
Abstract
Commercial workplace violence (WPV) prevention training programs differ in their approach to violence prevention and the content they present. This study reviews 12 such programs using criteria developed from training topics in the Occupational Safety and Health Administration’s (OSHA) Guidelines for Preventing Workplace Violence for Healthcare and Social Service Workers and a review of the WPV literature. None of the training programs addressed all the review criteria. The most significant gap in content was the lack of attention to facility-specific risk assessment and policies. To fill this gap, health care facilities should supplement purchased training programs with specific training in organizational policies and procedures, emergency action plans, communication, facility risk assessment, and employee post-incident debriefing and monitoring. Critical to success is a dedicated program manager who understands risk assessment, facility clinical operations, and program management and evaluation.
The National Institute for Occupational Safety and Health (NIOSH) defines workplace violence (WPV) as violent acts (including physical assaults and threats of assaults) directed toward individuals at work or on duty. Workplace violence ranges from offensive or threatening language to homicide (NIOSH, 2002). Violence has long been recognized as a major hazard in health care although its systematic recognition as an industry-specific hazard has evolved only since the 1970s (Madden, Lion, & Penna, 1976). The National Institute for Occupational Safety and Health lists three groups of risk factors that lead to violence in health care: clinical (e.g., individual pain, fear, anger, altered mental status, history of violence, and the influence of drugs and alcohol), environmental (e.g., layout, design, and amenities of the workspace), and organizational (e.g., understaffing and long work shifts, inadequate security procedures and protocols, discouragement to report and difficulty in reporting violent incidents, acceptance by management and staff that violence is “part of the job,” and lack of staff training and preparedness; NIOSH, 2013).
This review addresses WPV prevention training and preparedness. One of the first WPV training program models was developed in a Canadian hospital (St. Thomas Psychiatric Hospital, 1976). The U.S. Veterans Health Administration (VHA) expanded the Canadian model to a broader program called Prevention and Management of Disruptive Behaviors (PMDB), which consisted of four modules: awareness, de-escalation skills, personal safety (“breakaway”) skills, and therapeutic containment (Lehmann, Padilla, Clark, & Locks, 1983). As more WPV incidents occurred in the United States, occupational health researchers classified WPV into four types focused on the perpetrator–victim relationship: criminal, customer/client (including patients in health care), co-workers, and personal relationship (often domestic partner). These categories, first described in the 1990s (Howard, 1996; Peek-Asa, Howard, Vargas, & Kraus, 1997), received widespread recognition as a useful typology for developing interventions to prevent WPV. Growing concern among health care workers led to action from labor unions such as the American Federation of Labor and Congress of Industrial Organizations (AFL-CIO) and the Service Employees International Union (SEIU) to advocate for WPV prevention programs (Rosen, 2001) and a major research project in New York on the use of environmental design to prevent violence (Lipscomb et al., 2006; McPhaul et al., 2008).
In the 1990s, states began to enact WPV prevention legislation. California took the lead by passing the 1993 California Hospital and Security Act, which required WPV prevention programs be established in acute care and psychiatric facilities. Lipscomb and El Ghaziri (2013) evaluated the 1993 California Hospital and Security Act and showed “the impact of this state law in increasing violence prevention programs and reducing staff assault rates over time” (Lipscomb & El Ghaziri, 2013, p. 308). This research and other studies have led to additional state legislation and broader scope of WPV prevention programs. For example, in a study of emergency departments in California and New Jersey, Peek-Asa et al. (2007) noted gaps in WPV prevention and advocated legislation with enforcement as a strategy to increase health care facilities’ attention to the need for these programs (Peek-Asa et al., 2007). New York and New Jersey passed laws in 2009 and 2011, respectively, requiring that health care facilities have WPV prevention programs, including worker training, a violence prevention committee, an annual violence risk assessment, a written WPV prevention plan, and methods to decrease identified risks. In 2014, Maryland approved a law requiring health care facilities to establish a workplace safety committee and a program to prevent physical assault or threatening behavior against workers. Washington State enacted a law requiring health care facilities to implement a WPV prevention plan based on a hazard assessment and offer worker training on the prevention plan and appropriate responses to potentially violent situations.
In 1996, the Occupational Safety and Health Administration (OSHA) issued Guidelines for Preventing Workplace Violence for Healthcare and Social Service Workers (Guidelines), updating the guidelines in 2004 and 2015 (OSHA, 2015). Also in 1996, NIOSH published Violence in the Workplace, Current Intelligence Bulletin No. 57 (NIOSH, 1996). In the 21st century, the continued increase in occurrence and reporting of WPV incidents led The Joint Commission to issue two Sentinel Event Alerts, one on disruptive and intimidating behavior among health care professionals (The Joint Commission, 2008) and the other on preventing violence in health care (The Joint Commission, 2010).
