. Promising interventions include the presence of a CLP, on-site child care, and telephone and back-to-work consultations with an LC. Corporate lactations programs and on-site child care were shown to be consistently significantly associated with BF at 6 months in multiple studies; availability of an LC was only examined in one study. However, with three or fewer studies examining these three accommodations, generalizability of these findings is limited.
Many of the other accommodations were not consistently significantly associated with BF duration, and occupational health nurses may have a critical role in improving effectiveness. Although some of the inconsistent associations may have resulted from confounding variables such as lack of support from family and friends, low maternal self-efficacy for BF, personal or cultural beliefs about BF, and research design, worksite factors may contribute as well. Implementation of the accommodations may be a confounder, especially regarding adequacy of the accommodations, communication about and marketing of the accommodations, and supervisors and coworker encouragement for use of the accommodations.
Occupational health professionals can assure adequacy of accommodations by promoting current best practices, gathering feedback on accommodations, and monitoring the condition of physical facilities. In one study, participants reported that the designated lactation spaces were not adequately equipped to promote milk expression (Bai & Wunderlich, 2013). Interestingly, this study found a significant positive association between space and BF duration. A space for milk expression should be dedicated solely to lactation and have a locking door; be clean, private, and convenient to the worksite; be equipped with a power outlet, comfortable chair, sink, and refrigerator; and be available for use when mothers are ready to express (Eldridge & Croker, 2005; Marinelli, Moren, Taylor, & Medicine, 2013; Uriell, Perry, Kee, & Burress, 2009). An occupational health professional can assure spaces meet the recommended criteria and needs of mothers by providing feedback cards in the rooms, conducting ongoing surveys, and examining rooms for disrepair and inadequate hygiene.
BF employees may be hesitant to use accommodations without the support of supervisors and coworkers. Occupational health nurses can facilitate support for BF employees. Support from coworkers and supervisors is critical in promoting BF among working mothers (Bar-Yam, 1998a). The studies in this review found that support was significantly positively associated with longer BF duration (Alvarez et al., 2015; Bai & Wunderlich, 2013; Dabritz et al., 2009; Sattari et al., 2013); lack of support significantly shortened BF duration (Sattari et al., 2013). Qualitative studies and position papers have cited the importance of manager, coworker, and organizational support in promoting BF in the workplace as well (Bar-Yam, 1998b; O’Keefe & Henly, 1998). Encouragement from managers, coworkers, and the organization promotes taking lactation breaks, scheduling work hours around BF, and acceptance of working mothers’ decisions to work and breastfeed (Bar-Yam, 1998b). Occupational health professionals can improve supervisor and coworker support for BF by creating comprehensive workplace lactation policies, promoting BF throughout the worksite, providing education to all employees on the benefits of BF, and acting as a liaison between employees and supervisors in securing needed accommodations (Cohen & Mrtek, 1994; Mills, 2009; Ortiz et al., 2004; Rietz & McCullagh, 2010).
In many of the studies, it was unclear what information was provided to supervisors and coworkers to increase their support for BF. One study reported that managers were educated by corporate LCs on the needs of working, BF women (Ortiz et al., 2004). The purpose of this education was to assure managers that women’s participation in the program would not interfere with productivity and these women would only use their regular break schedule to express (Ortiz et al., 2004). This study was conducted prior to implementation of the PPACA in 2010. Education for employers should now include this legislation as well as any state or organizational policies mandating particular benefits. Managers and coworkers should also be aware of BF benefits, company lactation policies and available accommodations, and BF mothers’ need for support. Occupational health professionals can be instrumental in assuring effective BF education is provided to all employees.
Occupational health professionals can also facilitate communication in the workplace. Research shows that workplace communication about BF is limited (Anderson et al., 2015). Inadequate communication about workplace policies and availability of lactation breaks and spaces may limit use of the accommodations. Three of the studies examining the impact of a CLP on BF duration mentioned program promotion; however, they did not specifically describe the process of communicating about available accommodations and expectations for their use to BF employees. One study mentioned that the CLP was offered to all full-time, female employees (Ortiz et al., 2004) and another stated that women were informed about the CLP when they requested parental leave (Katcher & Lanese, 1985). The third simply mentioned that CLP promotion was more effective at one site than another (Cohen & Mrtek, 1994).
