
Abstract
Background
In the United States, millions of people contract the flu each year. Immunization has been shown to provide the best protection against the flu. Increasing flu vaccination rates can reduce the number of patients who get the flu and seek care for non-specific symptoms thus making detection of the coronavirus more efficient.
Method
A quality improvement project was implemented to increase the number of influenza vaccines received by employees at an onsite employer-based health clinic. Anonymous pre- and post-surveys were used to assess the flu knowledge of employees. Employees from a large financial group, who voluntarily participated, received an educational handout at the onsite health fair or at a lunch and learn. Full-time employees who carried their employer’s health insurance were eligible to participate, whereas, dependents and contract employees were excluded.
Findings
The number of employees who received the vaccination increased during the fall of 2019 (n = 406) when compared with the previous year (n = 337). Nineteen percent (n = 170) of employees completed surveys. There were statistically significantly more post- than pre-survey responses reflecting the participants’ perceived knowledge of influenza and the flu vaccine. The majority of participants in both the pre- and post-surveys reported that they learned “a lot” about both influenza and the flu vaccine.
Conclusion
Providing education and access to the vaccine in the workplace may improve flu knowledge, reduce barriers, and increase flu vaccine uptake among employees.
Background
Influenza (flu) is a contagious respiratory illness caused by influenza viruses and is easily transmitted from person to person through respiratory droplets (Centers for Disease Control and Prevention [CDC], n.d.-b). Influenza can cause mild to severe illness and even death. In the United States, approximately 9.3 million to 49 million people contract the flu annually (CDC, n.d.-a). According to the Centers for Disease Control and Prevention (n.d.-c), during the 2016–2017 flu season, the flu vaccine prevented an estimated 5.3 million illnesses, 2.6 million medication visits, and 85,000 hospitalizations associated with influenza. Immunization has been shown to provide the best protection against the seasonal flu; however, a relatively low percentage (41.8%) of the adult population receives the flu vaccine (CDC, n.d.-c). This percentage is well below the Healthy People 2020 goal of 70% immunized adults ages 18 and older.
The 2019–2020 flu season was occurring concurrently with the coronavirus (COVID-19) pandemic. The flu vaccine would not prevent a coronavirus infection; however, it is believed the flu vaccine may reduce complications associated with concurrent infections (Saplakoglu, 2020). Increasing flu vaccination rates may reduce the number of patients who get the flu and seek care for non-specific symptoms such as fever and cough thus making detection of the coronavirus more efficient. The symptoms of influenza and COVID-19 are very similar. Patients who develop symptoms but received the yearly flu vaccine are more likely to be diagnosed, treated, and quarantined for COVID-19 by healthcare professionals knowing they are less likely to have the flu as they received the flu vaccine. Receiving a flu vaccine will not protect against COVID-19; however, this is a great way to help ease the strain on the healthcare system, which is currently struggling to care for patients seeking care during the coronavirus outbreak (Saplakoglu, 2020).
In the United States, employers spend approximately 10.4 billion dollars yearly in direct cost for hospitalizations and outpatient visits for their employees who have developed seasonal flu (CDC, n.d.). McLellan et al. (2012) reported that the average employer’s medical cost increased rapidly between 2000 and 2010. Currently, there are no data to indicate a change in this upward trend. According to McLaughlin (2013), 5% to 20% of the U.S. population, or approximately 40 million people, get the flu every year, with the average direct cost of the flu being approximately $250 per person. Employers are affected by the flu due to absenteeism, which is 32% higher during flu season than the rest of the year (McLaughlin, 2013). The flu has a direct cost to employers of approximately $87 million and a loss of yearly business earnings average of $16.3 million due to the seasonal flu (McLaughlin, 2013).
According to Uscher-Pines et al. (2010), healthy adults ages 18 to 49 years are significantly less likely than other age groups to receive a flu vaccine or visit a primary care provider during fall and winter months. Therefore, the workplace is a logical place to reach healthy adults within this age group because a majority of workers are between the ages of 18 and 49 years old (U.S. Bureau of Labor Statistics, Office of Occupational Statistics and Employment Projections, 2013). Employers have a unique opportunity to offer education and access to onsite seasonal flu vaccines at low to no cost to their employees. By offering the flu vaccine to employees, employers are not only helping to prevent the spread of influenza within the workplace, but also within their community (Sherman & Fabius, 2012). Furthermore, according to Bright et al. (2012), working adults spend more than one third of their time at work, as a result, implementation of an onsite flu clinic provides employees with convenient access to the vaccine without taking any time off from work.
