
Abstract
Low back pain (LBP) is a major public health problem that adversely affects the quality of life (QOL) of workers. The etiology of LBP is considered to be multi-factorial with individual, physical, and psychosocial factors contributing to its development and persistence. Although prevention of LBP in workers in the workplace is very important, only a small number of studies have assessed the risk factors and epidemiology of LBP among Japanese factory workers who stand as part of their job. This cross-sectional study investigated the prevalence of LBP in 691 factory employees who conducted their work while standing. Health-related QOL was evaluated using the Roland-Morris Disability Questionnaire (RDQ) to quantify the severity of LBP with the aim of identifying risk factors for LBP among workers who stand as part of their work in an electronics manufacturing company. We observed that the prevalence of LBP lasting for at least 48 hours within a week was 20.0% among participants, with female employees and those with a prior history of LBP having a significantly increased risk of developing LBP. The distribution of the RDQ score showed a negative regression curve among the employees, which was different from the normal distribution pattern reported previously in Japanese patients with LBP. These findings suggest that prolonged standing among factory workers poses an increased risk for LBP.
Introduction
Low back pain (LBP) is a serious public health issue. In addition to negatively impacting the well-being and quality of life (QOL) of workers, it also contributes markedly to the global disease burden due, in part to the difficulty with diagnosing and treating the condition (Dagenais, Caro, & Haldeman, 2008; Kikuchi, 2017). In an estimate of the global disease burden between 1990 and 2010, the World Health Organization found that musculoskeletal disorder sufferers were deprived of a mean 6.8 disability-adjusted life years. Low back pain is also associated with close to 50% of musculoskeletal disorders and was the most frequent condition among 289 diseases within the Asia Pacific region (Murray et al., 2012; Vos et al., 2012).
The development and persistence of LBP are thought to be associated with multiple factors, including individual, physical, and psychosocial factors. Studies to date have found that LBP was associated with middle age (45 to 64 years), being female, lower educational status, obesity, smoking, sleep deprivation, extended periods of driving, and prolonged time of computer use (Chen, Chang, Chang, & Christiani, 2005; Dionne et al., 1995; Juul-Kristensen, Søgaard, Strøyer, & Jensen, 2004; Kopec, Sayre, & Esdaile, 2004; Shiri et al., 2013; van de Water, Eadie, & Hurley, 2011). Psychosocial factors including stress and depressive symptoms may also increase the risk of LBP (Andersson, 1999; Hoogendoorn, van Poppel, Bongers, Koes, & Bouter, 2000). A systematic review of 18 prospective cohort studies reported conflicting findings between LBP and numerous factors including engaging in sports and exercise during leisure time, full body vibration during work, heavy physical work, and postures involving bending and/or twisting of the trunk while working (Bakker, Verhagen, van Trijffel, Lucas, & Koes, 2009). Several studies have reported prolonged standing as a risk factor for LBP due to increased trunk or gluteal muscle activity, and a higher load on the lumbar spine (Andersen, Haahr, & Frost, 2007; Coenen, Parry, et al., 2017; Coenen, Willenberg, et al., 2016; Fewster, Gallagher, Howarth, & Callaghan, 2017; Gregory, Brown, & Callaghan, 2008; Gregory & Callaghan, 2008; Macfarlane et al., 1997). In contrast, some studies have demonstrated no significant associations between prolonged standing and LBP (Harkness, Macfarlane, Nahit, Silman, & McBeth, 2003; Yip, 2004). To date, no studies have been carried out in workers at an electronics manufacturing company in Japan, in which workers are consistently exposed to prolonged standing. This cross-sectional study aimed to examine the prevalence of LBP in employees at an electronics manufacturing factory in Japan who conduct their work while standing.
Materials and Methods
We carried out a cross-sectional survey of employees at an electronics manufacturing factory (TDK Corporation) in Japan. This private factory, one of biggest electrical companies in Japan, manufactures and assembles electric parts such as capacitors, sensors, batteries, and other components. Our study was approved by our institution’s institutional review board for observation and epidemiological studies at Chiba University. Informed consent was obtained from all participants.
