
Abstract
Nurses often encounter situations that require lifting patients, often using awkward body positions. Hiring nurses with strength suitable for these jobs decreases nurses’ risk for illness and injury and would be expected to result in more appropriate and lower health care, pharmacy, and disability costs. The physical strength of new hire nurse applicants was assessed using a defensible isokinetic evaluation in the years 2011 and 2012. Health care and pharmacy costs were monitored for the first 12 months following date of hire and compared with costs for nurses hired without screening during the prior 2 years (2009 and 2010). The strength assessment group had significantly (p < .05) lower health care and pharmacy costs per member per month (PMPM) compared with the comparison group. The study suggests that use of physical capability strength assessment is effective in hiring nurses with appropriate strength capability, resulting in significant health care and pharmacy cost avoidance.
Nursing can be a physically demanding profession. Although the Occupational Safety and Health Administration (OSHA) reports that work-related injuries are decreasing in all industries, workplace injury and illness rates in hospitals are nearly twice those in private industry as a whole, surpassing even manufacturing and construction (U.S. Department of Labor, Occupational Health and Safety Administration, 2013). This finding highlights the need to decrease on-the-job injuries, especially in hospital settings.
With regard to overall workforce health, recent publications report that population health management programs have gained popularity as a tool to control health care costs (Bolnick, Millard, & Dugas, 2013; Byrne et al., 2011; Consensus Statement of the Health Enhancement Research Organization, American College of Occupational and Environmental Medicine, and Care Continuum Alliance, 2013; Lerner, Rodday, Cohen, & Rogers, 2013; Parkinson, 2013; Parry & Sherman, 2012; PMA Companies, 2013). In some instances, the studies have shown returns on investment (ROI) of about US$3 for every US$1 spent (Caloyeras, Liu, Exum, Broderick, & Mattke, 2014; Cherniack, 2013; Nyman, Jeffrey, Abraham, Jutkowitz, & Dowd, 2013). In addition to implementing population health management to control health care costs, businesses are focusing on the worker more holistically (individual–environment fit). Today, an increasing number of businesses manage total worker health, including the integration of workers’ compensation, disability, medicine, pharmacy, safety, and related disciplines (Caspi et al., 2013; Dinenberg, 2013; Hymel et al., 2011; Loeppke et al., 2013; Robertson et al., 2013; Sorensen et al., 2013).
Most programs focus on measuring workplace health once employees are enrolled in the health plan. Very few programs start by looking at employee selection processes that facilitate the hiring of nurses who will have the strength to meet the physical demands of their jobs. Many companies with physically demanding jobs require applicant assessment to measure nurses’ abilities to safely perform the essential functions of the job. Most of these new-hire physical capability assessment programs focus on injury prevention with very little emphasis on the health risks of the applicants.
Companies that offer biometric screenings through their wellness programs generally focus on life-threatening diseases such as hypertension and diabetes (Consensus Statement of the Health Enhancement Research Organization, American College of Occupational and Environmental Medicine, and Care Continuum Alliance, 2013). Muscle strength, an occupational risk factor, is usually not considered. It is the contention of the authors of this study that strength will become a new vital sign of workplace health for specific occupations. The only way to maintain a healthy muscle mass is through physical activity, and considerable evidence exists that individuals who are physically active are also physically healthier than individuals who are physically inactive (Garber et al., 2011). Thus, the rationale behind hiring workers with physical capabilities that best fit the job at the onset, using a new hire screening program, is that costs associated with employees’ risk for illness and injury should be lower than those for employees who are not part of a new hire physical capability evaluation (PCE).
Applying Research to Practice
These findings have relevant implications for hiring nurses in a variety of settings. The aim of new-hire strength screening was to recommend appropriate workers for physically demanding jobs, which combats higher workers’ compensation costs. This study showed significant health care and pharmacy cost differences between nurses who met the physical capability requirements for nursing positions and those who were not screened. Further implications included cost savings related to retaining talent and decreasing turnover. Although this study focused on new-hire applicants, screening could also be applied to returning injured workers, job transfers, recreational injuries, or as part of overall wellness biometric screenings. Strength screening at the time of hire could also apply to other organizations, including heavy industry such as warehousing, utilities, transportation, food services, manufacturing, mining, and construction.
