
Abstract
Background:
There are numerous health benefits related to high adherence to the Mediterranean diet (MedDiet), providing a protective effect against cardiometabolic diseases, but there are very few MedDiet studies conducted in the workplace. Therefore, the purpose of this systematic review is to analyze the effectiveness of MedDiet workplace interventions on cardiovascular risk factors.
Methods:
Studies were identified in four databases: PubMed, Scopus, Web of Science, and CINAHL, published from the earliest time point until 15 May 2021. The inclusion criteria were (a) adults aged 18 to 70 years; (b) MedDiet intervention only; (c) intervention was conducted in a workplace; and (d) the outcomes included measurement of cardiometabolic biomarkers. Exclusion criteria were (a) abstract not in English; (b) full-text non-available; and (c) review articles. Ninety-five studies were retrieved and assessed for inclusion by two independent reviewers, who also used the Cochrane Collaboration Tool to assess study quality and risk of bias.
Results:
Five high-quality studies were included (n = 436, 89% male). MedDiet interventions carried out within the workplace were effective in improving cardiovascular risk factors such as lipid profile and insulin sensitivity compared with a low-fat diet, especially among obese participants. Blood pressure and inflammatory markers were not improved after the MedDiet interventions.
Conclusions:
Worksite occupational health teams should consider promoting MedDiet by conducting regular nutritional sessions and providing tailored menus in workplace cafeterias. However, more high-quality studies are necessary to bring more evidence to this topic.
Background
The Mediterranean diet (MedDiet) is characterized by consumption of foods that are high in monounsaturated fatty acids (MUFA), polyunsaturated fatty acids (PUFA), polyphenols, and fiber; as well as low in saturated fat, red meat, and salt (Rees et al., 2019). There are numerous health benefits related to adherence to the MedDiet, including lower systemic inflammation, (Sureda et al., 2018; Yarla et al., 2018) lower DNA oxidative damage (Schwingshackl et al., 2015, 2017; Sies, 2015), greater insulin sensitivity, lower blood pressure, healthier lipid profile, and improved endothelial function (Garcia-Arellano et al., 2015; Saklayen, 2018; Schwingshackl & Hoffmann, 2014; Tresserra-Rimbau et al., 2014), providing a protective effect against cardiometabolic diseases (Estruch et al., 2018; Minelli & Montinari, 2019). However, there is little evidence of association between MUFA intake, total fat intake, PUFA intake, saturated fat intake, and cardiovascular risk, in contrast to popular beliefs (Clifton & Keogh, 2017). There is evidence of a small (5%) decrease in cardiovascular risk in individuals with high PUFA intake in studies with a 10-year follow-up period (Zhu et al., 2019). Similarly, MedDiet interventions have minimal effect on reducing cardiovascular mortality and improving lipid profile, and a moderate effect on reducing heart attacks and lowering blood pressure (Rees et al., 2019).
Despite the beneficial health effects traditionally attributed to the MedDiet, more randomized controlled trials (RCT) are necessary to obtain scientific evidence about the effectiveness of MedDiet interventions on cardiometabolic health. The MedDiet should be promoted in all age groups since health risk factors develop from childhood (Shrestha, 2015). However, the work environment is very appropriate to promote healthy lifestyle habits such as adherence to the MedDiet, due to the high number of hours spent in the workplace. Therefore, the investigators considered a review of MedDiet interventions in the workplace to be timely and relevant. Prior to this review there was only one narrative review which included relative few low quality intervention studies (Korre et al., 2014).
Therefore, our objective was to analyze the effectiveness of MedDiet interventions carried out in the workplace on cardiovascular risk factors.
Methods
This systematic review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Moher et al., 2009).