Education in the workplace has the possibility to improve flu knowledge and reduce barriers to receiving the flu vaccine. Education is the key to help generate better vaccination uptake. Providing educational resources to employees by either distributing an educational handout or during a lunch-and-learn activity are ways to help relay accurate information and combat flu vaccination myths. According to Wong et al. (2014), brief education can be a cost-effective strategy to increase influenza vaccination uptake and may prevent unnecessary influenza-related hospitalizations and death. By incorporating workplace education programs and offering multiple onsite flu vaccination clinics, it is believed that the number of employees who receive an annual flu vaccine will increase during the flu season (Lee et al., 2010).
The purpose of this quality improvement project was to increase the number of influenza vaccines received by employees at an onsite employer-based health clinic. This project quantitatively investigated the effectiveness of an onsite employer-based health clinic on improving the influenza vaccination rates among employees who received the influenza vaccine, by assessing onsite education of employees via an educational handout regarding influenza, influenza vaccines, and myths surrounding the vaccine, and dates and times of flu vaccine clinics were offered in the onsite employer-based health clinic.
Methods
This was a comparative, descriptive study in which quantitative data were collected in a convenience sample of 170 employees who were employed at a large financial group. The employees were either full-time (40 hours/week) or part-time (<32 hours/week), carried their primary insurance through their employer, were 18 years of age and older, and willing to complete the survey. This project excluded employee dependents, those whose insurance was provided by a significant other or parent, and contract employees who were not eligible for insurance through the employer. The vaccination rates of the 2018–2019 and 2019–2020 flu seasons were compared in this project. After the post-surveys were completed on December 13, 2019, a clinic audit was completed to assess the number of flu vaccines given during the 2019–2020 flu season from October 2019 through December 2019 and compared the results with the number of flu vaccines given during the 2018–2019 flu season.
This project began in early September 2019 by performing a clinic audit to obtain the number of employees who received the influenza vaccine for the 2018–2019 flu season from the onsite health clinic. Voluntary, anonymous pre- and post-surveys were distributed to 170 employees who were eligible to participate. The pre-survey was administered from September 25, 2019, to November 8, 2019, with the kick-off of the pre-surveys during a health fair held on September 25, 2019, outside the cafeteria, as well as, during a lunch and learn held on October 2, 2019, in a conference room outside the onsite health clinic.
The purpose of the pre- and post-surveys was to assess the employee’s knowledge of influenza, the influenza vaccine, and barriers to receiving the flu vaccine. Questions were the same for both pre- and post-surveys; however, the post-survey had one additional question which asked, “Did you receive the flu vaccine this year?” The surveys were developed to elicit information for a quantitative analysis. Questions such as “How familiar are you with influenza?” required a categorical response through a 5-point Likert-type scale (extremely familiar, very familiar, somewhat familiar, not so familiar, not at all familiar); “Have you ever received the flu vaccine?” required a yes/no response, and demographic responses for gender, age, and race were collected.
A flu clinic held by the onsite health clinic ran from October 14, 2019, to October 25, 2019, although flu vaccines were available daily, at no cost, in the health clinic for those employees unable to attend the flu clinic. Once the flu clinic was completed, eligible employees were asked to complete the post-survey between November 11, 2019, and December 13, 2019. The information provided from the post-survey responses was used to determine whether the employees perceived the same barriers, learned any new information, and if they received the flu vaccine. After the post-surveys were completed on December 13, 2019, another clinic audit was completed to assess the number of flu vaccines given during the 2019–2020 flu season from October 2019 through December 2019. The surveys were completed anonymously; therefore, it was unknown whether the same participants completed one or both surveys.
There was no incentive offered to employees to complete the surveys. Informed consent was inferred by completing the survey. The project was reviewed by the University of Cincinnati Institutional Review Board (IRB) and it was determined that IRB approval was not required for this project.