In addition to the personal, physical, and emotional strain of workplace injury, institutional business concerns include increased direct costs (i.e., short- and long-term disability, liability, and health care and pharmacy costs) and indirect costs (i.e., increased absenteeism, presenteeism, and workers’ compensation). The Centers for Disease Control and Prevention (CDC; 2013) estimated that these indirect costs represent 2 to 3 times the direct costs. The impact of hiring nurses with appropriate skills has important implications for business and worker burdens. Additional research is needed to strengthen the business case to integrate health protection and overall wellness by deepening the evidence around health outcomes and costs (Pronk, 2013).
Hiring employees with the skills that make them capable of successfully performing their jobs would not only prevent injuries and disability but also lead to better patient care, increase retention, and ultimately save resources and reduce personal pain and suffering. Pre-placement functional capacity evaluations are currently used in industry as a way to determine if individual applicants can perform the tasks required by a specific job role. In effect, hiring a workforce that is functionally capable of performing explicit job tasks is an “upstream” solution to preventing workplace injuries and disability.
This research study examined the impact of new hire strength assessment on health care and pharmacy claims within the first year of employment for nurses at a hospital facility, with further implications for how the program could improve patient care and the retention of qualified employees. The primary research hypothesis is that implementation of a screening for new hires to assess strength capabilities related to job functions would lower the risk of injury and illness as represented by lower health care costs.
Method
This quasi-experimental, non-randomized study was conducted at a large hospital group in northeast Ohio; the study was designed to assess the impact of a strength assessment for nurses at the time of hire and compare the difference in health plan costs with newly employed nurses who were not screened for strength. Participants were identified from the applicant pool from January 2009 through December 2012. Applicants were either registered nurses, licensed vocational nurses, licensed practical nurses, or patient care nursing assistants applying for a nursing position in any unit of the hospital. The interviewing process for potential candidates consisted of an online application, followed by a phone interview, and then an in-person interview, if warranted. Nurses who passed these initial requirements for selection were then scheduled for a physical examination and drug screen. A strength assessment screening was added to the existing hiring protocol as the last segment of the interview process for nurses hired between January 2011 and December 2012.
Nurses hired between January 2009 and December 2010, prior to the strength assessment screening implementation, served as a historical comparison group (HCG). No significant environmental or business practices were changed from January 2009 through December 2012, and health plan coverage did not change across the two time frames. The only difference in the selection process in 2011 and 2012 compared with 2009 and 2010 was the addition of the PCE™. The project was overseen by hospital administrators and conducted based on quality improvement protocols. Given that this was a retrospective analysis of a hiring practice policy and not a formal research study, Institutional Review Board approval or research consent was not required.
Strength Screening Intervention
The comprehensive strength screening evaluation for new hires in this study was conducted through an objective PCE™. The PCE was designed to measure applicants’ isokinetic force-generating capability (strength) of muscle groups based on the outcomes of a defensible job task analysis (JTA). The JTA was conducted according to guidelines of the Americans With Disabilities Act of 1990 (ADA) to determine the skills necessary to safely and effectively perform the essential functions associated with nursing duties (e.g., lifting, carrying, bending, stooping, climbing.). These validation studies were completed to identify appropriate cutoff scores using the U.S. Department of Labor strength definitions for medium, heavy, and very heavy job tasks (Dictionary of Occupational Titles, 2015). It was determined that the “target score” for the nursing job category would be set at the medium strength level. The results of the JTA indicated that movement patterns of the major muscle groups included shoulder flexion and extension and knee flexion and extension, critical to safely perform the essential functions of nursing jobs.
