
Abstract
The annual costs of influenza are in the billions of dollars, with employers bearing substantial burdens. Yet, influenza vaccine uptake is sub-optimal. A random survey was administered to employees at a Midwestern public university using mixed quantitative and qualitative methods to identify the rate, characteristics, and barriers of self-reported flu vaccine uptake during March-April of 2012. The lowest uptake was among adults, ages 18 to 49 (29.8%), even though they are included in universal recommendations. Multiple regression analysis adjusted for demographic confounders showed an increase in self-identified protective hand hygiene behavior among those who reported influenza vaccine uptake compared with those who did not. Qualitative thematic analysis revealed contextual accounts of why vaccine uptake was declined including structural, perceptual, and knowledge barriers. Implementation and evaluation of novel multicomponent worksite vaccine interventions tailored to reach young and middle-aged employees including utilization of risk communication is needed to facilitate increased uptake.
Each year in the United States, seasonal influenza results on average in hundreds of thousands of hospitalizations (Reed et al., 2014; Thompson et al., 2004), and approximately 3,000 to 49,000 related deaths (Thompson, Shay, Zhou, Bridges, & Cheng, 2010). Molinari and colleagues (2007) estimated direct and indirect costs of influenza at US$87 billion which included 31.4 million outpatient visits, 3.1 million hospitalized days, lost productivity at work, and lost years of life. Influenza vaccination uptake is the most effective strategy to prevent influenza and associated complications (Ho, Wang, & Liu, 2010). Groups at highest risk are the very young, the elderly, and those with chronic diseases. However, because the H1N1 influenza of 2009-2010 was associated with higher rates of mortality and hospitalizations in children and young adults compared with previous seasons, the Centers for Disease Control and Prevention (CDC) issued universal influenza vaccination guidelines in 2010, which include healthy adults ages 19 to 49. The new guideline has the potential to improve outreach efforts by sending one simple message for public health promotion to all age populations. This guideline is especially salient, as recent research indicates that some adults may unknowingly be at higher risk for influenza even though they may not have been diagnosed with chronic diseases, such as those who are obese (body mass index [BMI] > 30) or morbidly obese (BMI > 40), members of specific racial or ethnic groups, and women in the post-partum period (CDC, 2010; CDC, Division of Media Relations, 2010). Yet, despite universal guidelines, vaccine uptake rates remain lowest among all races in adults between the ages of 18 years and 49 years and sub-optimal among adults between the ages of 50 years and 64 years (McIntyre et al., 2013).
Approaches to increasing influenza vaccine coverage have focused on strategies in the clinical setting, including automated email reminders, mailed reminders, chart reminders, patient reminders, and standing orders (Guide to Community Preventive Services, 2014a; Poland et al., 2003; Szilagyi et al., 2005). However, recent research has found that healthy adults ages 18 years to 49 years are significantly less likely than other groups to recognize health care providers as their primary source for vaccine information and to report visiting a clinic during the autumn or winter when most vaccines are dispensed (Uscher-Pines, Maurer, Kellerman, & Harris, 2010). Moreover, Healthy People 2020 objectives are to increase vaccination rates among adults ages 18 years to 49 years to 80% (U.S. Department of Health and Human Services, Office of Disease Prevention and Heath Promotion, 2014). As such, alternative strategies are needed to achieve these objectives.
The workplace is a logical location to reach healthy adults within this group because most workers are between the ages of 18 years and 49 years (U.S. Bureau of Labor Statistics, Office of Occupational Statistics and Employment Projections, 2013); they spend nearly half of their waking hours in this setting and are a captive audience. In addition, 17% of adults were vaccinated at their place of employment during the 2010-2011 influenza season (CDC, 2011). Although workplace interventions hold the possibility to improve knowledge and beliefs, and reduce barriers to influenza vaccine uptake, further information is needed from healthy adults working in organizational settings to inform such interventions.
This study used mixed quantitative and qualitative methods to examine characteristics of those who are and are not vaccinated against influenza, and explore perceived barriers to vaccination among employees at a Midwestern public university. The CDC has recommended a three-tiered strategy in workplaces to prevent the spread of influenza: (1) getting a seasonal influenza vaccine; (2) practicing proactive hand hygiene practices and cough etiquette; and (3) recognizing influenza symptoms and staying home when ill. Hand hygiene is the gold standard for reducing the spread of pathogens associated with nosocomial infections in clinical settings (Boyce, Pittet, & Healthcare Infection Control Practices Advisory Committee, 2002). In community settings, hand hygiene interventions are associated with reductions in respiratory and gastrointestinal infections (21% and 31%, respectively; Aiello, Coulborn, Perez, & Larson, 2008).
Three hand hygiene interventions were studied in Europe and the United States with significant reductions in infectious diseases among office-based workers. Two interventions educated workers about the use of soap and water vs. hand sanitizer and found positive effects (Hubner, Hubner, Wodny, Kampf, & Kramer, 2010; Stedman-Smith et al., 2015). A third intervention found using behavioral recommendations about hand hygiene also reported an effect (Savolainen-Kopra et al., 2012). Community guidelines for healthy hand hygiene practices have been issued by the CDC (2013). Recent research has found associations between health behaviors and reduced likelihood of influenza vaccine uptake, in addition to an association between increased physical activity and increased likelihood of vaccine uptake (Takayama, Wetmore, & Mokdad, 2012). However, little is known about the association between influenza vaccine uptake and health promoting hand hygiene behaviors among workers, or worker demographic characteristics associated with vaccine uptake among public university employees. Quantitative surveys have been used to determine barriers to vaccine uptake (Blue & Valley, 2002; Harris, Maurer, & Lurie, 2009; Johnson, Nichol, & Lipczynski, 2008; Ofstead et al., 2013; Shahrabani & Benzion, 2010); however, few, if any, qualitative research studies have focused on healthy working populations to identify perceived barriers. A qualitative approach has the potential to yield a real-world, contextualized perspective to inform interventions (Creswell, 2012).
