
Abstract
Registered nurses suffer from depression at almost twice the rate of individuals in other professions. Major depression affects both employees and organizations. Depression is linked to increases in work absenteeism, short-term disability, and decreased productivity and presenteeism. Depression experienced by registered nurses may not be fully preventable, but realizing its presence and prevalence in the workplace is of vital importance. It is essential that we have a healthy, vibrant, and present registered nurse workforce to ensure that quality patient outcomes are achieved. This review of 36 articles assesses the current state of the science related to depression in registered nurses so that occupational health nurses can create pathways and work environments for better mental health for registered nurses.
Keywords
More than 4 million registered nurses are employed in the United States, with females representing 90% of the nursing workforce (Budden, Zhong, Moulton, & Cimiotti, 2013). Nursing is a stressful, demanding, and taxing profession; job stress is linked to higher rates of depression (Centers for Disease Control and Prevention [CDC], National Institute for Occupational Safety and Health, 2013). Nurses experience depressive symptoms at a rate twice as high as individuals in other professions (S. Letvak, Ruhm, & McCoy, 2012). In this article, the authors assess the current state of the science related to depression in registered nurses so that occupational health nurses can identify personal and organizational factors that influence depressive symptoms and create pathways for better mental health for registered nurses. The correlates and predictors of depression in registered nurses discovered in the literature are summarized. Last, the authors identify gaps in the literature that may guide further research.
Background
Depression is estimated to affect more than 350 million individuals (World Health Organization [WHO], 2012). Globally, an estimated one in 20 individuals reports an episode of depression in the previous year (WHO, 2012). In the United States, more than 16 million adults have had at least one major depressive episode in the last year (National Alliance for Mental Illness [NAMI], 2015; National Institute of Mental Health [NIMH], 2014). The CDC estimate that one in 10 adults in the United States will at some point in their lifetimes report suffering from depression (CDC, 2012).
Major depressive disorder, frequently referred to as depression, is the most common mental disorder in the United States (NAMI, 2008). Depression and its associated symptoms present in each individual differently. Generally, depression is characterized by persistent sad, anxious, or empty feelings; feelings of hopelessness or pessimism; feelings of guilt, worthlessness, or helplessness; irritability; restlessness; and loss of interest in activities or hobbies once pleasurable (NAMI, 2015; NIMH, 2014). Additional symptoms include fatigue and loss of energy; difficulty in concentrating, remembering details, and making decisions; insomnia, early-morning wakefulness, or excessive sleeping; overeating, or appetite loss; thoughts of suicide and suicide attempts; aches or pains; headaches; cramps; or digestive problems that do not ease even with treatment (NAMI, 2015; NIMH, 2014). These problems can become chronic or recurrent and lead to substantial functional impairments.
Major depression affects employee performance as well as organizational productivity (American Psychiatric Foundation [APF], Partnership for Workplace Mental Health, 2015; Langlieb & DePaulo, 2008; S. A. Letvak, Ruhm, & Gupta, 2012). Depression is linked to increases in work absenteeism, short-term disability, and decreased productivity and presenteeism (CDC, 2012). Depressed employees may have impaired judgment, and lapses of judgment in the workplace may produce serious occupational injuries (Langlieb & DePaulo, 2008). Depression is estimated to cause 200 million lost workdays each year at a cost to employers of US$17 billion to US$44 billion (APF, Partnership for Workplace Mental Health, 2015). Depression accounts for as much health care and disability costs as chronic diseases such as hypertension, diabetes, musculoskeletal disorders, and heart disease (APF, Partnership for Workplace Mental Health, 2015). Nurse-reported productivity loss due to depression is estimated to be US$14,339 per nurse and US$876.9 million per state. These costs equate to a national productivity loss of US$22.7 billion per year (S. A. Letvak et al., 2012).
However, it is presenteeism that may have the most impact on worker performance (S. A. Letvak et al., 2012; J. Wang, Schmitz, Smailes, Sareen, & Patten, 2010). Presenteeism is the productivity loss that occurs when workers are present at work, but are not functioning at peak performance because of health problems (S. Letvak, 2013). Depressed workers continue to work, but underperform due to their symptoms (Putnam & McKibbin, 2004; J. Wang et al., 2010). Registered nurses who report presenteeism are more likely to report more medication errors, patient falls, and overall poorer quality of care received by patients. (S. A. Letvak et al., 2012).
