
Abstract
Concerns of violence in hospitals warrant examination of current hospital security practices. Cross-sectional survey data were collected from members of a health care security and safety association to examine the type of personnel serving as security in hospitals, their policies and practices related to training and weapon/restraint tool carrying/use, and the broader context in which security personnel work to maintain staff and patient safety, with an emphasis on workplace violence prevention and mitigation. Data pertaining to 340 hospitals suggest security personnel were typically non-sworn officers directly employed (72%) by hospitals. Available tools included handcuffs (96%), batons (56%), oleoresin capsicum products (e.g., pepper spray; 52%), hand guns (52%), conducted electrical weapons (e.g., TASERs®; 47%), and K9 units (12%). Current workplace violence prevention policy components, as well as recommendations to improve hospital security practices, aligned with Occupational Safety and Health Administration guidelines. Comprehensive efforts to address the safety and effectiveness of hospital security personnel should consider security personnel’s relationships with other hospital work groups and hospitals’ focus on patients’ safety and satisfaction.
Keywords
Recent data from 112 U.S. hospitals suggest the rate of violence directed against hospital workers has increased since 2012, from 4 per 10,000 full-time equivalents to 5.9 per 10,000 full-time equivalents, with rates nearly doubling for some occupational groups (Gomaa et al., 2015). In the wake of increasing attention to violence in U.S. hospitals, regulatory and industry groups have called for enhanced, comprehensive programs to maintain the security and safety of patients, hospital visitors, and staff (ASIS International Healthcare Security Council, 2010; The Joint Commission, 2010; U.S. Department of Labor Occupational Safety and Health Administration [OSHA], 2015). Law enforcement and security specialists can provide valuable expertise in performing risk assessments to recognize hospitals’ areas of vulnerability to workplace violence as well as understand the appropriateness and effectiveness of engineering, administrative, and work practice controls.
Hospital security personnel, who are typically called to provide tertiary prevention once an event has escalated, have also been recognized as a group at high risk of being assaulted (Pompeii et al., 2013; Pompeii et al., 2015) and in need of tools to recognize, mitigate, and prevent violent events in hospitals. The importance of sound policies and security personnel training have been recognized (Meyer & Hoppszallem, 2011), and many hospitals provide restraint tools and weapons to security personnel. Such provision, particularly of non-lethal intermediate weapons (e.g., oleoresin capsicum [OC] such as pepper spray, conducted electrical weapons [CEW] such as TASERs®) and/or lethal weapons (e.g., hand guns) has been debated given the ethical, legal, and financial issues surrounding the safety and well-being of both patients and staff in hospitals (Bastianelli, 2013; Greene, 2011).
Several observational studies have described hospital or emergency department security practices and policies (Blando et al., 2012; Campus Safety Magazine, 2011; Ho et al., 2011; Lavoie, Carter, Danzl, & Berg, 1988; Meyer & Hoppszallem, 2011; Peek-Asa et al., 2007), including the availability of weapons for use by security personnel. Researchers need to examine current hospital security policies and practices in diverse hospital settings, particularly as they relate to the management and prevention of violence, with emphases on occupational safety and broader contextual factors that should be considered when developing, modernizing, or implementing a comprehensive hospital-based security program.
The purpose of this study was to examine security policies and practices (e.g., hospitals’ security team characteristics and responsibilities, components of hospitals’ workplace violence security policies, and security personnel’s training in workplace violence recognition and prevention and tools to mitigate such events) in U.S. hospitals. The researchers also sought to understand the context in which hospital security practices and prevention efforts are employed, in part through an understanding of the relationship between security personnel and other hospital workers in patient care settings.
Method
A cross-sectional study was developed in which members of the International Association of Healthcare Security & Safety (IAHSS), working in U.S. hospitals, were invited to complete an Internet-based survey. A multi-disciplinary team of academic researchers and health care security program leaders developed the survey. Designed to take 15 minutes, this survey ascertained details about participants’ work experience and recommendations to improve hospital security as well as information on up to three hospitals in which they had worked: hospital demographics; type of security staff employed; hospital security policies and practices as they pertained to security personnel outfitting, role, training, workplace violence prevention and mitigation, weapons availability and use, and data collection by the security team; and interactions between security personnel and other hospital staff.
The IAHSS provided a membership list of those working in a U.S. hospital, including each member’s email address, membership status, and employer name and location. Dillman’s (2000) online survey techniques were used to recruit participants. The research topic was identified by health care security program leaders as one of importance to hospital security personnel. The IAHSS provided information about the study to potential participants through informational website and email announcements. The recruitment email, with the survey link, was sent via the Qualtrics’s secure online survey platform from the study investigator with the logos of both International Healthcare Security and Safety Foundation (IHSSF) and the academic institution at the top. Participants were not offered compensation for participation. Questionnaire data were collected through Qualtrics over a period of 6 weeks. Data were analyzed using SAS data analysis software (www.sas.com). Study procedures were reviewed and approved by the Duke University Health System Institutional Review Board.
Variables of Interest
Participants were asked to provide details on hospital characteristics (e.g., private vs. public, size, type), security policies and procedures (e.g., policy components, training, security codes, use of metal detectors, security reports, data collection related to workplace violent events), security personnel (e.g., type, appearance, coverage, roles, rapport with other staff), and characteristics of available weapons and tools (e.g., type of weapon/tool, carrying by security personnel type, time in use, training required).
