
Abstract
Hospital emergency preparedness has evolved in response to and been challenged by threats of terrorism, meteorological disasters, and public health emergencies. In this case study, the authors examined emergency preparedness policy and practice in Massachusetts hospitals following 9/11/2001, identifying areas of success and opportunities for improvement. Using a qualitative descriptive approach, data analysis included the examination of documents and public health policy. Snowball technique was used to recruit nurses, public health policy makers, and other first responder leaders with historical and present knowledge of emergency preparedness policy and practice. Content analysis identified emerging themes and lessons learned. Key findings included the importance of standardized training, the value of interprofessional collaboration and communication across organizations, and the impact of decreased funding and prior incidents. The lessons learned from this case study contribute to the evolving body of knowledge about emergency preparedness for all hospitals and public health facilities, and their community health partners. Emergency preparedness is a dynamic process, and as it continues to evolve, additional research will be needed to standardize training, encourage collaboration, and facilitate communication so that incident response by hospital professionals, including occupational health nurses, and their public health and community partners is more effective.
Dramatic changes in the health care landscape since the beginning of the 21st century are exemplified by the need for the U.S. health care system and public health professionals to respond effectively and efficiently to disasters. According to Blanchard (2008), emergency preparedness is defined by the Federal Emergency Management Agency (FEMA) as, “The discipline that ensures an organization or community’s readiness to respond to an emergency in a coordinated, timely, and effective manner to prevent the loss of life and minimize injury and property damage” (p. 373). This definition applies broadly across many domains including federal, state, and local government; all health care and public health disciplines; and emergency management and public safety entities. Emergency preparedness knowledge, training, and skills are critical for safe and effective disaster management in today’s health care environment. Health care providers’ education and training should prepare them to provide care during and after all-hazards incidents, and communicate and collaborate, working effectively with other first responders.
Background
An analysis of the nation’s response to the 9/11/2001 U.S. terrorist attacks revealed a lack of readiness and resilience to respond to future terrorist incidents (U.S. Department of Homeland Security, 2008). The government recognized the importance of equipping the nation with the tools and training necessary to respond to incidents in an organized, effective manner. Initially focusing on the management of terrorist attacks (e.g., chemical, biological, radiological, nuclear, and explosive [CBRNE] incidents), knowledge and skills about disaster preparedness have improved after responding to domestic and foreign terrorist incidents, pandemic influenza, and catastrophic weather events that include an all-hazards approach to every disaster. Using an all-hazards approach provides a common framework and promotes a common understanding and coordination among all responders.
The Department of Homeland Security (DHS) developed the National Response Framework (NRF) as the scaffolding for national-level policy, providing operational direction and effective federal support for incident management (U.S. Department of Homeland Security, 2008). Under this framework, the DHS developed the National Incident Management System (NIMS; U.S. Department of Homeland Security, 2009), a comprehensive, nationwide, systematic approach to incident management, including the use of the Incident Command System (ICS), multiagency coordination systems, and public information. The National Incident Management System includes essential preparedness principles for a common operating response among all first responders, influencing preparedness programs for health care providers in the public and private sector, public health, emergency management, and public safety arenas. Hospitals and health care systems receiving federal preparedness grants, contracts, or cooperative agreements must implement NIMS.
In 2002, the Department of Health and Human Services (DHHS) created the National Bioterrorism Hospital Preparedness Program. Renamed the Hospital Preparedness Program (HPP) in 2006, it has provided approximately US$400 million annually to support hospital preparedness (Levi, Segal, Lieberman, & Laurent, 2011) by enhancing the ability of U.S. hospitals and health care systems to prepare for and respond to threats and disasters of all types. The program provides grant funding to states, territories, and eligible municipalities to enhance community and hospital preparedness for public health emergencies (U.S. Department of Health and Human Services, 2014). The Office of the Assistant Secretary for Preparedness and Response (ASPR) provides programmatic oversight and, in Massachusetts, has partnered with the Massachusetts Department of Public Health to ensure the program’s goals are met. The HPP requires hospitals to provide leadership and systems to coordinate all major aspects of incident management (e.g., use the ICS, triage, victim stabilization, surge capacity, decontamination; meet behavioral health needs; and provide accountability and safety for all responders). With nurses and public health professionals as key participants, the program has evolved over time to include regional preparation and response capabilities under the Health and Medical Coordinating Coalitions (HMCC) representing formal regional collaboration among public health and health care organizations preparing and responding to catastrophic health events (Boston University, n.d.). Core members of the HMCC (i.e., hospitals; other acute care, long-term care, community and ambulatory care, and public health agencies; and public and private emergency medical services) provide a more integrated preparedness approach.