Studies were identified in four databases: PubMed, Scopus, Web of Science, and CINAHL, published from the earliest time point until 15 May 2021. The search terms were “Mediterranean Diet and (Worksite OR Workplace).” Gray literature (e.g., abstracts, conference proceedings, and editorials) and reviews were excluded. After the duplicates were removed, two authors (G.G.P.S. and B.S.P.P.) independently screened the titles and abstracts and then evaluated the full text of potentially relevant studies. The criteria for inclusion were (a) population: men or women aged between 18 and 70 years old; (b) type of intervention: a MedDiet intervention only; (c) intervention was carried out in the workplace; and (d) the outcomes included short term or long-term measurement of cardiometabolic biomarkers. Finally, the exclusion criteria were (a) abstract not in English; (b) full-text non-available; (c) review articles. All studies that were removed were recorded, with the reasons of exclusion. Only 5% of the studies initially identified met the selection criteria.
Data Extraction
Full-text articles were retrieved for all studies matching the inclusion criteria. They were stored electronically and systematically reviewed. Pre- and post-intervention mean and standard deviation of demographic variables (age, gender) and cardiometabolic biomarkers outcomes were extracted and recorded using a spreadsheet, by two authors (G.G.P.S. and B.S.P.P.). The characteristics of the MedDiet interventions, the type of workplace, and the characteristics of the occupational health unit were also extracted and recorded. Characteristics of studies, interventions, and participants were summarized in tables. Revised Cochrane risk-of-bias tool for randomized trials (RoB 2) (Sterne et al., 2019) was used to assess the following characteristics: (a) bias arising