Findings
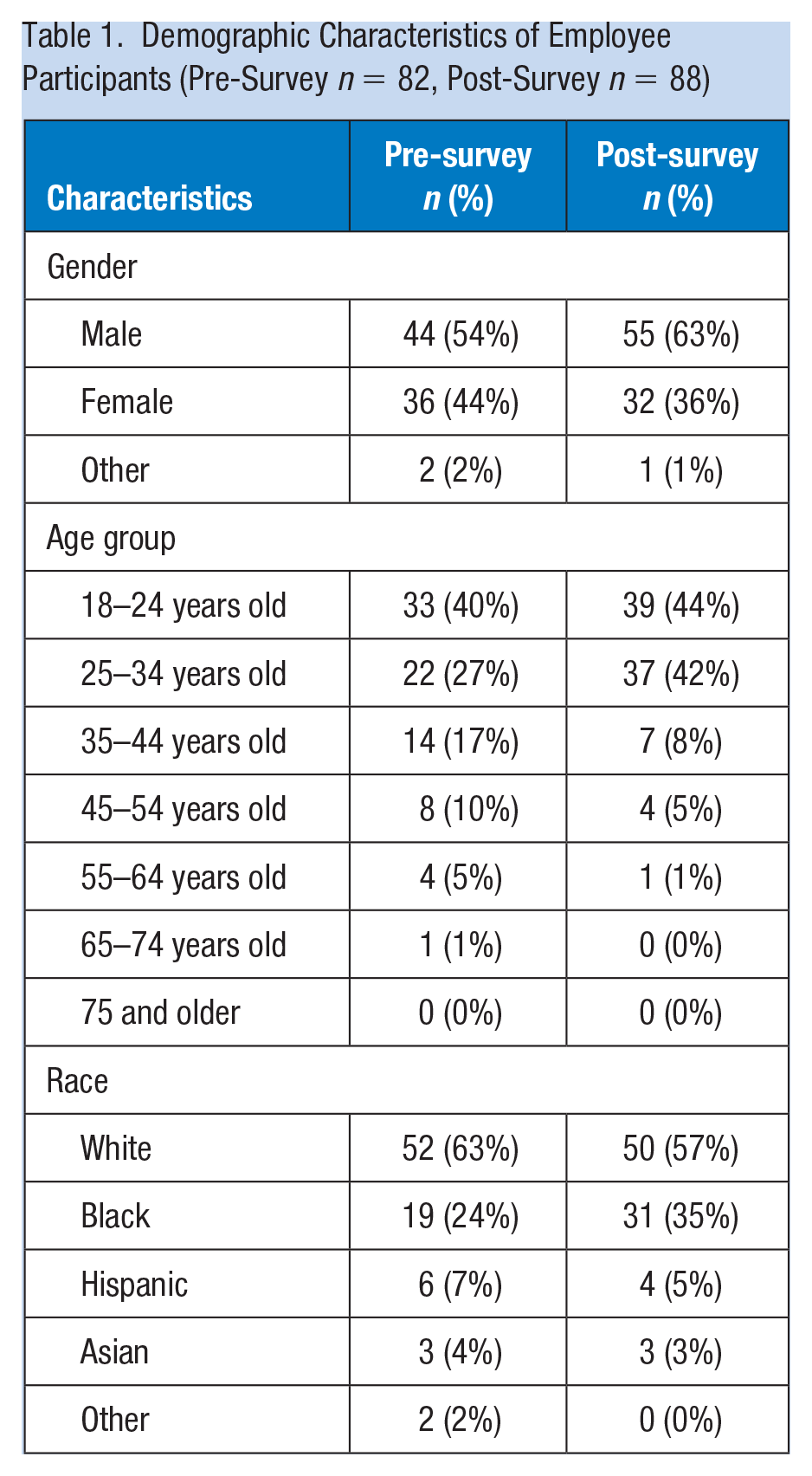
A total of 82 pre-surveys were completed out of 264 eligible employees who attended the health fair to receive the educational handout or during the lunch and learn. There were 88 post-surveys completed out of 291 eligible employees. It is unknown if these participants also completed the pre-survey and/or both surveys. Approximately, 19% of employees participated (170/910). Not all participants who completed the surveys receive the flu vaccine. The post-survey reported that 69% of the participants did receive the flu vaccine; however, it is unclear as to when or where they received the vaccine. The demographics of the employees who participated are outlined in Table 1. In the pre- versus post-surveys, respectively, the demographics showed that 54% versus 63% of the participants were mostly male, 40% versus 44% the ages of the participants were 18 to 24 years old, and 63% versus 57% were white.
