
Abstract
Background:
The threat of workplace violence (WPV) is a primary safety concern for home health care workers (HHCWs). WPV prevention training is a critical tool for HHCWs’ safety. Yet, most existing WPV prevention training is limited or not specific to HHCWs’ environment, the patient’s home, and neighborhood. The purpose of this study was to describe WPV prevention training, resources used, and commitment to HHCWs’ safety.
Methods:
Using a cross-sectional design, HHCWs from two sites located in Southwestern Ohio completed the Violence Against Home Healthcare and Hospice Workers survey, a 37-item survey used to describe frequency and characteristics of WPV prevention training and resources. Descriptive statistics were used to analyze the data.
Findings:
Half (n = 25) of the HHCWs received WPV prevention training. Training content focused on characteristics of aggressive/violent patients and family members (n = 19, 82.6%), but limited content about characteristics of hazardous neighborhoods (n = 15, 65.2%). Cellular phones (n = 43, 97.7%) were primarily used as a resource to promote safety, few cellular phones (n = 1, 2.3%) were provided by the agency.
Conclusions/Application to Practice:
HHCWs described WPV prevention training content and resources used to promote safety. WPV prevention training is deficient in procedures for seeking psychological care, screening patients for violent behavior, skills for self-protection, characteristics of hazardous neighborhoods, and physical maneuvers and verbal methods to diffuse or avoid aggressive behavior. Access to WPV prevention training and resources for HHCWs needs to be strengthened. Occupational Health Nurses can assist their employers with developing WPV prevention training for HHCWs.
Home health care provides highly complex nursing care as well as critical personal care services to individuals in their homes reducing the cost of hospital stays and institutional long-term care (Centers for Medicare & Medicaid Services, 2020). Home health care is projected to be the fastest growing industry in the U.S. health care sector with an estimated growth of 33% from 2020 to 2030 (Bureau of Labor Statistics [BLS], 2021). In 2020, there were more than 3 million jobs for home health and personal care aides (BLS, 2021). Providing care in the home does not come without concerns for workplace violence (WPV). Previous research demonstrates home health care workers (HHCWs) reported experiencing WPV between 2.5% and 65.7%; psychological abuse, physical violence, and sexual harassment were the most pervasive (Byon et al., 2016; Hanson et al., 2015; Nakaishi et al., 2013). A primary safety concern for HHCWs is WPV; other safety concerns included guns in the home, evening assignments, and neighborhood crime (Hanson et al., 2015; National Institute for Occupational Safety and Health [NIOSH], 2012). Among HHCWs, unique risks for WPV include working alone in unpredictable work environments, uncertain escape routes, lack of security and immediate social support from coworkers, exposure to guns, weapons, and hostile animals, caring for patients with complex psychosocial and physical conditions, and working in high crime neighborhoods (Byon et al., 2016; NIOSH, 2012). It is crucial to address and control the safety risks in the home health care work environment to protect the workforce and ensure availability of services (Institute for Healthcare Improvement, 2018).
WPV prevention training is essential for promoting personal safety in the workplace (Occupational Safety and Health Administration [OSHA], 2015). According to OSHA’s 2015 Guidelines for Preventing Workplace Violence for Healthcare and Social Service Workers, OSHA recommended that employers provide a comprehensive WPV prevention program, which includes WPV prevention training for all workers including HHCWs. Previously, Arbury et al. (2017) conducted a review of 12 commercial WPV prevention programs. Using OSHA’s WPV Prevention Guidelines as a framework, analysis revealed numerous gaps in training content and policies and procedures (e.g., safety issues while working alone, procedures for reporting WPV incidents, and agency specific policies and procedures). The agreement among both regulatory and professional agencies is training helps employees recognize potential hazards and how to respond to WPV through established policies and procedures (American Nurses Association, 2015; OSHA, 2015). However, researchers have found access to WPV prevention training and resources were severely lacking among HHCWs (Gross et al., 2013; Nakaishi et al., 2013; Vladutiu et al., 2016).
