
Abstract
The primary cause of death for men and women in the United States is heart disease. Obesity and diabetes are major contributors to heart disease, and the risk is worsened in the presence of stress. It is clinically useful to identify predictors of obesity and prediabetes in a working population. The purpose of this current cross-sectional, correlational study was to examine relationships among obesity, prediabetes, and perceived stress in municipal workers using a subset of worksite wellness program data from employees screened in 2010 and 2011. Multiple regression models indicated that age, gender, race, HA1c, shift schedule, physical activity, and occupation were significant predictors of obesity in municipal workers (p < .01). Prediabetes in municipal workers was predicted by age, Black race, and body mass index (BMI; p < .01). Perceived stress was not a significant predictor of obesity or prediabetes in municipal workers. Overall, the findings of this study provide guidance to occupational health nurses when evaluating individuals in an occupational health setting. Further research is needed to examine relationships among the variables and validate the models.
Keywords
Obesity and diabetes are major contributors to heart disease, which is the primary cause of death in the United States for men and women (Centers for Disease Control and Prevention [CDC], 2015; LeBlanc, O’Connor, Whitlock, Patnode, & Kapka, 2011). Obesity affects all segments of the population in the United States regardless of gender, race, or socioeconomic status and is a known risk factor for chronic diseases such as diabetes, hypertension, and heart disease (Flegal, Carroll, Ogden, & Curtin, 2010; U.S. Department of Health and Human Services, 2010). The number of U.S. adults with excess weight surpassed the number of those who are underweight regardless of socioeconomic status, possibly related to the urbanization of rural communities, sedentary lifestyles, and lack of physical activity (World Health Organization, 2012).
Based on fasting glucose or glycosylated hemoglobin (HA1c) levels, 35% of U.S. adults aged 20 years or older have prediabetes, which is associated with US$25 billion in higher health care costs annually (CDC, 2014; Dall et al., 2010). Individuals diagnosed with prediabetes are at increased risk for developing diabetes. Compounding the problem of chronic health conditions is the presence of stress, which increases the risk for obesity, diabetes, and heart disease (Azagba & Sharaf, 2011).
The aging of the workforce and delays in retirement have contributed to employees’ health care burden and the rise in chronic health care costs for conditions such as diabetes and obesity (Lee et al., 2012). The proportion of workers aged 55 years and older is projected to increase from 18.1% of the labor force in 2008 to 23.9% in 2018 (Bureau of Labor and Statistics, 2011). Seventy-eight percent of all health care spending in the United States and seven of 10 deaths per year are attributable to chronic illnesses, many of which are preventable (CDC, 2012). These chronic health conditions result in an enormous burden for individuals and their employers, especially considering that employers are the primary payers of health insurance premiums for American workers (United Health Foundation & American Public Health Association, 2014). Employer profits can be reduced by as much as 10% when health care is needed to treat stress-induced chronic illnesses (American Psychological Association, 2010; Azagba & Sharaf, 2011).
Given the dramatic increase in the prevalence of obesity, prediabetes, and stress in the last three decades, a better understanding about the influence of stress and personal factors on obesity and prediabetes is warranted. The goal of this study was to examine relationships among obesity, prediabetes, and perceived stress in municipal workers. An exploration of the nature of the relationships among the variables was based on a combined expanded biobehavioral interaction (EBI) model and Karasek and Theorell’s (1990) demand control model related to occupational stress. The EBI model explores links among psychosocial, behavioral, individual, and biological factors and health outcomes, and the Karasek and Theorell model focused on individuals at the worksite and the psychosocial characteristics of the work environment (Fernandez, Su, Winters, & Lang, 2010; Kang, Rice, Park, Turner-Hanson, & Downs, 2010; Karasek & Theorell, 1990).