Demographic Characteristics of Employee Participants (Pre-Survey n = 82, Post-Survey n = 88)
Participants reported their knowledge about influenza and the flu vaccine in both the pre- and post-surveys. In the pre- versus post-surveys, respectively, 13% versus 39% reported that they were very familiar with influenza, 15% versus 35% reported that they were very familiar with the flu vaccine, and 29% versus 44% reported that they feel that they learned a lot about influenza and the flu vaccine (Table 2). Based on non-overlapping 95% confidence intervals, a statistically significantly higher percentage of post-education respondents were “extremely familiar” and “very familiar” with influenza and the influenza vaccine than were the pre-education respondents.
Perceived Knowledge of Influenza and Flu Vaccine Among Employee Participants (Pre-Survey n = 82, Post-Survey n = 88)
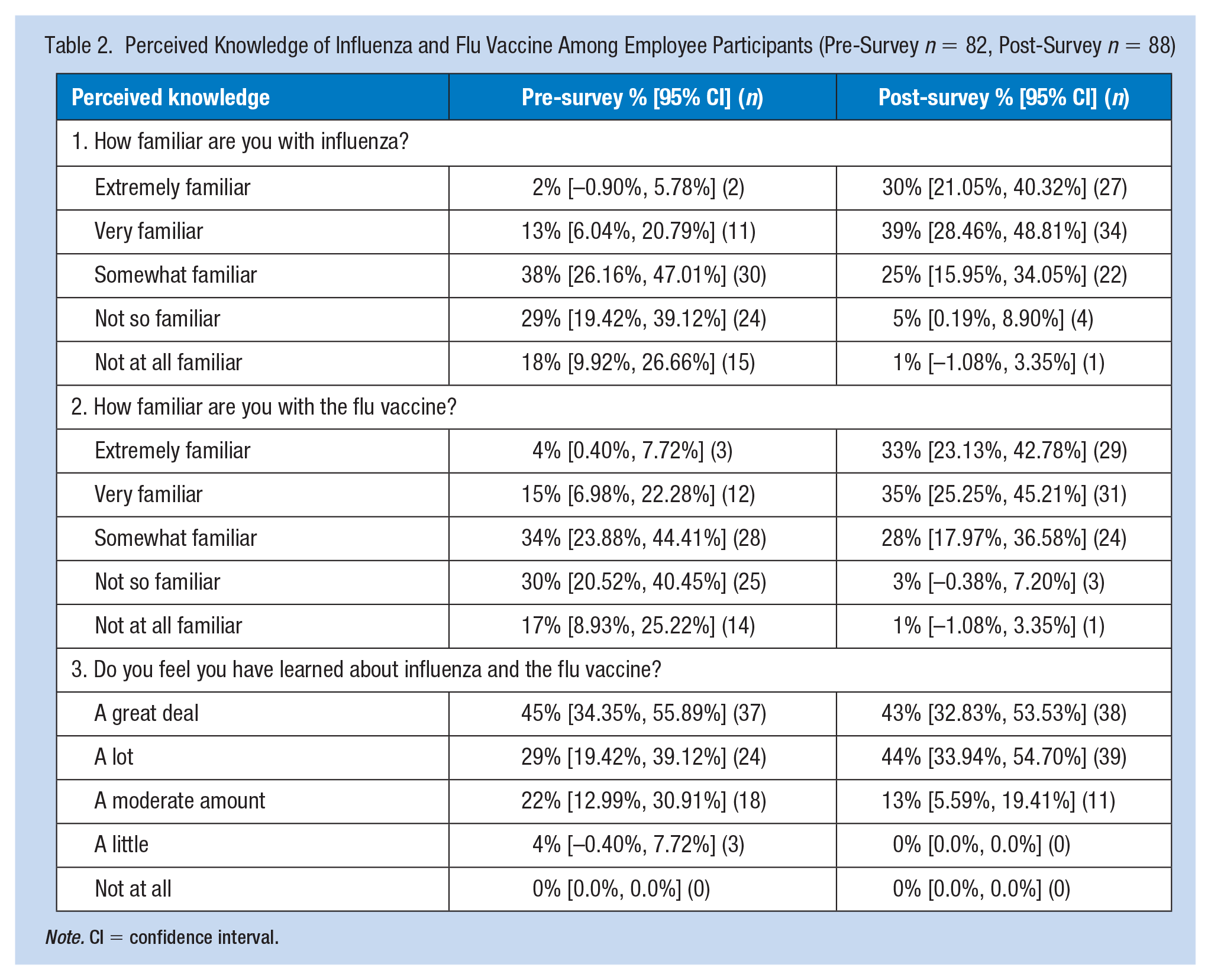
Note. CI = confidence interval.