PCE testing was conducted in the Occupational Medicine Department, in a controlled environment using isokinetic equipment (Biodex, 2015) and a standardized testing process (i.e., tested at 60° per second, two sets of five repetitions flexion and extension for knees and shoulders) administered by trained professionals. To improve reliability of the measure, health system physical therapists and athletic trainers were trained and observed for proper technique administering the PCE, verifying that they completed the evaluation correctly. PCE results were collected at the time of the assessment and submitted to a centralized database for interpretation. These objective evaluations were then interpreted by a third-party company (Industrial Physical Capability Services, Inc., n.d.). The interpretation included isokinetic measurements through
a force curve analysis in which the applicant’s force curves were compared with an unmatched normative force curve derived from nearly 300,000 normative curves in the existing database;
a body muscle symmetry analysis, which compared each applicant’s right and left shoulder and knee scores, agonist to antagonist muscle groups and upper and lower body scores to a normative database consisting of more than 300,000 symmetry scores; and
assessing each applicant’s strength to body weight ratio score.
The screening took approximately 30 minutes to complete per applicant. PCE results were collected during the assessment and submitted to a centralized database for data interpretation. PCE data were analyzed based on proprietary algorithms, and scores were electronically returned to human resources in summary reports. An applicant was recommended for hire if the PCE strength screening score was equal to or greater than the “target score.” The target score was based on the strength level of the job as determined by the JTA.
Data Sources and Analysis
Health care and pharmacy claims cost data for the first 12 months of employment were obtained for each annual cohort from the employer-sponsored health plan. The analyses included data for all newly hired nurses who had 12 months of continuous enrollment in the employer-sponsored health plan after their hire dates.
Total annual and per member per month (PMPM) paid health care and pharmacy costs were calculated for nurses hired in each of the 2 years prior to initiation of the PCE (2009 and 2010) and for nurses hired after the PCE program was initiated (2011 and 2012). Due to unequal sample sizes and unequal variances, the Kolmogorov–Smirnov test was used to calculate significant differences between the HC and PCE groups.
Results
Of the 3,205 nurses who were included in this study, 86% were females. No nurses refused to participate in the physical capability screening. Table 1 shows the number of eligible nurses hired for each group each year. In 2009-2010, 1,120 eligible nurses were hired and included in the HCG; 2,085 eligible nurses were included in the PCE group. The total member months for the HCG was 13,440 months (7,500 + 5,940) and for the PCE group 25,020 months (8,520 + 16,500) as shown in Table 1.
Number of Eligible Nurses Hired Each Year by Group
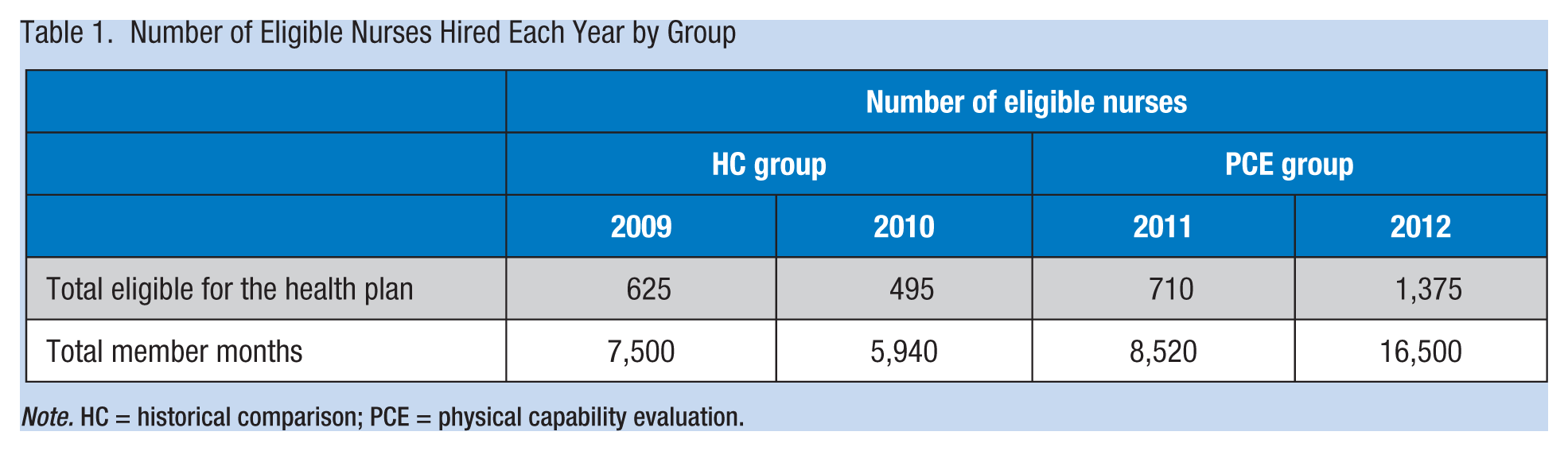
Note. HC = historical comparison; PCE = physical capability evaluation.