Method
A review of the literature was conducted using the electronic databases CINAHL and PubMed. In addition, the search engine Google Scholar was used to detect other relevant literature sources. Please refer to Figure 1 for the diagram of the review process. The original search was limited to 10 years, articles written in English, and outcome variables related to depression. To refine this topic for a review of the literature, a Population, Intervention, Comparison, and Outcome (PICO) question was generated. The PICO question for this research included the terms registered nurses, predictors, and depression. In CINAHL, the terms depression and registered nurses were explored using the “major exact subject heading” field generating 15 articles, of which eight were further examined.
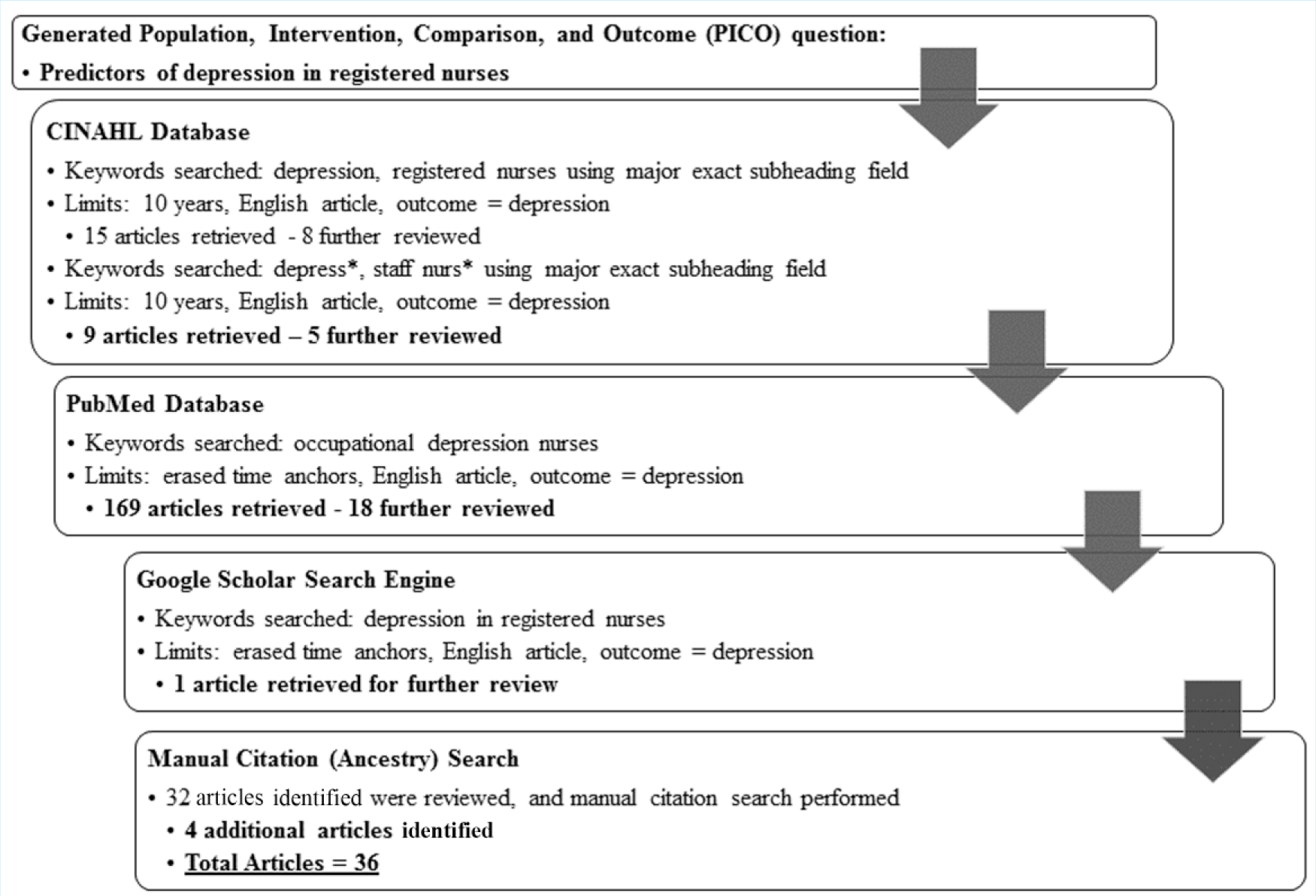
Diagram of review process.