In the pre- versus post-surveys, respectively, 59% versus 70% had previously received a flu vaccine (Table 3). Approximately 80% of the both the pre- and post-survey respondents reported that they were planning to receive the flu vaccine. Approximately 69% of the post-survey respondents reported that they had already received the vaccine this current 2019–2020 flu season. Among the employees who participated in this project, 80% reported that they planned to receive the flu vaccine while 69% of the respondents reported that they did receive the flu vaccine, this was most likely due to the project ending in December 2019, which shortened the timeframe as compared with the typical flu season period. There were no significant differences between the pre- versus post-surveys perceived plans to receive a flu vaccine, nor the vaccination status of the participants.
Perceived Plans to Receive Flu Vaccines and Vaccine Status Among Employee Participants (Pre-Survey n = 82, Post-Survey n = 88)
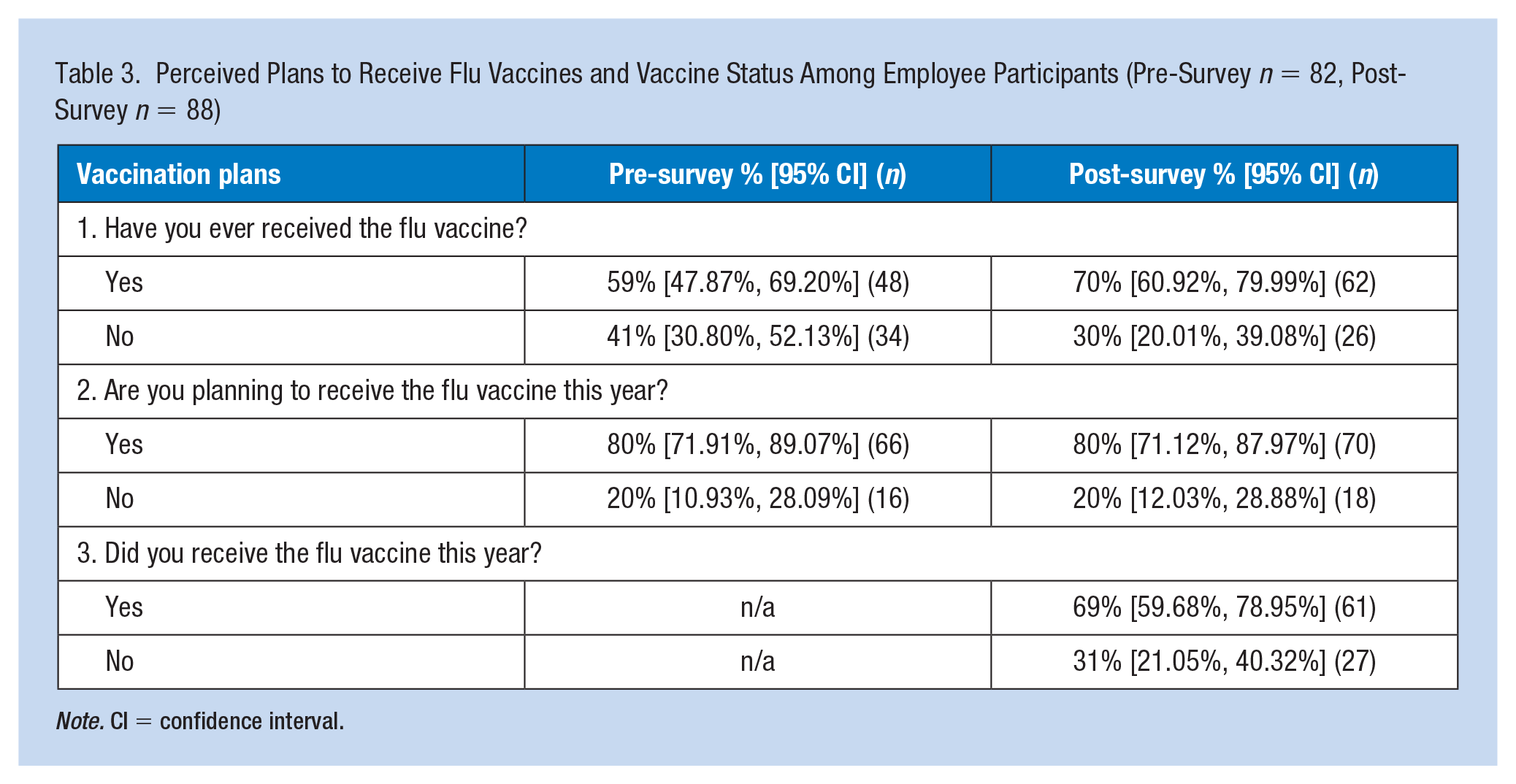
Note. CI = confidence interval.