Only one study of a CLP mentioned that employees were offered return-to-work consultations with LCs and meetings with supervisors (Cohen & Mrtek, 1994). The supervisor meeting was included “to clarify any remaining issues regarding the maintenance phase of the lactation program” (Cohen & Mrtek, 1994), possibly meaning a discussion of the expectations for using breaks and accommodations. The relationship between employee–employer communication and BF duration was not considered in any of the studies. Occupational health nurses can address this challenge, as they are knowledgeable mediators able to speak on behalf of both parties.
As mentioned previously, occupational health nurses can establish employer-sponsored lactation programs (Rietz & McCullagh, 2010). If an employer has multiple barriers preventing implementation of a CLP, occupational health nurses could also assist in developing a work-from-home or flex-work program. Some research has shown that women who are able to work more hours from home, or are self- or non-formally employed, breastfeed longer than those in formal employment (Jacknowitz, 2008; Rivera-Pasquel, Escobar-Zaragoza, & González de Cosío, 2015; Roe, Whittington, Fein, & Teisl, 1999). These options could be less burdensome for employers, as it would only require mothers to have resources needed to do their jobs from home instead of altering work environments.
Future research should focus on the interactions between the amenities included in lactation rooms, the rooms’ proximity to mothers’ work stations (Hojnacki, Bolton, Fulmer, & Olson, 2012), whether rooms are designated for lactation, and supervisors’ and coworkers’ promotion of, and support for, use of spaces, and BF duration. In addition, more insight into BF education provided to employers and employees, the educational methods used, and the impact on BF duration may also be beneficial. Communication between employee and employer regarding needed lactation accommodations and recommendations for best practices may also be a critical area of research for the future. Evaluative research should focus on absenteeism among BF employees, use of health care benefits for infants, total length of BF duration, and changes in normative perceptions of BF in the workplace to demonstrate benefits of the program to the employer. Finally, if occupational health nurses have opportunities to initiate CLPs, data on BF prevalence and duration should be collected before and after programs are implemented for comparison.
Several research limitations have been identified for this review. First, none of the identified studies were experimental. Many had small, homogeneous samples. Several of the studies included mostly White (Bai & Wunderlich, 2013; Balkam et al., 2011; Jacknowitz, 2008; Ortiz et al., 2004; Waite & Christakis, 2015), college-educated women (Alvarez et al., 2015; Bai & Wunderlich, 2013; Balkam et al., 2011; Dabritz et al., 2009; Hills-Bonczyk et al., 1993; Jacknowitz, 2008; Sattari et al., 2013; Waite & Christakis, 2015) who were above 30 years of age (Alvarez et al., 2015; Balkam et al., 2011; Jacknowitz, 2008; Ortiz et al., 2004; Sattari et al., 2013), and married (Alvarez et al., 2015; Bai & Wunderlich, 2013; Balkam et al., 2011; Hills-Bonczyk et al., 1993; Jacknowitz, 2008; Sattari et al., 2013; Waite & Christakis, 2015). Research suggests that BF duration is longer in women who fit these demographic characteristics (Chin, Myers, & Magnus, 2008; Persad & Mensinger, 2008; Ryan & Martinez, 1989). In addition, this group of women may be more motivated to participate in research studies and thus be over-represented. Recall bias could have also been an issue with several studies (Bai & Wunderlich, 2013; Balkam et al., 2011; Dabritz et al., 2009; Katcher & Lanese, 1985; Sattari et al., 2013; Waite & Christakis, 2015). BF duration was defined in different ways among the identified studies. In addition, the authors found a lack of research conducted in the United States that examined the association between, or effect of, lactation accommodations on BF duration, so this review is based on very limited data. Finally, some studies included in the review were more than 5 years old; these studies may not reflect current workplace BF practices.
In Summary
Workplace BF accommodations may have the potential to extend BF duration for the working mother.
Occupational health professionals should promote BF by assuring that a well-written lactation policy is in place and fully implemented, maintaining equipped lactation facilities, increasing communication about and marketing of BF, and supporting working BF mothers.
Future research should include type and impact of BF education provided to all employees; best practices for BF communication and how to facilitate communication between employers and employees; the impact that education and communication has on BF duration; and comparison of BF duration among employees before and after implementation of a CLP.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Elizabeth Dianne Hilliard is a registered dietitian and an assistant professor of practice at North Dakota State University in Fargo, North Dakota. She is currently pursuing a PhD in exercise science and nutrition with a research focus on promoting breastfeeding in the workplace.