Weapon was defined as a tool that security personnel may use to defend themselves or others in an event or potential event of violence, including a hand gun, K9 unit, CEW (e.g., TASER®), OC product (e.g., pepper spray, pepper foam), baton, and handcuffs. Workplace violence was defined as any form of physical abuse, verbal abuse/threat, or sexual harassment/abuse. The perpetrator of violence may be a patient/visitor, staff members, spouse/significant other (i.e., domestic violence on property), or any other individual performing an act of violence in the hospital setting.
With regard to hospitals’ security policy elements, the authors were interested in the extent to which the components aligned with recommendations of the OSHA’s Guidelines for Preventing Workplace Violence for Healthcare and Social Service Workers (U.S. Department of Labor OSHA, 2004, 2015). These components include management commitment and employee participation (including in the development, implementation, evaluation, and modification of the program), worksite analysis and hazard identification, hazard prevention and control, safety and health training, recordkeeping, and program evaluation.
The researchers were also interested in capturing information about security personnel type, which was defined by whether the worker was directly employed by or contracted to the hospital, as well as whether personnel were “sworn” or “non-sworn.” “Sworn” security personnel, typically police, sheriff, or highway patrol officers, are those who have taken an oath to uphold the law, often having completed academy training and with the authority to carry a lethal weapon, issue citations, and make arrests; in contrast, although the role of “non-sworn” (i.e., “civilian” support personnel) may also include some basic policing duties, they do not work under an oath, are not typically armed, and do not have the authority to issue citations or make arrests (Public Safety Career Information Center, 2015; “Law Enforcement Officer,” 2015).
Finally, the researchers asked participants several questions related to the interaction, including rapport between security personnel and other hospital staff. In addition to specific questions about communication between occupational groups, participants were asked to provide their “general impression of the relationship between security personnel and other staff (e.g., physicians, nurses, aides)”; response options included “excellent rapport,” “some difficulties,” and “major difficulties.” For participants who answered having “some” or “major” difficulties, they were asked to briefly describe (in a free-text response box) “the source of difficulties in this relationship and/or ways in which you think the interaction between these groups can be improved.”
Analyses