This study posed the following research questions:
Method
A cross-sectional, correlational design was used to examine relationships among obesity, prediabetes, and perceived stress in municipal workers employed in a large southeastern U.S. city. These municipal workers participated in health risk appraisal screening as part of a worksite wellness program. The municipality employs more than 5,000 workers representing all municipal departments. The three largest departments (i.e., Police, Fire, and Public Works) account for approximately two thirds of all city employees. Hemoglobin A1c measurements are routinely measured for employees aged 40 and older. This study examined a subset of worksite wellness program data from employees screened in 2010 and 2011. A total of 3,501 municipal employees were included in this study, and HA1c was measured for 1,963 participants.
After the study was approved by the institutional review board, a limited data set was provided for this research from the original database and coded to maintain anonymity of the participants. Height, weight, BMI, waist circumference, and other physiological measurements, including glycosylated hemoglobin, were collected.
Instruments
Health risk appraisal instruments were used to collect data (i.e., both self-report and staff-measured biophysical data such as height, weight, BMI, waist circumference, and HA1c) for this study. The full self-report health risk appraisal consisted of 84 questions regarding demographic data, health habits, and personal and family health history. Only measurements pertaining to the present study were analyzed.
In this study, obesity was defined as a BMI of 30 kg/m2 or greater (World Health Organization, 2011); prediabetes was defined as the presence of elevated blood glucose reported as a glycosylated hemoglobin (HA1c) level between 5.7% and 6.4% (CDC, 2011); perceived stress was defined as self-reported level of stress in the past 2 weeks (i.e., “a lot,” “moderate amount,” “relatively little,” and “almost none”); level of activity defined as self-reported activity level (i.e., “at least 3 times a week,” “1-2 times a week,” and “less than 1 time a week”); and waist circumference was defined as high risk if greater than 40 inches in men and greater than 35 inches in women (CDC, 2012). Other variables included age (birth date), gender (male or female), race (White, Native American, Asian, Black, Pacific Islander, Other, or not known), education (grade school or less, some high school, high school graduate, some college, college graduate, and post graduate or professional degree), occupation (Police, Fire, Public Works, and City Hall), and shift schedule (7:00 a.m.-3:00 p.m., 8:00 a.m.-5:00 p.m., 3:00 p.m.-11:00 p.m., 11:00 p.m.-7:00 a.m., Shift A Fire, Shift B Fire, Shift C Fire, and other) were self-reported on the health risk appraisal instrument. The term public safety workers referred to police officers and firefighters.
Reliability of data collected by wellness program personnel was ensured by using a standardized procedure manual, data collection and entry procedures, and standardized training of wellness program personnel. Measures for BMI, waist circumference, and HA1c were based on guidelines and procedures recognized as valid (Flegal, Carroll, Kit, & Ogden, 2012; National Institutes of Health [NIH], National Heart, Lung, and Blood Institute, 2000)
Data Analysis
The secondary data set in this study was analyzed using the Statistical Package for the Social Sciences (SPSS) software program Version 21 with the significance criterion set at p < .05 and the power set at the conventional standard of 0.80 (Polit & Beck, 2012). Frequencies, means, percentages, and standard deviations were calculated to describe the sample and answer Research Question 1. For Research Questions 2 and 3, relationships among variables were tested with chi-square and Spearman’s rho, depending on the level of variable measurement. Logistic regression was used to answer Research Question 4, which examined the influence of the multiple independent variables (i.e., perceived stress, age, gender, race, HA1c, shift schedule, occupation) on the dependent variables (i.e., prediabetes and obesity) as defined by BMI and waist circumference. When the level of variable measurement was ordinal or nominal, dummy coding was used in the preparation of the data. Collinearity diagnostics did not reveal any issues with multicollinearity.
Results
As shown in Table 1, of the 3,501 municipal employees included in this study, 72% were male, the most common age group was between 40 and 49 years, 66.9% were Black, and 29.8% White. Almost one fifth (21.3%) of the sample had completed high school and nearly double that number had completed some college. More than one third (35.3%) of the employees were college graduates.