Few studies have focused on emergency preparedness policy and practice in hospitals from the perspectives of nurses, other first responders, and public health policy makers at the state level (Baack & Alfred, 2013). Wilkinson and Matzo (2015) found few studies examining the issues, concerns, and attitudes of nurses regarding disaster response or their perceived preparedness. Cagliuso (2014-2015) found the impact of several incidents, with significant implications for all U.S. hospitals, was all but nonexistent in the peer-reviewed literature.
Research Questions
This research examined the development and implementation of emergency preparedness policy and practice in Massachusetts hospitals from the perspective of nurses, public health policy makers, and first responders. The transfer of emergency preparedness knowledge in Massachusetts hospitals can be mapped by reviewing the translation of policy into practice, beginning with the precipitating event of 9/11/2001 to present day. Understanding the development and implementation of emergency preparedness policy and practice in Massachusetts hospitals may inform nursing, public health policy makers, and first responders by illuminating areas of success and those areas that need improvement as these stakeholders face future terrorist incidents, public health epidemics, or meteorological disasters.
Method
A case study was used to explore emergency preparedness policy and practice in Massachusetts hospitals post 9/11/2001; the case study was viewed through the lens of the Institute of Medicine’s (IOM; 2012) Systems Framework for Catastrophic Disaster Response, which guided data collection and analysis (Yin, 2014). The IOM (2012) report presented a comprehensive systems framework for understanding disaster response and integrated all interdependent values and response capabilities necessary for effective response. The standards of care within the framework apply in all-hazards disasters, under conditions of scarce resources, and focus on the needs of the community rather than the needs of an individual (Figure 1).
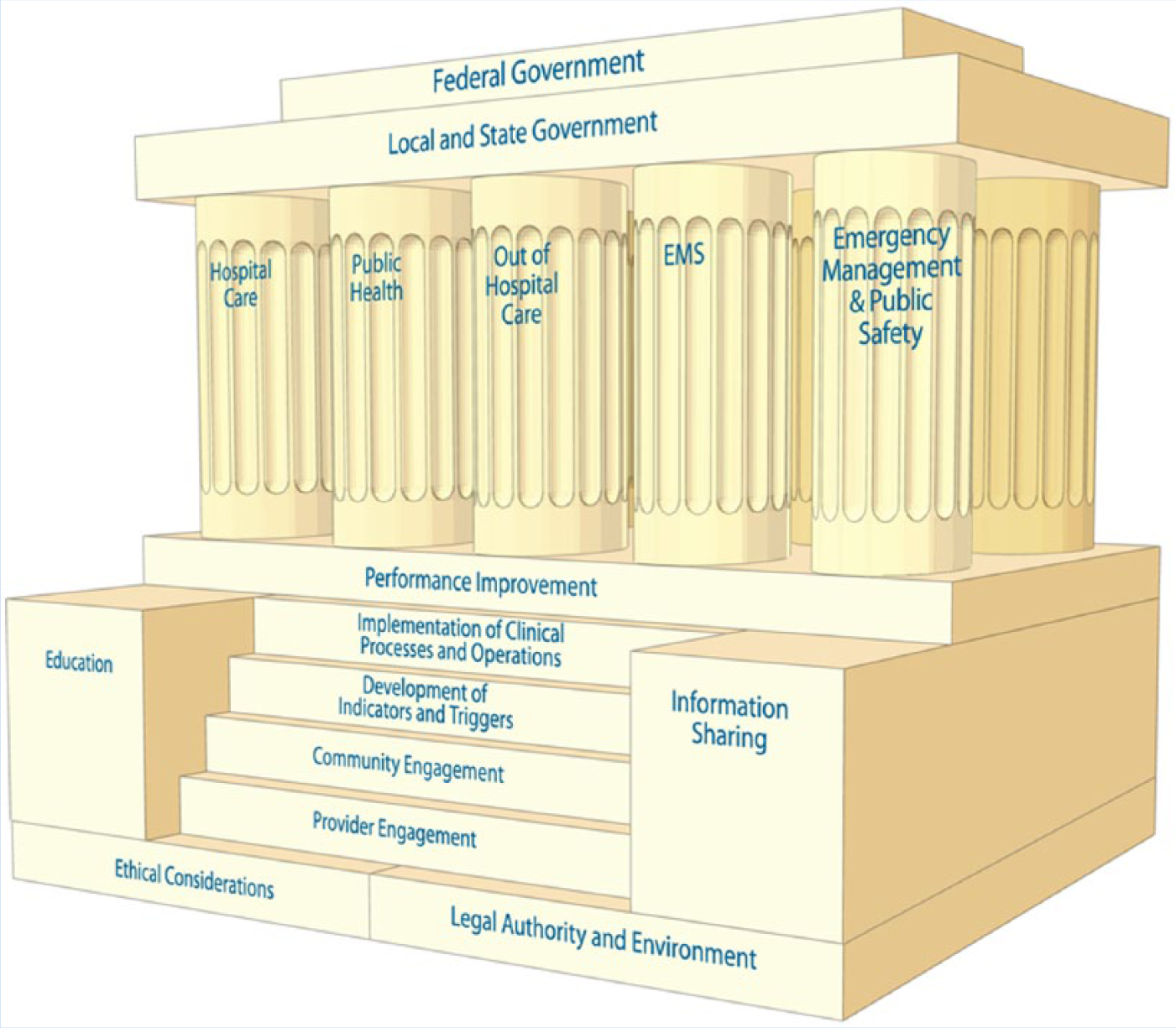
A systems framework for catastrophic disaster response.
This case study proposed that emergency preparedness policy at the federal and state levels influenced emergency preparedness policy and practice in Massachusetts hospitals. Data collection included a review of the DHS, DHHS, and Massachusetts Department of Public Health emergency preparedness policies, programming, and directives that impact hospitals, public health policy makers, and first responders. Additional data included evidence-based, policy literature relative to hospital emergency preparedness. Documentation tied to precipitating events in Massachusetts hospitals (i.e., post 9/11 anthrax white powder incidents, pandemic influenza planning, and the Boston Marathon bombing) was also reviewed. Nursing personnel representing public health policy and practice, along with first responders, were queried to expand documentation data sources. These data provided a framework for the research questions.