Descriptive statistics were calculated to describe the study participants’ demographic and work history characteristics, including years in health care security and type(s) of workplace violence prevention training personally received. Characteristics of the study hospitals were described as well, including demographics, type(s) of security personnel employed/contracted and their respective authorities (including use of weapons/tools), and elements of hospital security policies and procedures. Members’ employer details were used to identify and remove duplicate data from members employed at the same hospital. Distributions within hospital security characteristics, including weapons availability, roles of security personnel, and other policies/practices, were examined across hospital demographic characteristics (i.e., status, type, size, or whether the hospital was part of a larger system) and type of security personnel employed/contracted. The χ2 test was used to examine associations of interest; Fisher’s exact test was used in instances where 25% of cells had expected counts less than five.
Participants’ free-text responses, related to (a) rapport between hospitals’ security and non-security workers and (b) recommendations to improve hospital security and prevent workplace violence, were analyzed using content analysis (Patton, 2002); identified themes were summarized quantitatively and qualitatively for presentation. Free-text responses from all participants were analyzed, regardless of whether they worked at the same hospital.
Results
A total of 299 IAHSS members responded to the survey, with most (94%) being senior IAHSS members. More than half (62%) had worked in health care security for at least 10 years. Ninety-five percent of respondents were currently employed in a security role in a hospital, and one third (34%) of these participants worked in more than one hospital.
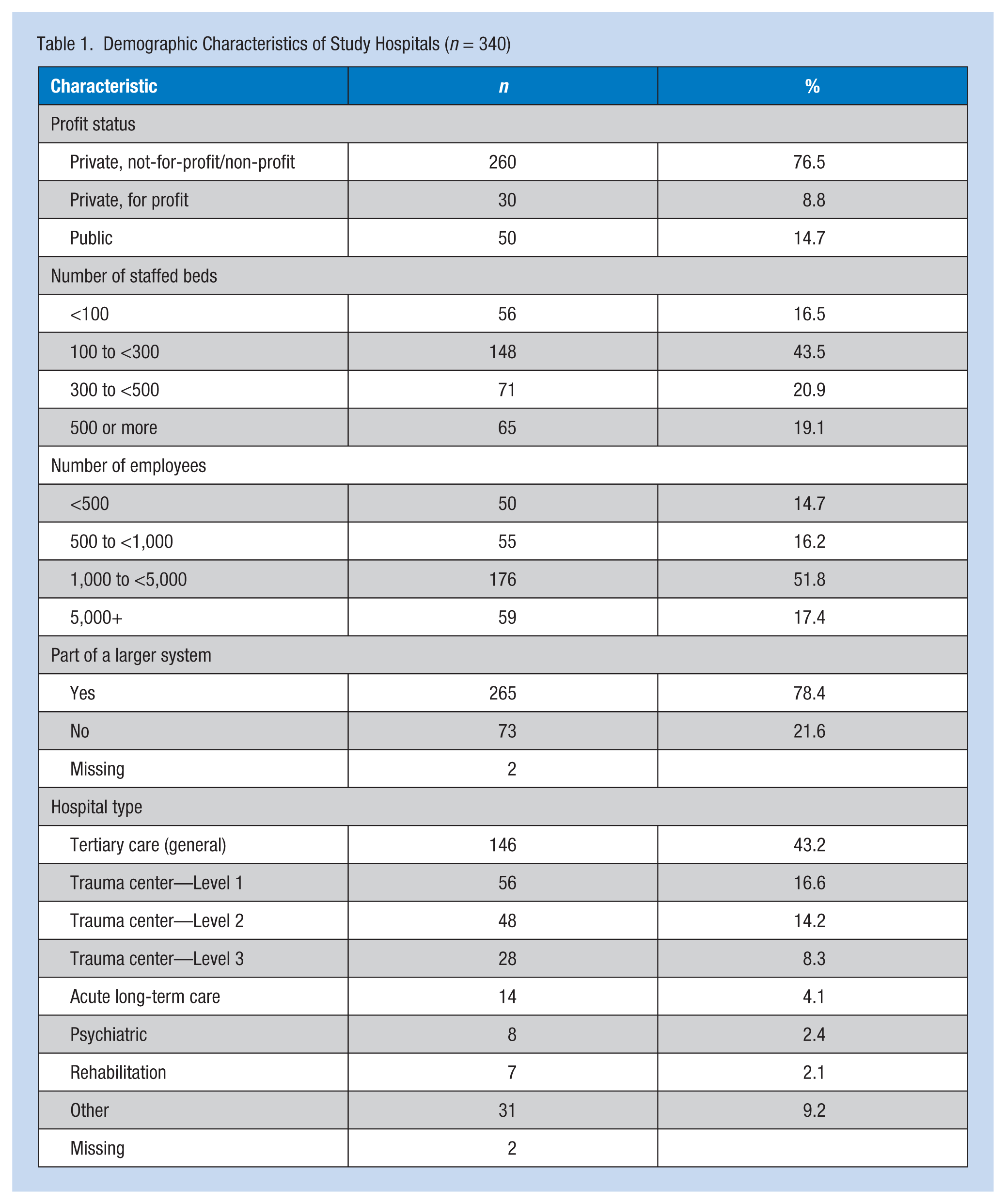
Participants provided details for a total of 340 unique hospitals in which they currently worked across 42 U.S. states. For 10 of these hospitals, data were provided by more than one participant; although data for the open-ended questions were retained from all of these participants, other data were limited to those provided by the most tenured participant. Most of these hospitals (77%) were private, non-profit/not-for-profit (Table 1). Seventy-eight percent were part of a large health care system. Common hospital types were general tertiary care (43%) and trauma centers (39%). Two thirds (69%) of the hospitals employed more than 1,000 employees.
Demographic Characteristics of Study Hospitals (n = 340)
Hospital Security Policies and Procedures Related to Workplace Violence
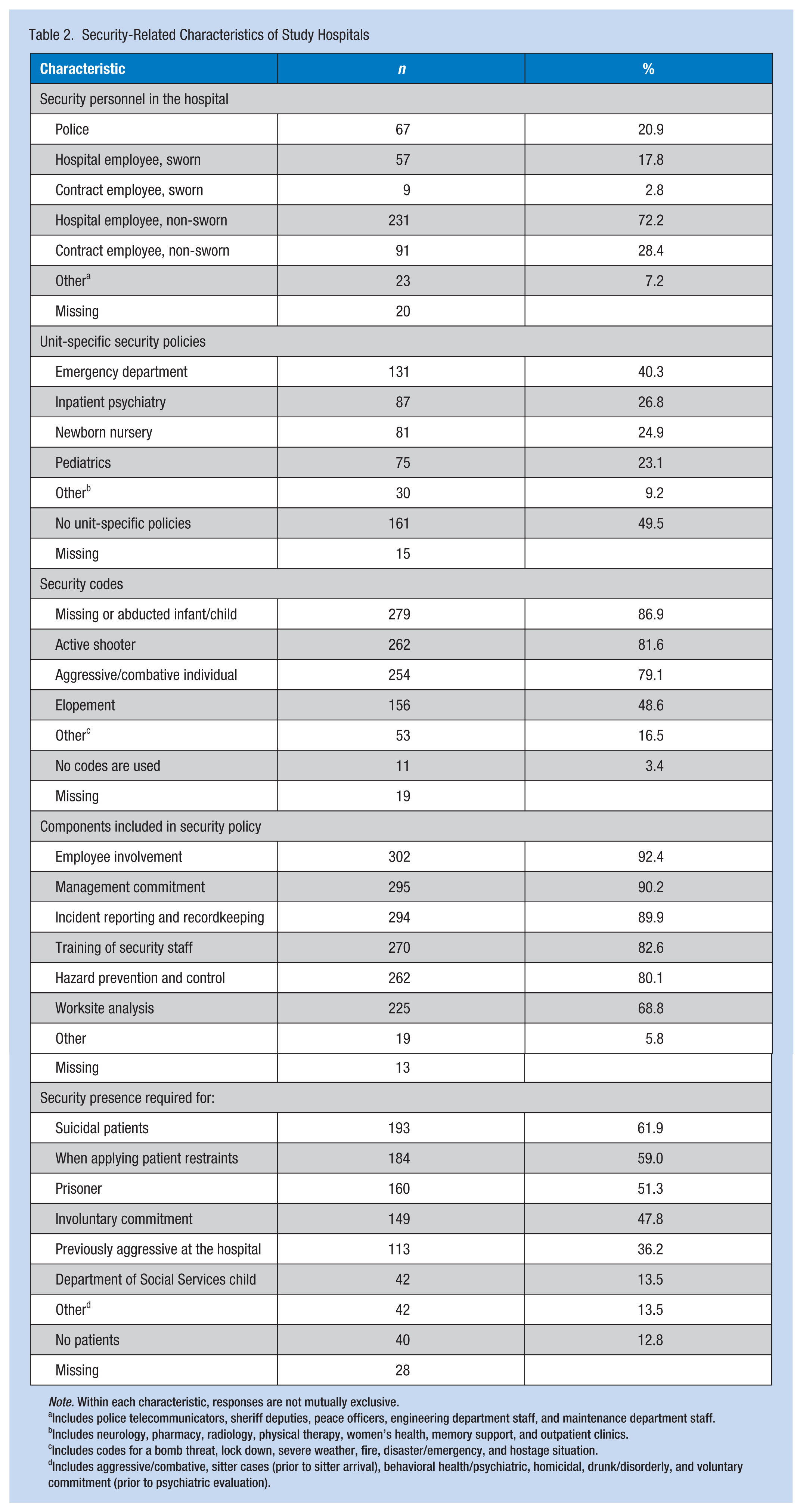
Nearly all hospitals’ security policies related to workplace violence (99%) had at least one of the following components recommended by OSHA included in a workplace violence policy: management commitment, employee involvement, worksite analysis, hazard prevention and control, safety and health training, and recordkeeping (Table 2). About half of hospitals (55%) had all of these components included in their security policy, and this proportion did not vary by hospital status, type, size, or whether the hospital was part of a larger system. Half of hospitals (50%) had at least one unit-specific security policy in place, most commonly in the emergency department (40%), followed by inpatient psychiatry units (27%), newborn nurseries (25%), and pediatric units (23%). The proportion of hospitals with any unit-specific policy did not vary by hospital status, type, size, or whether the hospital was part of a larger system.