Previously, researchers found that content on WPV prevention training was not specific to HHCWs’ work environment, which is the patient’s home and neighborhood (Gross et al., 2013). WPV prevention training should be informed by risk assessments completed on the patient population, staff/provider population, and physical and social environment in which the interaction takes place (Lipscomb & Ghaziri, 2013). The purpose of this study is threefold: (a) describe employer provided WPV prevention training for HHCWs, (b) identify resources used to promote HHCWs’ safety, and (c) examine the employers/employees perceived commitment to HHCWs’ safety.
Methods
Research Design
A cross-sectional design was used to gather information about WPV prevention training elements on policies and procedures and prevention strategies. The methods and materials used for this research study were approved by the University of Cincinnati Institutional Review Board (protocol # 2019-0550).
Setting
The partnering sites used for this study were in Southwestern Ohio (United States). The first site was a for-profit, privately owned home care agency with several locations throughout Southwestern Ohio. WPV prevention training was required upon hire and annually. The second site included agencies registered with the Ohio Department of Medicaid (ODM) who were participating in the home and community-based waiver programs. Both agencies served patients who were Medicare and Medicaid eligible living in urban, suburban, and rural areas.
Study Population
Participants included HHCWs employed by the private home care agency as advanced practice nurses (APNs), physician assistants (PAs), or social workers (SWs). The list obtained from ODM included HHCWs identified as home care aides, nurse aides, licensed practical nurses, and registered nurses who provide home care services in Southwestern Ohio.
Recruitment/Sampling of Participants
Researchers used a nonprobability sampling strategy for this study. In April 2020 after IRB approval was granted, the survey was distributed via email to a convenience sample of 254 HHCWs (48 HHCWs employed with the home care agency and 206 HHCWs registered with ODM). The final sample and the total denominator of the sampling frame included 50 HHCWs. Eligible participants were required to be 18 years and older, have a valid employee email with the home care agency or registered with ODM, and be English speaking. The initial recruitment email included informed consent information. Reminders were sent to employee email addresses weekly for 3 weeks after the initial recruitment. After agreeing to participate, participants received the study survey. Compensation was a US$20 Amazon electronic gift card.
Measures
Demographic information included age (25–35 years, 35–45 years, 45–60 years, more than 60 years); race (person of color, White or Caucasian); gender (female or male); education (no college, undergraduate degree, graduate degree); occupation (nurse aide/home care aide, nurse, APN, other such as PA, SW); years worked in home care (less than 1 year, 1–5 years, 5–10 years, 10–20 years, more than 20 years); years in current position (less than 1 year, 1–5 years, 5–10 years, 10–20 years); employment status as defined by their employer (per diem, part-time, full-time). The number of visits completed after dark and the number of home visits conducted during the workday were assessed on the demographic survey. Questions for the demographic survey were derived from a literature review that discussed interventions and resources used by HHCWs to prevent WPV (Small et al., 2020).
The Violence Against Home Healthcare and Hospice Workers survey, originally developed by Vladutiu et al. (2016), was adapted with permission for this study (M. Nocera, personal communication, July 11, 2019). The 37-item tool has four sections: (a) training, policies, and procedures; (b) prevention strategies; (c) commitment to safety; and (d) violent events. The survey was used to describe the frequency and characteristics of WPV prevention training and resources used by HHCWs to promote personal safety since the start date of their current employment.
The WPV prevention training items included 22 questions specific to HHCWs and policies and procedures. The instructions asked participants to indicate with yes, no, or unknown if specific content was included in their WPV prevention training, policies, or procedures. Examples of questions asked were as follows: (a) Did your employer include content on WPV prevention and safety policies and procedures of the agency? (b) Does your employer provide policies for reporting a violent event while conducting a home visit? and (c) Does your employer provide procedures for seeking medical care if a violent event is experienced? The modified survey was pretested in a sample of HHCWs (n = 5) that were not included in this study. After pretesting the survey, two items were removed, because they related to worker satisfaction with the agency’s response to WPV prevention.