To capture additional articles, a search of the terms depress* and staff nurs* using the “major exact subject heading” field was completed, yielding another nine articles, five of which were relevant and marked for additional examination. Because few relevant articles were discovered, the researchers eliminated the 10-year time anchor to capture sentinel research articles. A subsequent search of PubMed, using the search terms “occupational depression nurses,” yielded 169 articles; 18 were flagged for further review.
At this step, the majority of articles were rejected because the articles did not focus on depression in registered nurses, the focus of this review. The abstracts of remaining articles were reviewed to ascertain that the remaining research studies matched the purpose of this review. At this point, the search engine Google Scholar with keywords “depression in registered nurses” was explored with no time limitations. This search uncovered a sentinel article from 1990 that had not been previously identified. Next, the authors conducted a manual citation search using the identified articles; this process yielded five additional research articles.
After adjusting the search criteria to capture the most significant research articles, 36 articles were retained for this review of the literature (See Figure 1). Because of the limited number of articles retrieved from the chosen databases, the researchers did not evaluate the studies for methodological and theoretical rigor. The remaining 18 studies were then reviewed, analyzed, and organized around the outcome variable of depression. Results of the review were categorized into themes found in the literature including stages of depression research, geographical features, observations of depression in registered nurses, depression correlates, depressive symptomatology, and personal and workplace predictors of depression. Table 1 presents a summary of 36 studies reported between 1983 and 2015 that met the inclusion criteria. The information identified in the table includes the author(s), year, location, purpose/research questions, design, sample size, depression measurements, other measurements, and key findings.
Comprehensive Table of Literature Review Articles

Note. GHQ-30 = General Health Questionnaire; JDI = Job Descriptive Index; ICU = intensive care unit; IM = internal medicine; PSR = Provision of Social Relations; BDI-R = Beck Depression Inventory–Revised; CES-D = Center for Epidemiologic Studies Depression Scale; ER = emergency room; HADS = Hospital Anxiety and Depression Scale; PSQI = Pittsburgh Sleep Quality Index; KSQ = Karolinska Sleep Questionnaire; SHC = Subjective Health Complaints Inventory; GSES = General Self-Efficacy Scale; PSS-10 = Perceived Stress Scale–10 items; PANSI-PI = Positive and Negative Suicide Ideation [Positive Ideation]; SCS = Self Control Schedule; BIS = Bergen Insomnia Scale; AUDIT-C = Alcohol Use Disorders Identification Test; JCQ = Job Content Questionnaire; ERI = effort reward imbalance; BDI = Beck Depression Inventory; MBI = Maslach Burnout Inventory; DASS = Depression Anxiety Stress Scale; HTEC = Hospital Trauma Exposure Checklist; PHQ-9 = Patient Health Questionnaire–9; TDS = total depression score; BMI = body mass index; ERI = Effort Reward Imbalance; JCQ = Job Content Questionnaire; WCCL = Ways of Coping Checklist; LOT-R = Life Orientation Test–Revised; JAWS = Job-Related Affective Well-being Scale; CIDI = Composite International Diagnostic Interview; SSICFS = Standard Shiftwork Index Chronic Fatigue Scale; BAI = Beck Anxiety Inventory; CSEI = Coopersmith Self-Esteem Inventory; STAI = Strait-Trait Anxiety Inventory; ASES = Adult Self Expression Scale; DIS = Diagnostic Interview Schedule; SCL-90R = Symptom Checklist–90 Revised; TDQ = Taiwanese Depression Questionnaire; OSI-R = Occupational Stress Inventory revised edition; ELS = Emotional Labor Scales; NIOSH = The National Institute for Occupational Safety and Health; GJSC = Generic Job Stress Questionnaire; HPI = Health Practice Index.
