
Abstract
High-rise (HR) building fires remain a tragic cause of preventable injury and death in the United States. Recent incidences of HR building fires have served as high-profile reminders of the persistent threat that HR fires pose to public health. Fire safety is an important aspect of household emergency preparedness addressed by community/public health nurses (C/PHNs). This study aimed to address a gap in the literature regarding C/PHNs’ awareness of fire safety for people and families who reside in HR buildings. A descriptive qualitative study using key-informant and focus group interviews was conducted involving C/PHNs (n = 19) in Honolulu, Hawaii. Qualitative data analysis revealed three main themes related to this issue: (1) C/PHN awareness of HR fire safety issues, (2) C/PHN perceived barriers for HR building occupant fire safety, and (3) C/PHN suggested strategies to address HR fire safety for occupants. Findings highlight how more needs to be done to assure that C/PHNs are adequately prepared to work with occupants of residential HR buildings on matters related to fire safety.
Keywords
High-rise (HR) building fires remain a tragic cause of preventable injury and death in the United States. In recent years, cities such as New York City, Minneapolis, Los Angeles, and Honolulu have experienced tragedy due to deadly residential HR fires. These incidences serve as high-profile reminders of the persistent threat that HR fires pose to public health. HR buildings are defined as buildings greater than 75 feet (23 m) in height from the ground level to the highest floor. Across the United States, an estimated 14,500 fires occurred in HR buildings between 2009 and 2013, resulting in an annual average of 40 civilian deaths and 520 injuries. The majority of these fires (62%) occurred in apartments and other multi-family housing (Ahrens, 2016). HR fire safety has emerged as an important public health issue due to key demographic and environmental trends. First, the proportion of people in the United States living in urban areas has been steadily increasing decade over decade. This demographic shift of the population away from rural settings and concentration in urban areas has led to an estimated 82.45% of the total U.S. population living in urban settings in 2019, compared with 79.05% in the year 2000 (World Bank, n.d.). The explosive growth of cities has resulted in an unprecedented number of people living in high-density housing settings, such as HR buildings. Second, the number of disasters affecting urban areas is trending upward as more people become urban dwellers (United Nations, 2015). HR buildings subjected to various natural and manmade hazards may sustain damage, leading to the incapacitation of building operations, and partial or complete building collapse (Kodur et al., 2019). Fire is a serious hazard for HR buildings that can threaten the safety of its inhabitants. Many cities in the United States have a large number of aging residential HR buildings that were built before fire safety codes began requiring fire sprinklers and advanced alarm systems. In many municipalities, these structures are not always retrofitted to the current standard, leaving residents who live in these buildings at a greater risk for injury or death during a building fire.
Undertaking proper fire safety precautions is important for mitigating the impact that fire hazards have on individuals, households, and building communities. Fire safety involves preventing or reducing the likelihood of a fire resulting in death, injury, or property damage (Kodur et al., 2019). An important element of fire safety is ensuring building occupants adopt behaviors to prevent situations that are most likely to cause fires, such as maintaining fire safety equipment (such as fire extinguishers or smoke alarms) and practicing fire escape plans to prepare themselves for emergency evacuation (Ready.gov, n.d.). Fire safety behaviors of HR residents are influenced by various individual and organizational or communal factors (Gerges et al., 2018). Greater uptake of fire safety and emergency preparedness behaviors have the potential to save lives in the event of a HR fire.
Community/public health nurses (C/PHNs) have sought ways to better prepare households and communities for various types of emergencies, and have recognized the importance of greater research in the areas of emergency preparedness (ACHNE, 2010). Fire safety is one important aspect of household emergency preparedness addressed by C/PHNs. Successful household fire safety interventions involving nurses have included the development of resident fire safety checklists, home fire safety inspections, and installation of smoke detectors (Lehna et al., 2014, 2015a, 2015b; Omaki et al., 2018). Literature regarding C/PHNs’ engagement in fire safety among residential HR building occupants remains a little explored area, despite the growing population of HR dwellers across the country at-risk for building fires. The purpose of this study was to address a gap in the literature regarding C/PHNs’ awareness of residential HR fire safety issues.