Method
A voluntary online survey was administered via Survey Monkey to a random sample of 1,600 employees at a Midwestern public university. The survey was developed to better understand baseline behaviors and attitudes regarding daily hand hygiene practices and influenza vaccine uptake among employees in this work setting. The survey was administered from March 7 to April 2, 2012. Questions were constructed to elicit information for qualitative and quantitative analyses. Items generated categorical responses through a 5-point Likert-type scale (always, usually, sometimes, rarely, never); bivariate, yes/no responses; and open-ended qualitative perceptions. An email was sent announcing the study with a link to an informed-assent page followed by the survey. At the end of the survey, a link took participants to a separate website where they could register for a drawing to receive a free US$10 gift card. The study was approved by the university institutional review board.
Quantitative Methods
Survey items for the hand hygiene behavioral construct were based on CDC community hand hygiene guidelines and existing literature; the items had been used in two previous studies that validated the constructs through exploratory and confirmatory analysis and structural equation modeling (Stedman-Smith, DuBois, & Grey, 2012, 2013). Questions elicited information on a 5-point scale from strongly agree to strongly disagree about usual hand hygiene practices including after using a toilet or urinal; handling money; coughing, sneezing, or blowing one’s nose; using a shared keyboard or keypad; using shared pens; touching public surfaces; picking up items from the floor; and before eating or handling food. The vast majority of respondents reported performing hand hygiene after using a toilet or urinal; as such, this item fell out of the model due to lack of variation and, thus, was excluded in the final composite score variable. A hand hygiene behavior score was generated for each respondent that ranged from less than 1 to 4 points and was calculated by averaging all construct items. To address missing data, 10 imputations of the parent data set were generated using a sequential regression multiple imputation method (Raghunathan, Lepkowski, Van Hoewyk, & Solenberger, 2001) that assumes data were missing at random. Descriptive statistics were delineated by flu vaccine status (did not receive/received). Multivariable logistic regression was used to analyze the odds ratio of influenza vaccine uptake by demographic characteristics. Multivariable linear regression tested hand hygiene behavior scores by vaccine status and included potentially confounding factors that could influence hand hygiene practices. The imputed datasets were analyzed using the statistical methods described, and parameter estimates were combined using the Rubin (1987) variance formula to produce estimates that incorporate missing-data uncertainty.
Qualitative Methods
Two questions were inserted in the survey to assess vaccine uptake: (1) “Did you receive an influenza vaccine during this flu season? (yes/no). (2) If no, please explain why you did not.” Descriptive thematic analysis was completed separately by M.S.S and C.L.Z.D using techniques developed by Corbin and Strauss (2008). Transcripts were read in hard-copy, and over-arching major themes were identified using open and axial coding and written memos. Researchers met, agreed upon major themes, and developed a schematic pattern of code identification using numbers. The data were transported to an Excel spread sheet. Several iterations of line-by-line coding were conducted independently by the two researchers, using constant comparative analysis, followed by sorting and re-sorting of the Excel spreadsheet according to the numerically identified themes. An audit trail was generated during qualitative data analysis to document decision-making processes. Cohen’s Kappa coefficient for interrater reliability (IRR) was calculated between the final coding by M.S.S. and C.L.Z.D. (Creswell & Clark, 2011; Gordis, 2000). Final negotiation led to agreement on one remaining difference in coding after IRR was calculated. A third team member who did not conduct qualitative data analysis (D.M.K.) reviewed the qualitative data set, coding, and memos for credibility.
Results
A total of 1,600 surveys were randomly distributed via email from a potential 5,504 employees. From these, 47 emails were either non-functional or had blocked all internally sent surveys via Survey Monkey. Approximately, 23% participated (361 / 1,553). A majority of respondents were female (72%), self-identified as non-Hispanic White (86%), and had completed graduate degrees (60%). Respondent ages ranged from 22 years to 72 years. Greater than 33% reported raising young children in their households, and nearly 33% were employees that reported also taking courses at the university. Average household income ranged from US$11,000 to greater than US$500,000. Of these, 95.3% (344 / 361) replied to the questions pertaining to vaccine status. Approximately, 40.7% (140 / 344) reported that they did receive an influenza vaccine; 59.3% (204 / 344) said they did not receive an influenza vaccine during the 2011-2012 flu season.
Quantitative Results
Participants were more likely to report having received a flu shot if they self-identified as (a) 65 years of age and older, (b) female, (c) White or “other” race, (d) earning a household income of US$90,659, and (e) completing some community college or an associate degree (Table 1). Employees who identified as full-time students and those who were raising children in their households were less likely to report influenza vaccine uptake. Table 2 shows the response percentages for hand hygiene behaviors by vaccine uptake status. Those who self-identified as having received the influenza vaccine used more protective hand hygiene across all items. The most pronounced differences in self-reported hand hygiene behavior by vaccine uptake status were seen after sharing pens, after using a shared keyboard or keypad, and after picking up items from the floor.