Findings
Of the 36 studies identified for this review, 10 used a descriptive design, 11 used a correlational design, and 15 used a mixed descriptive/correlational design. Sample sizes ranged from 29 to 3,474 nurses. Of the 36 studies, seven were conducted in the United States with the remaining 29 conducted internationally. The time span for the studies ranged from 1983 to 2014. Table 1 provides a comprehensive examination of each of the 36 studies reviewed.
Stages of Depression Research
The investigation of depression in registered nurses spans several decades. The landmark article on the subject was written by Italian researchers in 1983 and examined depression and anxiety in psychiatric nurses (De Leo, Magni, Vallerini, & Dal Palu, 1983). Between 1985 and 1993, researchers published four articles investigating depression in registered nurses. These authors mainly focused on predictors and correlates of depression in registered nurses. Between 1998 and 2003, researchers began to focus on personal factors associated with depression such as secondary trauma, demographic characteristics, and personal protective factors. During this time frame, investigators published seven articles that contributed to understanding how depression affects registered nurses. Since 2004, a resurgence of articles examined the prevalence and predictors of depression; the emphasis in these articles was on personal and occupational stress experienced by registered nurses. Between 2004 and 2015, researchers published 25 articles exploring the relationship of these phenomena; research in the last decade accounted for close to 70% of current knowledge on the topic. Table 1 provides a chronological summation of research studies about depression in registered nurses.
Geographical Scope of Depression Research
Examining and predicting depression in registered nurses are domestic and international imperatives. Research on the topic in the United States has been published in New York, North Carolina, New Jersey, Tennessee, California, and most recently in Kentucky (Glass, McKnight, & Valdimarsdottir, 1993; S. Letvak et al., 2012; Ruggiero, 2003; Skipper, Jung, & Coffey, 1990; van Servellen, Soccorso, Palermo, & Faude, 1985; Welsh, 2009). However, the majority of research investigating depression in registered nurses has been conducted outside the United States (i.e., Australia, Canada, China, England, Japan, Norway, Taiwan, and the Caribbean countries of St. Vincent and Trinidad and Tobago). Table 1 provides a comprehensive list of international depression research and corresponding countries.
Observations of Depression in Registered Nurses
The research revealed a variety of factors that predicted depression in registered nurses. The highest rates of depression were among young, female registered nurses (Arafa, Nazel, Ibrahim, & Attia, 2003; Ardekani, Kakooei, Ayattollahi, Choobineh, & Seraji, 2008; Ohler, Kerr, & Forbes, 2010; van Servellen et al., 1985; Yoon & Kim, 2013; Yoshizawa et al., 2016). In addition, depression was cited as more frequent in single and divorced nurses versus married nurses (Ardekani et al., 2008; Chang, Wang, Li, & Liu, 2011; S. M. Wang et al., 2015; Yoon & Kim, 2013). Nurses working in intensive care units and psychiatric units reported higher levels of depression (Arafa et al., 2003; Bjorvatn et al., 2012; Chiang & Chang, 2012; De Leo et al., 1983; Gong et al., 2014; Kawano, 2008; S. M. Wang et al., 2015) than nurses working on other types of units. Registered nurses reporting higher levels of workplace violence or traumatic events also reported higher levels of depression (Gong et al., 2014; Lam, Ross, Cass, Quine, & Lazarus, 1999; Yoshizawa et al., 2016). In addition, nurses with positive evaluations and expectations of themselves and others reported lower depression levels (Chang et al., 2011).