In the pre- versus post-surveys, respectively, participants reported that the barriers to getting the flu vaccine was 32% versus 27% due to lack of access of the vaccine, 28% versus 32% side effects, 26% versus 17% cost of vaccine, 10% versus 15% fear of injections, and 4% versus 9% undisclosed other reasons (Figure 1). There were no significant findings between the perceived barriers to the flu vaccine of the pre- versus post-surveys. Both the pre- and post-surveys were similar in the barriers that prevented employees from receiving the flu vaccine. The most common barriers were side effects, lack of access, and cost.
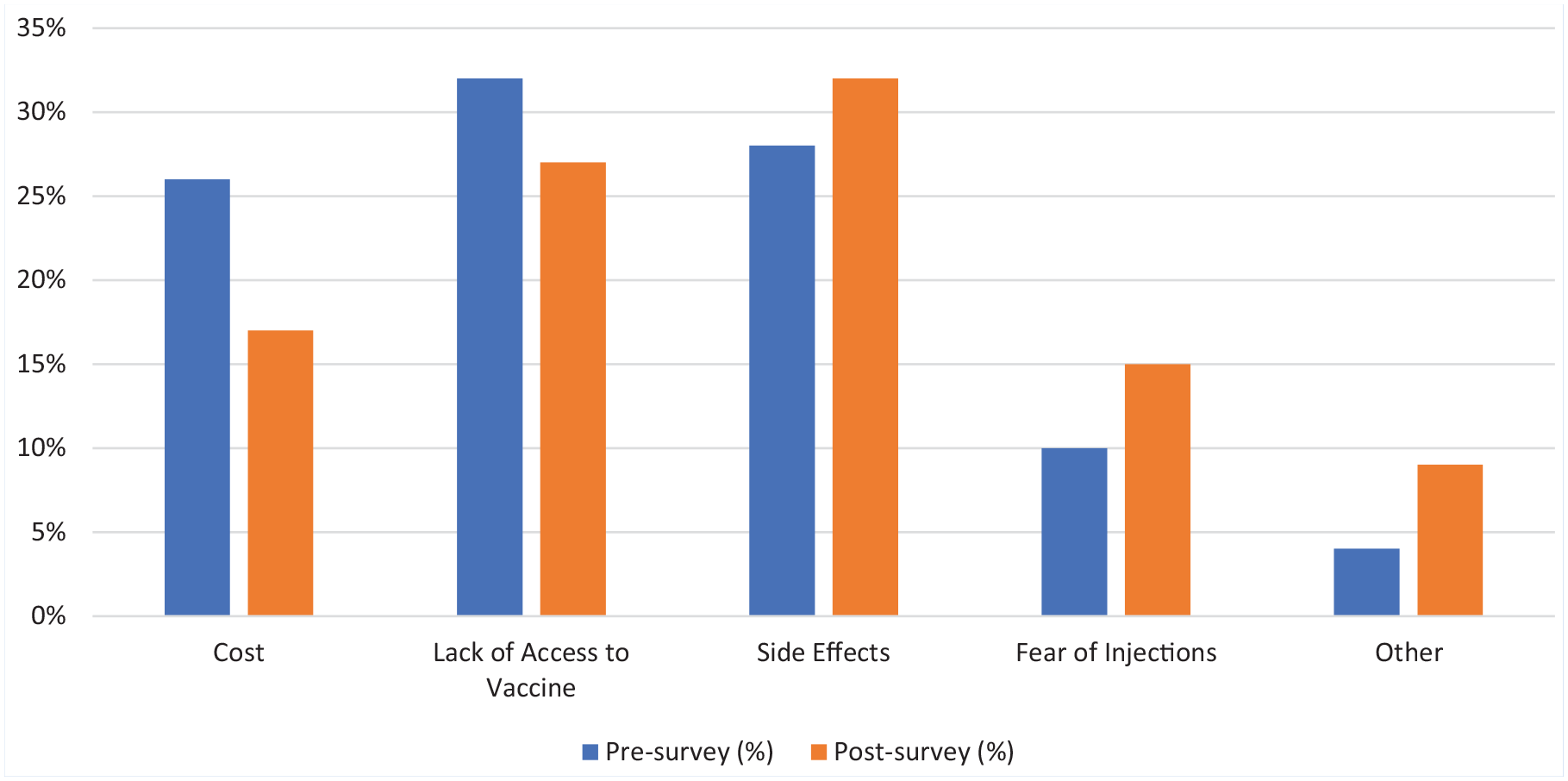
Perceived barriers to the flu vaccine.