from the randomization process; (b) bias due to deviations from intended interventions; (c) bias due to missing outcome data; (d) bias in measurement of the outcome; (e) bias in selection of the reported result. Two investigators (G.G.P.S. and B.S.P.P.) performed separate assessments of risk-of-bias. We did not perform a meta-analysis because there were not enough variables in common in the studies analyzed.
Results
The search strategy identified 95 articles from electronic databases. Following removal of duplicates, 40 articles were initially screened via title and abstract, and 10 were identified as potentially relevant. Full-text examination further excluded six articles, leaving five articles for inclusion in this analysis, all were RCTs except one, and two articles reported on different outcomes from the same study (Figure 1).
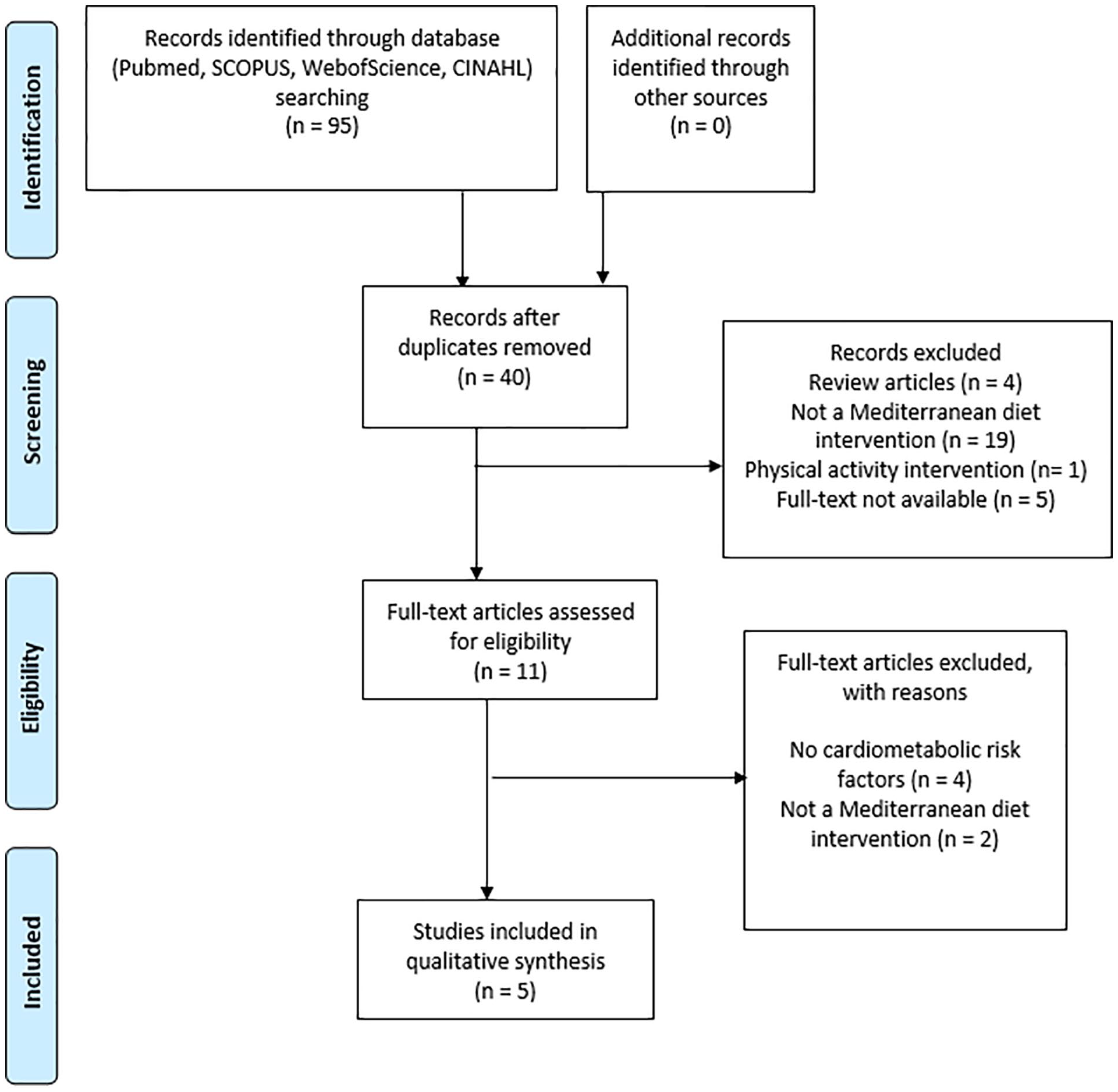
Preferred reporting items for systematic reviews and meta-analyses flow diagram for study selection.
Participant demographics, intervention characteristics and cardiometabolic outcomes are outlined in Table 1. Five articles, two about the same study, examined cardiometabolic outcomes in 436 middle-aged adults (range = 39–52 years) (89% male), most (%) of them obese/overweight. Participants were U.S. firefighters from the Indianapolis Fire department (Sotos-Prieto et al., 2020), employees in a nuclear research center in Israel (Gepner et al., 2018; Schwarzfuchs et al., 2012; Shai et al., 2008), and office workers and technical personnel from a heavy machinery maintenance and repair company for the mining industry in Chile (Leighton et al., 2009).
Participants Demographics, Program Characteristics, and Cardiometabolic Risk Outcomes for Included Studies
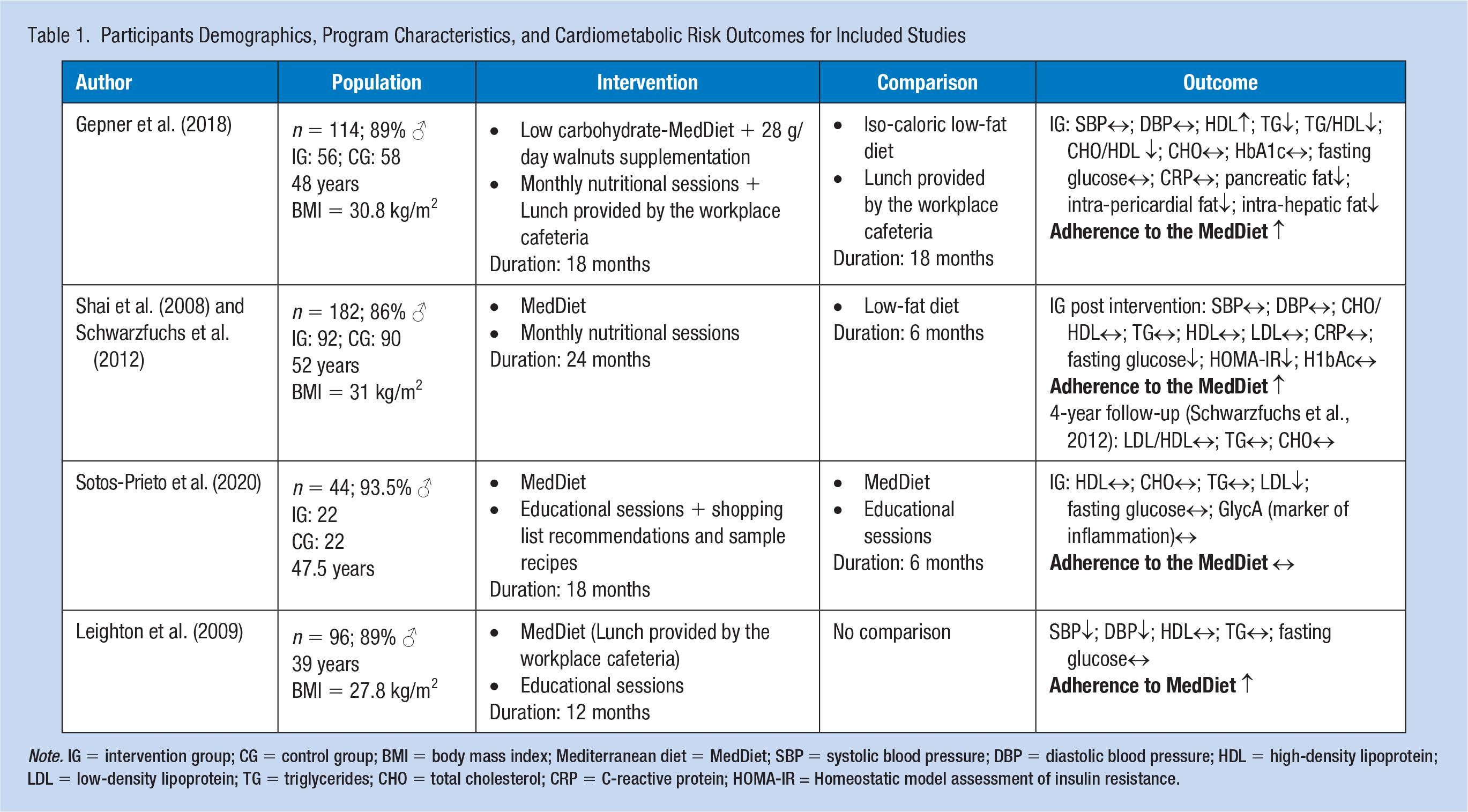