Depression Correlates
Depression was positively correlated with female gender, marital status, and length of employment (Baba, Galperin, & Lituchy, 1999; Chang et al., 2011; Gao et al., 2012; S. M. Wang et al., 2015). Also, as age increased, the risk for depression decreased (Bjorvatn et al., 2012; Skinner & Scott, 1993). Depression in registered nurses was also correlated with other mood disorders like anxiety, and somatic symptoms such as fatigue, pain, and trouble sleeping (Morrissy, Boman, & Mergler, 2013; Welsh, 2009). Depression showed significant positive associations with role overload, role conflict, stress, burnout, absenteeism, intention to leave, and turnover (Baba et al., 1999; Chang et al., 2011; Glass et al., 1993; Hegney et al., 2014; Kawano, 2008; Lin, Probst, & Hsu, 2010; Wu, Ge, Sun, Wang, & Wang, 2011; Yoshizawa et al., 2016). Overcommitment and job strain were also significant correlates of depression (Mark & Smith, 2012). Shift work or working alternating shifts was positively associated with depression (Arafa et al., 2003; Eldevik, Flo, Moen, Pallesen, & Bjorvatn, 2013; Flo et al., 2012; Flo, Pallesen, Moen, Waage, & Bjorvatn, 2014; Ruggiero, 2003). Higher job satisfaction, self-efficacy, optimism, learned resourcefulness, and positive ideation were negative correlates and significant buffers against depression (Chang et al., 2011; Chung et al., 2012; Gao et al., 2012; Morrissy et al., 2013; S. M. Wang et al., 2015).
Depressive symptomatology
The most frequently reported depressive symptoms by registered nurses included continual fatigue, trouble sleeping, thoughts about death, depressed mood (2 weeks or more), and trouble concentrating (van Servellen et al., 1985; Welsh, 2009). In addition to these depressive symptoms and somatic complaints, depression in some instances was accompanied by anxiety or anxious feelings (Ardekani et al., 2008; Bjorvatn et al., 2012; De Leo et al., 1983; Hegney et al., 2014; Morrissy et al., 2013; Oyane, Pallesen, Moen, Akerstedt, & Bjorvatn, 2013; Ruggiero, 2003). Depression was often accompanied by report of at least one chronic disease (Gao et al., 2012; Ohler et al., 2010).
Personal Characteristics
The literature consistently cites age as a main contributor to depression in registered nurses. Unlike the general population, as nurses age, they are less likely to suffer from depression and depressive symptomatology (Arafa et al., 2003; Ohler et al., 2010; Yoon & Kim, 2013). Ohler and colleagues (2010) found in their study of 9,322 registered nurses that younger nurses had nearly double the odds of depression. This finding is supported by other research that reported increasing age was a protective factor against depression (Skinner & Scott, 1993; Yoshizawa et al., 2016). In addition, marital status was also a strong predictor of depression in registered nurses with the research showing that single and divorced nurses had the highest prevalence of depressive factors (Ardekani et al., 2008; S. M. Wang et al., 2015; Yoon & Kim, 2013).
Work Characteristics
Acute hospital-based registered nurses reported higher levels of depression; the level of clinical unit acuity was directly related to this finding with psychiatric, intensive care and surgical units’ nurses reporting the highest levels of depression or depressive symptomatology (Arafa et al., 2003; Bjorvatn et al., 2012; Chiang & Chang, 2012; De Leo et al., 1983). Job strain, role overload, role insufficiency, and diminishing role boundaries predicted depressive symptoms in a sample of 1,986 Chinese nurses (Wu et al., 2011). Furthermore, according to Ohler and colleagues (2010), nurses experiencing job strain were 80% more likely to suffer from depression. Other factors such as lack of supervisor support, job insecurity, lack of reward, and job-related stress are strongly correlated with depressive symptoms (Yoon & Kim, 2013). It is quite plausible that younger nurses have higher rates of depression due to the work environment. Work satisfaction, shift work, fatigue, and fewer years of work experience have been found to be strong correlates of psychological health (Arafa et al., 2003; Flo et al., 2012; Flo et al., 2014).
Discussion
This review explored the prevalence and predictors of depression in registered nurses from 36 published studies. Overall, evidence from this review confirmed a troubling prevalence of depressive symptoms in this population. Figure 2 provides a brief summary of the results.