A clinic audit was performed to determine the number of employees who received the flu vaccine during the 2018–2019 flu season which resulted in a total of 337 flu vaccines that were administered to employees in the onsite health clinic. A clinic audit was also performed to identify the number of flu vaccines administered during this project time period of October 2019 through December 2019 which resulted in 406 flu vaccines after the educational handout was distributed in the cafeteria as well as after the lunch and learn held in the conference center.
Discussion
During the same timeframe as the project, the employer-based health clinic revealed that there was an increase in the number of employees who received the flu vaccine from the months of October 2019 through December 2019. During this time frame, 45% of the adult employees received their flu vaccine through the onsite health clinic, when compared with the previous 2018–2019 flu season of 37% of the adult employees who received their flu vaccine. This finding highlights an increase in the number of employees who received the vaccine in the 2019–2020 season compared with the previous flu season. The percentage was still below the Healthy People 2020 goal of 70% immunized adults against influenza ages 18 and older; however, the percentage increased in this onsite employer-based health clinic from previous year.
In the pre- versus post-surveys, respectively, the largest population who participated in the pre- and post-surveys were between the ages of 18 and 34 (67% and 86%), which suggested that this population received the educational handout or attended the lunch and learn perhaps because this is the largest age population of employees and were more likely to get involved with health fairs and informational lunch-and-learn activities. It is unknown whether the participants received the educational intervention; therefore, these results cannot be compared directly with the CDC percentage for that age group.
Worksites are among the most common places to receive a flu vaccine and have shown that worksite vaccination programs can result in increases in employees who are vaccinated due to the large amount of time spent at work (CDC, n.d.). This project suggests that education and access to the flu vaccine in the workplace may be an attributing factor to vaccination. The authors speculate that providing education to employees may have been one reason why we saw an increase in the number of employees who received the flu vaccine onsite during this season as compared with the prior season. It is unknown whether or not the participants received the educational handout or attended the lunch and learn as the surveys were completed anonymously.
Improving access, such as providing free onsite flu clinics where employees do not have to take time off work and pay out-of-pocket for the flu vaccine, may serve as an incentive to increase vaccination rates among employees. Similar studies demonstrated that improving access to the vaccine improved flu vaccination rates. According to Ofstead et al. (2013), convenient access to free vaccines was key to vaccine acceptance among employees. Vaccinations to a large population of employees can be accomplished at a low cost, which may result in reduced employee absenteeism and presenteeism (Ofstead et al, 2013). Improving access to the vaccine while on paid time served as an incentive to receive the flu vaccine (Lee et al., 2010). Strong flu vaccine recommendations from a health care professional are a critical factor that affects whether or not one gets the flu vaccine (CDC, 2020). This project adds to these findings by showing that both in the pre- and post-surveys, lack of access to the vaccine was a barrier to employees not receiving the flu vaccination.