Note. IG = intervention group; CG = control group; BMI = body mass index; Mediterranean diet = MedDiet; SBP = systolic blood pressure; DBP = diastolic blood pressure; HDL = high-density lipoprotein; LDL = low-density lipoprotein; TG = triglycerides; CHO = total cholesterol; CRP = C-reactive protein; HOMA-IR = Homeostatic model assessment of insulin resistance.
Interventions
In three studies, the MedDiet intervention consisted of monthly group nutritional sessions of 90 minutes each, as well as motivational telephone calls. These interventions were carried out by dietitians, who also worked closely with the kitchen staff to adjust specific food items. The duration of these interventions was 24 months (Schwarzfuchs et al., 2012; Shai et al., 2008) and 18 months (Gepner et al., 2018). In addition, in the study conducted by Gepner et al. the participants were provided with tailored menus at the workplace cafeteria. In the study carried out on U.S. firefighters, the MedDiet intervention consisted of monthly group educational sessions, educational materials delivered via website, text message encouragement, and discounted access to healthy foods consistent with the MedDiet. This intervention lasted for 12 months (Sotos-Prieto et al., 2020). Finally, in the study carried out on heavy machinery maintenance and repair workers, the MedDiet intervention consisted of a MedDiet-based menu at the workplace canteen 5 days a week during 12 months, and group educational sessions led by nutritionists with personal nutritional advice every 4 months (Leighton et al., 2009).
In all of the studies, the educational sessions talked about the advantages of consuming MedDiet for the prevention of chronic diseases, and the employees received recommendations for the application of this diet in their household.
Only one study performed a long-term (4 years) post-intervention analysis (Schwarzfuchs et al., 2012).