Methods
This research study used a descriptive qualitative approach to inquiry using key informant and focus group interviews. This qualitative approach was appropriate since little is currently known about C/PHNs' awareness of residential HR occupant fire safety issues. The study aimed to answer the following research questions:
What is the level of awareness of residential HR fire safety issues among C/PHNs? What current practices and future intentions do C/PHNs have for preparing clients who live in HR buildings for fires or other building emergencies?
Participants and Sampling
A convenience sample of C/PHNs was recruited for participation in this study. The criteria for inclusion in the study included being a currently practicing C/PHN on the island of Oahu, in the State of Hawaii at the time of the study. An email explaining the study was sent to the representatives of community/public health nursing agencies to invite them to participate in the study. Agencies contacted were those located in geographical areas with high concentrations of residential HR buildings that provide services to clients/families living in HR buildings. The University of Hawaii Human Research Protection Program reviewed and approved this project as exempt.
Data Collection Procedures
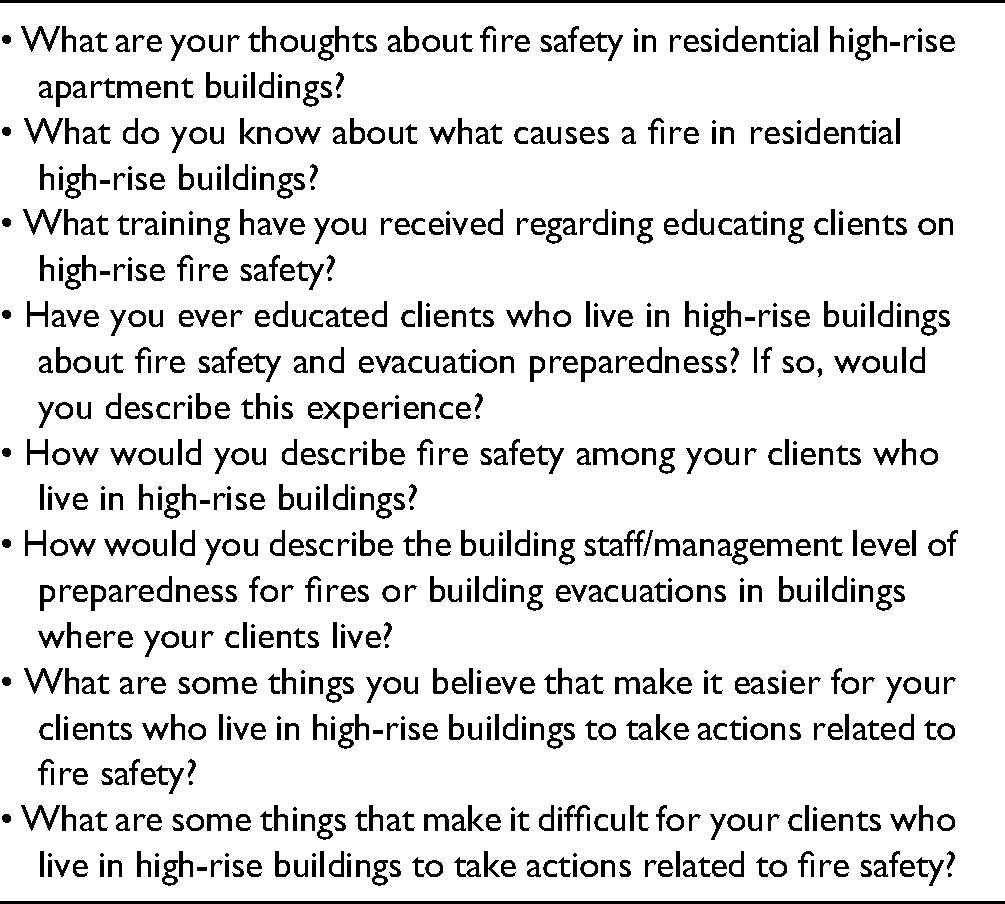
A nine-question sociodemographic questionnaire was used to collect descriptive demographic data from study participants. An eight-question semi-structured interview guide (Table 1) was developed based on the theory of planned behavior (Ajzen, 1991). Both the socio-demographic questionnaire and interview guide were refined with input from HR building fire safety experts for appropriateness and validity before their use. Qualitative data were collected via one key informant interview and three focus group interviews. The key informant interview was conducted first. Findings from the key informant interviews informed refinement of the focus group interview guide. All data collection sessions were conducted in-person at the C/PHNs’ place of employment for convenience of the participants. Locations included an occupational health clinic, two community health centers, and a public health nursing office. Each interview lasted approximately 30–60 min. The order of questions followed the semi-structured interview guide with probing follow-up questions. Two researchers participated in each session: one researcher asked questions, another researcher took handwritten notes on a large notepad visible to participants. As a form of member checking, one researcher would read back handwritten notes to participants periodically during the interview to confirm that what was stated was accurately noted. Each interview was recorded with a digital voice recorder and later transcribed verbatim. Researchers conducted focus groups with different participants until data saturation was reached.