Despite state legislation and organizations’ alerts and warnings, violence remains a hazard in health care and social services. In 2014, the rate of injury from violence in this industry was 14.4 per 10,000 workers, 3 times the rate of 4.0 per 10,000 workers in all private industries (Bureau of Labor Statistics (BLS), News Release, 2014a). One hundred six fatalities in health care and social services were reported in 2014, 28 of which were caused by WPV (BLS, 2014b, Table A1).
OSHA’s Guidelines list five “building blocks” necessary for developing an effective WPV prevention program:
Management commitment and employee participation,
Worksite analysis,
Hazard prevention and control,
Safety and health training,
Recordkeeping and program evaluation
Management commitment and employee participation are the foundation for the other building blocks (Lipscomb & El Ghaziri, 2013). However, this review focuses on the fourth block. Worker training is an essential part of an effective and comprehensive program and the content and frequency of training, as well as how and by whom it is delivered, are critically important. The OSHA Guidelines state, “In general, training should cover the policies and procedures for a facility as well as de-escalation and self-defense training. Both de-escalation and self-defense training should include a hands-on component” (OSHA, 2015, p. 26). The Guidelines provide a list of possible training topics (Appendix A).
Method
Because of the increasing number of WPV cases coming to the agency’s attention, OSHA’s Office of Occupational Medicine and Nursing (OOMN) examined the types of training provided to workers by reviewing commercially available WPV prevention training programs. At an initial planning meeting, OSHA personnel and external WPV prevention experts established that the review’s objectives were to determine the training topics that should be covered by each program, compare these topics with specific criteria, and identify gaps in content and limitations of programs. The OOMN staff then completed a literature review and used those findings and the OSHA Guidelines’ training topics to develop a list of key training program elements to serve as review criteria (Appendix B). They identified 13 vendors that provide WPV prevention training to health care facilities and requested a copy of their training materials, offering to provide feedback to all participating companies upon completion of the analysis. Twelve vendors agreed to share their programs. The OOMN staff evaluated each program using selected review criteria. Each criterion element was coded according to the following scheme: 0 = absence of a key element in the training materials, 1 = limited presence of a key element, 2 = significant presence of a key element. Data were then analyzed to find commonalities, gaps, and program limitations.
Results
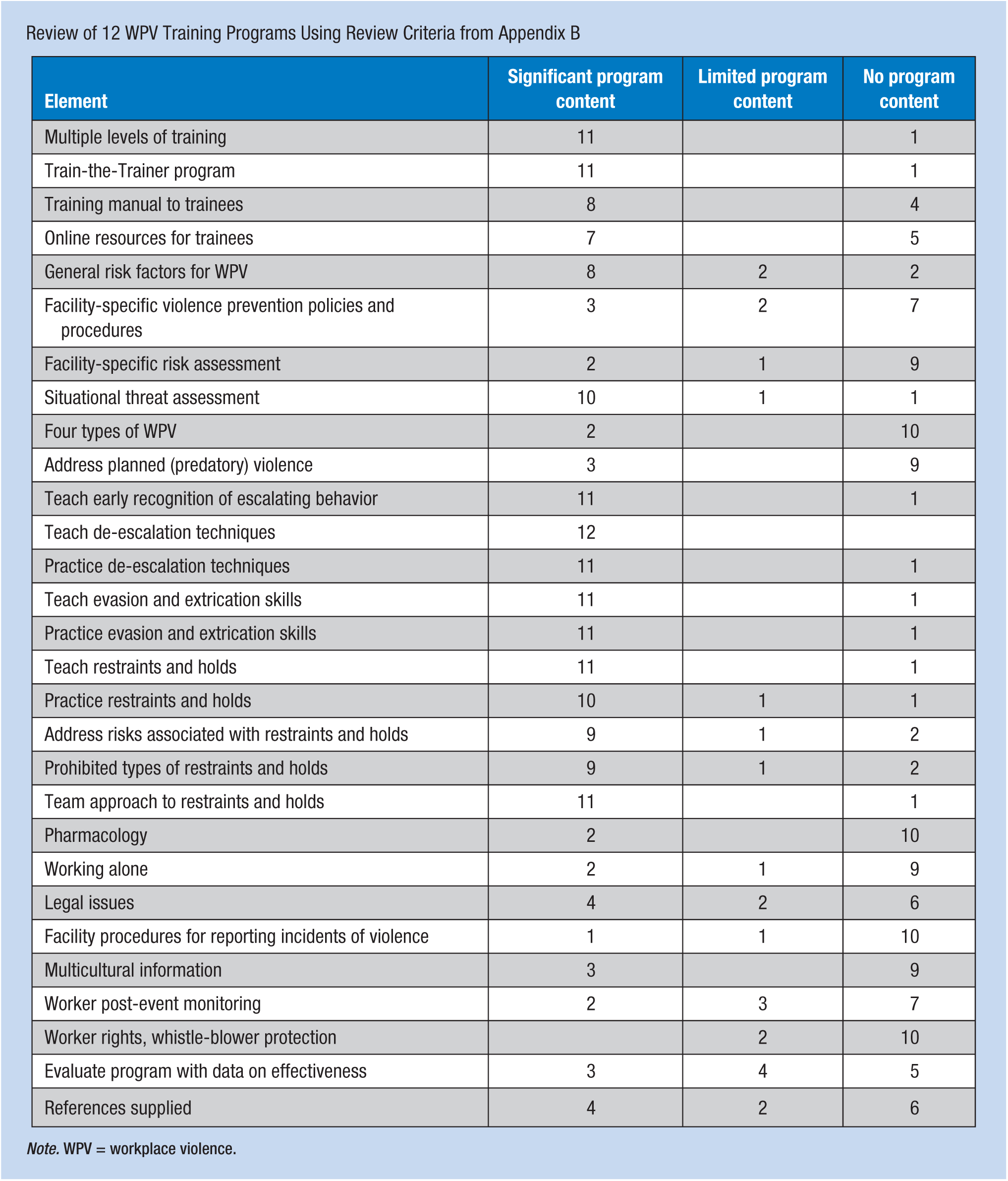
Review of the 12 training programs found variability in the degree to which the key training elements were included. Appendix C shows the results of the review with the number of programs that included each element.
The only element included in every program was de-escalation of potentially violent situations. Elements included in 11 of the 12 programs were as follows: train the trainer approach, de-escalation practice, evasion and extrication with practice, restraints and holds, and the team approach. Elements addressed with significant content by less than half of the programs were facility-specific WPV policies and risk assessment, the four types of violence, predatory violence, pharmacology, legal issues, working alone, multicultural information, worker post-event monitoring, and evaluating program effectiveness with supporting references.