Characteristics of Sample (N = 3,501)

Note. BMI = body mass index; HA1c = Glycosylated Hemoglobin.
M = 43.77; SD = 10.75
Police officers were the largest group (30%) of municipal workers in this sample. One fourth (24.9%) of the sample were employed in Public Works, another fourth (24%) were employed at City Hall, and 20.3% were firefighters. Most employees (47%) worked during the hours of 7:00 a.m. to 5:00 p.m., but shifts were worked throughout the 24-hour period. The majority of the 3,501 participants reported a moderate amount of stress (41%) or a lot of stress (11.9%). Almost 48% of the participants reported physical activity at least 3 times per week.
The obesity and prediabetes data indicated that the majority of the 3,501 municipal employees were obese (n = 1,908; 55.8%) using BMI measurements (Table 1). The lowest BMI measured was 16.62 and the highest was 67.03. The percentage of municipal workers who were of normal weight or underweight was particularly low at 12% and 0.2%, respectively; the rest of the participants were classified as overweight or obese. When obesity was defined by waist circumference, 53% of the sample was obese; the mean waist circumference was nearly 40 inches for both males and females. Hemoglobin A1c was measured in 1,963 participants. Of this number, 1,001 (51%) were identified as prediabetic, and 309 participants (15.7%) were identified as diabetic. The highest HA1c measured was 14.4.
A moderate amount of stress was the most frequently reported level of stress across all occupations. Among the different municipal occupations, police reported the most stress in three of four stress categories. Public Works employees were most likely to report almost no stress. In this study, no significant relationship was found between perceived stress and obesity or between perceived stress and the presence of prediabetes.