Interview Guide Questions.
Data Analysis
Socio-demographic data were entered into MS Excel to calculate descriptive statistics of the sample. Interview transcripts were analyzed using qualitative content analysis (Graneheim & Lundman, 2004; Hsieh & Shannon, 2005). Two researchers concurrently and independently read and reread transcripts and handwritten notes to conduct initial coding. Researchers then met to compare codes. Differences in coding were discussed and mutually resolved. Initial codes were combined into categories that reflected emergent themes. Transcripts were again reviewed to validate the codes and categories. (Graneheim & Lundman, 2004).
Results
Participant Characteristics
Nineteen (N = 19) C/PHNs participated in the study (Table 2). All were female and nearly all had a bachelor's degree or higher (n = 18, 95%). The majority (n = 11, 69%) were aged 25–39 and had worked as a C/PHN for 5 years or less. Participants’ nursing practice settings varied, including an occupational health clinic, community health center, school health clinic, and public health nursing. Participant roles included public health nurses (PHNs), care coordinators, school, and occupational health nurses. The sample included a mix of generalist RNs as well as advanced practice registered nurses (APRNs). All participants worked in agencies that serve urban Honolulu, the area with the greatest density of HR buildings in the state.
Characteristics of Study Participants a .

Note. C/PHN = community/public health nurse.
Total of 19 study participants.
Three participants declined to answer.
Three participants declined to answer.
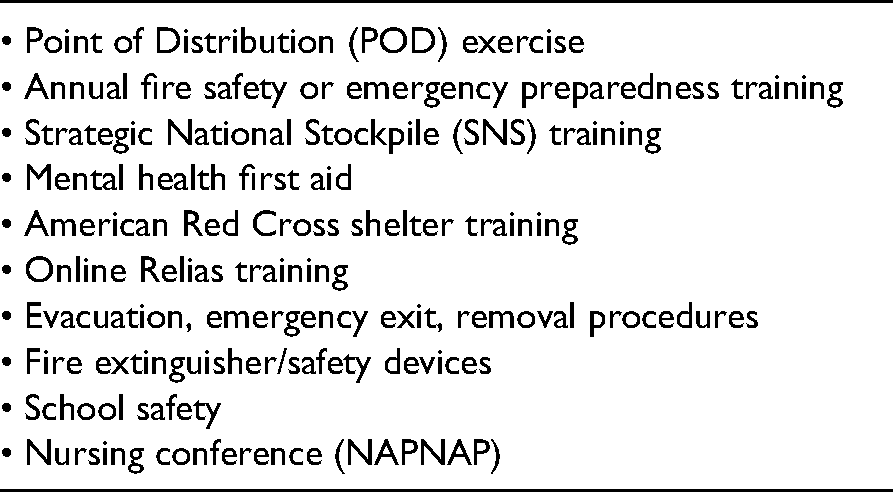
Participants’ experience related to HR building fire safety is summarized in Table 3. While none of the participants currently lived in a HR building, over half (n = 12, 63%) had lived in one in the past. Four (21%) had experience evacuating from a HR building. While nearly three-quarters (n = 13, 72%) of the participants reported feeling concern regarding their clients’ HR fire safety, only about a quarter (n = 5, 26%) had ever discussed fire safety with their clients. One-quarter (n = 4, 24%) reported that a HR fire had occurred in their district. Participants shared the types of emergency preparedness training they had received, summarized in Table 4.