A qualitative descriptive approach to key informant interviews emphasized hospital and public health emergency preparedness programs in Massachusetts hospitals. The findings from key informant interviews validated emergency preparedness documentation and vice versa. Informant interviews with Massachusetts emergency preparedness policy and practice leaders explored the development, implementation, and adaptation of emergency preparedness programs over time. Purposeful sampling and a snowball technique was used to identify potential study participants including nurses, public health policy makers, and first responders who were chosen from multiple disciplines representing the functions shown on the pillars in the systems framework.
Informants shared common characteristics, including all were current leaders in Massachusetts emergency preparedness policy or practice and had been identified because of their senior-level or mid-level positions and involvement with hospital emergency preparedness. Encompassing the disciplines of hospital-based and public health nursing, public health, medicine, epidemiology, health care management, fire service, hazardous materials response, emergency medical services, and emergency management, most participants represented more than one discipline by education, training, or experience. Four participants were registered nurses. Nine informants (75% of sample) had statewide responsibilities; their view was representative of all Massachusetts hospitals. Three (25% of sample) were employed by one hospital, but each of these participants was involved in regional hospital preparedness, thus representing a singular hospital and a regional hospital preparedness perspective. This study was approved by the institutional review board of the author’s affiliated university.
Measures
In the summer of 2014, 12 informants were interviewed in person for approximately 60 to 90 minutes each, using a semi-structured interview with open-ended questions. Interviews were scheduled at a mutually convenient time in a location of the informant’s choosing, audio recorded and transcribed. Transcripts were reviewed for accuracy by the primary researcher and the informants. Participant demographic information included current position; positions held since September 11, 2001; organizational responsibilities; scope of practice; and affiliation and role with other emergency preparedness organizations.
Analytic Strategy
The qualitative data analysis occurred concurrently with data collection to provide an emerging understanding of the phenomenon. This iterative process of data collection and analysis continued until no new categories or themes emerged (DiCicco-Bloom & Crabtree, 2006).