Type of Occupational Health Unit
In the study carried out on U.S. firefighters (Sotos-Prieto et al., 2020), the MedDiet intervention was led by Harvard investigators, the Public Safety Medical Services of Indianapolis, and a registered dietitian.
In the studies carried out on workers of a nuclear research center in Israel, which had an on-site medical clinic, the MedDiet intervention was carried out by dietitians, and all the outcomes were assessed by the doctors of the on-site medical clinic (Gepner et al., 2018; Schwarzfuchs et al., 2012; Shai et al., 2008).
Finally, in the study carried out on heavy machinery maintenance and repair workers, the MedDiet intervention was carried out by a nutritionist, with additional support from the industrial workers’ safety organization ACHS (Asociacion Chilena de Seguridad).
Outcome Measures
All the studies obtained fasting blood samples to measure the lipid profile, the glycemic profile, as well as inflammatory biomarkers. In addition, one study (Gepner et al., 2018) performed a magnetic resonance imaging scan to assess body fat depots.
Results
The outcomes extracted from this review were the following: Adherence to the MedDiet assessed with the Food-Frequency Questionnaire (FFQ), PREDIMED score (Martínez-González et al., 2012), and modified MedDiet Score; and cardiometabolic biomarkers, which were grouped into three different categories according to the objective of the study: (a) Lipid profile: high-density lipoprotein (HDL), low-density lipoprotein (LDL), total cholesterol (CHO), triglycerides (TG), CHO/HDL, TG/HDL; (b) Glycemic profile, Blood pressure, and inflammation: glucose, H1bAc, systolic blood pressure (SBP), diastolic blood pressure (DBP), C-reactive protein, GlycA; (c) Ectopic fat: pancreatic fat, intra-pericardial fat, intra-hepatic fat (Figure 2).
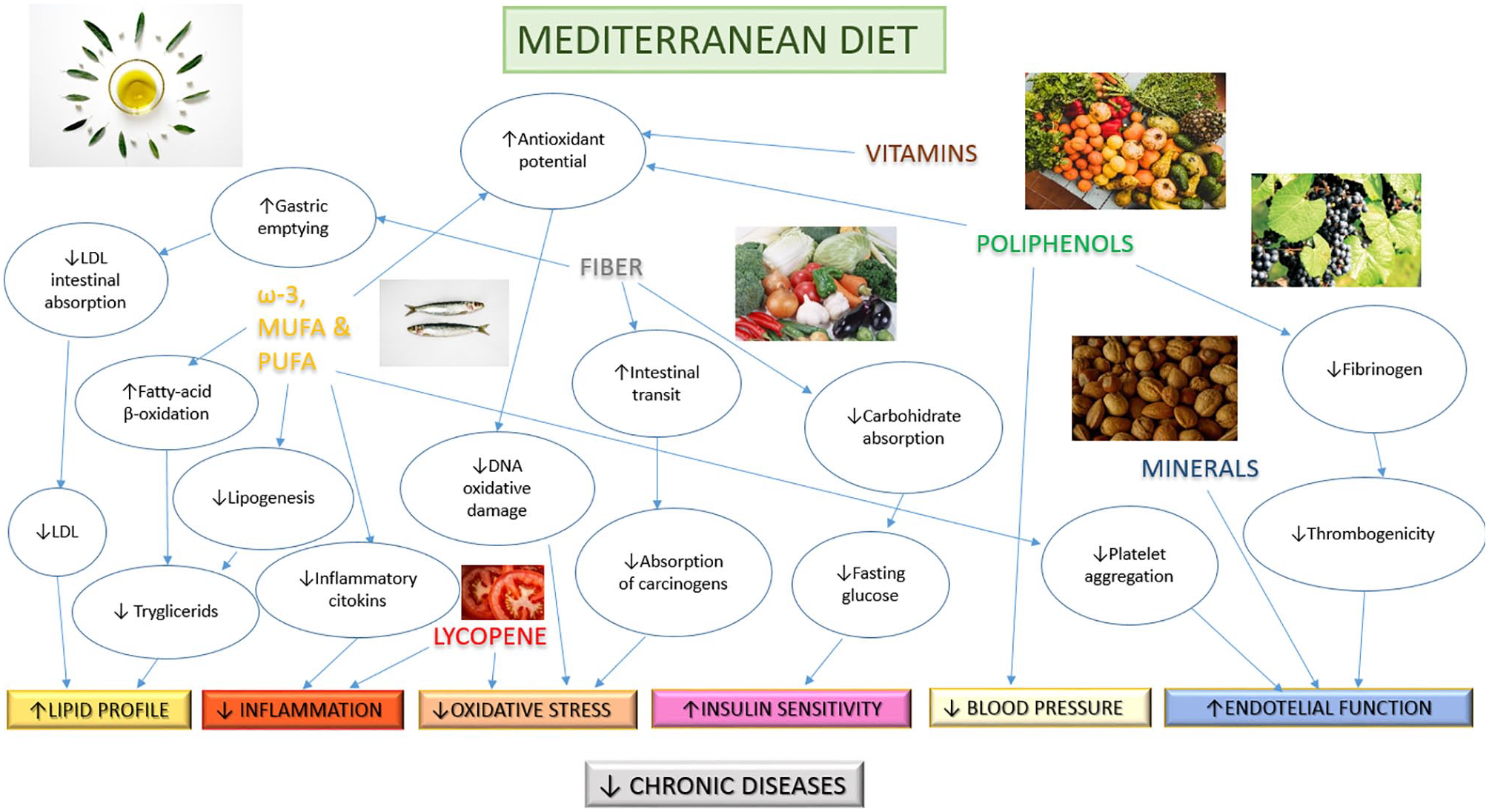