Sociodemographic Characteristics by Flu Vaccine Uptake (N = 344)
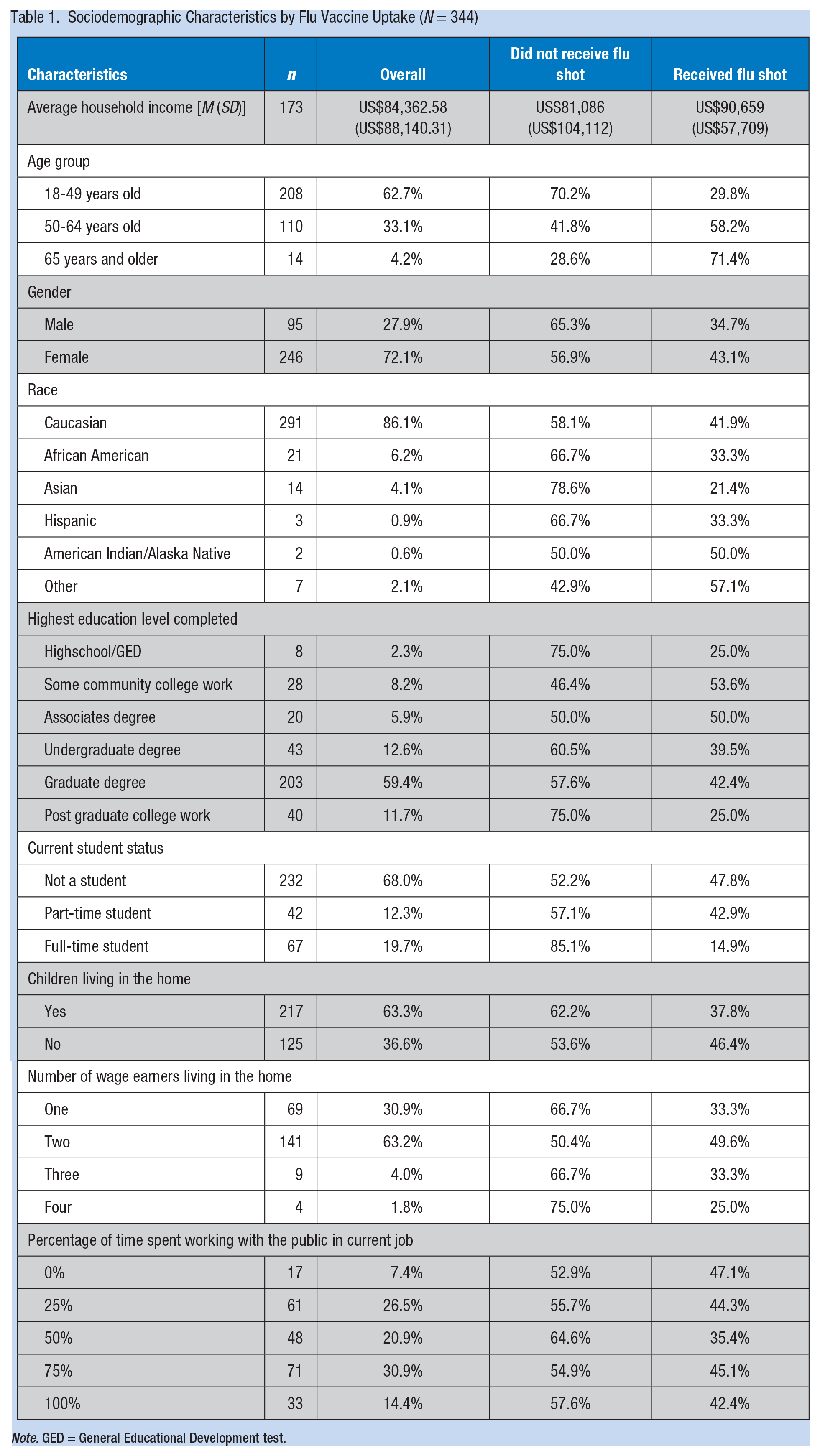
Note. GED = General Educational Development test.