Three transcripts were coded by hand by the primary researcher, initially identifying 17 recurring themes. An expert researcher was recruited to facilitate researcher and research reliability. Several themes were discarded and, with continued analysis, were reduced to five themes. A fourth transcript was coded by hand by the primary researcher to determine whether the data were identified, fit, and inclusive within the five identified themes. NVivo™ was used for computer-assisted qualitative data management and analysis using inductive coding to identify themes. Data were first displayed and coded by transcript using the identified themes, then displayed and coded by interview question, and then displayed by themes and organized and analyzed by theme and subtheme. An electronic database matrix was created in NVivo™ to manage qualitative data and to further analyze themes by additional criteria or subgroup, using demographic information.
Scientific rigor was determined by auditability, credibility, and fittingness. Auditability was established by the accountability of the researcher, case study protocol, and database matrix providing reasoning about each step of the research process. The electronic database established an audit trail, and a chain of evidence was established during data analysis. Credibility was established by a subject matter expert who piloted the interview guide, an informant who reviewed a draft of the study, and explanation building in the data analysis, a step-by-step cumulative approach, building one finding upon another. Fittingness was established by describing the data in sufficient detail so others could evaluate its application to their own practices. Triangulation of the data was accomplished by using multiple data sources and multiple methods for securing data. Documentation review and informant interviews were used to study the same phenomena and presented using the Systems Framework for Catastrophic Disaster Response (IOM, 2012) as a guide.
Results
Content analysis with nursing, public health, health policy, and first responder informants extracted the following five themes: training, communication, organization, funding, and events influencing emergency preparedness. Informants identified the inter-relatedness of each of the five themes.
Training
Most informants noted standardized training in hospitals with hospital personnel and other first responders after 9/11 has dramatically improved emergency preparedness. Generally, training was based on federal guidelines incorporated into the HPP and implemented statewide, by region. Nurses identified HPP training as “the most important training mechanism, and perhaps the only training mechanism, for the majority of hospital workers” and as “an important method of encouraging interprofessional training and emergency preparedness exercises and drills.” Training and collaboration were often paired; identifying standardized and collaborative training opportunities among disciplines and agencies led to effective incident response. Interprofessional training fostered understanding of emergency management roles and incident response across hospitals, regions, disciplines, and agencies. The importance of prior collaboration was highlighted as “key for other hospitals and hospital partners to understand how each hospital will respond to an incident and to appreciate their strengths, challenges and limitations.” Referencing the comprehensive hazard vulnerability analysis completed for each hospital and shared throughout the hospital region, an informant stated, “Because of this joint planning, a more inclusive risk assessment has been completed for each hospital and the region in which they are located and is now shared by all hospitals and community partners within the region.”
Hospital workers, particularly senior nurses, cited the priority of scene safety training before attending to patients as a counterintuitive challenge to the nursing code of ethics. Caring for critically ill patients who had not been decontaminated or placing themselves in danger while caring for patients during a hospital active shooter incident were examples given. The need to “give nurses permission to take care of themselves first,” and “health care providers need to understand the importance of not becoming a victim and thereby adding to the load of those requiring treatment” was reported by others. Hospital worker turnover and employees new to the workforce were identified as challenges to hospital preparedness.
The ICS was identified as a key management tool in small and large hospitals’ planned and unplanned incident management. Incident Command Service training and practice were “important facilitators in effective incident response.” The ICS common language, common roles, and chain of command contributed to better response among all partners. One health policy leader noted, “ICS training was initially considered a burden for hospital workers requiring time away from usual duties and limiting resources.” A nurse informant stated, “As ICS was utilized during incident response over a period of time and incorporated into hospital practice, the benefits became apparent.”
A number of training gaps were delineated. All nurses, with mid-level or senior-level positions, identified the majority of staff nurses as unaware and uninvolved in emergency preparedness as a gap, stressing the importance of including emergency preparedness training within basic nursing curricula for today’s nurse. Fire service informants cited the importance of statewide mass decontamination training and hospital capability to continue functioning during an incident with contaminated victims. Health policy leaders noted, “Interprofessional multiagency hospital decontamination training is a large cost to the hospitals; decontamination capability is an expectation but without commiserate funding for training and exercises,” and “You cannot maintain readiness without training and you cannot conduct training without resources.” Mass decontamination capability was described as a “high cost-low priority for hospitals, often unfunded or underfunded.”