Summary of beneficial health effects of the MedDiet, which prevents the development of chronic diseases (Estruch et al., 2018; Garcia-Arellano et al., 2015; Minelli & Montinari, 2019; Saklayen, 2018; Schwingshackl et al., 2015, 2017; Schwingshackl & Hoffmann, 2014; Sies, 2015; Sureda et al., 2018; Tresserra-Rimbau et al., 2014; Yarla et al., 2018).
Quality assessment of study methodology
The risk of bias analysis revealed that the four RCTs (Gepner et al., 2018; Schwarzfuchs et al., 2012; Shai et al., 2008; Sotos-Prieto et al., 2020) (100%) included presented low risk in the five domains. The quasi-experimental study (Leighton et al., 2009), in the absence of a control group, presented a high risk of bias.
Adherence to the MedDiet
Two studies (Gepner et al., 2018; Shai et al., 2008) observed improvements in the adherence to the MedDiet according to the FFQ, as the participants increased the consumption of monounsaturated fatty acids (MUFA), polyunsaturated fatty acids (PUFA), fiber, and reduced the intake of carbohydrates, saturated fat, trans fat, and dietary cholesterol; one study (Leighton et al., 2009) observed improvements in the adherence to the MedDiet according to the PREDIMED score, while one study (Sotos-Prieto et al., 2020) observed no changes in this regard (Table 1).
Lipid profile
HDL and TG showed a statistically significant decrease in one study (Gepner et al., 2018) and a maintenance in the other three (Leighton et al., 2009; Shai et al., 2008; Sotos-Prieto et al., 2020). Regarding LDL, one study (Sotos-Prieto et al., 2020) reported a significant decrease, while another (Shai et al., 2008) did not. The two studies that analyzed total cholesterol (Gepner et al., 2018; Sotos-Prieto et al., 2020) reported no changes in this variable. A significant decrease was observed in TG/HDL ratio in the only study that analyzed this variable (Gepner et al., 2018). Finally, a significant reduction in the CHO/HDL ratio was observed by one study (Gepner et al., 2018) and a maintenance in this variable by another one (Shai et al., 2008) (Table 1).