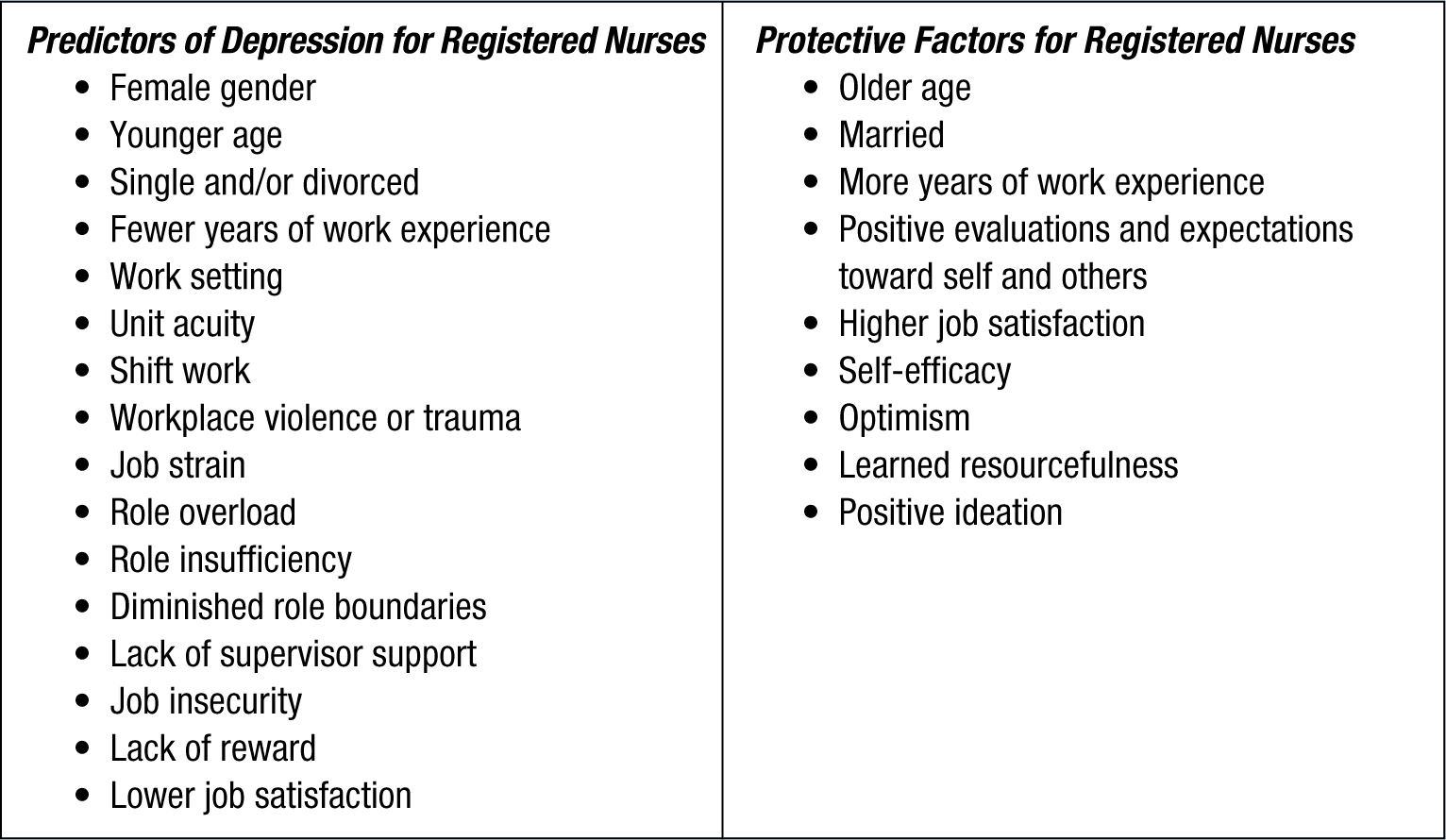
Depression in registered nurses: Brief summary of results.
Currently, insufficient rigorous research studies using randomized samples or longitudinal analyses have examined this issue. Research is scattered globally with limited study designs and samples. Additional research is needed that will further guide and define depression in registered nurses.
Although nursing is predominantly a female profession, the review revealed that when gender was included, female registered nurses experienced higher rates of depression. In the U.S. population, women experience depression at a rate twice that of men with an estimated 7 million women diagnosed with major depression each year (NAMI, 2008). This excessive rate is often attributed to additional stressors and challenges faced by women at home and work (Bronder, Speight, Witherspoon, & Thomas, 2014; NIMH, 2014; Williams et al., 2007). This review of the literature noted mixed results for the role of social and family support and depression among nurses. More research should be conducted to provide foundational knowledge about the complexities of interactions between work, and family and community roles among registered nurses, particularly among female nurses who have increased risk for depression.