Personal and Occupational Experience Related to High-Rise (HR) Building Fire Safety.

Note. HR = high-rise; EP = emergency preparedness.
One participant declined to answer.
Two participants wrote “unknown.”
Types of Emergency Preparedness/Fire Safety Training Received by C/PHNs.
Three major themes emerged from the qualitative data: (1) C/PHN awareness of HR fire safety issues, (2) C/PHN perceived barriers for HR building occupant fire safety, and (3) C/PHN suggested strategies to address HR fire safety for occupants. Themes and subthemes are summarized in Table 5.
Summary Table of Key Themes and Subthemes.

Note. HR = high-rise; EP = emergency preparedness; FS = fire safety; C/PHN = community/public health nurse.
C/PHN Awareness of HR Fire Safety Issues
It was generally noted that fire safety is an important topic for C/PHNs to engage in with clients living in HR buildings. For example, a nurse working as a care coordinator at a community health center stated, “It's especially important for families that have medically needy members of the family. In a condo where we were at… there were several elderly that can't get down the stairs.” A PHN also commented, “[HR fire safety] is related to health and safety for us… For us [PHNs] the focus is mainly on elderly and emergency preparedness in general.”
All participants were keenly aware of common fire risks present in their clients’ homes, describing various potential fire safety hazards they have witnessed or were made aware of during interactions with clients. Fire hazard risks were related to infrastructure (faulty electrical wiring or overloaded extension cords), unsafe behaviors (cigarette smoking, unsafe cooking practices, improper use of electrical appliances, children playing with matches), or other factors. A major risk for starting kitchen fires mentioned was older adults with dementia.
While most respondents felt that the topic of HR fire safety was important, many admitted that it was not something they thought of regularly. One participant remarked, “I don't know if people actually think about [fire safety] on a regular basis. If there's a fire … we just kind of assume that people can find the exit and get themselves out.” An APRN who works in a school clinic commented, “I definitely know we have children that live in HR buildings and it's never discussed in my setting.” Many remarked that it is not until a significant event occurs that HR fire safety is discussed. Multiple participants described the impact that a major HR building fire had on the public's general awareness of HR fire safety. One nurse recalled the incident, which had resulted in the death of four people, stating, “[HR fire safety] is not really something people are aware about until something happens… with what happened with the Marco Polo [building fire] … until that happened no one was really aware about evacuation safety.”
While most nurses were aware of general fire safety concerns for households, some nurses noted that they were not aware of whether or not their clients live in HR buildings, despite many such buildings being present in the districts they serve. One nurse commented, “Honestly, it's not something that we would really ask our patients about. We ask their address, but not whether they live in a HR building … unless they bring it up and have concerns about it.” One APRN asked other members of her focus group, “Has that ever been a part of your screening? I don't think I ever really asked … ‘Do you live in an apartment building or a house?’ The only time you really ask in primary care is when you’re asking about how old the building that they live in is because you’re worried about lead.”
C/PHN Perceived Barriers for HR Building Occupant Fire Safety
Participants identified a wide variety of factors that stand in the way of their clients’ fire safety behaviors. The barriers mentioned were grouped into two categories: personal and communal/environmental.