Study Participants
The TDK factory, in the Kanto region of Japan, and its subsidiary companies conduct annual general health checkups, which include standard internal medical counseling and physical assessments. For the present study, all eligible employees among the 2,025 employed at this TDK factory completed a general checkup and survey on LBP within a few days of their annual general checkup. According to the Japanese Labor Standards Law, all employees work 8 hours per day and a total of 40 hours per week, and have a 45- to 60-minute break every day. We checked the employees’ schedule and recorded their standing time during the workday. Employees who satisfied the following criteria were included in the analysis: (a) standing for more than 70% of their work day; and (b) conducting at least one of the following work activities in the standing position as part of their daily work including continuous arm movements, lifting, some rotation of the trunk, and/or heavy lifting. These tasks were ascertained through self-report from the worker. Data on demographic variables such as age, sex, height, and body mass index (BMI) expressed as kilograms (kg) per meters2 (m2) were collected during the checkup. Data on the details of the individual’s work, and whether it involved heavy lifting of >20 kilograms (kg) were also collected. In addition, we collected data on other possible risk factors for LBP, such as how often workers engaged in regular exercise, current or former smoking status, past history of continuous LBP for 1 week or more, and past history of lumbar spine surgery. Regarding exercise, the participants were asked to report whether they undertook a modest to competitive amount of physical activity such as jogging, tennis, swimming, gymnastics, and/or soccer for at least 30 minutes per day (Björck-van et al., 2008). Positive smoking status included smoking five cigarettes or more every day for 1 month or more (Deyo & Bass, 1989).
LBP Measurement
Each employee was asked whether they had experienced LBP lasting 48 hours or more within the week prior to their general health checkup. LBP was defined as pain located in the region between the costal margin and inferior gluteal folds (Krismer & van Tulder, 2007). Only participants with LBP who attended the annual screening and met our inclusion criteria were asked to complete the Roland-Morris Disability Questionnaire (RDQ). RDQ is an established scale used to assess the severity of LBP and allows patients to answer questions about the disability they experienced during usual daily activities as a result of LBP. The questionnaire includes 24 items about disability that may occur during daily activities such as standing, walking, sitting, lying, dressing, sleeping, and working. Each item in the RDQ can be answered as either “Yes” or “No.” The RDQ score is calculated as the total number of positive responses, with the scores ranging between 0 and 24, with a higher score indicating greater disability (Roland & Morris, 1983). The Japanese version of the RDQ has been validated in a study by Suzukamo et al. (2003) with Japanese patients with LBP.
Data Analysis
Statistical analysis was performed using SPSS Software, version 25 (IBM, Armonk, NY, USA). The unpaired t test was used to analyze mean values between the two groups and the χ2 test to examine proportions for categorical data. The prevalence of LBP was assessed by gender, age (≤29, 30-39, 40-49, or ≥50 years), height (<165 cm or ≥165 cm), and BMI (<18.5, 18.5-25, or ≥25 kg/m2) strata. The prevalence of LBP was also compared in groups involved with or without heavy lifting, past history of LBP, past history of lumbar spinal surgery, and smoking status and exercise habits. Univariate analysis was performed for each factor, and the odds ratio (OR) and 95% confidence intervals (CI) were calculated, with factors with P values <.15 used for inclusion of variables in the multivariate logistic regression models. The distribution of the RDQ scores and its regression curve were determined in the study cohort for comparison with the general population. In addition, the mean RDQ scores were examined across demographic and occupational study variables.
Results
A total of 691 of 694 employees (570 males, 121 females) met the criteria for standing 70% of the time at work. Table 1 summarizes the employees’ baseline characteristics. The employees had a mean age of 40.1 years (range, 15–68 years); most were in their 30s (n = 264, 38.2%), followed by those in their 40s (n = 144, 20.8%), with their mean height and BMI being 167.5 cm and 23.0 kg/m2, respectively. Heavy lifting >20 kg was carried out by 45.2% of employees. In total, 24.9% (n = 172/691) of employees had previously experienced LBP lasting for 1 week or more, and 0.9% (n = 6/691) of employees had a past history of lumbar spinal surgery. For smoking status, 61.9% (n = 428/691) of employees have never smoked, 2.7% (n = 19/691) were former smokers, and 35.3% (n = 244/691) were currently smoking. Regarding exercise, 27.9% (n = 193/691) exercised 1 to 4 days/week, and 1.9% (n = 13/691) exercised 5 to 7 days/week. In total, 70.2% of employees (75.2% of females and 69% of males) failed to exercise at least once a week.