When the differences in obesity by shift work, education, and gender were evaluated, all fire shifts had the lowest BMI compared with the rest of municipal workers’ shifts. The mean BMI (30.34) by fire shifts was lower than the mean BMI (31.63) of the entire sample. The highest BMI (32.84) recorded was for the 11:00 p.m. to 7:00 a.m. shift. The municipal workers with some college education had the highest BMI (31.98), and those workers with high school or less had the lowest BMI (30.36). Female municipal workers had a mean BMI of 32.75, and males had a mean BMI of 31.21.
Age, gender, race, HA1c, shift schedule, physical activity, and occupation were significant predictors of obesity (BMI > 30) for these municipal workers. These predictors contributed to a statistically significant model predicting obesity in the current sample of municipal workers. Shift schedule was the weakest predictor, but when it was omitted from the model, no improvement was seen overall and so it was retained in the model. This model correctly predicted 96.1% of those workers who were obese. However, the model predicted only 12.4% of workers who were not obese (Table 2).
Binary Logistic Regression Analysis Predicting Obesity (BMI) of Municipal Workers (n = 1,865)
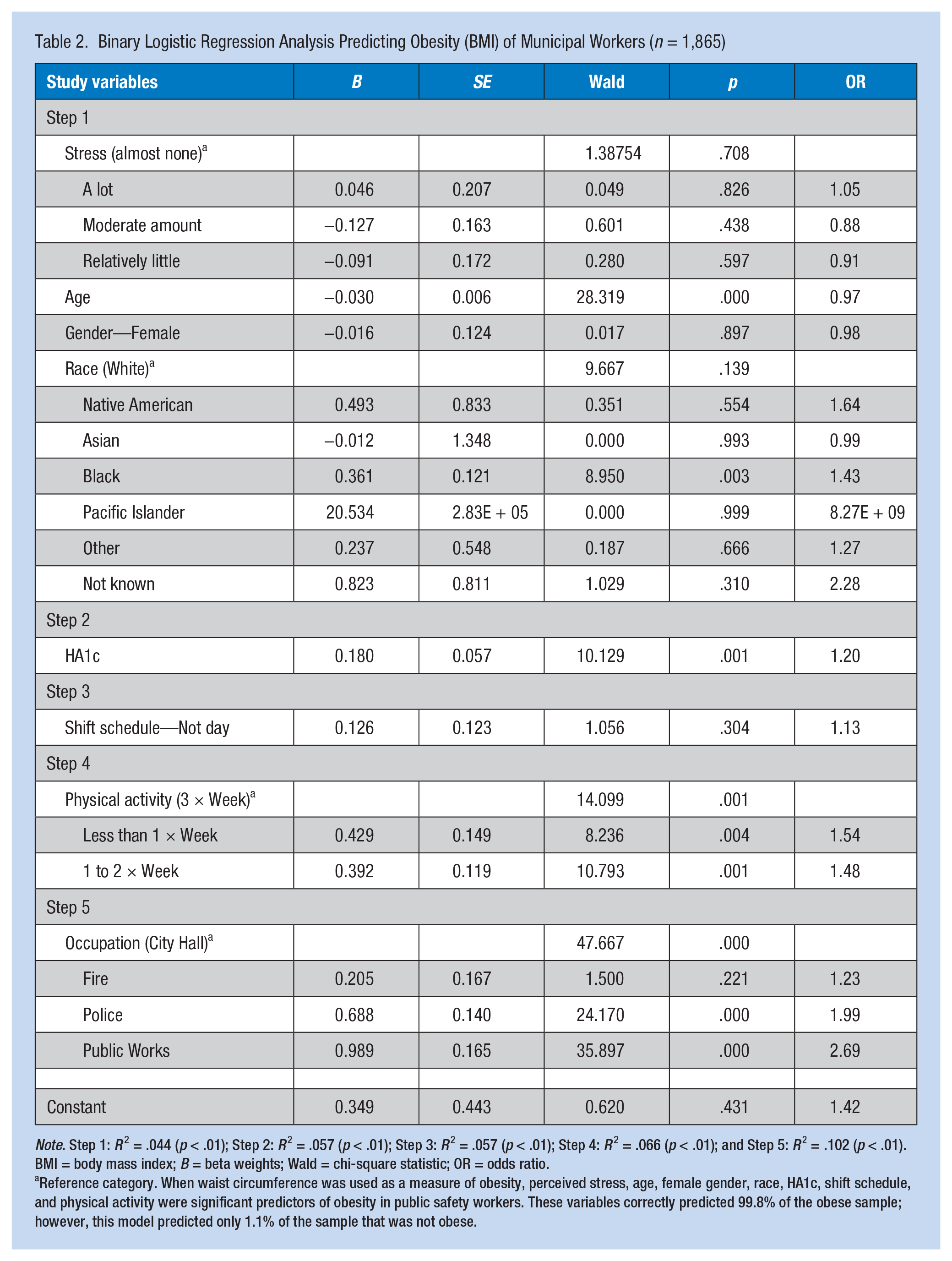
Note. Step 1: R 2 = .044 (p < .01); Step 2: R 2 = .057 (p < .01); Step 3: R 2 = .057 (p < .01); Step 4: R 2 = .066 (p < .01); and Step 5: R 2 = .102 (p < .01). BMI = body mass index; B = beta weights; Wald = chi-square statistic; OR = odds ratio.
Reference category. When waist circumference was used as a measure of obesity, perceived stress, age, female gender, race, HA1c, shift schedule, and physical activity were significant predictors of obesity in public safety workers. These variables correctly predicted 99.8% of the obese sample; however, this model predicted only 1.1% of the sample that was not obese.
Age, Black race, and BMI (Model 2) were significant predictors of prediabetes in municipal workers. Model 2 correctly predicted 83.2% of the sample as prediabetic (Table 3).