Personal Barriers
Low Levels of Education or Knowledge Regarding Fire Safety: Participants mentioned that many of the clients have a low level of knowledge about fire safety and emergency preparedness, and lower levels of education in general. One APRN mentioned, “there probably isn't very much [fire safety] education out there for families … I would doubt that they have any idea what they should be thinking. The community I work in is very undereducated.”
Financial Hardships and Housing Instability: Nurses mentioned that many of their clients experience financial barriers that may stand in the way of purchasing or maintaining fire safety equipment such as smoke alarms or fire extinguishers. Instability in housing was also mentioned as a barrier to fire safety. For example, one RN noted that “sometimes our patients don't have a stable home … they go from home to home. And with that comes a challenge … they don't even know where they’re going to sleep that night.”
Persons With Mobility or Sensory Deficits: Many participants identified how mobility or sensory deficits pose challenging barriers for their clients to practice fire safety behaviors. Examples included older adults, patients in wheelchairs, those with vision or hearing deficits, chronic diseases, and persons using supplemental oxygen, which were noted as populations of major concern when considering fire safety. One nurse explained, “Naturally, with our population, its mobility. It's the number one thing. I know a lot of our patients that need assistive devices to get anywhere, or who don't have a caregiver or are living alone.” Another nurse added, “A lot of our patients are wheelchair-bound. A lot live in public housing, in buildings taller than 7 stories. So it's a big struggle for them to even get to an appointment with their provider. So we have to arrange an ambulance for them to get home [from an appointment] because they cannot walk.” A PHN noted, “I have had elderly clients that either had dementia or were hard of hearing. Quite frankly, I don't know if they would be able to hear [the smoke alarm]. Even when I’m knocking on their door or ringing the doorbell, sometimes they don't answer because they don't hear it.”
Cultural/Linguistic Barriers: Many nurses recognized how clients who came from places with different cultural or linguistic backgrounds experience barriers at a major disadvantage in regards to fire safety. Clients who live in households where English is not the primary language often have to rely on their children to translate important information. According to some participants, these households are not likely to have discussions regarding household fire safety. “I feel bad for the patients that English is not their first language. Most signs or directions are in English … The language barrier, that's number one.” Nurses also remarked on how cultural differences in the way people live may pose challenges to household fire safety. One nurse case manager remarked how many of her clients come from cultures where it is the norm for a large number of people to live in one home, noting that “There are several intergenerational family members sharing rooms, living in the same home, sleeping in living rooms, like eight in a one-bedroom apartment.”
Communal/Environmental Barriers
HR Building Community Leadership/Management: Many nurses commented on the importance of building community leadership in regards to fire safety and emergency preparedness within HR buildings where their clients live. A PHN noted that building management and resident managers have a big role in taking the lead to help residents with fire safety issues in the building. Where building management is very proactive, nurses noted greater levels of overall emergency preparedness knowledge among residents. Other times, despite intent for improving fire safety and EP, there is not always a strong follow-through. A PHN recounted her efforts to engage one of the elderly housing buildings in her district in emergency planning. “We tried to do a COOP (Continuity of Operations Plan). They wanted to do something with fire safety. But every time we tried … they were busy or something came up. It wasn't a priority.” Participants shared how when building leadership is lacking, the residents are at a disadvantage because overall, the building community will have less awareness of knowledge or resources available to them regarding fire safety. This is the situation for some building communities where their clients live, where there appeared a void of leadership/management involvement in fire safety or EP. One nurse stated, “Some of the HR buildings don't have any staff on site … they just posted ‘don't use the elevator, go down the stairs [during an emergency],’ that's it.”
Lack of Trust in Authority: Nurses noted that some members of their patient population are wary of letting outsiders into their homes, which may contribute to unsafe conditions in the home. An APRN noted, “The American Red Cross will do free smoke alarms … but our patient population sometimes has friends or family staying with them, and they might be in [public] housing, so they don't want to get in trouble for breaking the rules. They often are suspicious of letting any outsiders inside.”