Security-Related Characteristics of Study Hospitals
Note. Within each characteristic, responses are not mutually exclusive.
Includes police telecommunicators, sheriff deputies, peace officers, engineering department staff, and maintenance department staff.
Includes neurology, pharmacy, radiology, physical therapy, women’s health, memory support, and outpatient clinics.
Includes codes for a bomb threat, lock down, severe weather, fire, disaster/emergency, and hostage situation.
Includes aggressive/combative, sitter cases (prior to sitter arrival), behavioral health/psychiatric, homicidal, drunk/disorderly, and voluntary commitment (prior to psychiatric evaluation).
Most hospitals (97%) used a security warning code(s) to alert staff of a violent, or potentially violent, event. The most common type of code was for a missing or abducted infant or child (87%), followed by codes for an active shooter (82%), an aggressive or combative individual (79%), and elopement (49%). Private hospitals were more likely than public hospitals to have active shooter codes (84% vs. 69%; p = .0125), and tertiary care hospitals were more likely than trauma centers to have a code for aggressive/combative individual (83% vs. 73%; p = .0413). Compared with larger hospitals, smaller hospitals were more likely to have codes for active shooter (86% vs. 75%; p = .0151) and aggressive/combative individual (86% vs. 68%; p < .0001).
Metal detectors were used in one third (33%) of hospitals. At these hospitals, metal detectors were most commonly placed in the emergency department’s main entrance (40%); they were rarely placed at the main hospital entrance (3%). Metal detectors were more likely to be used in larger hospitals compared with smaller hospitals (44% vs. 26%; p = .0009), including at the emergency department main entrance (22% vs. 8%; p = .0005). Hand-held wands or other portable metal detecting devices were used in 17% of hospitals.
Hospital Security Personnel Types, Training, and Roles
Hospitals employed and/or contracted with a variety of types of security personnel, with the most common being non-sworn security personnel employed by the hospital (i.e., not contracted; 72%). Police officers were present in 21% of hospitals. The presence of non-police security personnel did not vary by hospital characteristics. Police officer presence, however, was more likely in public hospitals compared with private hospitals (35% vs. 18%; p = .0075) and in larger hospitals compared with smaller hospitals (28% vs. 16%; p = .0108). Twelve percent of hospitals used undercover security personnel, as well, and use was more likely in trauma centers than tertiary care hospitals (18% vs. 9%; p = .0354) and in larger versus smaller hospitals (18% vs. 8%; p = .0055). Among hospitals with undercover security, 90% of all other security personnel were outfitted in a “hard look” (i.e., typical look of a police officer, often with garrison belt, metal badge, and hat). Among hospitals without undercover security, 70% had security personnel outfitted in a “hard look.” Seventy-four percent of hospitals had constant security presence in the emergency department.
Eighty-seven percent of hospitals required all hospital security personnel to receive training specific to workplace violence. This proportion did not vary by hospital status, type, size, or whether the hospital was part of a larger system. Most hospitals (98%) themselves offered some type of workplace violence training to their security staff, including that related to general workplace violence (83%), crisis intervention (82%), active shooter (77%), and conflict management (68%). Many hospitals required non-security staff to receive workplace violence training as well, often including direct patient care staff (64%), housekeeping (28%), food service workers (27%), and facilities’ workers (4%). Some hospitals required training of workers within particular units or areas, notably the emergency department (8%) and psychiatric/behavioral health patient units (7%). Fourteen percent of hospitals required all hospital staff to be trained in workplace violence prevention.
Overall, 88% of hospitals had security personnel who were permitted to handcuff. Approximately two thirds (64%) of hospitals had security personnel with the authority to restrain patients. About half of hospitals had security personnel with the authority to issue citations to (54%) or arrest (49%) visitors or non-admitted patients. These job responsibilities were dependent on type of security personnel at the hospital; compared with hospitals without police and/or sworn security personnel presence, hospitals with police and/or sworn security personnel presence were more likely to have security personnel with the authority to arrest (92% vs. 34%; p < .0001), issue citations (86% vs. 46%; p < .0001), and restrain (94% vs. 59%; p < .0001). No differences in the authority of hospital security personnel to handcuff by presence of police or sworn security personnel were found.
More than half of hospitals required security personnel to be present with a suicidal patient (62%) and with patients on whom restraints were being applied (59%). Required security presence was also common for inmates (51%) and patients who were involuntarily committed (48%). About one third of hospitals (36%) required security presence with patients who were known to have a history of aggression at the hospital.