Demographic Characteristics of Factory Employees (n = 691)
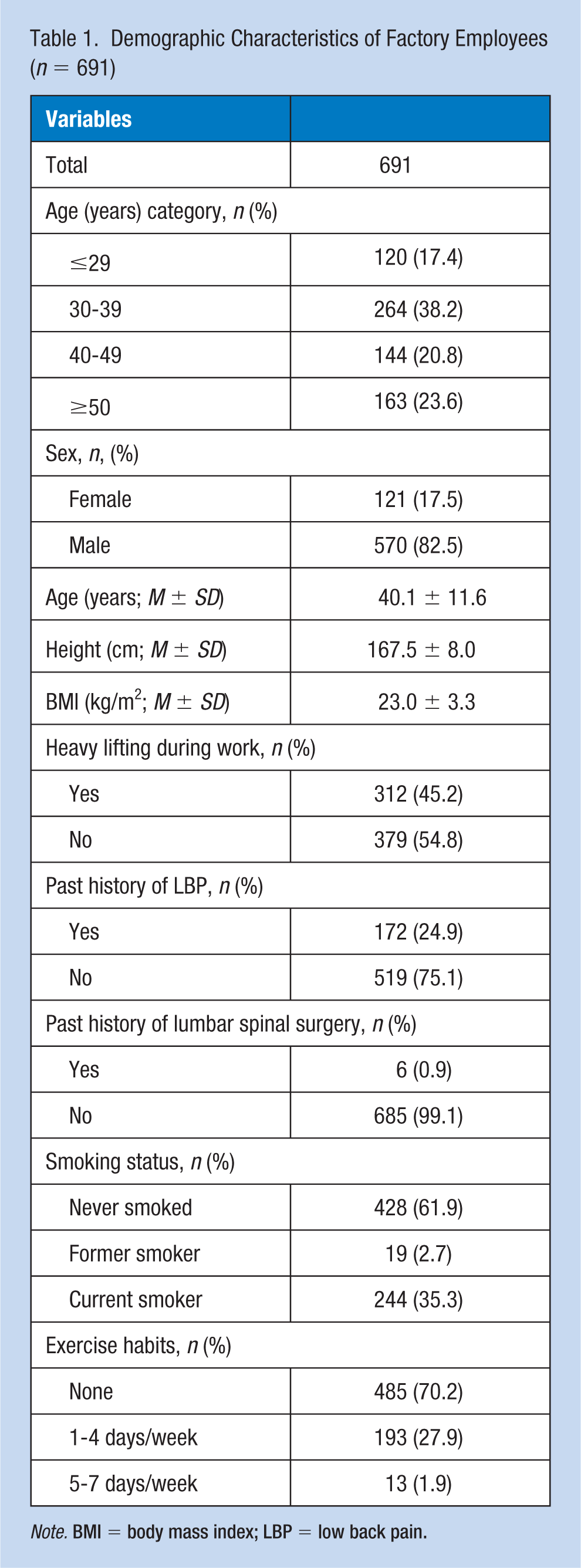
Note. BMI = body mass index; LBP = low back pain.
Prevalence and Risk Factors for LBP
Of the 691 employees, 138 (20.0%) indicated that they had experienced continuous LBP for 48 hours or more within the week before their general health checkup. Table 2 shows the comparison of demographic variables between employees with and without LBP. The prevalence of LBP was highest in employees aged 50 years or older (28.2%), followed by those aged 40 to 49 years (22.2%). The incidence increased gradually in higher age stratum. Females had a higher incidence of LBP than males, although this difference was not statistically significant (25.6% vs. 18.8%, p = .06). Employees who performed heavy lifting (23.4% vs. 17.2%), or had a past history of