Structural Barriers: Nurses recognized that many HR buildings in their community lacked safety systems that protect residents in the event of fires, such as intercom systems or fire sprinklers. “A lot of HR buildings were built in the 70s, so they wouldn't have the mandatory sprinkler system in case of a fire. They’re expensive to put in once it's already built.” Others noted having observed HR settings where it is difficult to navigate emergency exit routes. A community health nurse noted, “If you’re visiting, building staff don't tell you… where the fire exit is. And there are times that you cannot go on a different floor because you need to get access… you don't know where is the exit.”
C/PHN Suggested Strategies to Address HR Fire Safety for Occupants
Participants reflected on what C/PHNs could do to be more engaged in HR fire safety issues for their clients. Many mentioned the need to improve their fire safety habits, noting that they would discuss fire safety with their household members following their participation in the study. One CHN suggested that her clinic increase their awareness of the type of living environment their patients inhabit. She said, “Something we can bring back to our clinics when they check into our front desk when they give their address, the front desk could additionally ask, ‘Do you live in a high rise?’ That will kind of help because that will alert the provider or the nurse care coordinators to add it into [their medical record].” Nurses also discussed developing stronger communal/professional ties with other agencies to address fire safety. One PHN mentioned the need to strengthen links with the fire department, stating, “We don't really have a relationship with them… we never did anything about fire safety. We need training too.”
Participants noted that fire safety discussions are often limited in scope if brought up with clients, and rarely was included as part of a broader discussion on family emergency preparedness. One RN stated, “In discussing fire safety with patients, we only ask ‘Do you have a smoke alarm with working batteries?’ But beyond that I haven't really engaged in a bigger conversation” regarding knowing an evacuation route or a family reunification plan. An APRN, noting how clients are unlikely to access fire safety educational materials commented, “To assume that they have a fire safety plan, that they know what they can do in an event of an emergency like that… I think that would be underestimated. It makes me feel like I should do more in the area of fire safety education.”
Strategies were suggested regarding how clients living in HR buildings can enhance fire safety behaviors. At the individual household level, participants shared that residents should seek out more information about fire safety and take steps to prepare their households for building emergencies. Examples of actions their clients could take included assembling emergency preparedness kits, family emergency plans, and talking to their building's management to learn more about emergency plans for their building.
At the building community level, participants suggested that various actions could be taken to improve overall fire safety behaviors of clients living in HR buildings. Examples included disseminating fire safety educational information during building meetings or posting such information in public spaces. One nurse commented, “The building owner or management should send out information to people either via email or mail, hold monthly or quarterly meetings, and post signs that remind people about fire safety escape routes… a couple of times a year because new people move in, and people forget.” Many nurses suggested that new residents should receive this information with a building orientation when they first move in that informs residents about emergency procedures, and locations of emergency exits, evacuation routes, and meeting places. Such information should be provided in various languages. Other actions that buildings could take to encourage fire safety is to conduct emergency drills quarterly or monthly to assure that residents know exactly what to do in case of an actual fire. Nurses also noted that while some buildings maintain a list of individuals who would need assistance during an emergency, not every building has this practice and some that do, do not keep their lists up to date. Additionally, nurses noted that building management could work toward maintaining positive and trusting relationships with clients. This is because nurses noted that a building's management team has a strong influence on the behaviors of its residents. HR building communities and management could also seek options for enhancements to building infrastructure to improve resident safety in older structures, such as the installation of fire sprinklers and advanced intercom systems.
Finally, participants suggested changes at the systems level, such as providing more public education and services, as well as advocating for public policy changes. One nurse described the positive impact of public fire safety education programs such as “fire safety month,” and school fire safety week. Various methods were described to bolster community education outreach efforts, such as TV commercials, pamphlets, and community health fairs that provide demonstrations or hands-on training on how to prevent or put out fires. One PHN noted that special emphasis should be placed on reaching out to older community members, stating, “I think the focus should mainly be on elder and emergency preparedness in general. I think kids are pretty much covered at the schools. My kids come home and they have to draw the evacuation plan. We can work that way with the elderly.” Participants also called for government policies requiring safety standards and safety checks to occur on a regular schedule. They felt many of these practices should be mandated, expressing doubt that if such practices were not mandated, they would not be done.