The total paid annual and PMPM health care and pharmacy costs for the PCE group were significantly lower than for the HCG (see Table 2). As shown in Table 3, the difference in health care paid PMPM between the HCG and the PCE™ groups was US$107.60. The total estimated cost avoidance in health care paid cost for the PCE™ program participants over 2 years was US$2,692,152 based on the reduced health care paid PMPM for the PCE™ group.
Paid Annual Health Care and Pharmacy Claims for HC and PCE Groups
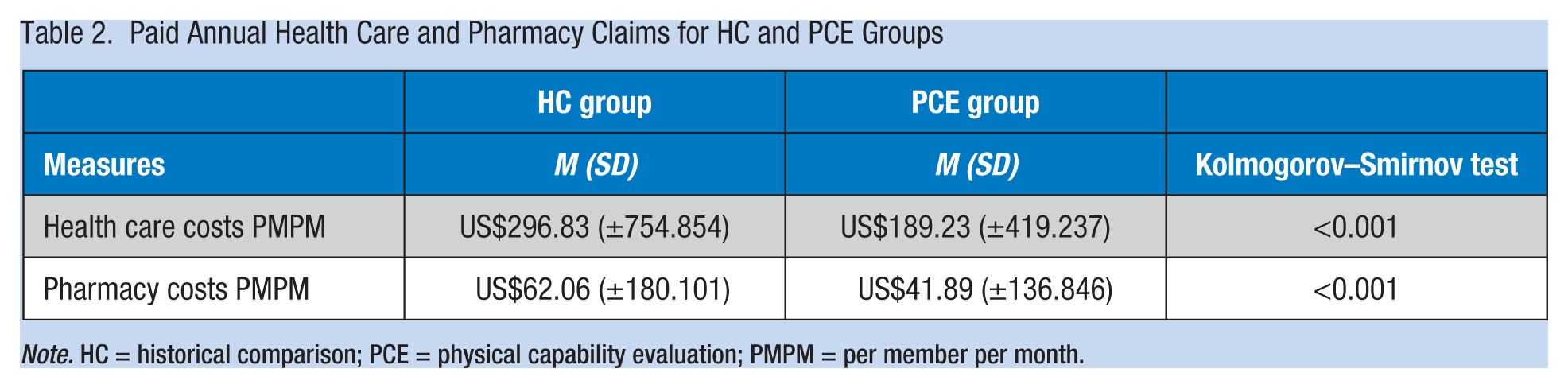
Note. HC = historical comparison; PCE = physical capability evaluation; PMPM = per member per month.