either LBP (47.7% vs. 10.8%) or lumbar spine surgery (66.7% vs. 19.6%) had a significantly higher incidence compared with employees without these experiences (p < .05). There was no significant difference in the prevalence of LBP according to height or BMI stratum. The prevalence was also not different in employees with different smoking status or exercise habits.
A Comparison of the Demographic Characteristics Between Employees With and Without Low Back Pain
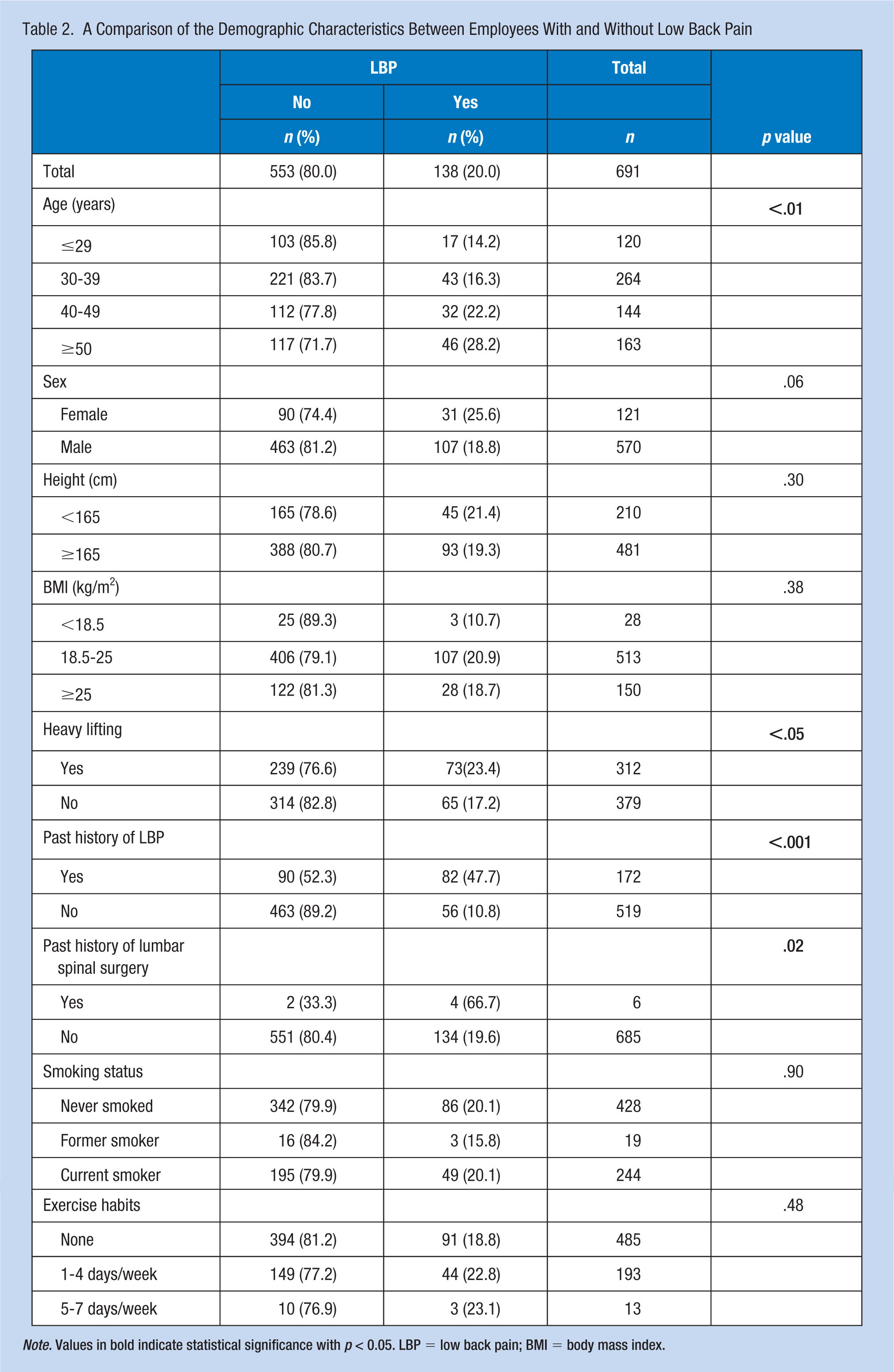
Note. Values in bold indicate statistical significance with p < 0.05. LBP = low back pain; BMI = body mass index.
The risk factors for the development of LBP in the employees using univariate and multivariate analysis are presented in Table 3. The univariate analysis showed that being at least 40 years of age (OR = 1.84), performing