Hand Hygiene Behavior Responses by Vaccine Uptake (N = 344)
Survey Question: As You Answer the Questions Below, Think About Your Usual Actions Regarding Hand Cleaning (Percentages for Each Response Are Reported)
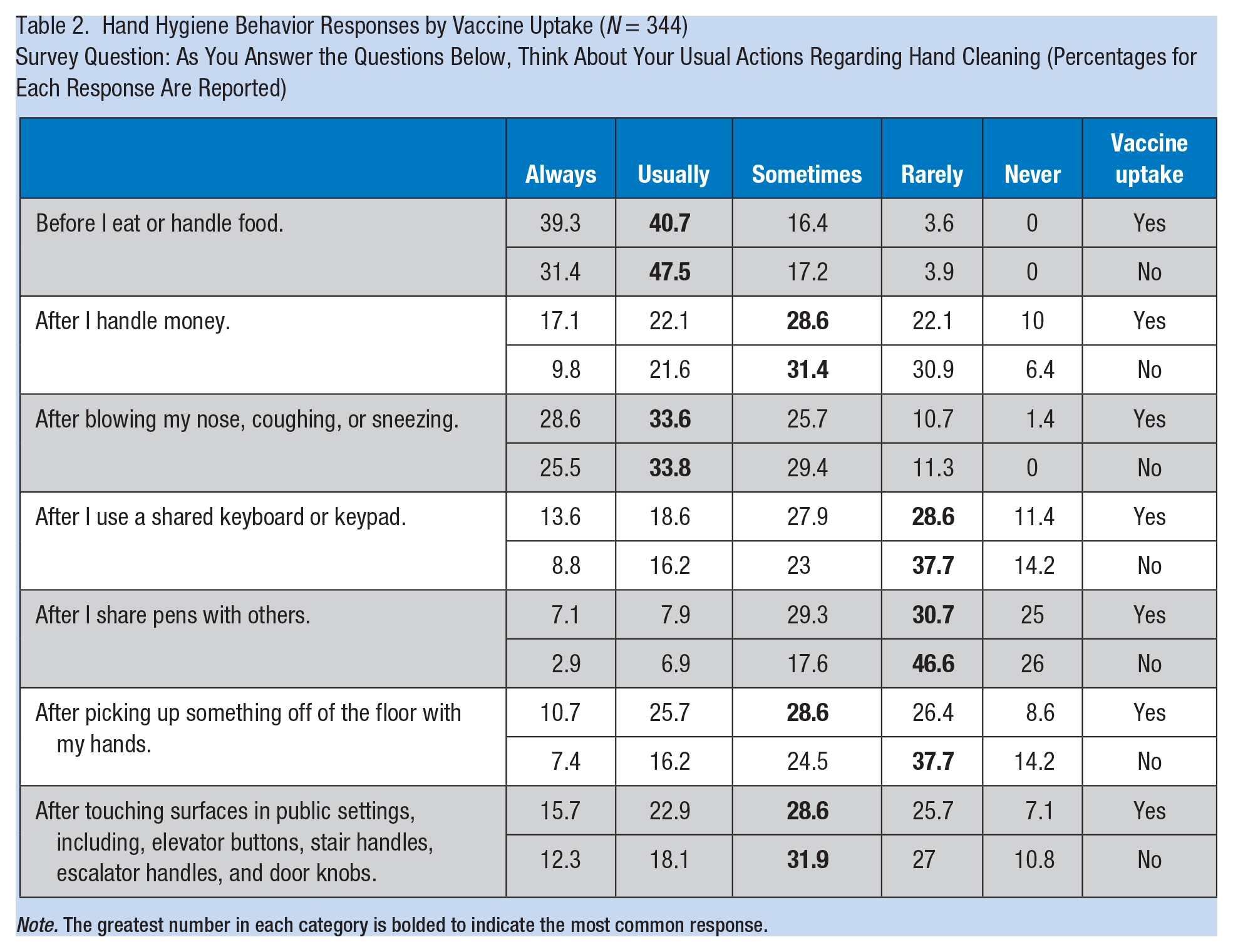
Note. The greatest number in each category is bolded to indicate the most common response.
Analytic statistics
The results of logistic regression analysis included reporting the odds ratios of influenza vaccine uptake by demographic characteristics (Table 3). Only age was significantly associated with vaccine uptake. With each year increase in age, a worker had 6% higher odds of receiving an influenza vaccination. Although females had nearly twice the odds of reporting influenza vaccine uptake than males, these results did not reach statistical significance.
Odds Ratio of Flu Vaccine Uptake by Demographics
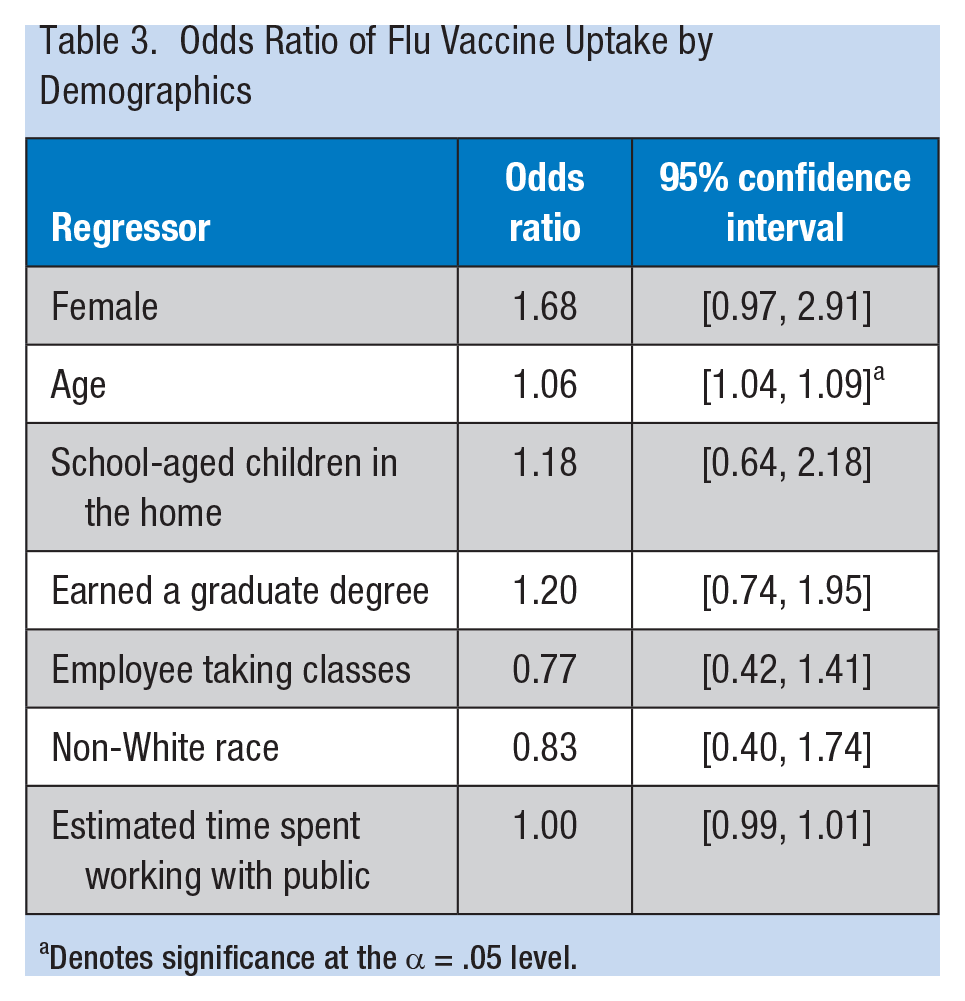
Denotes significance at the α = .05 level.