PMPM Cost Differentials for the Historical Comparison Group Versus the PCE Group
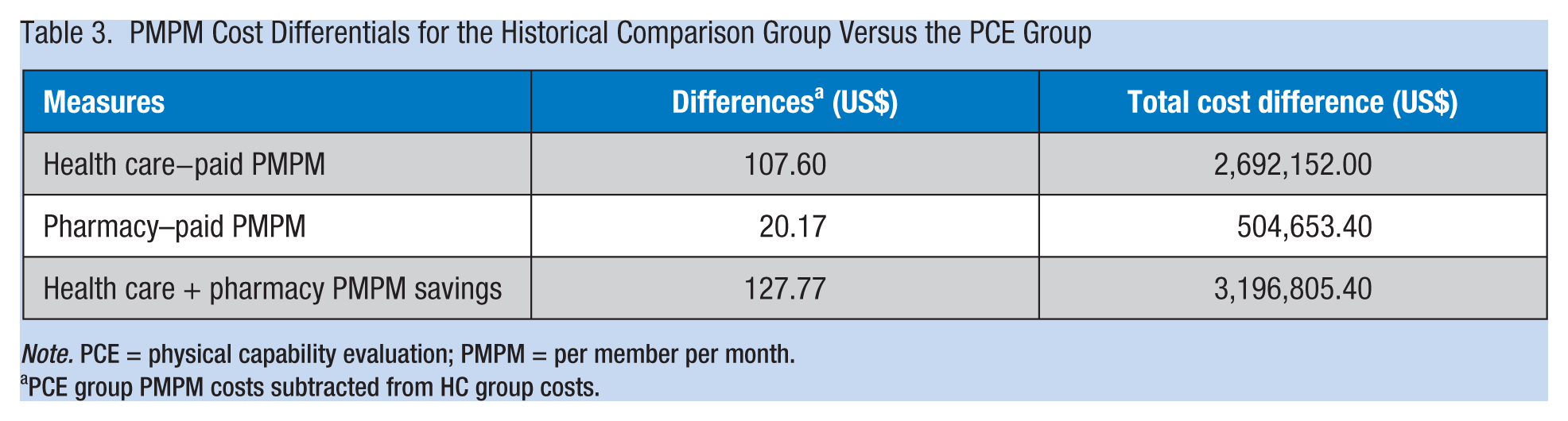
Note. PCE = physical capability evaluation; PMPM = per member per month.
PCE group PMPM costs subtracted from HC group costs.
The difference in pharmacy paid PMPM between the HC and the PCE™ groups was US$20.17. The total estimated cost avoidance for pharmacy paid cost for the PCE™ program participants over 2 years was US$504,653 based on the reduced pharmacy paid PMPM for the PCE™ group. The expenses for the PCE™ program in 2011 and 2012 were US$410,985. Based on the savings generated by the PCE™ of $3,196,805 for two years, or $1,598,403 per year, the return on investment for those in the health plan is calculated to be 7.8:1.
Discussion
This study is one of the first to look at the impact of hiring nurses with adequate physical capabilities on health care and pharmacy paid claims costs and workers’ compensation costs. The findings show significant differences in health care and pharmacy PMPM costs equal to reductions of 36% and 33%, respectively. Grossmeier et al. (2013) calculated total wellness savings of more than US$17 million based on 291,149 wellness participant months. Although the current study had fewer participants, its PMPM total savings of US$127.77 is greater than the PMPM savings reported by Grossmeier.
In addition to the health care and pharmacy analysis, tracking is ongoing for PCE and HC group workers’ compensation claims. Preliminary analysis of the loss runs showed that the frequency and severity of workers’ compensation claims were less for the PCE™ group than for the HCG.
In general, most industry sectors are taking a more holistic view of workers in an effort to better manage health care costs. Most population health management studies look at workers once they are hired (Parry & Sherman, 2012; Grossmeier et al., 2013). This initial study investigated the impact of a new hire selection program designed to hire healthier workers based on a work-justified strength assessment. The outcome supports the integration of multiple disciplines when studying the health of workers.