heavy lifting >20 kg (OR = 1.47), and a previous history of either LBP (OR = 7.53) or lumbar spinal surgery (OR = 8.22) were significant risk factors for developing LBP in the previous week (all p < .05). Although being female (OR = 1.49) was not a significant factor, it was included in subsequent multivariate logistic regression analysis. The results of this multivariate analysis found female sex (OR = 2.13) and a previous history of LBP (OR = 7.42) were significant risk factors for developing LBP.
Univariate and Multivariate Analyses of Risk Factors for the Development of LBP
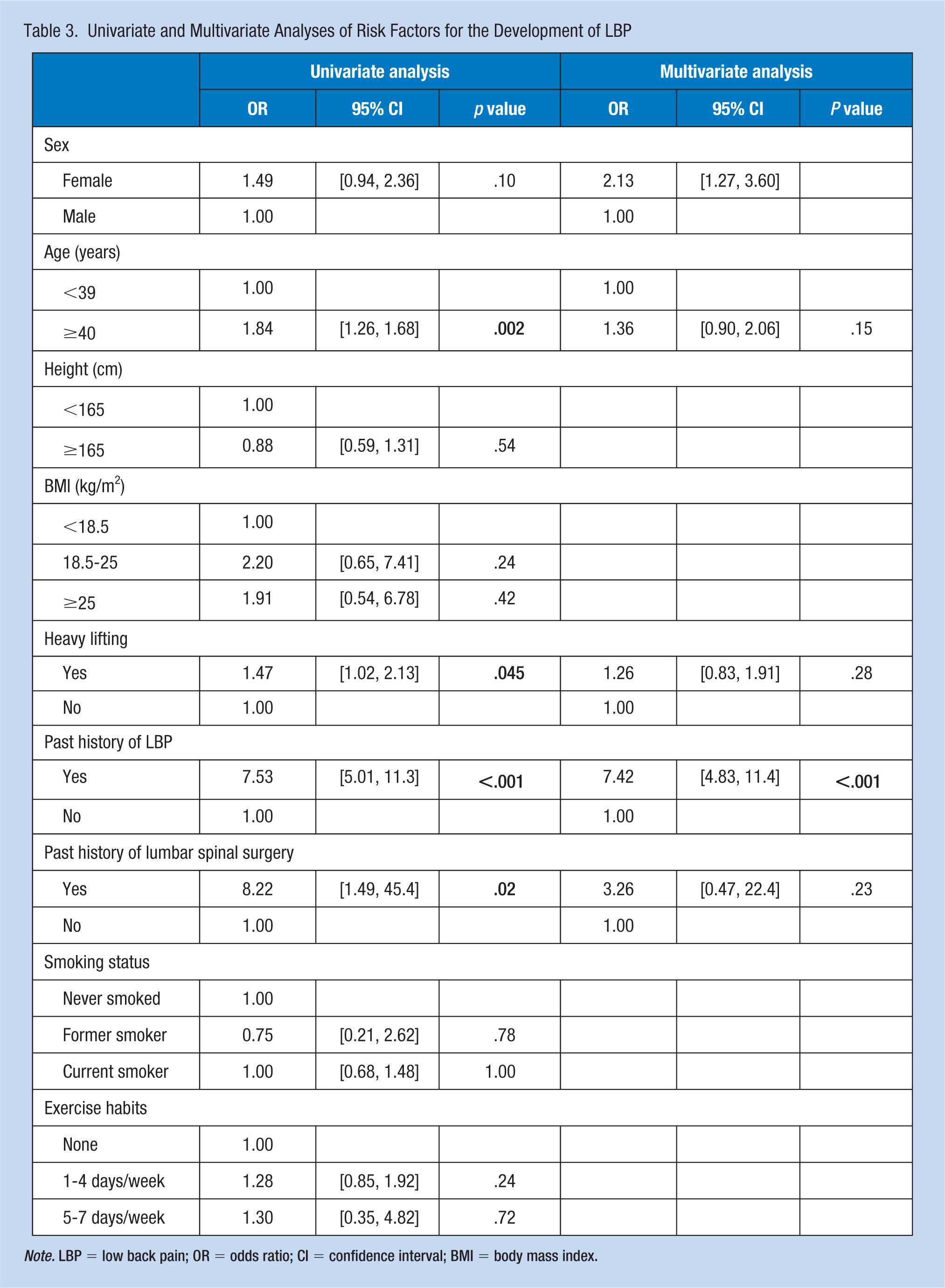
Note. LBP = low back pain; OR = odds ratio; CI = confidence interval; BMI = body mass index.
RDQ Among LBP Workers Only