Data Analysis
Survey data were managed using REDCap software and analyzed using IBM SPSS Statistics (Version 24). Frequencies and percentages were computed for demographic variables. For the number of home visits conducted per shift and after dark, the mean, median, and SD are reported. Frequencies and percentages were calculated for characteristics of WPV prevention training, safety resources used, commitment to safety, and violent events.
Results
Among the participants’ email addresses, 4 (1.6%) of 254 participants email addresses replied undeliverable due to unknown emails or failed delivery after multiple attempts. The total delivered emails were 98.4% (n = 250). Two participants submitted incomplete surveys, meaning the information page was downloaded but no survey questions were completed. Therefore, these two cases were deleted during the data cleaning process. The total analytical response rate was 19.7% (n = 50). The majority of participants were between 35 and 60 years old (n = 34, 68%), persons of color (n = 26, 52%), female (n = 43, 86%), graduate degree prepared (n = 29, 58%), and APNs (n = 27, 54%). Participants reported employment status included per diem (n = 20, 40%), part-time (n = 16, 32%), or full-time (n = 14, 28%). The average number of home care visits completed per day was 3.8 (SD = 2.20). The number of home care visits conducted after dark was a median of 0.50 (interquartile range [IQR] = 0–1.25; Table 1).
Demographics of the Study Sample (n = 50)
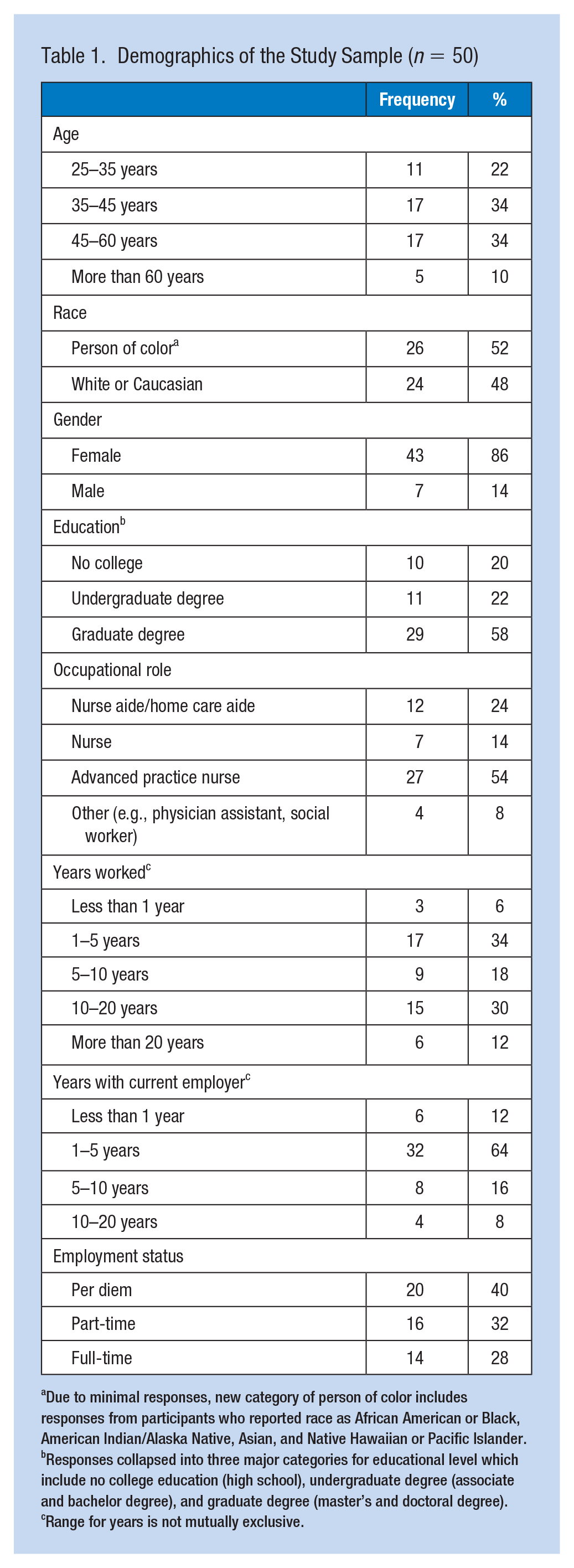
Due to minimal responses, new category of person of color includes responses from participants who reported race as African American or Black, American Indian/Alaska Native, Asian, and Native Hawaiian or Pacific Islander. bResponses collapsed into three major categories for educational level which include no college education (high school), undergraduate degree (associate and bachelor degree), and graduate degree (master’s and doctoral degree). cRange for years is not mutually exclusive.