Discussion
The review of WPV training programs identified a number of gaps in training content (Appendix D). First, nine of the training programs did not identify or provide any information on facility-specific risk assessment. When they stated that their training was customized to a specific facility, they meant that the client facility could choose to include or omit training topics. The lack of facility-specific information contributed to overlooking each facility’s distinctive risks. Assessing these risks is critical to overall violence prevention program design and management and to individual response when interactions escalate. In addition, only three of the 12 training programs included attention to the client facility’s policies and procedures. Employers may assume that trainers will introduce facility-specific information, but the training materials may provide no evidence of this. Management may be unaware that they need to complement the contracted training program with additional staff training on facility-specific risks, policies, and procedures.
Importantly, nine of the training programs did not address safety issues when working alone. One program included an optional module addressing this topic that could be added to the training if the facility requested it. The risk of violence to a health care worker who is working alone (e.g., admitting a patient on the night shift) is well documented and is a critical issue that should be addressed in WPV prevention programs.
Another concern is that only five of the programs addressed post-event monitoring of workers affected by a violent incident. It is appropriate for health care facilities to re-establish therapeutic relationships with patients involved in violence, but this should be coupled with therapeutic support for all involved staff. Along with any necessary health evaluation and treatment, workers may need psychological support: access to stress debriefing, counseling, and the facility’s employee assistance program.
The focus on therapeutic relationships with patients leads to a majority of programs lacking content on worker rights. One program provided information regarding protections for both patient and worker, and another that demonstrated attentiveness to patient rights also focused on workers. None of the 12 programs reviewed mentioned that violent workplaces can result in worker complaints to state agencies or to OSHA, or that these workers are protected from employer retaliation by whistle-blower protection laws.
The programs reviewed varied widely in content about restraints and holds. Training programs focused on select restraints and holds based on their theoretical constructs about WPV prevention. These programs failed to discuss that little evidence supports one approach for restraints over another. They did not describe the principles underlying holds and breakaway techniques or clearly define fundamental distinctions between passive and active or between pain-free and pain-inducing techniques. As a result, workers provided training may not gain an adequate understanding of self-defense and containment and sufficient preparation for violent incidents.
Only two of the programs included in this review addressed the use of chemical means (medications) to manage aggression, only three programs considered that violent actions are not always spontaneous emotional reactions but can also be planned (predatory) events, and only three programs included multicultural information to increase staff sensitivity to cultural differences.