Multiple regression analysis tested the hand hygiene behavior score by vaccine status (Table 4). Potentially confounding variables for hand hygiene practices in the model included race, age, education, and gender. Unadjusted estimates showed a statistically significant relationship between flu shot status (yes) and hand hygiene behavior, with an increase in hygiene behavior scores of 0.19 among those who identified as having received the vaccine. After adjusting for confounders, this relationship became stronger, with a 0.26 increase in hand hygiene behavior scores among individuals reporting influenza vaccine uptake. In addition, a 0.31 reduction in hand hygiene behavior scores was found for each unit increase in educational level above a bachelor’s degree (Table 4).
Flu Vaccine Uptake and Hand Hygiene Behavior Score
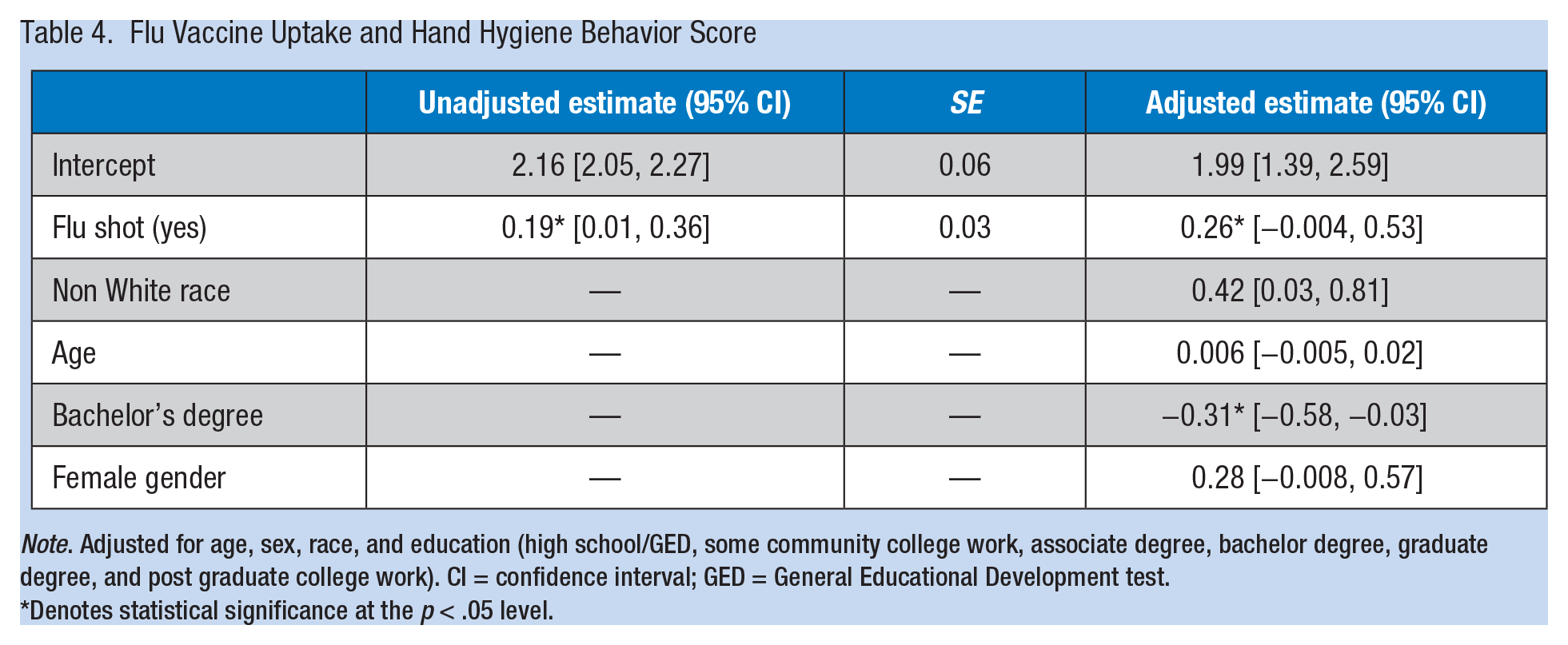
Note. Adjusted for age, sex, race, and education (high school/GED, some community college work, associate degree, bachelor degree, graduate degree, and post graduate college work). CI = confidence interval; GED = General Educational Development test.
Denotes statistical significance at the p < .05 level.