A senior-level policy informant noted, Emergency preparedness is not something you train for once and then you’re set for life. Emergency preparedness needs continual skill building and training because you lose the skills if you don’t use them and because the necessary skills change as technology develops. One thing we have learned is that you cannot fund emergency preparedness for a short period and then cut it back and expect that you are going to have the level of skill and expertise needed in a major emergency.
Communication
Hospital and public health informants noted improved communication and relationships with their community partners (e.g., other hospitals, local boards of health, local industry, local government, and schools) post 9/11/2001 citing “improved relationships,” “receiving important feedback,” “additional knowledge,” and “enhanced incident response” as examples. The key role nurses play in incident response and inter-hospital communication during incidents was echoed by all informants. Nurses provide triage and victim assessment and are key facilitators in maintaining clear, focused, and current communication between hospital workers in all departments.
The Health and Homeland Alert Network (HHAN) was found to be an effective tool to assist public health and hospital emergency preparedness planners in incident awareness, incident evolution, and incident impact throughout the region and state. Those participants in senior policy or practice positions noted crisis communication as a key response capability, both as a mechanism to keep hospitals, their partners, and the community informed and as a tool for hospital workers to personally and professionally plan to respond to an incident. The importance of knowing fellow emergency response agency partners before the emergency was cited by all, with one adding, “Communicating and working together in advance of an incident during training, exercises or drills allows responders to develop a level of trust before an incident occurs,” and “Recognizing the sound of their voice meant I knew there was a capable informed partner making decisions and I did not need to waste time figuring out if they were credible.”
Organization
Changes influenced by 9/11 included, Before 9/11, hospitals worked in silos; they did not collaborate with nearby hospitals; they did not share plans or capabilities; and they competed against each other. After 9/11, hospitals began to work collaboratively with other hospitals and public health and community partners which fostered communication and understanding between organizations.
Limited roles for hospital emergency management planners were an organizational concern. “Planners are required to manage hospital-wide emergency preparedness on a part time basis as these duties compete with their additional job responsibilities.” Difficulty in implementing ICS within the hospital organization was highlighted, “Hospitals generally follow a medical model, a top down approach with physicians leading the health care team as opposed to the ICS model, which assigns roles to the best qualified person responding to the incident at the time” and “This change in roles, command structure, and chain of command presented organizational challenges when the ICS was introduced.” These challenges decreased over time as ICS became integrated into the organization.
A significant difference in organizational response capabilities of urban versus rural hospitals, large versus small hospital systems, and non-profit versus for profit health care systems was identified by all participants who reported frustration with hospitals having fewer capabilities and resources devoted to emergency preparedness. Friction among regional hospitals with competing gaps in their capabilities was cited as regional hospitals determined the best way to allocate federally funded HPP funds. Concern about a decreased workforce leading to diminished response capability was identified: Health care providers may work for more than one hospital or may participate on a regional Medical Response Team (MRT) . . . they may be counted by more than one agency for response availability. First responders and/or their families or home communities may be impacted by the incident leaving first responders unable or unwilling to respond further decreasing the number of responders.
Funding
All informants commented on the impact of decreased funding on hospital readiness and the burden new HPP requirements over time have added, coupled with the expectation that previous requirements and capabilities are maintained. As the emphasis has shifted away from individual hospitals to regional collaboration and HMCC, funding for individual hospitals has diminished further, while funding for regional efforts has increased. Most informants identified hospitals as having ever tightening budgets, fewer resources, and more demands placed upon them. Examples cited were, “the impact of a just in time economy” and “every hospital position is designed for maximum efficiency and no excess capacity but preparedness is considered excess capacity,” and One of the things we are always faced with is funding. Any time you have built an infrastructure, there needs to be the will and the funding to maintain and improve what you have in place or what you have built.
Events Influencing Emergency Preparedness
A number of events impacting emergency preparedness were recalled. Most prominently, “The 9/11 terrorist attacks provided ‘a wake-up call’ and a notice that one event could change a city, a state or a nation overnight,” and “9/11 acted as a catalyst which spurred hospitals to plan and mobilize resources for unanticipated incidents.” A majority cited the initial HPP training after 9/11/2001 focused on the ICS and hospital response to CBRNE terrorist threats requiring hospital decontamination and personal protective equipment capability. “Hospitals were not used to identifying themselves as victims and understanding that they needed to protect themselves presented a stark reality after 9/11,” reported a nursing informant. Additional findings included, “The response to the Anthrax white powder incidents after 9/11/2001 required extensive hospital preparation for receiving anthrax victims fostering collaboration between the state department of public health, the state laboratory, select hospitals, fire departments and the DFS hazardous materials teams,” and “Following Hurricane Katrina, hospital evacuation planning came to the forefront. Hospitals began to plan for extended operational periods,” and “Following the 2009-2010 H1N1 influenza pandemic, hospital and public health planning focused on hospital surge capacity.” The Joplin, Missouri, tornado (May 2011) was seen as, “a lesson learned in community preparedness including the impact of providing health care absent a functioning hospital or additional health care resources or other functioning community resources.”