Discussion
A key objective of this research study was to determine the awareness of residential HR fire safety issues among C/PHNs. This study found that C/PHNs had a keen awareness of fire hazard risks faced by their clients. Participants noted fire hazard risks present within their clients’ homes that are well described in the literature. Previous studies involving home health care providers found that multiple types of home fire hazards are commonly encountered when visiting clients, such as faulty electrical outlets, smoking with oxygen in use, and using the stove for heat (Polivka et al., 2015). This study's participants expressed a low level of confidence that their clients recognize such risks in their home settings. This situation may contribute to the fact that many Americans die or are injured due to HR fires. While more recent data on HR fire injuries and deaths is not readily available, between 2009 and 2013, the United States experienced an annual average of 40 civilian deaths and 520 injuries due to HR fires (Ahrens, 2016). Results of this research identified how specific groups in C/PHNs' client populations are perceived to be at greater risk for injury or death due to fire. The C/PHNs reported that clients in their community who are older, have sensory deficits, mobility issues, and/or are from households with different cultural or linguistic backgrounds are most vulnerable to fire risk. This is consistent with findings from other research studies that report that the risk of death due to fire is spread disproportionately among specific vulnerable populations. Older adults age 65 years or greater are more likely to die in a fire than the general population (Gilbert & Butry, 2018; Lehna et al., 2015a). Persons with mobility impairments, as well as racial/ethnic minorities also experience a higher proportion of fire injury and deaths in this country (USFA, 2019). The disproportionate level of injury and death is avoidable and highlights this serious health disparity issue.
Common recommendations by emergency preparedness agencies related to household fire safety include installing smoke alarms in every level of the home, testing smoke alarms every month, changing batteries if they are not working, and creating a fire escape plan that is practiced at least twice a year (American Red Cross, n.d.; USFA, n.d.). The reported presence of smoke detectors in homes among the U.S. population is very high (Wood et al., 2016). However, oftentimes smoke detectors are not present on every floor or room, not audible in sleeping areas, or non-functioning (Gielen et al., 2012; Omaki et al., 2018). Missing batteries were reported as the most common cause for non-working smoke-alarms (Ta et al., 2006). Only about half of U.S. households report the possession of a family fire escape plan (Wood et al., 2016). However, of the households that do have fire escape plans, most report never having practiced the plan (Lehna et al., 2015a, 2017). Findings from this study found that clients of C/PHNs living in HR buildings encounter various barriers that prevent them from implementing recommended fire safety behaviors. These barriers include financial, cultural, and mobility/sensory deficit issues that may make it difficult for clients to carry out recommended household fire safety and emergency preparedness actions on their own. Addressing these barriers experienced by HR residents should be incorporated into any planning for fire safety programs.
The second objective was to determine what current practices and future intentions that C/PHNs have in regards to preparing clients who live in HR buildings for fires or other building emergencies. Despite general recognition of the risks for fire present in clients’ homes, few participants of this study had experienced engaging in fire safety education with their clients. However, it was noted that more could and should be done to address this issue with their clients. Various evidence-based approaches have been described in the literature regarding C/PHNs engagement with fire safety topics. For example, a fire alarm installation program in Maricopa County, Arizona, involving a partnership between a nursing school and fire department resulted in 94% of homes visited receiving at least one working smoke alarm at the end of a home visit (Omaki et al., 2018). This study demonstrated how partnering with home visiting nurses and fire departments can be successful to increase the number of vulnerable homes with smoke alarms. A study in north-central Kentucky found that while most participants (95%) were able to describe a home escape plan with two ways out of each room and most had an emergency place after escape (90%), none of the participants reported having ever practiced their fire escape plans. The study described how applying train-the-trainer methods can be used to improve home fire safety in vulnerable populations (Lehna et al., 2017). Other studies have shown how the use of video media as a fire safety educational tool can be an effective method for improving home fire safety knowledge, behavior, and ability outcomes over time (Lehna et al., 2014, 2015b). C/PHNs can adapt such community-based fire safety education programs to incorporate distinct features of HR building environments.