WPV Prevention Training and Resources
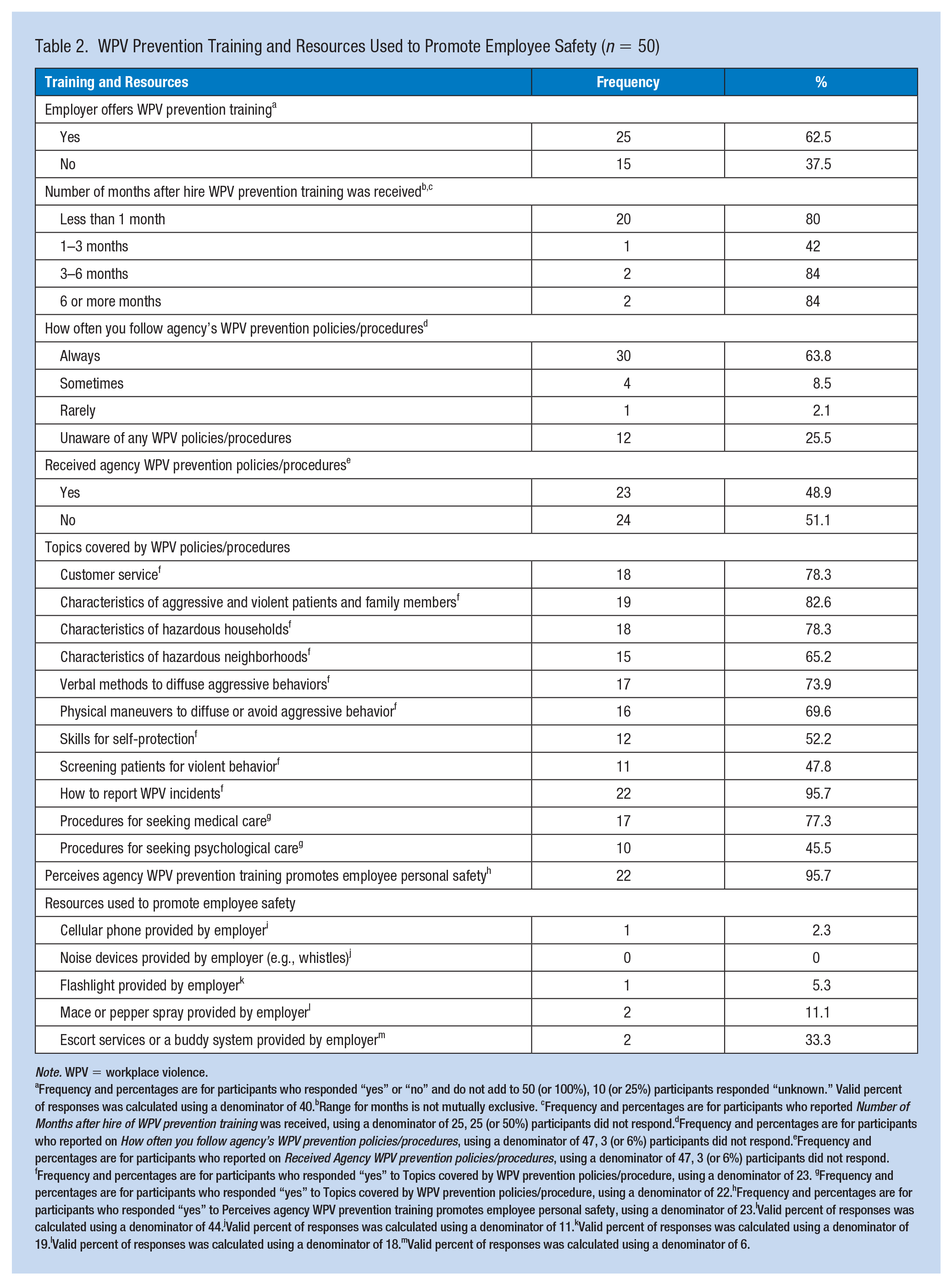
The characteristics of WPV prevention training and resources used by HHCWs to promote personal safety while at work are described in Table 2. Twenty-five participants (62.5%) indicated receiving training from their employer. Only 23 (48.9%) of 47 participants indicated receiving policies and procedures regarding WPV prevention. Yet, participants (n = 30, 63.8%) indicated they always follow their agency’s policies and procedures for WPV prevention. Of 23 participants, most indicated receiving training on reporting WPV incidents (n = 22, 95.7%), characteristics of aggressive and violent patients and family members (n = 19, 82.6%), characteristics of hazardous households (n = 18, 78.3%), and customer service (n = 18, 78.3%). Of 22 participants who reported on procedures for postvictimization care, the majority indicated receiving information on procedures for seeking medical care (n = 17, 77.3%) but fewer indicated receiving information on procedures for psychological care (n = 10, 45.5%).
WPV Prevention Training and Resources Used to Promote Employee Safety (n = 50)
Note. WPV = workplace violence.
Frequency and percentages are for participants who responded “yes” or “no” and do not add to 50 (or 100%), 10 (or 25%) participants responded “unknown.” Valid percent of responses was calculated using a denominator of 40.bRange for months is not mutually exclusive. cFrequency and percentages are for participants who reported Number of Months after hire of WPV prevention training was received, using a denominator of 