Glycemic profile, blood pressure, and inflammation
No changes were observed concerning H1bAc, C-reactive protein, (Gepner et al., 2018; Shai et al., 2008), and GlycA (Sotos-Prieto et al., 2020) in the studies analyzed. Regarding fasting glucose and Homeostatic model assessment of insulin resistance (HOMA-IR), one study (Shai et al., 2008) reported a significant decrease, but no changes were observed regarding glycemic profile in the other studies included in this review (Gepner et al., 2018; Leighton et al., 2009; Sotos-Prieto et al., 2020). Regarding systolic and diastolic blood pressure, only the quasi-experimental study (Leighton et al., 2009) reported a significant decrease (Table 1).
Ectopic fat
Gepner et al. (2018) reported a significant decrease in pancreatic fat, intra-pericardial fat, and intra-hepatic fat.
Discussion
The two studies (Gepner et al., 2018; Shai et al., 2008) that compared a MedDiet intervention with a low-fat diet intervention reported an increase in the adherence to the MedDiet of the participants, and an improvement of the lipid profile (Gepner et al., 2018) and the insulin sensitivity (Shai et al., 2008), thus reducing the cardiometabolic risk of the participants, who were mostly obese. The study that compared a long MedDiet intervention, 18 months, with a short one, 6 months, did not achieve significant improvements in terms of cardiometabolic risk factors, nor did it manage to increase the adherence to the MedDiet of the participants.
In the studies analyzed, an increase in adherence to the MedDiet, without implying a reduction in body weight, was associated with greater insulin sensitivity (Shai et al., 2008), healthier lipid profile (Gepner et al., 2018; Leighton et al., 2009), lower ectopic fat (Gepner et al., 2018), and therefore lower cardiometabolic risk. These findings are in line with the results previously reported in epidemiological studies (Garcia-Arellano et al., 2015; Saklayen, 2018; Schwingshackl & Hoffmann, 2014; Sureda et al., 2018; Tresserra-Rimbau et al., 2014; Yarla et al., 2018) and two meta-analyses (Potì et al., 2019; Rees et al., 2019).
The participants analyzed in this systematic review were middle-aged, mainly men. In the two studies that reported positive effects (Gepner et al., 2018; Shai et al., 2008) on cardiometabolic health, the participants were obese, and presented high levels of total cholesterol and fasting glucose. Possibly, these participants were more sensitive to the beneficial effects of the MedDiet (Engin, 2017; Vekic et al., 2019; Yazıcı & Sezer, 2017). Sotos-Prieto et al. did not report the body mass index of the participants who were firefighters. Leighton et al. achieved a significant reduction in both systolic and diastolic blood pressure, but there was not a control group, so these improvements cannot be attributed to the intervention.
Reducing obesity is a very complex task, as most of the studies that provide nutrition and exercise interventions in the obese population are not effective in the long term since they are unable to maintain healthy lifestyle habits (Middleton et al., 2013). The clinical importance of reducing obesity lies in the fact that obesity is associated with higher chronic systemic inflammation and with increased insulin resistance, which predisposes to developing cardio-metabolic diseases (Asghar & Sheikh, 2017; Karczewski et al., 2018; Reilly & Saltiel, 2017; Sureda et al., 2018; Yarla et al., 2018). Obesity is also associated with numerous psychiatric disorders, including a decline in mental health (Avila et al., 2015).
The study carried out by Sotos-Prieto et al. was the only one that did not achieve significant results regarding adherence to the MedDiet. This study indeed took place in the United States, where the MedDiet is not part of its culture. The two studies conducted in Israel, within the Mediterranean basin, increased the consumption of monounsaturated fatty acids (MUFA), polyunsaturated fatty acids (PUFA), fiber, and reduced the intake of carbohydrates, saturated fat, trans fat, and dietary cholesterol in participants assigned to a MedDiet, in comparison with participants assigned to a low-fat diet. Despite not using a specific questionnaire for this purpose (Martínez-González et al., 2012), we consider that Gepner et al. and Shai et al. increased the adherence to the MedDiet, as did Leighton et al.