Employees’ knowledge of both the influenza and flu vaccine only slightly increased. The majority of respondents reported that they were “somewhat familiar” in the pre-survey to reporting that the majority were “very familiar” with influenza and the flu vaccine in the post-survey. These findings, along with an increase in vaccination rates this flu season suggested that improving employee knowledge served as a prompter to receive the flu vaccine. Although, based on the barriers reported by the participants, providing free onsite flu vaccines, in addition to an educational intervention, was a key factor in an increase in flu vaccination uptake in the workplace.
Several limitations were present in this project. The relatively small sample size 19% (170/910), was a significant limitation of this project as defined by the number of employees who chose to participate in either the pre- and/or post-survey. It is unknown if these participants completed the pre-survey, post-survey, and/or both surveys. The health fair and the lunch and learn were held during the lunch hours between 11:00 a.m. and 1:00 p.m. Therefore, all full-time employees were not present to receive the education. Responses could not be collected from employees who were not onsite during the time frame of the survey distribution, which may have led to a smaller sample size. It was not possible to ascertain the potential for selection bias if those who were more receptive to flu vaccination were more willing to participate in the surveys than those who were resistant to flu vaccination. The educational intervention (handout/lunch and learn) was held during the employees’ lunch break. During this time frame, employees may have felt rushed, which may have led them to answer inaccurately. Employees participated in this project anonymously, therefore, the employees were not tracked and could have answered either one or both of the surveys. So, while the employees included in the pre- and post-survey groups differed, the two groups were not mutually exclusive. Therefore, to the extent some employees answered only one survey, the two groups could have different knowledge. Participants in the post-survey group may not have received the educational intervention.
This project showed promising success with flu vaccination uptake during the 2019–2020 flu season compared with the 2018–2019 flu season. Future projects should include a time frame greater than 3 months to fully understand the impact of the educational intervention on the flu and flu vaccine, and the vaccination uptake among employees. During a severe flu season or pandemic such as the 2020–2021 season, the health and economic implications of the findings may be even higher among employees who receive the flu vaccine.
Conclusion
Incorporating education and offering multiple onsite flu vaccine clinics, as well as providing no-cost onsite access to the flu vaccine, have been shown to increase vaccination uptake rates (Ofstead et al, 2013). Education in the workplace has the ability to improve flu knowledge and reduce barriers to receiving the flu vaccine. Education is key to help generate better vaccination uptake. Providing educational resources to employees are ways to help relay accurate information and combat flu vaccination myths and increase flu vaccination rates among employees in the workplace. Healthy adults ages 18 to 49 years are significantly less likely than other age groups to receive flu and flu vaccine information or visiting a primary care provider during fall and winter months (Uscher-Pines et al., 2010). Therefore, the workplace is a logical place to reach healthy adults within this age group because a majority of workers is between the ages of 18 and 49 years old (U.S. Bureau of Labor Statistics, Office of Occupational Statistics and Employment Projections, 2013). According to Sherman and Fabius (2012), employers who offer the flu vaccine to employees were not only helping prevent the spread of influenza within the workplace and their community, they were also preventing negative economic impact on their businesses by less absenteeism thereby increasing work productivity and decreasing health care costs.
Applications to Professional Practice
Employees spend a majority of their time in the workplace leaving very little time to seek medical care, particularly preventive care. Employees who become sick are forced to take time off of work, thus decreasing work productivity. Employees who are educated on the importance of receiving the flu vaccine may be more likely to receive a vaccine. Incorporating onsite influenza education and no-cost flu vaccination clinics to employees may create a healthier workforce. Having a healthier workforce not only creates more productivity and decreased time off work, but it can help reduce healthcare costs that both the employees as well as the employers spend in medical cost due. Providing education and access to health care in the workplace can not only help with influenza and the flu vaccine, but can help improve the overall health and well-being of the employees.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Karen Landwehr, DNP, APRN, NP-C is a certified Family Nurse Practitioner and Adjunct Faculty for the University of Cincinnati College of Nursing. She recently finished her Doctor of Nursing Practice Degree from the University of Cincinnati. She served as the author and project leader of this Quality Improvement Project.
W. Jeff Trees, DNP, FNP-BC, CNP is an Assistant Professor of Clinical Nursing and Coordinator of Onsite FNP Programs at the University of Cincinnati College of Nursing. Served as Faculty Committee Chair for the author.
Susan Reutman, PhD, MPH, RN is an Assistant Professor and Director of Occupational Health Nursing MSN Program at the University of Cincinnati. Served as Faculty Committee Member for the author.