25, 25 (or 50%) participants did not respond.dFrequency and percentages are for participants who reported on How often you follow agency’s WPV prevention policies/procedures, using a denominator of 47, 3 (or 6%) participants did not respond.eFrequency and percentages are for participants who reported on Received Agency WPV prevention policies/procedures, using a denominator of 47, 3 (or 6%) participants did not respond. fFrequency and percentages are for participants who responded “yes” to Topics covered by WPV prevention policies/procedure, using a denominator of 23. gFrequency and percentages are for participants who responded “yes” to Topics covered by WPV prevention policies/procedure, using a denominator of 22.hFrequency and percentages are for participants who responded “yes” to Perceives agency WPV prevention training promotes employee personal safety, using a denominator of 23.IValid percent of responses was calculated using a denominator of 44.jValid percent of responses was calculated using a denominator of 11.kValid percent of responses was calculated using a denominator of 19.lValid percent of responses was calculated using a denominator of 18.mValid percent of responses was calculated using a denominator of 6.
Sixteen of 22 (72.7%) participants reported that resources were available to promote personal safety while at work. A cellular phone was primarily provided by the participant (n = 43 of 44, 97.7%); few cellular phones (n = 1, 2.3%) were provided by the agency. Only two (33.3%) participants indicated using an escort service or buddy system provided by the employer.