Qualitative Results
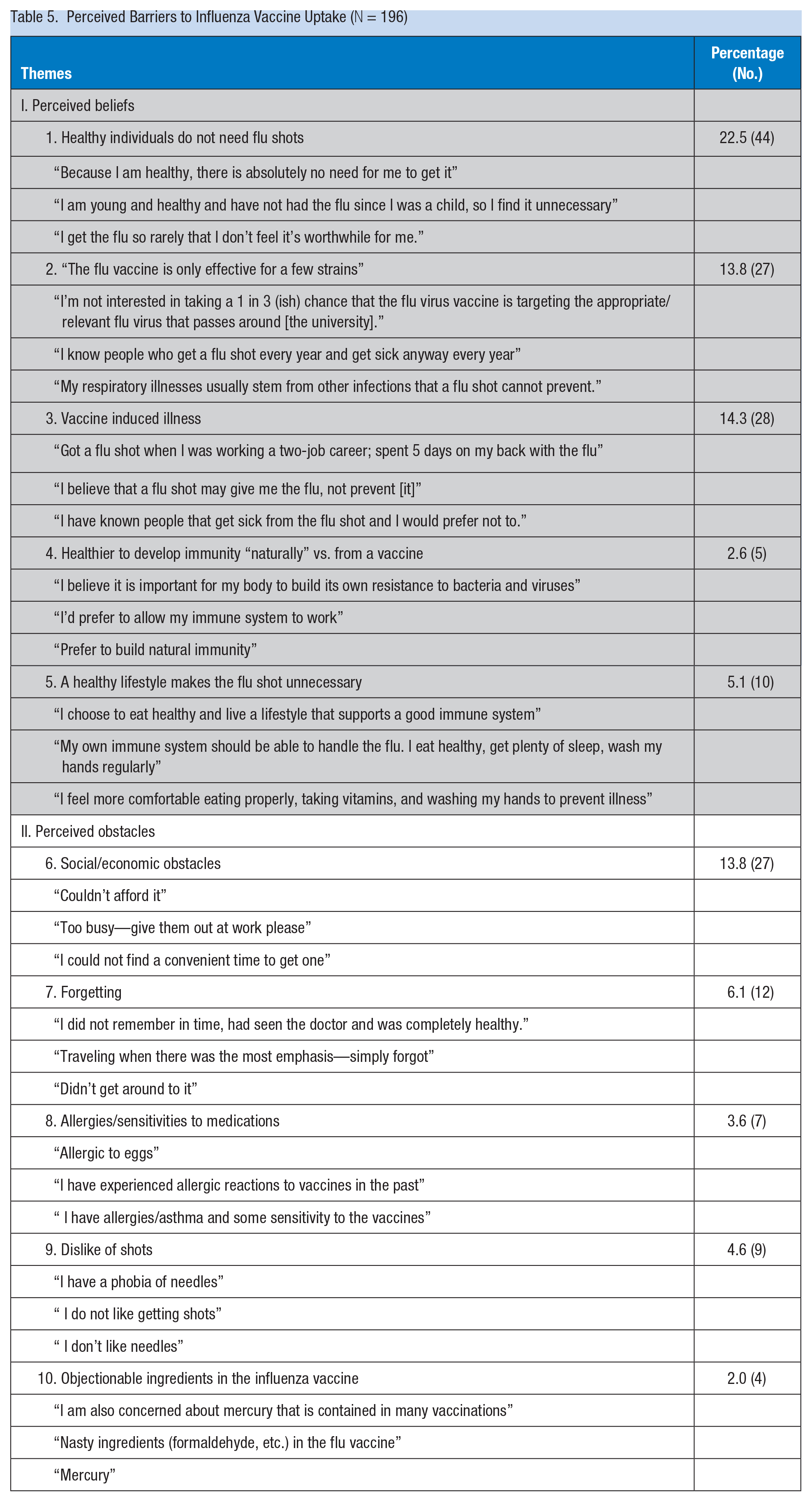
Of the 204 employees who did not receive an influenza vaccine, 96% (196 / 204) responded to the question: “If you did not get a flu shot during this flu season, please explain why not.” Two primary categories of barriers emerged through qualitative thematic analysis: perceived beliefs about the influenza vaccine and perceived obstacles. Each category was represented by five major themes. Themes for the perceived beliefs category included “I’m healthy,” “the flu vaccine is only effective for a few strains of influenza,” “it’s healthier to build one’s own immune system naturally,” “the flu shot can cause the flu,” and “I take care of myself through living a healthy lifestyle.” Themes for perceived obstacles included “encountering social/economic obstacles of convenience such as time and money,” “forgetting,” “having allergies/sensitivities to medications,” “disliking shots,” and “objecting to ingredients in the vaccine.” Representative quotes and frequencies for each theme are listed in Table 4. A third category of responses (n = 42) communicated a clear decision not to receive the influenza vaccine, yet did not specify a rationale (e.g., “it’s not for me,” “I don’t believe in them,” “I never get a flu shot.”). Cohen’s kappa coefficient for IRR of thematic analysis between M.S.S. and C.L.Z.D. was 99.5% (Table 5).
Perceived Barriers to Influenza Vaccine Uptake (N = 196)
Perceptions of drawbacks: Deliberating the decision to refuse the flu vaccine
A total of 40 respondents described two to four perceived barriers in a given response, arriving at an account of why they did not get the influenza vaccine. Descriptions revealed a vividly depicted process of deliberation which included five major themes pertaining to perceived beliefs that accounted for individual decisions to refuse the influenza vaccine. Themes 1 through 4 from Table 2 are represented in complex cognitive processes below:
I didn’t think it was necessary because the flu strain changes constantly. I’m also not one of the groups that is more susceptible to influenza (the elderly, immune compromised, an infant, a teacher, etc.), and I’m in good health. Because I am young and healthy, there is absolutely no need for me to get it. If I do get sick, beat it, my body will be healthier from the experience vs. taking the vaccine = NASTY cocktail that most people get some small variation of the flu from anyway. Also it only protects against a small amount of the virus strain where hundreds exist. . . . There are an almost infinite amount of strains of influenza, and it’s nothing more than a guess. I don’t see the point in inoculating myself for the hope that one strain of the flu won’t make me sick later. I’ve never had the flu when not getting a flu shot. I have had a flu shot twice in my life and both times I experienced a bad case of the flu. I usually get a cold or sinus infection but not the flu. I would prefer to take my chances rather than put foreign germs into my body. I have a sensitive immune system and terrible reactions to medication, so I do best with sticking to holistic approaches to health and changing my lifestyle to stay healthy . . . eating organic whole foods, taking vitamins, exercising regularly, no rugs in the house, sleep next to an air filter, and keep the house clean on a regular basis.