Binary Logistic Regression Analysis Predicting Prediabetes of Municipal Workers (n = 1,593)
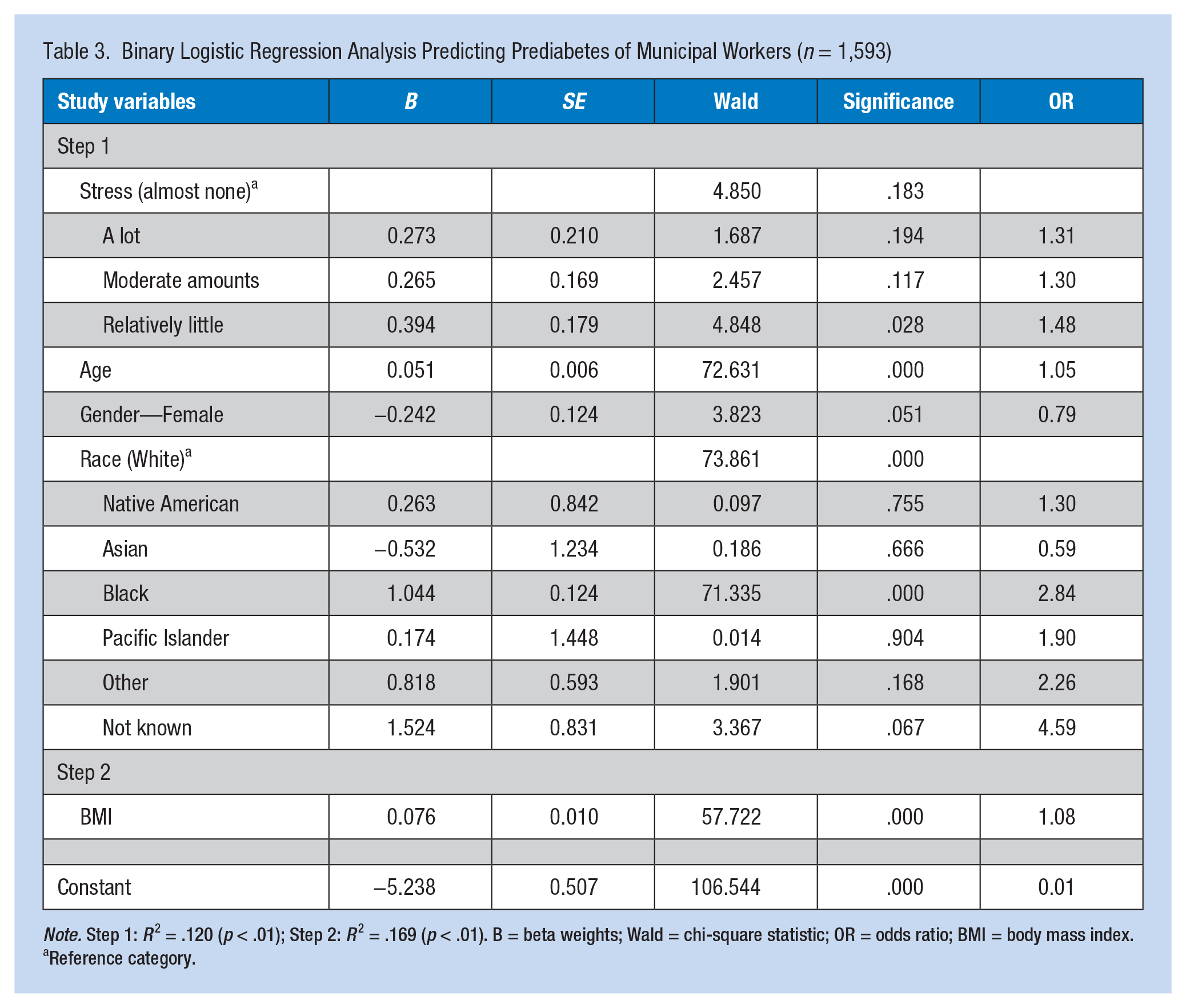
Note. Step 1: R 2 = .120 (p < .01); Step 2: R 2 = .169 (p < .01). B = beta weights; Wald = chi-square statistic; OR = odds ratio; BMI = body mass index.
Reference category.