Most hospitals’ security teams (99%) collected data on events of workplace violence, commonly the type of event (97%), whether a physical injury occurred (95%), and perpetrator type (94%). Eighty-three percent collected information on whether a weapon was used by security personnel when managing an event. Other commonly collected details were related to whether legal action was taken against the perpetrator (collected by 73%) and whether the event resulted in an investigation by a regulatory agency (collected by 57%).
Weapons and Other Tools Available to Security Personnel
Handcuffs were the most common type of weapon/tool available to and used by hospital security staff (96%), followed by batons (56%), OC products (e.g., pepper spray; 52%), hand guns (52%), CEWs (e.g., TASERs®; 47%), and K9 units (12%). For nearly all weapons/tools, a range of 73% to 84% of hospitals had provided them for at least the previous 5 years. The exception was CEWs, with 49% of hospitals implementing them in the previous 5 years.
The proportion of hospitals with particular types of available weapons varied somewhat by hospital characteristics (Table 3). Most notable was the greater availability, in general, of weapons for use by security personnel in hospitals with police or sworn security personnel present, and similarly in hospitals with security personnel who had the authority to arrest and/or issue citations. Although differences were not always significant, weapons availability was also nearly always greater in larger (vs. smaller) hospitals, in public (vs. private) hospitals, and in trauma centers (vs. tertiary care and other types of hospitals). Across weapon types, no difference was found in the proportion of hospitals with weapons available by whether metal detectors were used, or by whether the hospital was part of a larger health care system.
Stratified by Type of Weapon, the Percentage of Hospitals With Weapons Available, by Select Hospital Demographic Characteristics and Security Practices
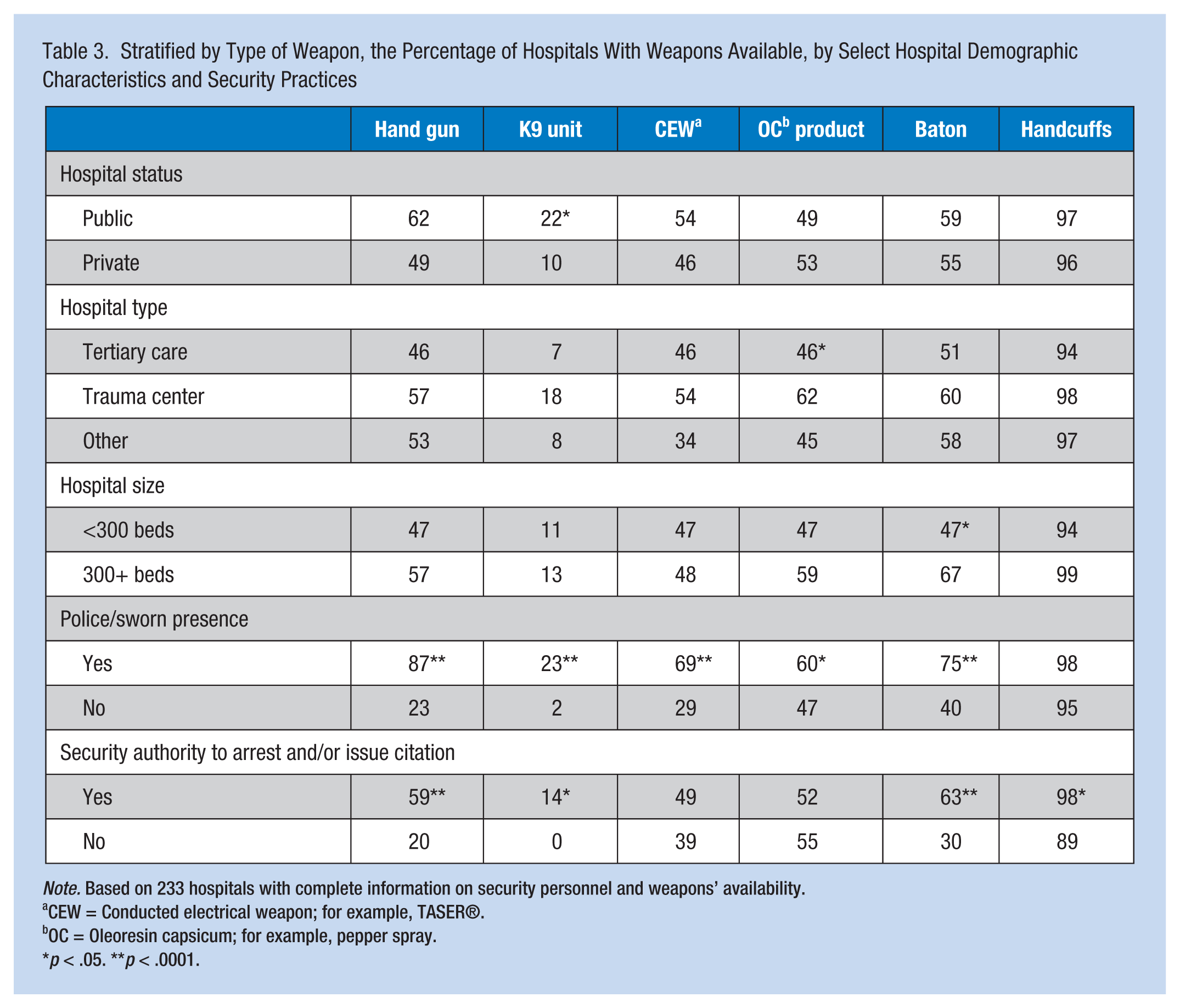
Note. Based on 233 hospitals with complete information on security personnel and weapons’ availability.
CEW = Conducted electrical weapon; for example, TASER®.