The mean RDQ score was 4.10 (SD, 4.15; range, 1–21) in the 138 employees with LBP. Figures 1 shows the distribution of RDQ scores, the trend line of which demonstrated a negative regression curve, indicating there existed more employees with modest LBP and few employee showed severe LBP with RDQ score ≥17. There was a significant difference in RDQ scores between employees who did and did not conduct heavy lifting as part of their usual work duties (M ± SD, 5.0 ± 4.6 vs. 3.2 ± 3.3, p = .01) (Table 4). In contrast, there was no statistically significant difference in RDQ scores stratified according to sex, age, height, BMI, and previous history of LBP and lumbar spine surgery.
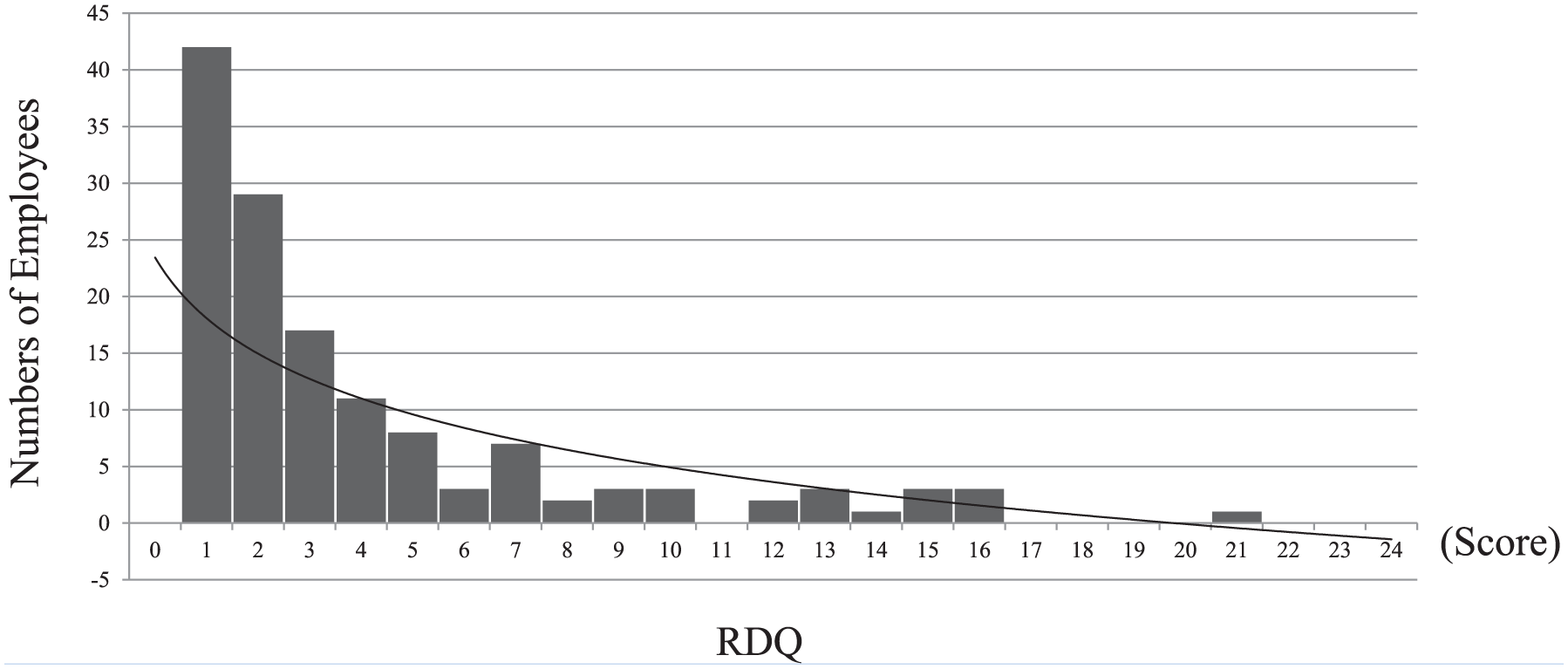
The distribution of the RDQ scores in all the employees.
A Comparison of Employees’ Demographics by the Mean RDQ Scores
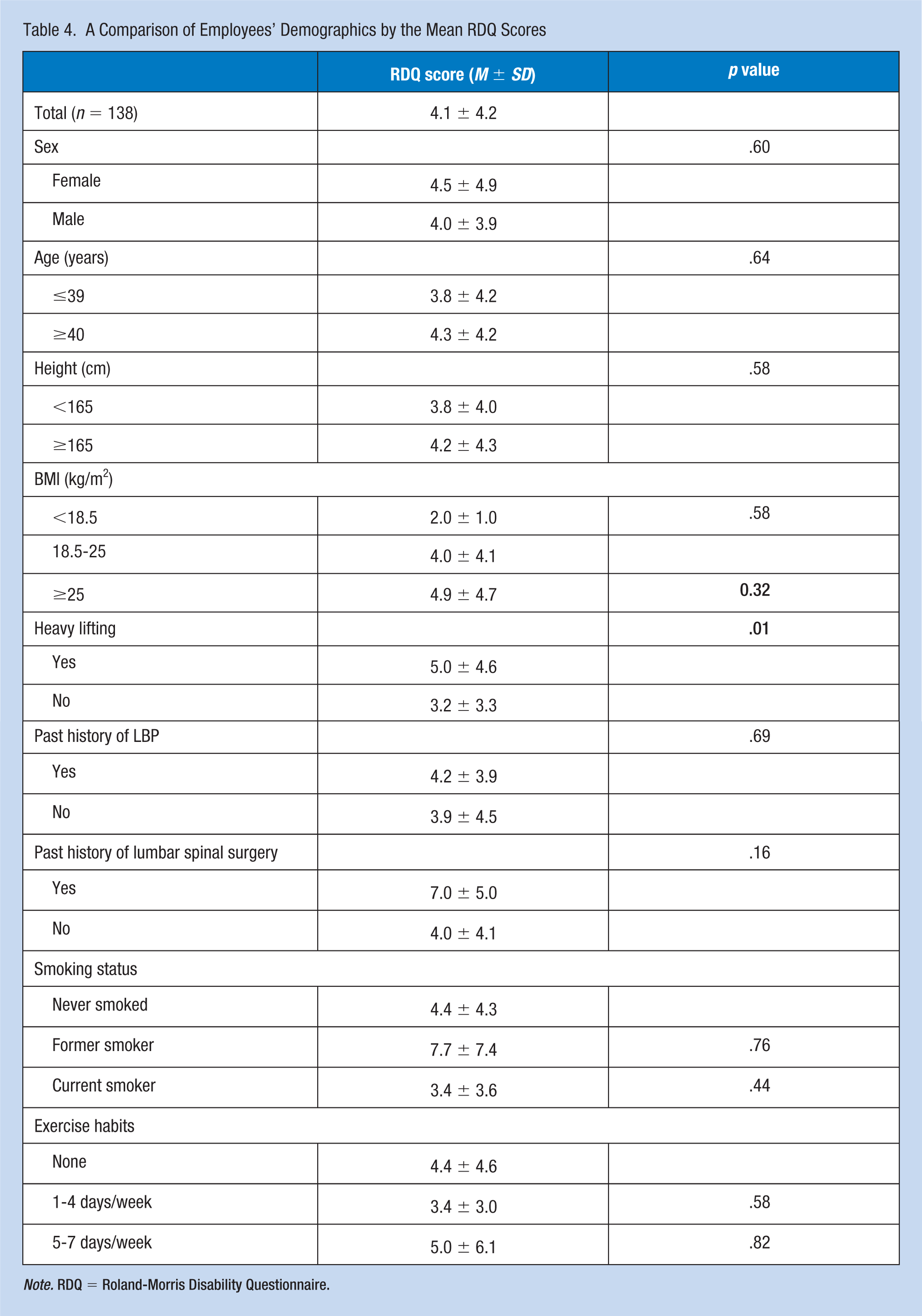
Note. RDQ = Roland-Morris Disability Questionnaire.