Discussion
This qualitative case study examined the development and implementation of emergency preparedness policy and practice in Massachusetts hospitals after 9/11. A case study methodology, including key leaders representative of first responder functions identified in the Systems Framework for Catastrophic Disaster Response (IOM, 2012), provided a valuable perspective. Using the experience, knowledge, and lessons learned from nurses, public health, and first responder leaders in Massachusetts, this study identified a number of key elements impacting preparedness response.
Standardized training is a key component of effective emergency preparedness. Interprofessional training with public health and other first responders and community partners fosters an understanding of integrated emergency preparedness roles and incident response. Training is needed to accommodate employees new to the workforce and hospital personnel turnover; ongoing interprofessional training is also needed to reinforce lessons learned and advance preparedness knowledge and skills. The HPP provides interprofessional preparedness planning and training opportunities for hospitals, public health, and other first responder agencies. Kellermann (2013) cited prior planning and training as critical to hospitals’ successful responses to the Boston Marathon bombing as did FEMA (U.S. Department of Homeland Security, 2014) in noting local, state, and federal agencies and community partners developed and tested plans, defined roles and responsibilities, and exercised communication and collaboration during prior large-scale events, all contributing to an effective response. The FEMA suggests this well-coordinated response can be replicated by sharing situational awareness across public agencies and their community partners and training to institutionalize unity of effort (U.S. Department of Homeland Security, 2014). Institutionalizing ICS in the hospital setting was pivotal for effective incident response by providing a coordinated and standardized approach for hospitals and their first responder partners. Hospitals initially considered ICS difficult to implement, but the standardization, structure, and scalability proved valuable and reliable with repeated use.
Gibson, Theadore, and Jellison (2012) identified communication and information flow as challenges in emergency preparedness. Hospitals learned the value of establishing relationships with other first responders and community partners, improving communication and enhancing understanding of multiple perspectives about the same incident. Cagliuso, Leany, and Sandoval (2010) identified communication, collaboration, and relationship building among hospital stakeholders as key to hospital emergency preparedness in the United States, noting it is often the weakest aspect of hospitals’ emergency management plans. Communication tools, such as the HHAN, provide public health and hospital personnel with real-time data impacting hospitals, the hospitals’ region or state, allowing each hospital to plan for additional patients from the incident or referred from impacted hospitals. Nurses, including hospital employee health nurses, are key contributors in emergency preparedness. Acting as communication conduits, nurses facilitate communication among all hospital workers and other first responders. The nursing role traditionally facilitates health care planning, teamwork, and collaboration across disciplines and organizations, an important function in preparedness response.
It might also be noted that emergency preparedness across and within health care organizations has evolved from hospitals functioning independently to sharing response plans and capabilities with other hospitals, public health and first responder agencies, and community partners (Boston University, n.d.). Sharing a hospital risk assessment with all community stakeholders can facilitate identifying regional strengths, gaps, and limitations in preparedness response; resource availability contributes to overall community preparedness. As the HMCC shifted their emphasis to developing a coordinated and collaborative preparedness coalition, health and public health organizations partnering with community organizations provided an integrated approach to emergency preparedness planning and response (Boston University, n.d.).
Kellermann (2013) reported overall funding for hospital and public health emergency preparedness had diminished, and this research confirms that finding. Hospitals have fewer resources and more demands with many needs competing for limited hospital dollars. Emergency preparedness is often considered a high cost–low probability threat and underfunded or unfunded, except to meet regulatory compliance requirements. Cagliuso, Smith, Antunez, and O’Reilly (2012) identified that hospital preparedness gains could be lost as programs are minimized or eliminated due to budget revisions. Each year, the HPP sets and funds new requirements, with the expectation that previous HPP requirements and capabilities be maintained. These unfunded mandates pose a significant financial burden to hospitals. With the HPP’s evolution from individual hospital response capability to regional collaboration inclusion of regional hospitals and their community partners, HPP funding for individual hospitals has decreased, adding to the financial burden.