Commitment to Safety and Violent Events
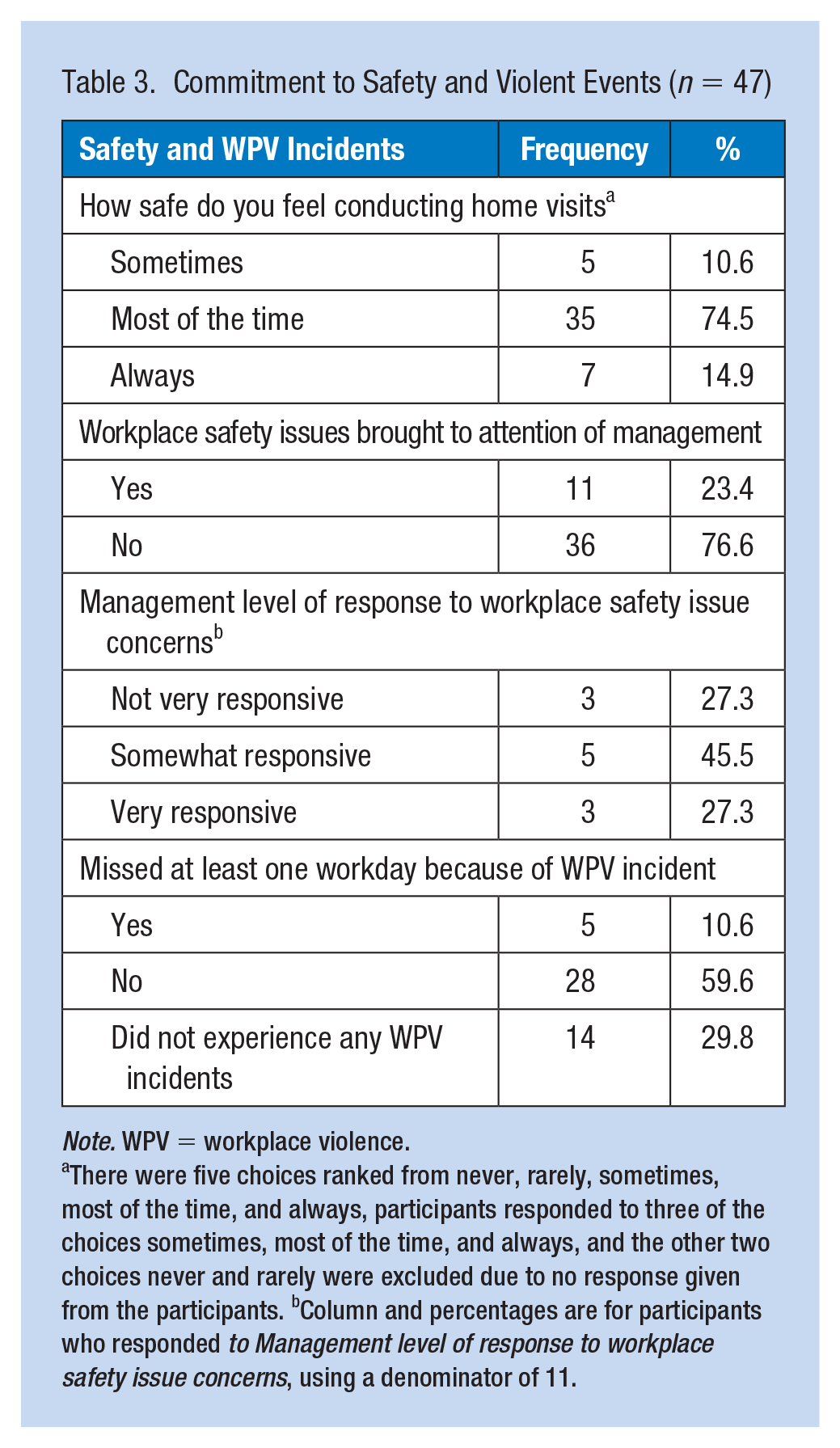
Table 3 displays findings for commitment to safety and violent events. When participants were asked if safety issues were brought to the attention of management, few participants (n = 11 of 47, 23.4%) reported yes. Of those who said yes, 3 of 11 (27.3%) indicated management was not very responsive. Five participants (10.6%) missed at least one workday due to a violent event. In general, many participants indicated they feel safe most of the time while conducting visits (n = 35 of 47, 74.5%).