Discussion
This study provided a unique examination of occupational, health risk, and demographic variables related to prevalence of obesity and prediabetes at the worksite. Although significant correlations between HA1c, BMI, obesity and prediabetes have been reported in previously published studies, those investigations lacked an occupational health nursing perspective; work-related factors have not been included in previous research on these conditions among workers. This study’s approach was unique because the researchers examined variables important to occupational health nurses, including work-related variables (e.g., shift schedule, occupation, and perceived stress). In addition, this study focused on a large municipal employee population that had health insurance. This study of risk factors for obesity and prediabetes in a large insured employee population contributes to the body of scientific knowledge for the occupational health field.
In the current study, age, Black race, HA1c, physical activity, and occupation were significant predictors of obesity in municipal workers. In terms of clinical practice, these predictors can be used to identify employees at highest risk for obesity and developing chronic illnesses associated with obesity. Findings from this study were congruent with previous research that modeled obesity (Paeratakul, Lovejoy, Ryan, & Bray, 2002). Of further importance are the findings that stress, gender, and shift schedule were not predictors of obesity.
Age, female gender, HA1c, and physical activity were significant predictors of obesity in public safety workers (i.e., police and firefighters). Public safety workers, especially firefighters, are expected to maintain a certain level of physical fitness to be effective at their jobs. In the current study, obesity, measured by BMI, was reported for 55.8% of the sample. Meanwhile, obesity, measured by waist circumference, was reported for 53.1% for the same sample. Body mass index is the gold standard for identifying adults at increased risk for adverse health outcomes related to obesity (NIH, National Heart, Lung, and Blood Institute, 2000). Waist circumference has utility in clinical situations, but BMI is linked with a broader range of health outcomes, and most published treatment studies use BMI as an obesity and disease marker (McTigue et al., 2003).
Age, Black race, and BMI were significant predictors of prediabetes in municipal workers. This finding is clinically significant because a health care provider who knows only three pieces of information (age, Black race, and BMI) could tailor interventions to avert the onset of prediabetes and diabetes. Interestingly, in examining the combination of factors which an occupational health nurse would be concerned about as possible predictors of prediabetes, it was found that the variables which did not predict prediabetes were shift schedule, level of activity, and occupation. Overweight, obesity, and non-White ancestry were among the risk factors identified by the American College of Endocrinology and the American Association of Clinical Endocrinologists for prediabetes screening (Garber et al., 2008). These risk factors were among the significant predictors of prediabetes in the current study as well.
The majority (87.8%) of the municipal workers in this sample were overweight or obese, which increases their risk for injury, absenteeism, unemployment, or disability (Schulte et al., 2007). An employee on the 11:00 p.m. to 7:00 a.m. shift had the highest BMI. Numerous studies have reported that shift schedules can affect workers’ health (Dobson et al., 2013; Han, Storr, Trinkoff, & Geiger-Brown, 2011; Munir, Clemens, Houdmont, & Randall, 2012; Zhao, Bogossian, Song, & Turner, 2011). Han and colleagues (2011) argued that work schedules may lead to obesity because long hours and varying schedules disrupt normal eating times and reduce access to healthy food; shift rotation may also affect circadian rhythms with detrimental effects on sleep quantity and quality. Employees working Fire Shifts A, B, and C had the lowest BMI (30.34). This finding was unexpected and unique because, as an occupational group, firefighters have one of the highest prevalence rates of obesity, ranking third among male occupations (Dobson et al., 2013). The results from this current study can possibly be explained by the level of firefighter physical fitness required to maintain job performance and a work schedule that guaranteed 2 days off duty between shifts promoting physically activity.
In the current study, female participants comprised 27.2% of the sample. When gender and BMI were compared, female municipal workers were more obese than males. This finding was consistent with results from other studies (Flegal et al., 2012). The largest ethnic group in the current study was African American, comprising 66.9% of the sample. Black race was a statistically significant predictor of obesity; this finding is consistent with other published studies (Flegal et al., 2012; Wang & Beydoun, 2007).