Discussion
This cross-sectional study examined the prevalence, possible risk factors, and characteristics of LBP in employees who conducted their work while standing at an electronics manufacturing organization in Japan. Among these employees, one fifth reported experiencing LBP within the week before their general health checkup. The 20% prevalence of LBP within a week of the checkup in the present study is lower than the 35.7% reported for the general Japanese population (Fujii & Matsudaira, 2013). A nationwide epidemiological survey of 11,507 randomly selected Japanese people aged 18 years or older demonstrated an approximately 25% prevalence of LBP within a week of their checkup (Nakamura, Nishiwaki, Ushida, & Toyama, 2011). The discrepancy between the prevalence of LBP in our study and previous reports suggests that our results may not be generalizable because our sample was confined to factory employees whose work did not involve extreme or awkward postures or exposure to full body vibration, which were previously reported as risk factors for LBP (Coenen, Willenberg, et al., 2016).
Recent studies have demonstrated that spending extended periods standing has an effect on the development of LBP (Coenen, Parry, et al., 2017; Coenen, Willenberg, et al., 2016; Fewster et al., 2017). Kopec et al. showed that men who stood as part of their usual daily activities were at greater risk of LBP (Kopec et al., 2004). Macfarlane et al. (1997) also showed that women who stood more than 2 hours per day were at greater risk of developing LBP. In contrast, a number of studies have demonstrated negative correlations between standing mechanical loads and LBP incidence (Harkness et al., 2003; Yip, 2004). The association should be evaluated in greater detail in future studies.
Our findings agree with a number of reports that showed female sex was a significant risk factor for LBP, especially chronic LBP, among the general population and certain types of employees (Spyropoulos et al., 2007; Tomita et al., 2010). However, a 2-year prospective study by Matsudaira et al. demonstrated that female Japanese employees had a lower prevalence of LBP among initially symptom-free employees (OR = 0.79) (Matsudaira et al., 2012). The discrepancies in these findings may have arisen from the use of different definitions for LBP between studies. LBP prevalence may be higher in females because of differences in either the subset of the population selected for our study or work activities between sexes. In addition, a previous study showed that most employees who experience an episode of LBP will have a recurrence within 1 year (Von Korff, Deyo, Cherkin, & Barlow, 1993). The result of our multivariate analysis that a prior episode of LBP is a risk factor for recurrence is consistent with previous findings (Papageorgiou et al., 1996).
Our univariate analysis showed aged 40 years or older were also at significant risk factor for LBP. In a study of 11,507 individuals in the general Japanese population, Nakamura et al. reported 16.5% and 15.0% LBP prevalence at age <40 and ≥40 years, respectively (Nakamura et al., 2011). In addition, the Japanese nationwide Research on Osteoarthritis/osteoporosis Against Disability (ROAD) cohort study reported that the incidence of LBP in the general population was independent of age stratum (Muraki et al., 2012). However, the correlation between age and LBP remains controversial among Japanese employees, suggesting that the prevalence among various age strata may be affected by differences in occupation or working environment (Kawaguchi et al., 2017; Matsudaira et al., 2011). Our univariate analysis also demonstrated that previous lumbar spine surgery was a risk factor for LBP. Even cases in which lumbar surgery was successful may also experience LBP due to soft tissue injury, diminished spinal stability, or spinal stenosis (Ragab & Deshazo, 2008).
We also examined the potential correlation between LBP and height, BMI, smoking, and exercise. Past reports including a meta-analysis have shown that being overweight is a risk factor for LBP (Heuch, Hagen, Heuch, Nygaard, & Zwart, 2010; Shiri et al., 2013). In addition, smoking can induce lumbar disk degeneration and subsequently LBP (Magora, 1972; Wang et al., 2012). However, we did not observe a significant correlation between these factors and LBP. Only 29.8% of the participants surveyed in this study exercised at least once a week, suggesting that these employees were primarily sedentary. However, reviews suggest that sports and exercise may not be associated with LBP (Bakker et al., 2009; Heneweer, Staes, Aufdemkampe, van Rijn, & Vanhees, 2011).