Commitment to Safety and Violent Events (n = 47)
Note. WPV = workplace violence.
There were five choices ranked from never, rarely, sometimes, most of the time, and always, participants responded to three of the choices sometimes, most of the time, and always, and the other two choices never and rarely were excluded due to no response given from the participants. bColumn and percentages are for participants who responded to Management level of response to workplace safety issue concerns, using a denominator of 11.
Discussion
This is the third study to describe WPV prevention training characteristics for HHCWs. Previously, researchers Vladutiu et al. (2016) and Gross et al. (2013) found gaps in WPV prevention training and training content including limited access to training for all HHCWs, timing of when training is provided (e.g., hire, annually, and recurrent), and training content was deficient in multiple topics. Vladutiu et al. (2016) found HHCWs reported training was deficient in self-defense methods, physical maneuvers to diffuse or avoid aggressive behaviors, resources for victims, and characteristics of hazardous households and neighborhoods. Gross et al. (2013) found few agencies trained HHCWs on methods to diffuse threatening situations or protect themselves and few agencies provided WPV prevention training for HHCWs participating in patient care. In our study, HHCWs reported training was deficient in procedures for seeking psychological care, screening patients for violent behavior, skills for self-protection, physical maneuvers and verbal methods to diffuse or avoid aggressive behavior, and characteristics of hazardous neighborhoods.
Whereas most HHCWs reported receiving training content on procedures for reporting a WPV incident and customer service, in health care, customer service can be used as a strategy to both prevent and encourage WPV. Customer service can prevent WPV through listening and responding to a patient’s need. Alternatively, customer service can encourage WPV when the employer adopts a customer-service mentality that the customer (e.g., patient) is always right. A customer-service mentality often results in no or little action taken against the perpetrator (Blando et al., 2015).
It was striking that psychological care was reported by very few HHCWs (n = 10, 45.5%). Based on recent findings, HHCWs primarily suffer from nonfatal injuries caused by verbal abuse (Karlsson et al., 2019). These instances of verbal abuse result in burnout, stress, sleep problems, job turnover, and decreased job satisfaction (Karlsson et al., 2019). Therefore, training on procedures for seeking psychological care is necessary.
The majority of participants reported their employment status was per diem which may explain why half of HHCWs reported they did not receive WPV prevention training. Fazzone et al. (2000) found that HHCWs employed in a part-time or per diem status expressed it was logistically difficult to attend a training course when not compensated for their time. Therefore, a possible explanation for the lack of WPV prevention training could be that these two employers do not provide the same training to per diem employees as they provide to full-time employees. Employment status may be a possible barrier to WPV prevention training for per diem and part-time employees due to training registration fee not paid by employer or training being difficult to access (Fazzone et al., 2000). Also, HHCWs may not be able to attend training without compensation for their time while in training.
Training requirements vary depending on employer type, insurance coverage, state, and occupation of the HHCW. Per Federal legislation (42 CFR 484.36) HHCWs must have a minimum of 75 hours of training, including 16 hours of on-the-job training if they are employed by an agency receiving funding through Centers for Medicare & Medicaid Services (Code of Federal Regulations, 2021). The American Nurses Association (2015) recommends WPV prevention training at the time of hire, annually, and as needed. OSHA (2015) in their Workplace Violence Prevention Guidelines for Healthcare and Social Services recommends that new and reassigned employees receive training prior to working in assigned job duties and annual training. OSHA’s 2015 Workplace Violence Prevention Guidelines are voluntary. However, these guidelines provide a comprehensive evidenced-based framework for employers to prevent WPV. It is important for occupational health nurses (OHNs) to know and understand the OSHA guidelines and that WPV prevention programs are required in nine states. In addition, OHNs may want to lobby and join coalitions such as the American Nurses Association who support passage of the U.S. Workplace Violence Prevention for Health Care and Social Service Workers Act H. R. 1195. This Act, if passed, would charge OSHA with developing a WPV standard for health care employers (H.R. 1195, 2021).