OC = Oleoresin capsicum; for example, pepper spray.
p < .05. **p < .0001.
Interactions Between Security Personnel and Other Hospital Staff
At most hospitals (92%), assistance for security services could be requested by any staff member. Requests could be made by telephone (98%), alarm button (e.g., on wall, under desk; 95%), verbally (e.g., yell for help; 90%), or through use of a pager (33%). Other methods of seeking security services included use of cell phones, radios, and Internet/email. The rapport between security and non-security personnel was described as “excellent” in 72% of the study hospitals. No hospitals were characterized as having “major difficulties.” Among the hospitals characterized as having “some difficulties” (28%), common reasons included a lack of clarity in job roles, poor communication, a need for training, and a need for enhanced respect of security personnel by other hospital workers (Table 4).
Factors Influencing Rapport Between Hospitals’ Security and Non-Security Workers, With the Percentage of Comments Falling Under Each Domain (Not Mutually Exclusive)
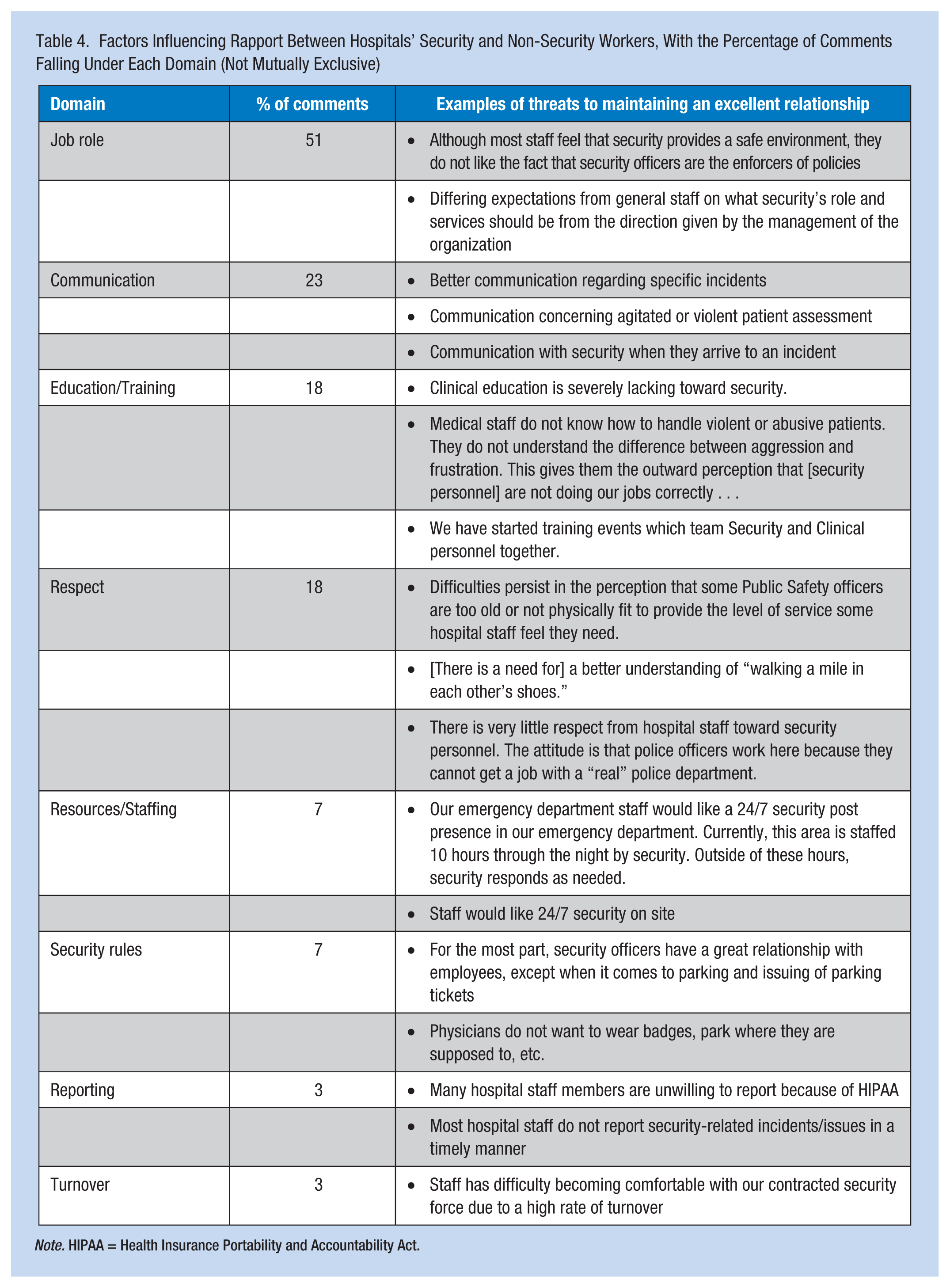
Note. HIPAA = Health Insurance Portability and Accountability Act.
Participants’ Recommendations to Improve Hospital Security Policies and Practices
The most common recommendation to improve hospital security, to prevent and manage workplace violence, was training security personnel and staff (63% of responses). Participants often suggested training all staff. Financial barriers to training were described, and participants described a need for training regarding specific topics (e.g., defensive tactics, hands-on restraint). Increased levels of security personnel staffing and nursing staffing were recommended by 21% of respondents. Fifteen percent of respondents recommended increased weapons availability for security staff and increased ability for security staff to defend themselves. Increased reporting and evaluation of data related to workplace violent events was recommended by 14% of participants. Twelve percent of participants recommended increased support from hospital administration in addressing workplace violence concerns, including hospital policies aimed at realistic prevention approaches, proactive (vs. reactive) approaches, visitor control, handling of specific situations (e.g., “active shooter”), and legal monitoring after events as appropriate. Finally, 9% of respondents recommended enhanced environmental controls, primarily physical access controls (e.g., use of metal detectors, card access).