The relationship between obesity and education was significant in this study. The highest BMI was found in participants who reported “some college” and the lowest BMI was found in those reporting “high school or less.” This finding was surprising and inconsistent with most studies for which an inverse relationship between obesity and education (e.g., obesity decreased with more education) was reported (Cavaliere & Banterle, 2008). These findings may be explained by employment that provided insurance coverage and easy access to health care, regardless of education. It should also be noted that regardless of education, the BMI in this population was above 30. Lack of variability in measures of obesity may have influenced these results.
In the current study, HA1c was measured on 1,963 participants, and 51% of these participants were identified as prediabetic. Hemoglobin A1c is routinely measured for employees aged 40 years or older. Consistent with other research, the current study demonstrated an inverse relationship between level of activity and prediabetes and between level of activity and obesity (Dorsey & Songer, 2011; Gill & Cooper, 2008; Hu, Lakka, Kilpelainen, & Tuomilehto, 2007; Look AHEAD Research Group, 2010; Malin, Gerber, Chipkin, & Braun, 2012). The association between obesity and prediabetes has been well established such that evidence-based weight loss programs are recommended for Medicare beneficiaries who are obese and at risk for developing diabetes (Thorpe & Yang, 2011). In the current study, the highest percentage of prediabetic workers was found in the obese group.
In this study, no significant relationships were found among perceived stress, obesity, and prediabetes. Brunner, Chandola, and Marmot (2007) reported employees who worked under stressful conditions had 50% higher odds of obesity than those who did not experience stress. Findings in the current study did demonstrate a significant relationship between perceived stress and occupation, with the most stress reported by police officers and the least stress reported by Public Works employees. Multiple studies have demonstrated a correlation between stress and occupation (Collins & Gibbs, 2003; Franke, Ramey, & Shelley, 2002; Peretti-Watel, Constance, Seror, & Beck, 2009; Ramey, Franke, & Shelley, 2004; Tomei et al., 2006; Violanti et al., 2006).
This study was designed to provide occupational health nurses with evidence (e.g., significant demographic, health-related, and occupational risk factors) of how to tailor health promotion programs to reduce obesity and the risk of prediabetes. Because one of the best places to promote the health of individuals is the worksite, occupational health nurses, using information from this study, could develop targeted screening and wellness programs to reduce obesity, prediabetes, and cardiovascular events.
Limitations
Several limitations of this study should be noted. The exploration of correlational relationships among perceived stress, obesity, and prediabetes was limited because of the temporal design of the survey question that measured the stress experienced by each participant in the past 2 weeks. The use of secondary data prevented additional variables or research questions (e.g., investigating the relationship among obesity, shift schedule, circadian rhythms, and obstructive sleep apnea) from being included in the study. A small amount of variance was explained by the three models applied in the current investigation. Adding more variables to the models in future investigations may improve their explanatory power and further enhance understanding the effects of obesity and prediabetes in this population. A methodological limitation was the cross-sectional, correlational design that precluded causal interpretations. The use of self-report survey items might have encouraged socially desirable responses on certain questionnaire items. The cohort of workers participating in this study were all employed, insured, and resided in the Southeast; however, even though race, gender, and age varied, the sample was somewhat homogeneous which limits the generalizability of the findings.
Implications for Occupational Health Nurses
Because age, race, HA1c, physical activity, and occupation were significant predictors of obesity, occupational health nurses should assess these factors when evaluating individuals at the workplace. On-site wellness clinics are growing in popularity based on their cost-saving benefits for both employers and employees. Occupational health nurses are uniquely educated to assume this role in wellness clinics because a large part of nurses’ education focuses on the prevention of illness and promotion of healthy behaviors. The current study emphasized the relationship of healthy behaviors, such as physical activity, with obesity and prediabetes.