To facilitate the development of such programs, C/PHNs can seek to strengthen partnerships with fire departments and residential HR building management agencies. A simple and commonly administered approach to home fire safety programs centers on the distribution and installation of smoke alarms. This approach has effectively reduced fire-related deaths and injuries in many types of populations (Istre et al., 2014; Yellman et al., 2018). Such programs are most effective when combined with fire safety education, low-cost or free equipment installations, and lithium battery alarms (Cooper et al., 2012).
Many C/PHNs in this study suggested systems-level changes to be made to assure fire safety in HR buildings in their community. One of the major needs identified is the installation of fire sprinklers to protect residents and their homes. While all newly built residential HR buildings must include fire sprinklers, many cities in the United States have aging residential HR buildings that were built before fire safety codes requiring fire sprinklers and advanced fire safety systems. In many municipalities, these structures are not required to be retrofitted to the current standard, leaving residents who live in these buildings at a greater risk for injury or death during a building fire. Some municipalities have passed legislation requiring the retrofitting of some or all HR buildings with sprinklers. Other municipalities have struggled to act, even after a tragedy occurs. In the wake of a HR fire in a building lacking fire sprinklers in Minneapolis, the Minnesota Department of Public Safety (2020) released a report that found that five people who died could have been saved by fire sprinklers. C/PHNs can contribute to advocacy efforts by lobbying to achieve safer health and housing policies related to HR fire safety. The National Fire Protection Agency (NFPA, n.d.) provides toolkits that nurses can use to advocate for policies supporting fire sprinkler installation.
Limitations
This study was limited by its involvement of a small number of participants from one U.S. city. Differences may exist in other locations regarding C/PHN practices, as well as statutes and policies regulating residential HR buildings. The study involved assessing C/PHNs awareness of fire safety risks and perceived barriers faced by clients who live in HR buildings. Further study should include direct input from clients to determine if C/PHNs’ perceptions accurately reflect the experiences of HR building residents. The study used a qualitative descriptive method, which is limited in that it only describes the phenomenon studied, and cannot be generalized to other settings.
Implications for Practice
This study provides valuable knowledge regarding C/PHN awareness of the fire safety risks and barriers faced among clients who live in HR buildings. Findings from this study identify specific populations that experience greater vulnerability to HR fires, such as older adults, persons with mobility or sensory deficits, people who speak languages other than English, and people who have moved to the United States from other countries. Perspectives from C/PHNs with experience serving these populations highlight the ways that may be magnified for these groups in the event of a HR fire in their building. Insights gained from this study provide starting points for developing C/PHN interventions for improving residential HR occupant fire safety. Such information may form the basis for future research or programs to train C/PHNs to more effectively serve their clients and promote fire safety in residential HR building communities.
Conclusion
While C/PHNs are very much involved in public education regarding household and community emergency preparedness efforts, findings from this study suggest that more can be done to ensure C/PHNs have the knowledge, skills, and tools to improve fire safety for clients and families who live in residential HR buildings. C/PHNs in this study were aware of the fire safety risks and barriers experienced among HR building occupants. Most participants had felt concern regarding their clients’ fire safety, but only a small portion had taken action to address concerns. Further research on this topic is recommended to inform new tools, outcome metrics, public education materials, and policies aimed at improving residential HR building fire safety. Residential HR fire safety is a public health issue that C/PHNs should be increasingly concerned with as population density in urban areas continues to rise in our country and globally.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
This work was supported by the Association of Community Health Nursing Educators (ACHNE) under the 2019 Small Research Grant Award #2.