Contextual perceptions of social/economic obstacles
Others provided a contextual account of perceived barriers based on structural constraints, such as convenience, perceived physical constraints, economic obstacles, and procrastination that resulted in individuals questioning their personal priorities in regard to vaccination.
I had a shot scheduled three different times and each time I had to cancel my appointment due to sick kids. By the time I rescheduled it again, the doctor’s office was out of the shot. I usually get one and this was the first time in years that I didn’t. Appointments for the date it was given were filled so I was unable to get an appointment. I didn’t bother to go to the doctor or health center on a later date. In my previous workplace it was available free of charge on certain days; but here I believe we have to pay. I had intended on getting the flu shot, but unfortunately procrastinated and never got around to it. Being a public health student I know that the flu shot is beneficial to myself, friends, family, and society but for some reason I do not make it a high priority. Maybe it is because I live a healthy lifestyle otherwise, and feel that I am not at a major risk? I did not get the flu this year.
Discussion
The findings revealed characteristics associated with vaccine uptake as well as perceived barriers to receiving the influenza vaccination, several of which were based on inaccurate information. Employees age 65 years and older were significantly more likely to have received the vaccine. The lowest reported influenza vaccine uptake was among workers between the ages of 18 years and 49 years, followed by 50 years and 64 years. Vaccine uptake in this study for employees between the ages of 18 years and 49 years (29.8%) was consistent with national statistics among the general public reported by the CDC in 2012 at 30%. In comparison, uptake among employees between the ages of 50 years and 64 years (58.2%) was higher in this study than the CDC 2012 national statistic of 45% (McIntyre et al., 2013).
Those individuals who received the influenza vaccine also reported the most proactive hand hygiene behaviors in the workplace which may indicate a conscious effort among employees to practice the two behaviors together as a more thorough approach to prevent infectious disease. Perhaps these employees are aware of and adhere to the CDC three-tiered guidelines. It is also possible that these employees may be more conscientious about their health in general and practice a constellation of other recommended lifestyle habits. This study is one of the first to assess the association between influenza vaccine uptake and protective hand hygiene behaviors.
Employees who were between 18 years to 49 years were the largest group by age in this study. The most common themes for refusing an influenza vaccine were “I’m healthy” and “I’m not in a high-risk category.” These responses may indicate a lack of knowledge about universal guidelines and the potentially serious effects of influenza. In one study conducted at the beginning of the 2010-2011 influenza season, only 46.2% of U.S. adults accurately reported CDC recommendations for the influenza vaccine. Working adults were 9.6% less likely than their non-working counterparts to know they were included in universal recommendations for influenza vaccine uptake. Those individuals who were 25 years to 49 years of age had the lowest levels of awareness (Maurer, Harris, & Parker, 2012). A second survey administered to U.S. manufacturing employees found 54% were aware they should receive the influenza vaccine; even after knowledge was provided as part of a vaccine intervention, their level of awareness concerning universal guidelines did not significantly change (Ofstead et al., 2013).
The Community Preventive Services Task Force recommends on-site workplace influenza vaccine administration at reduced cost and active promotion with or without multiple components (Guide to Community Preventive Services, 2014b). Approaches have included reducing structural barriers by providing vaccine at low or no cost, and increasing convenience by offering vaccination in departments for all shifts through mobile vaccination carts, at employee events such as health fairs, and at worksite clinics. Other strategies include launching vaccine campaigns, forming multidisciplinary teams with the authority to make ongoing adaptations that foster success, engaging influential peers, generating enthusiasm for vaccination, and providing information that dispels misconceptions about influenza vaccines (Dille, 1999; Higgins, Walls, Fisher, Smith, & Humphries, 1991; Nowalk et al., 2010; Ofstead et al., 2013; Streed & Everhart, 2000). Although these interventions have effectively demonstrated clear and significant increases in employee vaccine acceptance, a persistent and substantial proportion of employees have still refused uptake.
The meaning of health and illness is a social construction (Conrad & Barker, 2010). Kata (2010) identified the underlying resistance to vaccine uptake as a “postmodern” perspective, a view skeptical of the legitimacy of science and traditional authority that may include alternative understandings of health. In addition, she asserts the need for greater understanding of this perspective so that meaningful dialogue about vaccine uptake can occur. Risk communication is a dialogical process through which information is exchanged between public health professionals and community members about the nature of risk and concerns. The interaction can lead to a sincere conversation to which professionals can respond to concerns and mutual solutions are identified (U.S. Environmental Protection Agency, n.d.). Risk communication arose in the 1980s to facilitate communication with the public about controversial environmental problems (Fischhoff, 1995) that have evoked perceptions ranging from acceptance to distrust, fear, dread, and outrage (Slovic, 1987). Increasingly, risk communication has been used as a tool to prevent and control infectious diseases (Infanti, Sixsmith, & Barry, 2013). Risk communication is not an attempt to manipulate decisions and goes beyond conveying factual information to facilitate engagement in meaningful conversation. It is a process that includes seven cardinal rules:
Making community members legitimate partners;
Planning and evaluating communication with clear objectives;
Listening to concerns;
Speaking with honesty, frankness, and openness;
Collaborating with credible sources;
Being accessible and open with the media; and
Speaking clearly and compassionately (Covello & Allen, 1988).