Given the high percentages of obesity and prediabetes in the study population, screening with BMI, waist circumference, and HA1c by occupational health nurses is of utmost importance and relevance. Obesity is a known risk factor for chronic conditions such as metabolic syndrome, diabetes, and cardiovascular disease. Advanced practice nurses are especially well trained in counseling workers regarding lifestyle behaviors and identifying those individuals who are at risk or currently have prediabetes and diabetes.
Occupational health nurses should design programs to target obesity and prediabetes, and based on study findings, identify predictors of these chronic conditions (e.g., age, gender, race, HA1c, BMI, physical activity, and occupation). Obesity and prediabetes can affect work performance, especially for firefighters and police officers. Obesity can hinder performance when climbing a ladder or, in the case of a police officer, hinder reaction time when encountering violence. In maximizing the well-being and functional capacity of each individual, occupational health nurses can contribute to improved population health.
Conclusion
Despite health coverage and screening at this workplace, 32% of participants were overweight and 55.8% had BMIs consistent with obesity. Further research should investigate risk reduction programs aimed at limiting obesity and the prevention of prediabetes in this population. More research is needed to explore how work environments can foster or inhibit worker obesity. Employers are committed to lowering health care claims costs by retaining healthy and productive employees who engage in healthy behaviors to prevent obesity and prediabetes. Before implementation of new programs, researchers should investigate barriers to employees participating in existing programs.
Applying Research to Practice
As obesity and overweight were highly prevalent (87.8%) in the study participants, body mass index (BMI), waist circumference, and HA1c were found to be significantly related. Obesity is a known risk factor for chronic conditions such as hypertension, stroke, diabetes, and cardiovascular disease. Based on the findings from the current study, the predictors of these chronic conditions, namely, age, gender, race, HA1c, BMI, physical activity, and occupation, should be evaluated. Obesity and prediabetes can affect work performance especially in public safety jobs. In maximizing the well-being of each individual, occupational health nurses have the potential for improving the health of the working population.
Footnotes
Acknowledgements
Dr. O’Keefe acknowledges the National Institute for Occupational Safety and Health (NIOSH) for the fellowship award during her doctoral studies, the Good Health Program, the City of Birmingham, and the University of Alabama at Birmingham.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Louise C. O’Keefe, PhD, CRNP, is an assistant professor at the University of Alabama in Huntsville, College of Nursing. She established and is the director of the Faculty and Staff Clinic on the campus of the University of Alabama in Huntsville.
Kathleen C. Brown, PhD, RN, is currently an adjunct professor at the University of Alabama at Birmingham School of Nursing. At the time of this study, she was professor and chair of Community Health, Outcomes and Systems, teaching in a NIOSH-funded graduate program in occupational health nursing.
Karen H. Frith, PhD, RN, NEA-BC is the Associate Dean for Undergraduate Programs and Professor in the College of Nursing at The University of Alabama in Huntsville. Her area of specialty is nursing administration and informatics.
Karen L. Heaton, PhD, FNP-BC, FAAN, is associate professor and coordinator of the PhD program at the University of Alabama at Birmingham School of Nursing. She is also the OHN director for the NIOSH-funded Deep South Center for Occupational Health and Safety (T42OH008436).
Elizabeth H. Maples, PhD, was an assistant professor at the UAB School of Public Health during this study and served on Dr. O’Keefe’s dissertation committee.
Jennan A. Phillips, PhD, RN, FAAOHN, is an associate professor and program director for the Accelerated Masters in Nursing Pathway at the University of Alabama at Birmingham. Her research and scholarly contributions are in the areas of development and evaluation of educational materials for nurses, illness and injury prevention among disadvantaged communities, and occupational and environmental health nursing.
David E. Vance, PhD, MGS, is a professor of psychology and the associate director of the Office of Research and Scholarship, both within the UAB School of Nursing. He studies cognitive neuroscience in aging, driving behavior, HIV, breast cancer, and other health-related areas.