This study demonstrated that there is an opportunity for improvement to ensure HHCWs receive WPV prevention training. As recommended by OSHA, safety committees are one tool to assess the safety concerns of HHCWs, develop interventions to promote HHCWs safety, evaluate risks in the patient’s home and community, and ensure HHCWs receive WPV prevention training on content relevant to the home care setting (Glass et al., 2017; Morris & Yaross, 2013).
Through knowledge, expertise, research, and advocacy, OHNs are equipped to identify resources and implement WPV prevention training programs (American Association of Occupational Health Nurses [AAOHN], 2020).
Limitations
This study was conducted during the COVID-19 pandemic which may have impacted the training received by HHCWs and their responses to survey questions. WPV prevention training and resources were self-reported and are subject to errors in recall. The sample size for this study was quite small, and overrepresented APNs, which limits the scope of findings and generalizability. HHCWs recruited for this study were in Southwestern Ohio and may not represent similar populations located elsewhere, further, limiting generalizability. In this study, other occupations conducting home care visits were underrepresented such as nurses, SWs, and therapists. Self-reports may introduce social desirability bias when responding to questions regarding WPV prevention training, resources, and workplace safety.
Implications for Occupational Health Practice
The current study underscores the need for resources and WPV prevention training that is specific to HHCWs and their work environment. The AAOHN (2020) has identified WPV prevention resources and implemented WPV prevention programs that include policy, advocacy, and education. The AAOHN (2020) supports a safe and healthy work environment for employees and endorses a culture of safety and a zero-tolerance policy toward WPV.
Conclusion
There is a need to strengthen access to WPV prevention training and resources specific to HHCWs. The OHN is vital to employers keeping HHCWs safe by providing a worksite free of WPV. Future research should examine the effectiveness of WPV prevention training and resources used for preventing WPV incidents in the home care setting.
Applying Research to Occupational Health Practice
Home health care workers (HHCWs) primarily work alone, sometimes in precarious environments, and may be exposed to workplace violence (WPV). WPV prevention training and resources increase HHCWs awareness of WPV and promote a safe work environment. In this study, only half of HHCWs indicated they received WPV prevention training. In addition, HHCWs reported that their employer did not provide a cell phone, an essential resource used by HHCWs to promote personal safety. Occupational health nurses (OHNs) are poised to develop a comprehensive WPV prevention program that includes WPV prevention training for HHCWs. Through knowledge and expertise, OHNs can develop, implement, and evaluate WPV prevention training content that is relevant to HHCWs and their work environment. Finally, OHNs can advocate for mandatory WPV prevention training and provision of cell phones prior to the first home visit to promote a safe work environment for HHCWs.
Footnotes
Author Contributions
T.F.S. conceptualized the research idea, selected and constructed study instruments, contributed to the study design, data collection, analysis and interpretation of data, manuscript development and preparation, and revisions for important intellectual content. T.F.S. agreed to be accountable for all aspects of the work and approved the final version of this manuscript to be published.
C.R.S. contributed throughout the project and assisted in interpretation of the data. She also revised the paper critically for important intellectual content, approved the final version to be published, and agreed to be accountable for all aspects of the work.
S.H. contributed throughout the project, assisted in data interpretation, intellectual content, and manuscript development.
K.G.D. contributed throughout the project, assisted in data interpretation, and manuscript development.
G.L.G. contributed to the study design and the analysis and interpretation of the data. He also revised the paper critically for important intellectual content, approved the final version to be published, and agreed to be accountable for all aspects of the work.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this manuscript was provided by the National Institute for Occupational Safety and Health through the targeted research training program of the University of Cincinnati Education and Research Center Grant #T42OH008432.
Human Subjects
This research study was reviewed and approved by the University of Cincinnati Institutional Review Board on April 4, 2020, using an expedited review procedure in accordance with 45 CFR 46.110(b)(1). The identification number for this research study is 2019-0550.