Only Gepner et al. achieved clinically significant improvements in the lipid profile, as they reported an increase in HDL levels, a decrease in TG / HDL and CHO / HDL levels, and a reduction of the ectopic fat, leading to a notable reduction in cardiovascular risk (Estruch et al., 2018; Minelli & Montinari, 2019). They compared a low carbohydrate-MedDiet with a low fat-diet group, and there were no differences in terms of weight loss between the two groups. In contrast, the other three studies (Leighton et al., 2009; Shai et al., 2008; Sotos-Prieto et al., 2020) performed an intervention with a traditional MedDiet. Furthermore, in the intervention carried out by Gepner et al. the participants were given a tailored lunch in the workplace cafeteria. Leighton et al. also provided a tailored lunch in the workplace cafeteria, but their intervention was shorter. The success of Gepner et al. could be due to the combination of a long intervention, the tailored lunch, and the type of diet (low carbohydrate-MedDiet).
The study carried out by Shai et al. was the only one reporting a significant reduction in fasting glucose and HOMA-IR, thus increasing insulin sensitivity, compared with a low-fat diet group, despite no difference in weight loss. Gepner et al. did not achieve these results, despite using a low-carbohydrate diet (Tara et al., 2020), even if both managed to increase adherence to the MedDiet in a similar way.
Regarding other cardiometabolic risk factors, inflammatory markers were not modified after the MedDiet interventions, in contrast to the results reported in other studies (Garcia-Arellano et al., 2015; Schwingshackl & Hoffmann, 2014; Sureda et al., 2018; Yarla et al., 2018). Only Leighton et al. achieved a significant reduction in blood pressure, but as there was not a control group, these results should be interpreted with caution.
The three studies that increased the adherence to the MedDiet (Gepner et al., 2018; Leighton et al., 2009; Shai et al., 2008) managed to reduce the cardiometabolic risk of the participants.
Regarding the comparison group, Sotos-Prieto et al. compared two MedDiet interventions of different duration, while Gepner et al. and Shai et al. compared a MedDiet versus a low-fat diet, which could explain why the results reported by the latter two were more clinically relevant.
The limitations of this systematic review include that all the positive results were observed in obese/overweight patients, so they cannot be extrapolated to normal-weight populations. Furthermore, only four studies met the inclusion criteria, three being randomized controlled trials, so it was impossible to perform a meta-analysis to quantify the effect size. Finally, the four studies did not use the same instrument for assessing adherence to the MedDiet.
The strengths of this systematic review include the long duration of the follow-up period, 12 to 24 months, and that the interventions were performed in the workplace.
Despite the need for more quality studies in this field (Korre et al., 2014), these results add some evidence supporting MedDiet interventions conducted in the workplace to reduce cardiometabolic risk.
Implications for Occupational Health Practice
Long duration MedDiet interventions in the workplace improve cardiovascular risk factors such as lipid profile and insulin sensitivity compared with a low-fat diet. However, more high-quality studies are necessary to bring more evidence to this topic.
Therefore, company occupational health teams should consider providing MedDiet-based menus at workplace cafeterias, characterized by a high intake of fruit, vegetables, olive oil, seeds, and fish, and low intake of red meat, processed meat, and salt; as well as conducting regular nutritional sessions among their employees. Also, they should consider conducting regular nutritional sessions about the characteristics and beneficial effects of a healthy diet.
Footnotes
Author Contributions
G.G.P.S.: Writing and review of the drafts of the manuscript, acquisition, analysis, and interpretation of data, and approval of the final draft. B.S.P.P.: Design and conceptualization of the study, writing and review of the drafts of the manuscript, acquisition, analysis, and interpretation of data, and approval of the final draft. All Authors have read and accepted the submitted version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
PROSPERO Registration
This systematic review has been registered in PROSPERO (International prospective register of systematic reviews) on March 31, 2021, with the registration number CRD42021240008.
Author Biographies
Guillermo García Pérez de Sevilla: Physiotherapist, master’s degree in sports sciences, currently a professor at the Universidad Europea de Madrid (SPAIN), in the Faculty of sports sciences.
Beatriz Sánchez-Pinto Pinto: Physical medicine and rehabilitation physician, currently in the rehabilitation unit of the Puerta de Hierro Majadahonda University Hospital (SPAIN).