The RDQ revealed that the average RDQ score among the 138 employees with LBP was 4.1, which was lower than that observed in a previous validation study in which 214 patients with LBP reported a mean of RDQ = 9.1 (Suzukamo et al., 2003). These findings suggest that the severity of LBP in our study population was not sufficient to require clinical treatment. However, this RDQ score is comparable with that reported in our previous study in 201 employees from the same factory who conducted their work while sitting (mean RDQ = 4.0; SD, 4.2; range, 1–22) (Inoue et al., 2015). The score in this earlier study could have been relatively lower because there was a maximum 10-day interval between the day the employee felt LBP and the recording of LBP. The distribution of RDQ scores among all employees in our study produced negative regression curves. This trend differed from the almost normal distribution observed for the general population (Suzukamo et al., 2003), indicating that working while in a standing position is far from a normal daily work activity. However, we did not investigate the ergonomics of the working or standing environment.
The present study had several limitations. First, we did not examine the ergonomic factors that may affect employees who conduct their work while standing. Work environments can be adapted to improve employees’ postures such as adjusting the height of workbenches or providing options for back support to decrease overuse and tiredness of the back muscles. Both these strategies have been reported to help prevent the development or aggravation of LBP (Larivière, Gagnon, Gravel, & Bertrand Arsenault, 2008). Specifically, due to limited resources, we did not conduct a detailed examination of the workplace or equipment design, both of which could be associated with LBP (Driessen et al., 2011; Gilson, Suppini, Ryde, Brown, & Brown, 2012; Radas et al., 2013). Adjusting awkward postures can decrease LBP risk (Keyserling, Punnet, & Fine, 1998). Although the employees in this study were not exposed to continuous awkward postures, a further more detailed analysis of posture may help to improve methods for preventing. Second, we cannot conclude that LBP was related only to work. The design of the current study makes it difficult to determine whether LBP was related to work or nonwork, and therefore the onset of LBP can be affected by both lifestyle and work style. Third, while we evaluated demographic and physical factors, we did not examine psychosocial factors associated with LBP. Many studies have highlighted the significance of discerning the psychosocial characteristics of LBP (Andersson, 1999; Hoogendoorn et al., 2000; Matsudaira, Konishi, Miyoshi, Isomura, & Inuzuka, 2014). However, despite these limitations we consider that our results from one of the biggest companies in Japan can help to improve the working environment and prevent the occurrence of LBP in standing workers.
In summary, one fifth of our participants reported LBP lasting for 48 hours or more within the past week. Female sex and a history of LBP were significant risk factors for LBP in Japanese employees who conduct their work while standing. The mean RDQ score was relatively low with the distribution showing a negative regression. Further studies are required to assess posture and ergonomic factors to develop strategies to reduce LBP prevalence in employees and to minimize the psychosocial burden of LBP.
Applying Research to Practice
We carried out this study to clarify whether prolonged standing was associated with LBP in Japanese employees in the workplace of an electronics manufacturing company. 20.0% of employees reported LBP lasting for 48 hours or more within the past week, and being female and having a past history of LBP were significant risk factors for LBP. To reduce the occurrence of LBP, responsible person for employees’ health care should note that environmental maintenance to prevent prolonged standing during their workplace is important.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Gen Inoue, MD, PhD, is an associate professor of orthopaedic surgery, Kitasato University School of Medicine.
Kentaro Uchida, PhD, is a senior lecturer of orthopaedic surgery, Kitasato University School of Medicine.
Masayuki Miyagi, MD, PhD, is a senior lecturer of orthopaedic surgery, Kitasato University School of Medicine.
Wataru Saito, MD, PhD, is a senior lecturer of orthopaedic surgery, Kitasato University School of Medicine.
Toshiyuki Nakazawa, MD, PhD, is a clinical associate professor of orthopaedic surgery, Kitasato University School of Medicine.
Takayuki Imura, MD, is a clinical senior lecturer of orthopaedic surgery, Kitasato University School of Medicine.
Eiki Shirasawa, MD, is an assistant professor of orthopaedic surgery, Kitasato University School of Medicine.
Tsutomu Akazawa, MD, PhD, is a clinical professor of orthopaedic surgery, St. Marianna University School of Medicine.
Sumihisa Orita, MD, PhD, is a research associate professor in Center for Advanced Joint Function and Reconstructive Spine Surgery, Graduate School of Medicine, Chiba University.
Kazuhide Inage, MD, PhD, is an assistant professor of orthopaedic surgery, Graduate School of Medicine, Chiba University.
Masashi Takaso, MD, PhD, is a professor of orthopaedic surgery, Kitasato University School of Medicine.
Seiji Ohtori, MD, PhD, is a professor of orthopaedic surgery, Graduate School of Medicine, Chiba University.