In addition to gender, the review revealed that younger nurses had higher rates of depression than older nurses. This finding is inconsistent with general literature on the topic that suggests that as one ages, the risk for depression increases (CDC, 2012). In the general population, older individuals are at risk for persistent and recurring (chronic) depression, which may exacerbate health conditions or cause new issues (American Psychological Association, 2015). Findings of this study may be partially explained by the healthy worker survivor effect which describes a continuing selection process such that those who remain employed tend to be healthier than those who leave employment (Arrighi & Hertz-Picciotto, 1994). Due to the possibility of the healthy worker effect in registered nurses, some caution regarding this finding and a need for further research should be understood.
In addition to age, it is worth noting that length of employment is also strongly correlated with depression. Therefore, specific measures should be used to ensure that early psychosocial interventions for these nurses are introduced upon initial hire and not only when nurses first begin to exhibit symptoms of depression or concurrent syndromes like anxiety or fatigue. Peer support systems may assist new nurses as they enter the workforce (Harrison-White & Simons, 2013). The complexity of young registered nurses’ work may include additional pressures for advanced education, new family roles, and launching their careers which may combine to elevate the risk of depression (Charnley, 1999; Harrison-White & Simons, 2013).
The CDC’s (2015) Total Worker Health Model may be used by occupational health nurses to more fully assess the risk of depression among vulnerable employees. A Total Worker Health approach is defined as “policies, programs, and practices that integrate protection from work-related safety and health hazards with promotion of injury and illness prevention efforts to advance worker well-being” (CDC, 2015, para. 1).
Registered nurses at risk for depression should be monitored for somatic symptoms and chronic illnesses. Fatigue can be a somatic complaint related to depression; however, nurse fatigue can also result from shift work disorder (Flo et al., 2012; S. M. Wang et al., 2015). Much of the depression risk in younger nurses may be attributed to these nurses being immediately assigned to non-traditional shifts when they begin practice. Although younger nurses experience depression at higher rates than older nurses, older nurses should still be monitored for chronic illnesses that may increase their risk for depression (Gao et al., 2012; Ohler et al., 2010). The average age of the nursing workforce is steadily increasing; the average age of registered nurses working in the United States is 50; more than 53% of registered nurses work past the age of 50. With increased age comes increased risk for chronic illness. Older nurses tend to have greater body mass indexes (BMIs), higher pain scores, and less health-related productivity than younger nurses (S. Letvak, Ruhm, & Gupta, 2013).
In this review, studies could be better characterized as a patchwork quilt than a well-established, consistent examination of depression in registered nurses. Across studies, the research questions and specific aims were broad, and no gold standard depression instrument was used; instead, researchers used a variety of instruments. One of the ways to combat this problem is to have a clear conceptual picture and theoretical framework to guide research and practice. Based on the psychosocial risk management literature, this conceptual framework should include components that pose the greatest risk to worker health including personal characteristics, job content, workload and work pace, control, environment and equipment, organizational culture and function, interpersonal relationships at work, role in organization, and home and work interface (WHO, 2008).
Implications
These findings have far reaching implications for occupational health nurses. Registered nurses must be healthy and focused to function at optimal capacity. One practical starting point to address depression in registered nurses is to examine organizational structure and support. An essential role of occupational health nurses is to ensure that program policies support, encourage, emphasize, and prioritize worker health (Campbell & Hanna, 2014). As the review indicated, work environment is a major predictor of depression in registered nurses. Improving work environments for registered nurses might, in turn, improve their psychological health and decrease their risk for depression. As such, it is critical that occupational health nurses create workplaces that value and support health care workers (Campbell & Hanna, 2014).
From an occupational health and safety perspective, it is critical that occupational health nurses are advocates for health promotion and management. A well-planned needs assessment that measures workforce health risks, identified needs, employee productivity, and program costs and benefits may assist in the development of targeted interventions (Campbell & Hanna, 2014). Occupational health nurses have a unique ability as front-line providers to collect data, analyze trends, and report research findings on depression in registered nurses. Occupational health nurses can provide case management, clinical support, education, advocacy, and support for registered nurses experiencing depression (Campbell & Hanna, 2014).