Several qualitative themes voiced by employees who declined the influenza vaccine are consistent with postmodern discourse (Kata, 2010). Many respondents voiced awareness of the limitations of the vaccine (e.g., only covering a few influenza strains, lack of effectiveness, unable to prevent non-influenza upper respiratory infections). A meta-analysis of 10 randomized control trials among adults 18-65 years found a pooled trivalent inactivated vaccine efficacy of 59% (Osterholm, Kelley, Sommer, & Belongia, 2012). The CDC asserts the influenza vaccine reduces influenza infections by a range of 50% to 70%, and estimates vaccine effectiveness during the 2011-2012 flu season at 47% (CDC, 2012, 2014).
Of the 196 qualitative responses from those who declined vaccine uptake, only one response reflected upon the benefits of flu vaccine. Active listening, acknowledgment of concerns, and frank discussion of vaccine limitations through the process of risk communication have the potential to facilitate substantive dialogue and elucidate underlying meanings for those individuals resistant to influenza vaccine uptake. Without sincere acknowledgment of concerns and limitations, it may not be possible for individuals to consider benefits, discuss other protective strategies along with influenza vaccine (e.g., CDC three-tiered recommendations and appropriate use of antivirals), or engage in additional communication about vaccine readiness (Lundgren & McMakin, 2009).
Limitations
Several limitations were present in this study. Although the survey was distributed randomly, the response rate of 23% limits generalization of findings because those individuals who chose to respond may differ from the target population. Compared with the university as a whole, the sample was older in age, more educated, and had a higher percentage of female and White respondents. Because the study was not a randomized national sample, the findings cannot be generalized to all public universities. Third, hand hygiene relied upon self-report and past research has found an overestimation of performance with respect to self-reported hand hygiene (Harris Interactive, 2010). With that said, the CDC has advocated hand hygiene as part of a three-tiered strategy to prevent influenza among employees; few, if any, previous studies have measured to what extent those individuals who choose to receive an influenza vaccine also self-identify as practicing protective hand hygiene behaviors. Respondent fatigue may have occurred toward the end of the survey as evidenced by an increase in missing values as the survey progressed. Although randomized imputations were used for categorical questions, the method could not be used for missing open-ended responses; however, 94.5% of participants responded to this question. The written format of this qualitative question did not permit selective probing and clarification of meaning that would occur in traditional face-to-face interviews (Rubin & Rubin, 2012). As such, 40 responses that indicated a decision not to obtain an influenza vaccine, yet did not explicate a rationale, could not be used in the analysis. It was also not possible to explore the extent to which removal of perceived structural barriers (e.g., money and convenience) would have tipped the balance of decision-making toward vaccine uptake. With that said, the written format permitted data collection from a large employee population, and vivid, contextual decision-making processes from a real-world perspective were gathered.
Conclusion
A recent review has called for easing policy road-blocks to promote the active development of a universal, game-changing influenza vaccine (Osterholm et al., 2012). Absent this, intervention research is needed to evaluate multicomponent approaches using the tenets of risk communication and novel strategies that appeal to employees age 18 years to 49 years to facilitate meaningful dialogue among those employees resistant to influenza vaccine uptake. Although more proactive hand hygiene behaviors were reported by those who also reported vaccine uptake, improvement is needed. Inclusion of the CDC three-tiered approach should be an integral component of comprehensive worksite influenza campaigns. Occupational health nurses are well positioned to take a leading role in vaccine intervention research to assess the effectiveness of such approaches.
Applying Research to Practice
Influenza vaccine uptake for adults age 18 years to 49 years remains sub-optimal, and the workplace is a strategic location for promoting universal guidelines by reaching this group. Risk communication goes beyond the conveyance of accurate information by placing emphasis on the process of communication, and has the potential to facilitate open dialogue and increased understanding of the views of employees who are resistant to influenza vaccine uptake. Occupational health nurses are highly trusted by the public and are experts in therapeutic communication which includes components of the cardinal rules of risk communication (i.e., active listening, acknowledgment of client views, and facilitation of open and effective dialogue). Occupational health nurses, occupational physicians, and health promotion professionals are well positioned to implement and evaluate novel multicomponent vaccine interventions that appeal to young and middle-aged employees and include the tenets of risk communication. The occupational health team can incorporate tenets of risk communication in face-to-face interactions with employees about influenza prevention at lunch and learn seminars, health fairs, and visits to onsite occupational health clinics. Consistent with the CDC three-tiered strategy for influenza prevention, influenza campaigns should provide information about hygiene, along with symptoms of influenza and instructions to stay home when ill.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Maggie Stedman-Smith is assistant professor, Department of Biostatistics, Epidemiology & Environmental Health Sciences, College of Public Health, Kent State University, Kent, Ohio.
Diana M. Kingsbury is doctoral candidate in prevention sciences, Department of Social and Behavioral Sciences, Kent State University, College of Public Health.
Cathy L. Z. DuBois is associate dean for administration, Professor, Management and Information Systems, College of Business Administration, Kent State University, Kent, Ohio.
Scott F. Grey is senior statistician, Department of Internal Medicine, Division of Cardiology, University of Michigan, Ann Arbor, Michigan.