Finally, the majority of training programs did not evaluate their effectiveness using a systematic data-based approach. This gap was also a significant finding in research papers examined during this project’s literature review (Farrell & Cubit, 2005; Morrison & Carney-Love, 2003; Wassell, 2008). Evaluation requires the collection of data (e.g., number and location of violent incidents) and tracking changes over time. Evaluation should also be based on research supporting the behavioral theory on which the program’s content and training methods is based. Five of the programs reviewed addressed effectiveness, three with significant and two with limited content, and only four cited extensive references in support of their approaches to WPV prevention training.
Limitations
Data analysis relied on a small sample of 12 training programs. Of these, eight programs provided actual training manuals; the other four programs only offered general program description materials. Direct communication with training program vendor managers provided additional insight into the programs. However, additional program content was not included in the information provided, so the review proceeded with limited information and may not have fully described the programs. Finally, health care facility policies and restrictions on training program content may limit programs’ criteria for a comprehensive WPV prevention training program. For example, if a facility limits the use of restraints, training does not cover all possible behavior control measures, leaving workers with fewer options for responding to potentially violent acts. The exclusion of selected knowledge and skills may cause workers to be more vulnerable to WPV.
Conclusion
This review focused on commercial, contracted WPV training programs. An effective WPV prevention training program should be integrated into a health care facility’s own comprehensive violence prevention program. This program should incorporate the five “building blocks” identified by the OSHA Guidelines (OSHA, 2015). It is likely that training programs purchased from an outside vendor will need to be supplemented with customized on-site training in organizational policies and procedures, emergency action plans, communication, facility risk assessment, and thorough post-incident debriefing and monitoring policies.
Applying Research to Practice
Occupational health nurses in health care settings should be aware of the content of workplace violence prevention training conducted at their facilities. They should notify management of training gaps (e.g., lack of facility-specific risk assessment). Nurses should understand the physical and psychological effects of workplace violence on workers who experience a violent incident and provide appropriate services and support.
Footnotes
Appendix A
Possible Training Topics Listed in OSHA Guidelines
Appendix B
Criteria Used to Review Training Programs
Appendix C
Review of 12 WPV Training Programs Using Review Criteria from Appendix B
| Element | Significant program content | Limited program content | No program content |
|---|---|---|---|
| Multiple levels of training | 11 | 1 | |
| Train-the-Trainer program | 11 | 1 | |
| Training manual to trainees | 8 | 4 | |
| Online resources for trainees | 7 | 5 | |
| General risk factors for WPV | 8 | 2 | 2 |
| Facility-specific violence prevention policies and procedures | 3 | 2 | 7 |
| Facility-specific risk assessment | 2 | 1 | 9 |
| Situational threat assessment | 10 | 1 | 1 |
| Four types of WPV | 2 | 10 | |
| Address planned (predatory) violence | 3 | 9 | |
| Teach early recognition of escalating behavior | 11 | 1 | |
| Teach de-escalation techniques | 12 | ||
| Practice de-escalation techniques | 11 | 1 | |
| Teach evasion and extrication skills | 11 | 1 | |
| Practice evasion and extrication skills | 11 | 1 | |
| Teach restraints and holds | 11 | 1 | |
| Practice restraints and holds | 10 | 1 | 1 |
| Address risks associated with restraints and holds | 9 | 1 | 2 |
| Prohibited types of restraints and holds | 9 | 1 | 2 |
| Team approach to restraints and holds | 11 | 1 | |
| Pharmacology | 2 | 10 | |
| Working alone | 2 | 1 | 9 |
| Legal issues | 4 | 2 | 6 |
| Facility procedures for reporting incidents of violence | 1 | 1 | 10 |
| Multicultural information | 3 | 9 | |
| Worker post-event monitoring | 2 | 3 | 7 |
| Worker rights, whistle-blower protection | 2 | 10 | |
| Evaluate program with data on effectiveness | 3 | 4 | 5 |
| References supplied | 4 | 2 | 6 |
Note. WPV = workplace violence.
Appendix D
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Sheila Arbury is a health scientist in the Occupational Safety and Health Administration’s (OSHA) Office of Occupational Medicine and Nursing. She is the director of OSHA’s Graduate Nurse Internship Program.
Michael Hodgson is chief medical officer and director, OSHA’s Office of Occupational Medicine and Nursing. His prior work includes oversight of the behavioral threat management and violence prevention program at the Veterans Health Administration.
Donna Zankowski is an independent occupational health nurse consultant. She is the past president of the Seneca Valley Maryland chapter of AAOHN.
Jane Lipscomb is professor, University of Maryland Schools of Nursing and Medicine and director, University of Maryland Baltimore Center for Community-Based Engagement and Learning. She is an expert in the field of workplace violence prevention research.