Recommendations reflected the context in which hospital violence and related prevention efforts took place. Participants commented on the importance of integrating security programs in a hospital system, rather than independent efforts: “Effective security is an ongoing partnership. There are no ‘silver bullets.’ We seek to have security in depth and have designed some redundancies into the systems deployed. However, the critical element is an aware and engaged hospital community.” Participants highlighted broader factors that influence workplace safety as well: “Government regulations focusing on patient rights makes employees less safe or is cost prohibitive”; “Violence against healthcare workers, particularly for those assigned to the emergency department, is a growing problem. Widespread cuts of funding and programs to treat the mentally ill and addicted have mushroomed, sending surges of these patients into emergency departments. Long waits for placement and dedicated treatment has culminated in a perfect storm of fear . . .” Finally, they noted the importance of effective primary prevention approaches: “We know action is faster than reaction”; “Let’s not settle for a little. If we are going to do [violence prevention training], then do it right.”
Discussion
In this report, questionnaire data collected from members of the International Association for Healthcare Security and Safety were used to describe hospitals’ current security policies and practices, including the availability of weapons for use by hospital security personnel, hospitals’ experiences of workplace violence, and the interaction between hospital security personnel and other workers in these hospitals.
Current security practices observed in this study varied somewhat from those reported in the literature and suggest increased attention to U.S. hospital security over time, consistent with suggested increases in security-related factors (Peek-Asa et al., 2007), including funding (Meyer & Hoppszallem, 2011). Compared with a 1988 study by Lavoie et al., in this study, the researchers observed a larger percentage of hospitals with security personnel outfitted in a “hard look,” constant security presence in the emergency department, and security personnel with the authority to arrest. The Lavoie et al. (1988) study was focused on hospital emergency departments, so while a direct comparison was not made, the researchers expected the differences observed would be conservative.
The observed percentage of hospitals allowing weapons that could be carried and used by hospital security personnel was also not consistent with that reported in the literature, and the direction and magnitude of the difference varied by type of weapon. Compared with several previous studies, this study observed a greater percentage of hospitals with hand guns and/or CEWs available to security personnel. Specifically, hand guns were available in 52% of hospitals in this study, compared with 22% (Meyer & Hoppszallem, 2011) and 7% (Campus Safety Magazine, 2011) in other studies. The observed percentage of hospitals with CEWs available to be carried and used by hospital security personnel (47% in this study) was greater than in a previous study in which security personnel in 12% of hospitals carried TASERS®, with 9% of hospitals considering using such devices (Meyer & Hoppszallem, 2011). Another recent study observed TASERs® were carried by security personnel in 26% of hospitals (Campus Safety Magazine, 2011). The higher percentages observed in this study may reflect, in part, a changing profile of types of security personnel providing services to hospitals, as well as relatively recent adoption of CEWs in hospitals. It is important to note that hand guns and CEWs were more likely to be available in hospitals with police and/or sworn security personnel (vs. non-sworn security personnel only) as well as among hospitals with security personnel having more powerful legal control of perpetrators through arrest and/or issuance of citations.
The effectiveness and appropriateness of CEW use in hospitals regarding both staff and patient safety has received considerable attention in recent years. Among studies focused on CEW effectiveness in hospitals (Ho et al., 2011; Meyer & Hoppszallem, 2011), reductions in injuries to both security officers and patients have been observed. Notably, these studies suggest CEW effectiveness may be attributed to visual introduction, rather than actual deployment. Despite the potential for CEWs to provide a safer alternative to other non-lethal intermediate devices (e.g., broken bones may result from baton use, OC spray effects may reach innocent bystanders), concerns about risk of injury or death, as well as liability stemming from violations of patient care practices and standards, remain (Bastianelli, 2013; Greene, 2011; Tuttle, 2010).
Relatively few hospitals in this study had K9 units. A few reports have described the use of K9 teams in hospitals (Eddinger, 1990; Johnson et al., 2005; Katz & Spiegel, 1991); in addition to use for violence prevention and mitigation, K9 units may provide positive health benefits to patients who are anxious or depressed.
In April 2015, OSHA issued updated guidelines to prevent workplace violence in health care settings, including recommended violence prevention program elements: management commitment and employee involvement, worksite analysis, hazard prevention and control, safety and health training, recordkeeping, and program evaluation (U.S. Department of Labor OSHA, 2015). Approximately half of hospitals described in this study had all of these components included in their hospital security policy. Notably, participants recognized each of these components in their hospital security recommendations to prevent workplace violence.
Focused efforts were made in this study to examine workplace violence–related training in particular, including types of violence prevention training offered to hospital security personnel and types of hospital workers required to receive such training. OSHA guidelines support the training and refresher training of all personnel, including supervisors, managers, and security personnel (U.S. Department of Labor OSHA, 2015). Nearly all hospitals offered some type of training specific to workplace violence to their security staff. In addition to often requiring training of security staff, many hospitals required direct patient care and auxiliary staff to be trained as well. Despite the high prevalence of training among hospital security personnel, participants highlighted the need for continued efforts to enhance training availability, content, and reach.