As the lack of readiness and resilience to respond to disasters became apparent after 9/11/2001 (U.S. Department of Homeland Security, 2008), health care emergency preparedness policy was developed at the federal level and cascaded to the states and local government, with the HPP representing a critical program. Sentinel events have contributed to the cascade effect of distributing knowledge and lessons learned in the development of a coordinated and collaborative all-hazards approach by public health and other community partners to weapons of mass destruction, preparation for receiving contaminated victims, protecting hospital personnel, surge capacity, and limited or no hospital or community resources after an incident.
Limitations
The findings in this study reflect the experiences of nursing, public health and other leaders in Massachusetts emergency preparedness, derived from a purposeful sample with informants sharing common characteristics. Although the occupational health nursing perspective was not specifically sought, many of the findings are relevant to their practice. Participating in interdisciplinary teams, planning for all-hazards incidents, and collaborating with public health and community partners to meet the health and safety needs of personnel are core competencies for the occupational health community (American Association of Occupational Health Nurses [AAOHN], 2015). An investigation with more diverse participants, such as occupational health nurses, may yield additional results. If all individual Massachusetts hospitals were surveyed, some differences might emerge, but case study methods did not permit this approach. This study sought a wider perspective of statewide policy professionals rather than the overall hospital viewpoint.
The model used for analysis did not include measuring social capital at the community or national level. Future studies should incorporate an evaluation of community and organizational resilience as indicators of response and recovery capabilities (Morton & Lurie, 2013).
Informants were asked about events over the last 14 years; therefore, recall bias may exist. Although the themes of training, communication, organization, funding, and sentinel incidents are likely consistent in hospital and public health emergency preparedness across the United States, the study cannot generalize beyond Massachusetts. Emergency preparedness is a dynamic process, and as it continues to evolve, additional research is needed to facilitate standardized training, collaboration, and communication to improve incident response for hospital professionals, including occupational health nurses, and their public health and community partners.
Applying Research to Practice
Hospital emergency preparedness has evolved in response to threats of terrorism, meteorological disasters, and public health emergencies. This case study examined emergency preparedness policy and practice in Massachusetts hospitals following September 11, 2001, identifying areas of success and opportunities for improvement. It is imperative that the key findings, including the importance of standardized training, the value of interprofessional collaboration, and communication across public health and community partner organizations, are incorporated into emergency management planning. Given the impact of recent global terrorist events, hospital emergency preparedness programming with health care and community partners must continue to be funded, despite competing resources, to ensure an effective response. Emergency preparedness is a dynamic process, and additional research is needed to standardize training, encourage collaboration, and facilitate communication so that incident response by hospital professionals, including occupational health nurses, and their public health and community partners is more effective.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Mary A. Taschner is an occupational health nurse practitioner at Pfizer Biotech, Andover, MA, with research interests including emergency preparedness and occupational health biological exposures. She developed emergency preparedness programs for hospitals, fire service, and EMS working for the MA Department of Public Health. As an adult nurse practitioner for over 35 years, her experience includes occupational health, ambulatory care, and primary care as well as nursing education and consultation. This study was in partial completion of the doctorate of nursing practice degree at the University of Massachusetts Lowell.
Angela Nannini is an associate professor emeritus at the University of Massachusetts Lowell. Her public health research focuses on health policy related to health disparities, women’s health, maternal and child health, and health care workforce issues. As a family nurse practitioner for over 30 years, she has provided primary care to populations at risk for health disparities.
Margaret Laccetti is an assistant professor at the University of Massachusetts Lowell. Her numerous research interests include oncology, palliative care, pain management, and standardized patients/low fidelity simulation in nursing education. She is a clinical nurse specialist, with advanced practice certifications in both oncology and hospice and palliative care nursing.
Martin Greene was with the Bourne Fire Department since 1981, appointed as a career firefighter/paramedic in 1985, named Chief in 2011, and retired in 2015. He is a charter member of the Department of Fire Services, District One Hazardous Materials Response Team, and remains a member of the IAFC Hazmat committee and involved in teaching and consulting in Hazardous Materials/CBRNE and incident management response.