Hiring healthier workers and then maintaining worker health are critical to managing health care costs, especially when the average age of workers increases each year (Hymel et al., 2011; Matthews, Moore, George, Sampson, & Bowles, 2012; Reid & Fielding, 2012). In fact, Hymel states that a healthier workforce is a safer workforce, and a safer workforce produces a safer workplace, which in turn reduces health care costs (Hymel et al., 2011). The challenge is to sustain workers’ health.
Physical activity has been linked to health for many years (Kwak et al., 2014; Vehtari et al., 2014; Von Thiele Schwarz & Hasson, 2012). The U.S. Department of Health and Human Services in 2008 published Physical Activity Guidelines for Americans (U.S. Department of Health and Human Services, 2008). Those guidelines for the first time included recommendations to improve strength at all age levels. Strength has been shown to enhance metabolism, protect joints against injury, increase calcium uptake into the bone and prevent calcium loss, and improve functionality. Because the PCE™ program focuses on strength and strength relative to body weight, maintaining healthier workers could be accomplished through wellness programs that focus on maintaining or improving the strength of workers. This strategy is a challenge because most workers lose about 30% of their muscle mass between ages 30 and 65 (i.e., sarcopenia; Matthews et al., 2012; Reid & Fielding, 2012). The good news is that muscle loss is not inevitable to this extent if workers are provided appropriate incentives to maintain muscle mass (Garber et al., 2011). PCE™ assessments for incumbent workers could be offered every 2 years to assess the strength of workers. Incentives to participate could be based on the natural interest of individuals to maintain their health or avoid injury. Also, incentives could include adjustments to health plan premiums designed to encourage participation.
Study Weaknesses
Although the findings of this study support the use of PCEs when hiring nurses, several methodological weaknesses are worth noting. First, the study design is subject to temporal bias, given the possibility that practices other than the hiring protocol differed between the two time periods (pre- and post-PCE implementation). To the authors’ knowledge, no changes in hospital group policies, benefits coverage, or other protocols competed as explanations for the findings.
A second potential weakness of the study was that health care and pharmacy costs related to all causes were used as a proxy for occupational health care and pharmacy costs. Future studies should focus on health care and pharmacy costs and other outcomes that are more directly related to work-related performance, injuries, or lost time (i.e., absences, workers’ compensation claims). Because workers’ compensation claims generally take about 5 years to fully mature, a few more years are needed before an accurate assessment can be made but the downward trend is encouraging.
Conclusion
The results from this study show that it is possible to design a defensible strength test as part of the selection process for physically demanding nursing jobs. This study demonstrates the importance of physical strength, specifically in the nursing profession. When nurses’ physical capabilities are correctly matched to the physical demands of their jobs, nurses can better meet the essential functions of the job and better serve patients. Also, this study shows that it is possible to hire, through a work-justified strength screening program, healthier workers who will incur lower health care and pharmacy PMPM costs in the first year of benefit eligibility. The results of this study support the premise that strength is a new vital sign for workplace health.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Paul Terpeluk, DO, MPH is the Medical Director of Employee Health Services at the Cleveland Clinic. In this capacity, he is responsible for developing and implementing a comprehensive and wide-ranging strategy for the Clinic’s 40,000 employees that includes occupational health, workers’ compensation, disability and health plan management.
Bruce Rogen graduated from Brown University and then attended Tulane University Medical School for both his MD and MPH degrees, and completed his residency in general internal medicine at UCLA in 1991. He worked with Kaiser Permanente in Los Angeles for many years as a board certified internal medicine specialist, including positions as assistant chief of medicine, director of hospital medicine, and director of utilization. Since 2009 he has been Chief Medical Officer for the 85,000 member Cleveland Clinic Employee Health Plan, while maintaining a small clinical practice.
Thomas Gilliam earned his PhD in Exercise Physiology from Michigan State University in 1973 and served as a tenured faculty member at the University of Michigan until 1982. At that time, he entered industry to perform muscular strength test for new hire applicants and returning injured workers. He founded IPCS in 1998.