Participants’ recommendations also provided a broad picture of the context in which hospital violence is addressed, including the influence of factors considered in hospitals, for example, the deterrent value of a security approach versus a hospital’s public image, staff safety versus patient safety and satisfaction, and provision of patient violence history information to security personnel versus conservation of patient privacy. Despite hospitals’ best efforts, achieving balance can be challenging. For example, in one study, 16% of hospitals had at least one litigation against emergency department staff (including security personnel) in the previous 5 years, with litigation focused on restraining violent patients as well as failing to restrain violent patients (Lavoie et al., 1988). Regarding patient safety versus staff safety in particular, experts have described “a regulatory disconnection” between the federal agencies tasked with overseeing patient safety and worker safety (Greene, 2011).
Through free-text responses, participants provided detailed information about the interaction between security personnel and other workers, namely, clinical personnel, in hospitals. The relationship between these two groups, described as having “some difficulties” in approximately one in four hospitals in this study, can have implications for both staff and patient safety. In addition to their integration with clinical staff in responding to an escalating or already-developed event of violence, the involvement of security personnel is required or recommended in the planning of violence prevention approaches as well as in hospitals’ architectural design stages (Meyer & Hoppszallem, 2011).
Limitations and Strengths
The cross-sectional design of the questionnaire precluded the researchers from inferring causality in the associations between factors and the outcomes of interest. The study response rate of 15%, although comparable with that of another U.S. nationwide survey of hospital security representatives (Meyer & Hoppszallem, 2011), was lower than expected and raises the concern of selection bias. Compared with all hospitals in the United States, the hospitals on which data were provided by study participants were larger (based on number of staffed beds; American Hospital Association, 2011), potentially influencing the generalizability of study findings. The questionnaire was lengthy, particularly for participants who provided details on more than one hospital. To ease the time burden, the researchers provided all invited members with a downloadable, printable worksheet to assist in the collection of hospital-related details prior to starting the online questionnaire.
Despite these limitations, this study, using a collaborative approach, adds to the literature on security practices in hospitals, including a current snapshot of specific weapon availability. The sample size allowed for examination of security practices, procedures, and experiences across various types of hospitals. Qualitative data collected through free-text response fields in the questionnaire in combination with the quantitative data provided an understanding of the broader context in which hospital security personnel work to protect others and themselves.
Implications for Practice
The role of hospital security is essential to employee safety and health; it is recommended that occupational health nurses have collaborative relationships with this team. Occupational health nurses should be knowledgeable about the roles and responsibilities of hospital security programs and their personnel when developing, implementing, and evaluating workplace violence prevention policies and procedures. They should educate themselves on current security practices and risks at their own institution, as well as work with and educate relevant stakeholders (e.g., colleagues, hospital/health system administrators, direct care providers, security, and local law enforcement) in efforts to develop and implement effective intervention strategies. When providing direct care to workers who are victims of violence on the job, occupational health nurses could serve as liaisons between security and patient care units. Occupational health nurses may be knowledgeable about violent events occurring on a unit, and adverse worker consequences, of which security personnel may not be aware. In contrast, occupational health nurses could educate front line workers about the procedures for calling security when they are threatened or at risk of harm. The findings from this study suggest a need for occupational health nurses to work collaboratively with security to ensure their safety on the job, understanding the complex day-to-day roles and responsibilities of security personnel as well as their high risk of exposure to violence.
Security personnel are at particularly high risk of exposure to hospital violence. They need continual training and enhanced tools to perform their jobs in ways that maximize their safety as well as that of other hospital staff and patients. Future robust studies examining the association between the level of weapon, restrain tool availability and use by security personnel (e.g., number of security personnel authorized to use, brandishing vs. actual deployment), and hospital violence is warranted. Furthermore, intervention implementation should not be a stand-alone effort but rather part of a comprehensive violence prevention plan. Reflective of hospital patients’ and workers’ characteristics and needs, efforts to eliminate the incidence and effects of workplace violence should address primary, secondary, and tertiary prevention through administrative support, relevant policies, and staff training. Effective involvement of various stakeholder groups may benefit from rapport between such groups in the hospital, with an emphasis on defining these groups’ roles, enhancing between-group communication, and addressing training needs. Furthermore, violence prevention programs should recognize the context in which hospital violence occurs, including the sometimes opposing, but potentially influential, factors hospitals balance.
Applying Research to Practice
Security personnel are at high risk of exposure to hospital violence, warranting continued efforts to maximize their safety as well as that of other hospital staff and patients. Availability of and authority to use weapons and restraint tools, a related topic of discussion, should not be a stand-alone intervention but rather part of a comprehensive violence prevention plan that considers the characteristics and needs of both patients and workers in hospitals. Reflective of the hospitals’ characteristics and needs, primary, secondary, and tertiary workplace violence prevention efforts should include administrative support, relevant policies, and staff training. Effective involvement of affected stakeholder groups (e.g., security, nursing staff, occupational health nurses, local law enforcement) may benefit from clearly defining these groups’ roles, enhancing between-group communication, and addressing training needs. Furthermore, violence prevention programs should recognize the context in which hospital violence occurs.
Footnotes
Acknowledgements
The authors express sincere thanks to the Working Group assembled by the International Healthcare Security and Safety Foundation. They provided valuable insight to assist in the development of the study questionnaire. Thank you to the hospital security leaders who devoted their time to completing the questionnaire.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported through a contract with the International Healthcare Security and Safety Foundation.
Author Biographies
Ashley L. Schoenfisch is an occupational epidemiologist and an assistant professor in the Duke University School of Nursing. Her research focuses on understanding and improving the safety and health of workers in the health care and construction industries.
Lisa A. Pompeii is an occupational epidemiologist and an associate professor at the University of Texas Health Science Center at Houston. Her research interests include musculoskeletal and violence-related injuries incurred by workers in the health care setting.