In addition to clinical and management interventions, collaboration with primary care providers and mental health professionals to screen, diagnose, and treat depression in registered nurses is imperative. To achieve optimal health in registered nurses, it is crucial that occupational health nurses properly identify depression and additional risk factors for this disease. Because depression is complex and often associated with other chronic conditions, it may also be advantageous for occupational health nurses to form interdisciplinary health care management teams to strengthen early identification and treatment. It is vital for occupational health nurses to understand the implications behind these findings and create pathways to better health and workplace wellness.
Limitations
Currently, no accepted theoretical framework addresses personal and workplace concepts impacting depression in registered nurses. A comprehensive theoretical model is needed to fully conceptualize many of the variables identified in this review of the literature and understand their impact on depression. The bulk of the articles examined in this review were descriptive or correlational in design and used cross-sectional data from convenience samples. None of these design methods can definitively determine causality. Future research should incorporate more rigorous designs including experimental and longitudinal studies.
In addition to study design, the psychometric measures and instrumentation should be consistent across studies. This review identified a multitude of instruments that were used to assess the concept of depression including the Beck Depression Inventory I and II, Center for Epidemiologic Studies Depression Scale, Depression and Anxiety Stress Scale, General Health Questionnaire–28, Hospital and Anxiety Depression Scale, Patient Health Questionnaire–9, and Zung Self-Rating Depression Scale. The Beck Depression Inventory I and II and the Center for Epidemiologic Studies Depression Scale were used in more than half of the research articles. However, a standard measurement for depression across research studies is a needed step in establishing consistency across future research studies.
Finally, although the international burden of depression has been explored, the prevalence and correlates of depression in America’s two largest and fastest growing minority populations is not at the forefront of this literature. It is well established that individuals of diverse racial and ethnic backgrounds experience disproportionately higher rates of selected diseases and health conditions than the general population (American Public Health Association [APHA], 2014). Researchers have found that even though Black Americans have a lower lifetime risk for depression than White Americans, this population is more likely to be persistently ill once diagnosed with depression (Williams et al., 2007); chronic depression is substantially higher in Black Americans. Most recent chronic depression rates have been reported as 57% for Black Americans and 38% for White Americans (Kim, 2014). In Latinos, being U.S. born, or second or higher generation immigrant, was associated with higher levels of depression (Wassertheil-Smoller et al., 2014). In addition, Puerto Ricans experience higher prevalence of depression than Mexican Americans, women higher than men, those with less than a high school education higher than those with a high school diploma or higher, and those aged 45 to 64 years than those older or younger (Wassertheil-Smoller et al., 2014). With the increasing diversity of the U.S. population and the emphasis on cultural concordance for health care providers, understanding the impact of depression on minority workers is a crucial step in addressing depression in ethnic minority registered nurses. However, to date, no researchers have studied depression in ethnic minority registered nurses working in the United States. Thus, additional research investigating the mental health of nurses from racial and gender minority groups is needed.
Conclusion
Depression experienced by registered nurses may not be fully preventable, but realizing its presence and prevalence in the workplace is of vital importance. It is essential that the United States has a healthy, vibrant, and present registered nurse workforce to ensure that quality patient outcomes are achieved. Occupational health nurses are essential participants in improving the mental health of registered nurses. To fully comprehend the magnitude and impact of depression among registered nurses, occupational health nurses working in all settings must be cognizant of the role they play in assessing, recognizing, referring, collaborating, researching, and managing the care of this unique occupational group.
Footnotes
Acknowledgements
The authors acknowledge Bev Hilton, Medical Librarian-Liaison to the University of Kentucky College of Nursing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partially supported through the Central Appalachian Regional Education Research Center Occupational and Environmental Health Nursing PhD Training Program #1T42OH010278. Contents are the responsibility of the authors and do not reflect endorsement of the funding agency.
Author Biographies
Arica A. Brandford, Jonas Scholar, is a PhD Candidate at the University of Kentucky College of Nursing and trainee in the Central Appalachian Education and Research Center. Her research interests include diverse populations, health disparities, and workforce health.
Deborah B. Reed, is distinguished service professor and Good Samaritan Endowed Chair at the University of Kentucky College of Nursing. She has conducted occupational health research for 24 years across the United States.